
Abstract
Understanding the factors that influence people’s decisions regarding vaccination is essential to promote vaccination. We aimed to clarify the motivations for receiving booster vaccines. We conducted a paper-based questionnaire distributed during January–February 2022 involving students and faculty staff who received the first COVID-19 vaccination at the mass vaccination program during June–September 2021 at Keio University. A total of 1725 participants were enrolled, and all completed the survey. Among these, 64.9% reported a significant adverse event (AEs) affecting daily life after the second vaccine. “Fear of severe COVID-19 illness” (72.6%) was the most common reason for getting vaccinated, followed by “concern of infecting others” (68.4%) and “fear of COVID-19 infection itself” (68.3%). Television emerged as the most influential source of information (80%), followed by university information (50.2%) and social networking sites (42.8%). Multivariate analysis revealed “fear of severe COVID-19 illness”, “fear of COVID-19 infection itself”, and “trust in the efficacy and safety of the vaccines in general” were significantly correlated with willingness to receive paid vaccinations. The severity of AEs and source of information were not related to participants’ willingness to receive booster vaccinations. Participants with positive reasons for vaccination were more likely to accept a third dose.
Similar content being viewed by others

Introduction
Vaccines against severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) have been administered worldwide since the end of 2020 with the aim of achieving herd immunity against a pandemic using the first commercially available technology of mRNA vaccines1. However, the waning of vaccine efficacy2,3,4,5 and emergence of variant strains make it challenging to eradicate COVID-19 with vaccines alone; therefore, booster vaccinations are crucial6.
Providing adequate and accurate information to vaccine recipients is an important aspect for promoting vaccination7,8,9,10. Attitudes toward vaccines vary across demographic groups11,12,13; therefore, vaccine promotion strategies need to consider country or region-specific factors that motivate people to receive vaccines. Various factors have been reported to be associated with willingness to receive vaccination in Japan; for example, high levels of knowledge relating to vaccines14, information provided on LINE (a kind of social-network service provided by LY Co., Tokyo, Japan) or at workplace/school15, and several items in the health belief model (HBM, which is a widely used theory for predicting preventive health-related behavior) have been reported to be associated with the increased uptake of vaccination14,15,16,17. However, these factors are likely to be confounding factors; comprehensive assessments of the factors are scarce, and motivation for vaccination is still poorly understood, especially in Japan.
The present study aimed to address this gap in the knowledge by clarifying the motivations for receiving COVID-19 booster vaccinations in Japan. To this end, we analyzed the factors contributing to vaccine uptake from different perspectives. The findings presented here provide important information for the promotion of vaccines and future vaccination programs.
Material and methods
Participants' recruitment and data collection
This study was conducted through distribution of a paper-based cross-sectional questionnaire survey. The questionnaire (translated into English) is included in the Supplementary Material. From June 21 to September 3, 2021, Keio University's Mita Campus hosted mass vaccinations for the first series of doses (given twice, one month apart). Keio University is a general university located in the center of Tokyo, with a student population of over 30,000. Students and faculty staff who received vaccines through the program were invited to participate in this study via intranet announcements, the university's bulletin board, and Twitter (@keio_covid). Potential participants applied via our website from January to February 2022, the period before the participants received their third dose.
The questionnaire
The questionnaire included four sections: the first included basic information about the participants; the second included items about adverse events (AEs) after vaccination; the third included items about the history of COVID-19; and the final included items about thoughts about this vaccine and vaccines in general. The final section included questions such as "Would you like to receive the third vaccination?" and "If the third vaccination required charges, how much would you be willing to pay for it?" to further stratify participants' attitudes toward vaccines18.
The questionnaire consisted of six A4 pages and took approximately 10 min to complete. Questionnaires were mailed to the study participants in advance, who were asked to fill them out ahead of time. Completed questionnaires were brought to our study site by participants, where they were collected. The data were analyzed anonymously, and items that were not completely filled out were also included in the analysis.
The survey was conducted simultaneously with another study involving the measurement of anti-spike antibody titers from blood samples. Participants received 1000 JPY and the information on their antibody titer in return for their participation. We did not include antibody titers in the analysis.
Statistics
We performed modified Poisson regressions to estimate the influence of each variable on participants’ willingness to receive the third vaccination, which they had to pay for19. Items were scored using a five-point Likert scale and then analyzed by converting into binary variables according to whether they were positive (those ranked 4 or 5) or not positive (those ranked 1–3). The price paid for the third vaccination was analyzed as an ordinal variable, and the influence of each variable was estimated by ordinal logistic regression with a proportional odds model20. In ordinal logistic regression, participants who indicated that they would choose not to receive a third vaccination were assigned to the lowest class. Univariate regression analyses were performed using modified Poisson and ordinal logistic regression, followed by multivariate regression analysis using a model that included all variables to control for effects of other variables (e.g., confounding). Risk ratios and 95% confidence intervals (CIs) were estimated in modified Poisson regression, and odds ratios (OR) and 95% CIs were estimated using ordinal logistic regression.
All statistical analyses were performed by available case analysis using R version 4.2.1 (The R Foundation for Statistical Computing; Vienna, Austria).
Ethical approval and consent to participate
The study has been carried out in accordance with The Code of Ethics of the World Medical Association (Declaration of Helsinki) and was approved by the Keio University School of Medicine Ethics Committee (approval no. 20211089), and written informed consent was obtained from each participant.
Results
A total of 49,320 people were vaccinated at our university campus during the period of interest, with 1725 (~ 3.5%) of them participating in this study. All enrolled participants completed the questionnaire. The participants' characteristics are summarized in Table 1. Approximately 66.4% of the participants were undergraduate and graduate students, while 33.4% were faculty staff. Fewer than 10% of the participants had underlying medical conditions, with hypertension being the most common (3.1%). There were four pregnant women. All had received two doses of the vaccine with no booster dose. Thirty-six subjects (2.1%) had a history of COVID-19, with seven being asymptomatic, 26 having mild disease, and the remaining three being uncertain. In addition, 10 patients had a long COVID, defined by multisystemic condition comprising often severe symptoms that follow a SARS-CoV-2 infection21, six had a taste and smell disorder, and two complained of fatigue.
Postvaccination AEs are summarized in Figs. 1 and 2. We found that AEs were more common after the second vaccination compared with the first. After the second vaccination, 86.4% reported fever and 64.9% reporting a major impact on daily life (i.e., unable to work due to AEs).

Impact of adverse events (AEs) on daily lives after the first and the second vaccinations. We defined four levels of impact, with major impact indicating that they could not work due to AEs, moderate impact indicating that their work efficacy deteriorated, little impact indicating that their work was little affected, and no impact.

Summary of postvaccination adverse events. We have shown the percentage of participants who experienced each symptom after the first vaccination, as indicated by the gray bar, and after the second, as indicated by the black bar. “COVID arm” is a rash that can appear from a few days to more than a week after vaccination and can sometimes be quite large.
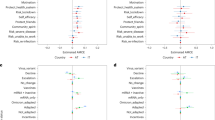
The factors that influenced the getting vaccinated, as well as the information resources used, are summarized in Figs. 3 and 4. Fear of severe COVID-19 illness (72.6%) was the most common reason for deciding to vaccinate, followed by concern of getting others infected (68.4%) and fear of COVID-19 infection itself (68.3%). In addition, 30.6% said they would be vaccinated because others around them were. Television was by far the most common information resource, accounting for 80% of respondents, followed by university information (50.2%) and social networking services (42.8%).

Reasons for getting vaccinated. The percentage of participants who said this was the reason for vaccination is shown for each item.

Sources of information on vaccines. We showed where the study participants received their information on vaccination, broken down into affiliations.
The responses on a five-point Likert scale questionnaire are depicted in Fig. 5. Despite some concerns about short- and long-term adverse reactions, 90.3% of respondents did not regret being vaccinated, and 86.5% of responders were optimistic about the third vaccination. Furthermore, 75.2% of respondents were willing to get vaccinated even if they had to pay for the third vaccination, with the median cost being 3000 JPY (Supplemental Fig. 1).

Thoughts on COVID-19 vaccines and vaccines in general. The study participants answered each of the 11 questions on a five-point Likert scale.
A complete case analysis using data from 1630 (94.5%) participants without missing values was conducted to analyze the factors influencing participants’ motivation for vaccination. As Table 2 shows, these factors influenced participants’ decision, even in cases where the vaccinations were not free. The Supplementary Table shows the results of our analysis of factors influencing participants’ willingness to pay. In multivariate analysis, the risk ratios and odds ratios with 95% CIs that did not include 1.000 are shown in bold, that is, “Everyone would get vaccinated,” “Fear of COVID-19 infection itself,” “Fear of severe COVID-19 illness,” “Do you hesitate to get vaccinated?,” “Do you think you were right to vaccinate?,” “Student,” “Smoking history,” “Newspapers,” “Did you expect that mass vaccination would loosen behavioral restrictions?”, “Do you believe in the efficacy of vaccines in general?”, and “Do you believe in the safety of vaccines in general?”.
Discussion
We conducted questionnaire survey to investigate the motivation to get vaccination. Many subjects did not regret receiving the vaccine and were willing to receive a third dose, although AEs after vaccination appeared to be much stronger than with conventional vaccines of other diseases. In fact, they believed in the vaccine's efficacy and safety and were willing to receive it at their own discretion, possibly due to the successful dissemination of information about the vaccine's efficacy and safety.
A variety of factors can influence the decision to receive vaccinations. These factors can be socioeconomic, psychological, and informational. We found health beliefs to be the major determinants for hesitancy relating to COVID-19 vaccination. The health belief model (HBM) is one of the most widely used models for understanding vaccination behavior against COVID-1910,17,18,22. According to the theory, health-related behavior is determined by a combination of several factors including perceived susceptibility, perceived severity, perceived benefits, perceived barriers, cues to action, and self-efficacy16,22. The present study evaluated factors that form part of the HBM items (Table 3); however, some items were unclassifiable, suggesting that vaccination motivation cannot be fully explained by the HBM alone. We found that perceived susceptibility, perceived severity, and perceived benefits are all positively correlated with willingness to receive a third COVID-19 vaccination, consistent with previous reports22, but items classified into cues to action in this study were negatively correlated. Other studies have used theories of health behavioral science to analyze vaccination motivations23,24,25; however, the present study and a previous report26 found that motivations vary depending on the type and source of information, suggesting that a multimodal approach is essential for effective vaccine promotion.
Belief in the efficacy and safety of the vaccine, as well as belief in the justification for vaccination, were highly correlated with intention to receive a third vaccination. Positive reasons for vaccination included trusting in the rightness of vaccination and believing in the efficacy and safety of vaccines in general. Participants with passive reasons for vaccination, such as “everyone will get vaccinated”, were more hesitant to vaccinate a third time. Trust is an important factor for vaccine promotion and has been reported to be a denominator for vaccine acceptance27. Our results suggest that vaccine promotion in Japan has been somewhat successful; however, our study design may have introduced some bias, as people who are in favor of vaccines may be more likely to participate. We also asked study participants to address those bias about their willingness to pay for vaccination to stratify willingness to vaccinate, based on a previous study18. We found similarities between the items involved in participant’s decision to receive a third vaccination. The primary reason for hesitance toward paid-for vaccinations in the students was considered to be financial insecurity. A history of smoking was correlated with a willingness to vaccinate, even if the cost was higher. This may be because of the perceived higher risk of serious illness.
Television was by far the most common source of information about vaccination. The majority of participants were young; although the media landscape is diversifying in Japan, television may remain an important source of information. Previous studies have shown both positive and negative effects of social networking services on vaccination28, but our study found neither. Further research is needed to determine how vaccine-related information sources influence vaccination intentions.
This study has some limitations that should be acknowledged. First, the number of participants was small compared with the total number vaccinated in the mass vaccination program. Participants were recruited via intranet announcements, campus bulletin boards, and Twitter; however, it was not possible to contact all 49,320 people who were vaccinated in the mass vaccination. In addition, the study period fell during a university holiday, resulting in low participation. Therefore, the study may have selectively attracted more people who were interested in the vaccine and were willing to be vaccinated, leading to potential bias. However, the percentage of people who reported getting vaccinated for the passive reason of “everyone will get vaccinated” was not significantly different from previous reports29,30,31, suggesting that the selection bias may not be significant.
Second, this study does not clarify the best approach to recruit participants who did not receive vaccination, because all subjects in this study favored vaccination. It is necessary, therefore, to conduct a study in which subjects are randomly selected from a population containing various people with different views on getting vaccinated and asked to complete a questionnaire.
It is also worth noting that the above vaccination arguments presume that the vaccine is effective and safe. Amid a pandemic, promoting the vaccination of the entire population with a vaccine with a completely new mechanism may pose a significant risk. For instance, a study found that the North American university COVID-19 vaccine was likely to cause net-expected harm to young healthy adults—they estimated approximately 18.5 severe AEs for each hospitalization averted, including myocarditis, and 1430–4626 disruptions of daily activities—that were not outweighed by a proportionate public health benefit32. The survey results indicate that the promotion in Japan was successful, but the correlation between the high vaccination rate and socioeconomic or public impact must be investigated further.
Conclusions
The severity of AEs and the source of information are not significantly related to individuals’ willingness to receive booster vaccinations for COVID-19. Factors that are most associated with willingness to receive a third dose are fear of severe COVID-19 illness, fear of COVID-19 infection itself, belief in the rightness of getting vaccination, and trust in the efficacy and safety of the vaccines in general.
Data availability
The datasets used and analyzed during the current study are available from the corresponding author upon reasonable request.
Abbreviations
- AEs:
-
Adverse events
- CI:
-
Confidence intervals
- COVID-19:
-
Coronavirus disease 2019
- HBM:
-
Health belief model
- SARS-CoV-2:
-
Severe acute respiratory syndrome coronavirus-2
References
Jain, S., Venkataraman, A., Wechsler, M. E. & Peppas, N. A. Messenger RNA-based vaccines: Past, present, and future directions in the context of the COVID-19 pandemic. Adv. Drug Deliv. Rev. 179, 114000 (2021).
Goldberg, Y. et al. Protection and waning of natural and hybrid immunity to SARS-CoV-2. N. Engl. J. Med. 386, 2201–2212 (2022).
Menegale, F. et al. Evaluation of waning of SARS-CoV-2 vaccine-induced immunity: A systematic review and meta-analysis. JAMA Netw. Open 6, e2310650 (2023).
Arashiro, T. et al. Immune escape and waning immunity of COVID-19 monovalent mRNA vaccines against symptomatic infection with BA.1/BA.2 and BA.5 in Japan. Vaccine 41, 6969–6979 (2023).
Ferdinands, J. M. et al. Waning of vaccine effectiveness against moderate and severe covid-19 among adults in the US from the VISION network: Test negative, case-control study. BMJ 379, e072141 (2022).
Regan, J. J. et al. Use of updated COVID-19 vaccines 2023–2024 formula for persons aged ≥ 6 months: Recommendations of the advisory committee on immunization practices—United States, September 2023. MMWR Morb. Mortal Wkly. Rep. 72, 1140–1146 (2023).
Rossi, M. M., Parisi, M. A., Cartmell, K. B. & McFall, D. Understanding COVID-19 vaccine hesitancy in the Hispanic adult population of South Carolina: A complex mixed-method design evaluation study. BMC Public Health 23, 2359 (2023).
Small, N. N. et al. COVID-19 knowledge, beliefs, and intention to get vaccinated: A brief educational intervention among black and Hispanic populations. Am. J. Public Health 114, S82–S86 (2024).
Piltch-Loeb, R. et al. Safety, efficacy, and ill intent: Examining COVID-19 vaccine perceptions among the new undervaccinated moveable middle in a U.S. cohort, October 2022. Vaccines https://doi.org/10.3390/vaccines11111665 (2023).
Yenew, C., Dessie, A. M., Gebeyehu, A. A. & Genet, A. Intention to receive COVID-19 vaccine and its health belief model (HBM)-based predictors: A systematic review and meta-analysis. Hum. Vaccin. Immunother. 19, 2207442 (2023).
Wong, L. P. et al. COVID-19 vaccination intention and vaccine characteristics influencing vaccination acceptance: A global survey of 17 countries. Infect. Dis. Poverty 10, 122 (2021).
Choi, J. & Ryu, J. G. COVID-19 vaccination intention among nursing, medical, and dental students: A systematic review and meta-regression analysis. Hum. Vaccin. Immunother. 19, 2253600 (2023).
Yassin, E. O. M. et al. COVID-19 vaccination acceptance among healthcare staff in Sudan, 2021. J. Immunol. Res. 2022, 3392667 (2022).
Takahashi, S. et al. A high level of vaccine knowledge increases people’s behavioral risks for contracting COVID-19 in Japan. Soc. Sci. Med. 310, 115256 (2022).
Hori, D., Takahashi, T., Kaneda, Y., Ozaki, A. & Tabuchi, T. The influence of information sources on intention changes to receive COVID-19 vaccination: A prospective cohort study in Japan. Environ. Health Prev. Med. 28, 10 (2023).
Rosenstock, I. M. The health belief model and preventive health behavior. Health Educ. Monogr. 2, 354–386 (1974).
Miyachi, T. et al. COVID-19 vaccine intention and knowledge, literacy, and health beliefs among Japanese university students. Vaccines https://doi.org/10.3390/vaccines10060893 (2022).
Wong, L. P., Alias, H., Wong, P.-F., Lee, H. Y. & AbuBakar, S. The use of the health belief model to assess predictors of intent to receive the COVID-19 vaccine and willingness to pay. Hum. Vaccin. Immunother. 16, 2204–2214 (2020).
Zou, G. A modified poisson regression approach to prospective studies with binary data. Am. J. Epidemiol. 159, 702–706 (2004).
Bender, R. & Grouven, U. Ordinal logistic regression in medical research. J. R. Coll. Physicians Lond. 31, 546–551 (1997).
Davis, H. E., McCorkell, L., Vogel, J. M. & Topol, E. J. Long COVID: major findings, mechanisms and recommendations. Nat. Rev. Microbiol. 21, 133–146 (2023).
Limbu, Y. B., Gautam, R. K. & Pham, L. The health belief model applied to COVID-19 vaccine hesitancy: A systematic review. Vaccines https://doi.org/10.3390/vaccines10060973 (2022).
Pedersen, B. et al. Development and assessment of a six-item index to gauge motivation to receive COVID-19 vaccination. Vaccines https://doi.org/10.3390/vaccines12010006 (2023).
Eitze, S. et al. Vicarious experiences of long COVID: A protection motivation theory analysis for vaccination intentions. Vaccine X 16, 100417 (2024).
Ma, M. et al. Temporal changes in factors associated with COVID-19 vaccine hesitancy among Chinese adults: Repeated nationally representative survey. SSM Popul. Health 25, 101574 (2024).
Nomura, S. et al. Reasons for being unsure or unwilling regarding intention to take COVID-19 vaccine among Japanese people: A large cross-sectional national survey. Lancet Reg. Health West Pac. 14, 100223 (2021).
Adhikari, B., Yeong Cheah, P. & von Seidlein, L. Trust is the common denominator for COVID-19 vaccine acceptance: A literature review. Vaccine X 12, 100213 (2022).
McKinley, C. J. & Limbu, Y. Promoter or barrier? Assessing how social media predicts Covid-19 vaccine acceptance and hesitancy: A systematic review of primary series and booster vaccine investigations. Soc. Sci. Med. 340, 116378 (2024).
Harada, T. & Watanabe, T. Changes in vaccine hesitancy in japan across five months during the COVID-19 pandemic and its related factors. Vaccines https://doi.org/10.3390/vaccines10010025 (2021).
Machida, M. et al. Acceptance of a COVID-19 vaccine in Japan during the COVID-19 pandemic. Vaccines https://doi.org/10.3390/vaccines9030210 (2021).
Okamoto, S., Kamimura, K. & Komamura, K. COVID-19 vaccine hesitancy and vaccine passports: A cross-sectional conjoint experiment in Japan. BMJ Open 12, e060829 (2022).
Bardosh, K. et al. COVID-19 vaccine boosters for young adults: A risk benefit assessment and ethical analysis of mandate policies at universities. J. Med. Ethics 50, 126–138 (2024).
Acknowledgements
The authors would like to thank the kind assistance of Kumiko Matsuzaki, Mari Katsumata, the faculty and the staff of Keio University Health Center, and all the university staff involved in this project. We also thank Enago (www.enago.jp) for the English language review.
Funding
This study was funded by the Japan Agency for Medical Research and Development [AMED; Grant No. JP21fk0108469 and No. JP223fa627011].
Author information
Authors and Affiliations
Contributions
Sho Uchida: Conceptualization, Methodology, Investigation, Data curation, Visualization, Writing-Original Draft; Shunsuke Uno: Conceptualization, Methodology, Investigation, Writing-Original Draft, Writing-review & editing; Masahiro Kondo: Data Curation, Formal analysis, Writing-Original Draft; Yoshifumi Uwamino: Conceptualization, Investigation, Project administration, Funding acquisition; Ho Namkoong: Investigation, Project administration, Funding acquisition; Tomoyasu Nishimura: Investigation, Supervision; Kana Misawa, Shoko Kashimura, Kei Yamato, and Tamami Ishizaka: Investigation, Project administration; Kengo Nagashima: Formal analysis, Supervision; Yuko Kitagawa and Naoki Hasegawa: Conceptualization, Supervision, Project administration, Funding acquisition.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Uchida, S., Uno, S., Kondo, M. et al. Factors affecting motivation for receiving a booster dose of the COVID-19 vaccine among Japanese university students and staff: a cross-sectional questionnaire survey. Sci Rep 14, 8009 (2024). https://doi.org/10.1038/s41598-024-58603-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-58603-9
Keywords
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
