
Abstract
Congenital Zika syndrome (CZS) is a cluster of malformations induced by Zika virus (ZIKV) infection and the underline mechanisms involved in its occurrence are yet not fully understood. Along with epidemiological and environmental factors, the genetic host factors are suggested as important to the CZS occurrence and development, however, few studies have evaluated this. This study enrolled a total of 245 individuals in a case–control association study compound a cohort of high specific interest constituted by 75 mothers who had delivered CZS infants, their 76 infants, and 47 mothers that had delivered healthy infants, and their 47 infants. Sixteen single-nucleotide polymorphisms on TREM1, CXCL10, IL4, CXCL8, TLR3, TLR7, IFNR1, CXCR1, IL10, CCR2 and CCR5 genes were genotyped to investigate their association as risk factors to CZS. The results show an association between C allele at TREM1 rs2234246 and C allele at IL4 rs224325 in mothers infected with ZIKV during pregnancy, with the increased susceptibility to CZS occurrence in their infants and the SNP CXCL8 rs4073 and the G allele at CXCL10 rs4508917 with presence of CZS microcephaly in the infants. Furthermore, the T allele at CXCL8 rs4073 and TRL7 rs179008 SNPs were associated with the severity of microcephaly in children with CZS. These results suggest that these polymorphisms in genes of innate immune responses addressed here are associated to increased risk of occurrence and severity of CZS in pregnant mothers infected with ZIKV and their CZS infants.
Similar content being viewed by others

Introduction
Congenital Zika syndrome (CZS) is a cluster of neurological congenital malformations, especially microcephaly, that can occur as consequence of vertical transmission of Zika virus (ZIKV) from mothers infected during pregnancy to their fetus1,2. The human infection by this arthropod-borne flavivirus is mostly transmitted by Aedes mosquitoes, although there are other forms of transmission3. Also, infections are usually asymptomatic or trigger mild disease4,5, however severe disease, represented mostly by neurologic disorders, as Guillain–Barré syndrome and the CZS1,6,7, can occur and are the most important clinical outcome o-f ZIKV infection. CZS occurs only in a small percent of infections during pregnancy1,8. The rate of occurrence of malformation resulting from CZS seems to vary according to geographical location, the gestational age and immune factors. These observations and the knowledge that the disease caused by ZIKV infection is multifactorial, in which environmental and epigenetic determinants, characteristics of the pathogen and the host, influence both the occurrence of the disease and its clinical presentation, suggests that host genetics might be an important factor to this outcome, although the genes involved still need to be better understood9,10.
Among other factors, as the ones linked to cellular maturity and placental permeability, the immune response developed during maternal–fetal transmission of ZIKV leading to malformations is not completely elucidated and there are difficulties in understanding which factors contribute to the worsening of clinical cases9,10. Previous studies have already demonstrated the participation of several genes or proteins of innate and adaptive immune responses as markers of ZIKV infection and CZS11,12,13, but in the context of disease it is difficult to know whether the seen phenotype is cause or consequence of disease.
Previous studies suggested that CZS may be influenced by genetic and/or epigenetic differences10 and shown association between variations in adenylate cyclases14, NOS2, TNFα15, Interferon-λ16 and TP5317 and de occurrence of CZS. Our group has shown an association between the single nucleotide polymorphism (SNP) in rs3775291 at TLR3, which has been previously shown to affect 50% of the function of this receptor to trigger to type I interferons antiviral responses18, in mothers infected by ZIKV during pregnancy and the CZS occurrence19. Additionally, this study also shown an association between the SNP rs1799964 at TNFα gene in the CZS babies, a low producer allele, with severe microcephaly19, reinforcing the relevance of genetic factors to ZIKV pathogenesis.
Here, using hypothesis-driven candidate genes and their previous report in the ZIKV pathogenesis or their function against viral infections or other infection disease, we tested SNPs in TREM120,21,22, CXCL1011,23, IL424,25, CXCL826, TLR319, TLR727,28,29, IFNR130,31, CXCR132, IL1033,34,35, CCR2 and CCR536 genes to investigate their association to CZS, in a cohort of mothers who had delivered CZS infants, their infants and healthy donors.
Methods
Characterization of the clinical cohort
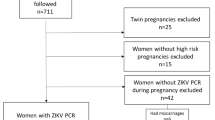
Seventy-five women who gave birth to babies with CZS (M-MICRO) from August 2015 to March 2017 and their seventy-six CZS babies (C-MICRO) were enrolled in this study and compound de case group. One of these mothers had monozygotic twins with CZS. The CZS children included here are attended at the pediatric service of the University Hospital of the Federal University of Sergipe, SE, Brazil, that is the reference center for treatment and follow-up of CZS babies in the State and were obtained by convenience and in a consecutive way. The children with CZS were followed over time by a multidisciplinary team, including pediatricians, neuropediatricians, physiotherapists, ophthalmologists, phonoaudiologists, among others. The medical team examining clinical history and performed clinical evaluation to confirm the absence of other complications during pregnancy, besides the ZIKV infection, as well as the presence of neurological congenital damage and other malformations that configure the CZS. According to the guidelines of the Brazilian Ministry of Health in Brazil, which follows the World Health Organization’s recommendations, the CZS babies were classified with severe microcephaly (CSM—more than 3 standard deviations below the mean for gestational age and sex) and microcephaly (CM—more than 2 standard deviations below the mean for gestational age and sex) at birth37. Other infections associated with neurological injury (STORCH) were discarded by serological tests. The control group was composed of 47 mothers (M-ZIKVexp) and their healthy babies (C-CT), who were matched to the CZS infants’ group by place of residence and month of birth (about 2 months of interval). All children were born in the municipalities of Sergipe state, northeast region of Brazil and all mothers lived in this same state as well. All Epidemiological data were obtained by a survey questionnaire developed by the research team. For serological assays we used Anti-Zika Virus ELISA (IgM) and Anti-Zika Virus ELISA (IgG) (Euroimmun, Medizinische Labordiagnostika AG), following manufacturer's instructions.
Genetic analysis
Whole blood samples were collected from all patients from which serum, plasm or DNA samples were obtained. Genomic DNA was extracted using PureLink® Genomic DNA Mini Kit (Invitrogem™) according to the manufacturer’s recommendations. After extraction, the DNA concentration was determined with a NanoDrop™ Lite (Thermo Scientific, Wilmington, EUA) and stored at 80 °C until use.
Sixteen SNPs from candidate genes were selected, based on their previous association with viral or other infectious diseases and the gene importance in the immune response against viruses or plausible contribution to by ZIKV diseases (Supplementary Table S1). The SNPs TREM1 rs2234246, CXCL10 rs4508917, IL4 rs2243250, CXCL8 rs4073, TLR3 rs3775290, TLR7 rs179008, IFNR1 rs2234711, CXCR1 rs2854386, IL10 rs1800871/ rs1800872/ rs1800896, CCR2 rs1799864 and CCR5 rs1800023/ rs1800024/ rs1799987/ rs1799987 were genotyped using TaqMan® probes by qPCR using 7500 Real-Time PCR (Applied Biosystems) following manufacturer’s instructions. Information about the polymorphisms evaluated are found in the Supplementary Table S1.
Statistical analysis
The Hard-Weinberg equilibrium (HWE) test was performed using GENEPOP (version 4.2). Categorical variables were compared between the groups by Chi-square test or Fisher’s Exact Test using GraphPad Prism (version 5.0). The associations between the occurrence of CZS and the SNPs were assessed by comparing case and control groups through a univariate logistic regression analysis using R software (version 3.4) with the package “SNPassoc”. To the descriptive analysis between groups, quantitative variables were tested through the Shapiro–Wilk test to verify their normality and according to the distribution found, Student’s t test or Mann–Whitney U test were utilized. The results were evaluated considering a confidence interval (CI) of 95% and the values were considered statistically significant when p < 0.05.
Ethics approval and consent to participate
This study was approved by the local Research Ethical Committee of the Federal University of Sergipe (advice number 1.486.302). All blood donors or their legal guardian gave written informed consent for their participation in the study.
Results
Clinical and epidemiological characteristics from the cohort
The characteristics of the patients included in this study are shown in Table 1. The age range in M-MICRO and M-ZIKVexp groups was 14–40 years, with an average of 25.4 and 24.3, respectively. Regarding to the presence of symptoms, higher frequency of mothers who composed the M-MICRO were symptomatic (76%), as compared to the M-ZIKVexp group (25.5%) (p ≤ 0.0001). The most frequent symptoms reported were axanthema, fever, and arthralgia, with 80.7%, 61.4% and 59.6% for the M-MICRO group and 50%, 66.7% and 58.3% for the ZIKVexp group, respectively. Regarding to the period of occurrence of symptoms, in most mothers in the M-MICRO group (50%), symptoms occurred during the first trimester of pregnancy, followed by 36.8% in the second trimester and 13.2% in the third trimester. In the M-ZIKVexp group, the trimester with the highest occurrence of symptoms was the second (50%), followed by the first trimester (33.3%) and the third trimester (16.7%).
The C-MICRO group was composed of 53.9% of females and 46.0% of males, while the C-CT group was composed of 36.2% and 63.8% of females and males, respectively. Regarding the classification of CP at birth, most children (70%) in the C-MICRO group were born with severe microcephaly (CSM), while 30% of them were born with microcephaly (CM) according to the classification explained previously. In the C-CT group, all children were born with an adequate CP for their gestational age. There were no significant differences between the period of birth of children included in the case and control groups.
To better characterize the C-MICRO group, children with microcephaly (CM) and with severe microcephaly (CSM) were evaluated and described in Table 2. Significant differences were found between groups in cephalic perimeter at birth (p ≤ 0.0001), birth weight (p = 0.004) and length at birth (p = 0.006). The differences between the groups regarding the duration of pregnancy, presence of symptoms in mothers during pregnancy and the trimester of occurrence of symptoms related to ZIKV infection were not significant.
Association of SNPs with CZS and clinical characteristics
General information about SNPs analyzed in the present work are presented in Supplementary Table S1. The EHW test showed equilibrium deviation in the control population for the SNPs CXCL10 rs4508917, TLR7 rs179008 and IL10 rs1800896.
The C allele for the SNP rs2234246 in the TREM1 gene was more frequent and associated with mothers who gave birth to CZS babies (M-MICRO) and their babies (C-MICRO) when compared with mothers (M-ZIKVexp) and children (C-CT) control groups (Table 3). Furthermore, the C allele for the IL4 rs224325 gene was more frequent and associated with mothers who gave birth to CZS infants (M-MICRO) (Table 4). No significant differences were found among case and control infants for this SNP regarding allelic or genotypic frequencies in any of the analysis performed.
The SNP rs4508917 in the CXCL10 gene was also associated with the occurrence of microcephaly when the C-MICRO group and the C-CT group were compared, showing a higher frequency and association of G allele in children with CZS. The SNP rs4073 in the CXCL8 gene was also associated with the occurrence of CZS. There were no significant differences in allele frequencies among case and control group of mothers regarding these SNPs (Table 4).
Stratifying the case group of children (C-MICRO) by the severity of microcephaly at birth, in children with severe microcephaly (CSM) and children with microcephaly (CM), the T allele in SNP rs4073 at CXCL8 gene and the T allele in SNP rs179008 at TRL7 was associated with severe microcephaly (Table 5).
There was no association between the case and control group for the other SNPs assessed (Supplementary Table S2) and the haplotype analyzed (data not shown).
Discussion
Faced with the serious public health problem occurring from ZIKV infections, the search for an understanding of the host factors that can modulate infections, interfering with their outcome, is essential. In this study, TREM1 rs2234246 and IL4 rs224325 in mothers infected with ZIKV during pregnancy was found to be associated with the occurrence of CZS microcephaly and the SNP CXCL10 rs4508917 and CXCL8 rs4073 in their children with presence of CZS microcephaly. Furthermore, the CXCL8 rs4073 and TRL7 rs179008 SNPs were associated with the severity of microcephaly in children with CZS.
The Triggering Receptor Expressed on Myeloid Cells 1 (TREM-1) is a cell surface receptor that is constitutively expressed in different types of human cells38,39,40. Its activation plays a key role in amplifying and regulating the inflammatory response in the innate immune response38 and has been studied in different diseases41,42. The rs2234246 in the TREM1 gene, located in the 3’UTR region, is characterized by a C > T variation and is described as a functional polymorphism, regulating TREM1 expression levels, with the T allele associated with higher levels of both gene expression and plasma levels of the soluble form of TREM-1 (sTREM-1) in healthy individuals22.
The findings of the present study show the association of the C allele for SNP rs2234246 in TREM1 as a risk factor for CZS. Although the role of TREM-1 has been little studied in viral infections so far, studies demonstrate increased gene expression of the TREM1 during viral infections in vitro, suggesting activation of TREM-1 signaling by viruses43,44. In addition, it is suggested that TREM-1 can recognize molecular patterns associated with viral pathogens, such as Polyinosinic:polycytidylic acid (Poly I:C), a TLR3 receptor ligand and important receptor in the pathogenesis caused by ZIKV45 and that this recognition leads to the induction of pro-inflammatory cytokines important for the reduction of viral load21,43.
Therefore, the data presented here suggest that this genetic variation in the TREM1 gene in pregnant women may influence the risk of developing CZS in their infants, indicating that lower expression/activation of TREM-1 may affect the control of ZIKV infection, which reinforces the need for a better understanding of the role of TREM-1 in the pathogenesis of CZS. Corroborating this hypothesis, previous data from our group has shown an association between SNPs in TLR3 and TNFα involved in the decrease of antiviral immune response, with CZS occurrence and severity19. In contrast, higher levels of sTREM-1 have been described as indicative of poor prognosis in early stages of DENV arbovirus infection46, and recently, on the outcomes of SARS-CoV-2 infections47.
The rs224325 SNP in the IL4 gene is in the UTR5' region and promotes the exchange of C>T nucleotides (-590C/T) and was shown that this SNP is functional, and that the alternative T variant increases IL4 promoting activity24, increasing levels of this protein48. The influence of this SNP on the outcome of diseases has been studied, with emphasis on the evaluation of its functioning in the pathogenesis of neoplasms, and it has already been associated with the susceptibility of different types of cancer49,50. In the present study, the C allele for IL4 rs224325 was more frequent and associated with mothers who had children with microcephaly due to ZIKV infection, which, according to the function described for this SNP, may be associated with lower levels of IL-424. It is possible that this gene variation helps to promote an imbalance between the Th1 and Th2 immune response. Recent study demonstrated that tissue damage in the placenta is induced by ZIKV51, but the modulation of tissue damage by the anti-inflammatory response still needs clarification. In contrast, higher levels of IL-4 were detected during the acute phase of ZIKV infection in a mother who gave birth to a child with CZS, when compared to mothers who gave birth to normal children11.
Several studies demonstrate a cytokine storm associated with children with CZS10,11,12,13,52. However, few studies evaluate genetic factors in this condition. In the infants evaluated here, an association was found between the presence of at least one G allele for the rs4508917 SNP in the CXCL10 gene and the occurrence of microcephaly. This SNP promotes a variation of A > G, with the G allele being correlated with increased expression of the chemokine of the same name23. The CXCL10 is pointed as the most promising biomarker for acute ZIKV infection due to its overexpression53. In agreement, overexpression of CXCL10 has been linked to virus-induced signaling of the type 2 interferon IFNγ pathway, although ZIKV seems to suppress the IFN-1 and IFN-3 pathway as an evasion mechanism54. This chemokine has already been associated with other neurological complications55,56. Higher levels of CXCL10 were found in children with congenital malformations born from mothers infected with ZIKV during pregnancy, when compared to those control children born normal from mothers who were also ZIKV positive during pregnancy11. In a complementary way, this same study also observed higher levels of CXCL10 in patients infected with ZIKV who developed neurological complications11.
To assess whether the SNPs evaluated in this study were associated with the severity of CZS microcephaly, the case group of children was stratified in the analysis. This apporach revealed significantly different frequencies in the rs4073 SNP in the CXCL8 gene, and the rs179008 in the TRL7 gene between the groups, associating these SNPs with the severity of microcephaly.
The CXCL8 gene is located on the short arm of chromosome 4 and encodes the protein of the same name, also known as IL-8, that crucially participating in several inflammatory processes57. The rs4073 SNP (-251A>T) is in the promoter region of the gene and is related to variations in gene expression and levels of the CXCL-8 chemokine, with the A allele being related to higher levels of CXCL-858,59. In the groups studied in this research, there was a higher frequency of the T allele in children with more severe microcephaly, an allele functionally associated with lower production of this chemokine. Due to the critical role that this cytokine plays, this SNP has been associated with different diseases58,60,61,62.
The endosomal receptor TLR-7 recognizes single-stranded RNA and plays an important role in the recognition of viral pathogens by activating the innate immune response to produce type 1 IFN29. The SNP rs179008 (A>T) is an intragenic variation and promotes the exchange of glutamine by leucine, affecting the quantity and functionality of the protein, with the T allele linked to the lowest expression of TLR7 and the lowest expression of IFNλ28. This variant has been associated with viral infections, being linked to different prognoses27,28,63,64. In the present study, an association between the T allele and more severe microcephaly is demonstrated.
Therefore, considering the functionality of these SNPs and the function of their produced proteins, the association of the T allele in CXCL8 rs4073 and the T allele in TLR7 rs179008 with the severity of microcephaly suggests that the impairing antiviral defense might attenuate a resolutive inflammatory response and contribute to CNS damage. These data agree with previous findings of our group that show an association of microcephaly with low producer alleles in genes from the antiviral response19. In line with this hypothesis, the presence of the TT genotype for this SNP in the TLR7 gene was previously associated with susceptibility to Herpes simplex virus -1 infection and an increased risk of placental infections27. Furthermore, higher levels of CXCL-8 in cerebrospinal fluid were found in neonates without CZS who were born from mothers infected with ZIKV during pregnancy, when compared to those born with microcephaly by CZS, suggesting an important role of this chemokine in protection against CZS26. Therefore, it is possible that the lower antiviral defense in the fetus predisposes to ZIKV invasion of the CNS and may be an aggravating factor in the neurological picture triggered by congenital ZIKV infection.
Despite being genes involved in immune response to viral infections and implicated in susceptibility to infections, no differences were found in genotypic and allelic frequencies between the groups of this study, in the analyzed SNPs TLR3, IFNGR1, CXCR1, IL10, CCR2 and CCR5. This fact does not rule out the influence of these SNPs on the pathogenesis triggered by ZIKV, since the non-association may have occurred due to the limited number of the samples, affecting the power of the study. In addition, differences in the frequencies of the SNPs that configurate the associations seen in the present study are limited to this population and not determinant to stablish cause and effect relation. Nevertheless, we had the opportunity to study a cohort of high specific interest, what reinforce the importance of this study as well of replication studies.
Together, the findings described here suggest that maternal genetics may influence the risk of the occurrence of CZS and that the genetics of children affected with CZS are associated with the severity of the syndrome, suggesting that an impaired antiviral response is associated with the immunopathogenesis of congenital ZIKV infection, and placing the genes TREM1, IL4, CXCL10, CXCL8 and TLR7 as promising genes for future functional studies, for a better understanding of their respective roles in the occurrence of CZS.
Data availability
All main data generated or analyzed during this study are included in this article. Additional information about the data and material collected during this study are available on reasonable request by contacting the corresponding author (Camilla Santos, camillanatallia@hotmail.com).
References
De Oliveira Melo, A. S. et al. Congenital Zika virus infection: Beyond neonatal microcephaly. JAMA Neurol. 73, 1407–1416 (2016).
Cugola, F. R. et al. The Brazilian Zika virus strain causes birth defects in experimental models. Nature 534, 267–271 (2016).
Musso, D. et al. Potential sexual transmission of Zika virus. Emerg. Infect. Dis. 21, 359–361 (2015).
Brasil, P. et al. Zika virus infection in pregnant women in Rio de Janeiro. N. Engl. J. Med. 375, 2321–2334 (2016).
Petersen, L. R. et al. Zika Virus. New Engl. J. Med. 64, 396 (2016).
Cao-Lormeau, V. M. et al. Guillain-Barré Syndrome outbreak associated with Zika virus infection in French Polynesia: A case-control study. Lancet 387, 1531–1539 (2016).
Calvet, G. et al. Detection and sequencing of Zika virus from amniotic fluid of fetuses with microcephaly in Brazil: A case study. Lancet Infect. Dis. 16, 653–660 (2016).
Jaenisch, T. et al. Risk of microcephaly after Zika virus infection in Brazil, 2015 to 2016. Bull. World Health Organ. 95, 191–198 (2017).
Pierson, T. C. & Diamond, M. S. The emergence of Zika virus and its new clinical syndromes. Nature 560, 573–581 (2018).
Caires-Júnior, L. C. et al. Discordant congenital Zika syndrome twins show differential in vitro viral susceptibility of neural progenitor cells. Nat. Commun. 9, 1–11 (2018).
Kam, Y. W. et al. Specific biomarkers associated with neurological complications and congenital central nervous system abnormalities from Zika virus-infected patients in Brazil. J. Infect. Dis. 216, 172–181 (2017).
Foo, S.-S. et al. Biomarkers and immunoprofiles associated with fetal abnormalities of ZIKV-positive pregnancies. JCI Insight 3, e124152 (2018).
de Sousa, J. R. et al. Correlation between apoptosis and in situ immune response in fatal cases of microcephaly caused by Zika virus. Am. J. Pathol. 188, 2644–2652 (2018).
Rossi, D. et al. Variations in maternal adenylate cyclase genes are associated with congenital Zika syndrome in a cohort from Northeast, Brazil. J. Intern. Med. https://doi.org/10.1111/joim.12829 (2018).
Gomes, J. A. et al. Association between genetic variants in nos2 and tnf genes with congenital Zika syndrome and severe microcephaly. Viruses 13, 1–13 (2021).
Rossi, Á. D. et al. Association between maternal non-coding interferon-λ polymorphisms and congenital Zika syndrome in a cohort from Brazilian northeast. Viruses 13, 1–6 (2021).
Gomes, J. A. et al. Functional polymorphisms in the p53 pathway genes on the genetic susceptibility to Zika virus teratogenesis. Front. Cell. Infect. Microbiol. 11, 1–8 (2021).
Zhou, P., Fan, L., Yu, K.-D., Zhao, M.-W. & Li, X.-X. Toll-like receptor 3 C1234T may protect against geographic atrophy through decreased dsRNA binding capacity. FASEB J. 25, 3489–3495 (2011).
Santos, C. N. O. et al. Association between Zika virus microcephaly in newborns with the rs3775291 variant in toll-like receptor 3 and rs1799964 variant at tumor necrosis factor-α gene. J. Infect. Dis. 220, 1797–1801 (2019).
Roe, K., Gibot, S. & Verma, S. Triggering receptor expressed on myeloid cells-1 (TREM-1): A new player in antiviral immunity?. Front. Microbiol. 5, 1–11 (2014).
Bleharski, J. R. et al. A role for triggering receptor expressed on myeloid cells-1 in host defense during the early-induced and adaptive phases of the immune response. J. Immunol. 170, 3812–3818 (2003).
Aldasoro Arguinano, A. A. et al. TREM-1 SNP rs2234246 regulates TREM-1 protein and mRNA levels and is associated with plasma levels of L-selectin. PLoS ONE 12, 1–16 (2017).
Jafarzadeh, A. et al. Higher circulating levels of chemokine CXCL10 in patients with breast cancer: Evaluation of the influences of tumor stage and chemokine gene polymorphism. Cancer Biomark. 16, 545–554 (2016).
Rosenwasser, L. J. et al. Promoter polymorphisms in the chromosome 5 gene cluster in asthma and atopy. Clin Exp Allergy 25, 74–78 (1995).
Lloyd, C. M. & Snelgrove, R. J. Type 2 immunity: Expanding our view. Sci. Immunol. 3, 1–12 (2018).
Nascimento-Carvalho, G. C. et al. Zika-exposed microcephalic neonates exhibit higher degree of inflammatory imbalance in cerebrospinal fluid. Sci. Rep. 11, 8474 (2021).
Sánchez-Luquez, K. et al. Impact of TLR7 and TLR9 polymorphisms on susceptibility to placental infections and pregnancy complications. J. Reprod. Immunol. 146, 103342 (2021).
Azar, P. et al. TLR7 dosage polymorphism shapes interferogenesis and HIV-1 acute viremia in women. JCI Insight 5, e136047 (2020).
Beutler, B. et al. Genetic analysis of host resistance: Toll-like receptor signaling and immunity at large. Annu. Rev. Immunol. 24, 353–389 (2006).
Cheng, L., Zhang, F., Wang, Y., Chen, J. & Yuan, X. Association between IFNGR1 gene polymorphisms and tuberculosis susceptibility: A meta-analysis. Front. Public Health 10, 976221 (2022).
Miner, J. J. et al. Zika virus infection during pregnancy in mice causes placental damage and fetal demise. Cell 165, 1081–1091 (2016).
Castellucci, L. C. et al. CXCR1 and SLC11A1polymorphisms affect susceptibility to cutaneous leishmaniasis in Brazil: A case–control and family-based study. BMC Med. Genet. 11, 10 (2010).
Alagarasu, K. et al. Association of combinations of interleukin-10 and pro-inflammatory cytokine gene polymorphisms with dengue hemorrhagic fever. Cytokine 74, 130–136 (2015).
Barkhash, A. V., Kochneva, G. V., Chub, E. V. & Romaschenko, A. G. Single nucleotide polymorphism rs1800872 in the promoter region of the IL10 gene is associated with predisposition to chronic hepatitis C in Russian population. Microbes Infect. 20, 212–216 (2018).
Chen, J. & Ma, A. Associations of polymorphisms in interleukins with tuberculosis: Evidence from a meta-analysis. Immunol. Lett. 217, 1–6 (2020).
Zapata, W. et al. Influence of CCR5 and CCR2 genetic variants in the resistance/susceptibility to HIV in serodiscordant couples from Colombia. AIDS Res. Hum. Retroviruses 29, 1594–1603 (2013).
Brasil. Ministério da Saúde. Microcefalia: causas, sintomas, tratamento e prevenção. http://portalms.saude.gov.br/saude-de-a-z/microcefalia (2019).
Bouchon, A., Dietrich, J. & Colonna, M. Cutting edge: Inflammatory responses can be triggered by TREM-1, a novel receptor expressed on neutrophils and monocytes. J. Immunol. 164, 4991–4995 (2000).
Bouchon, A., Hernández-Munain, C., Cella, M. & Colonna, M. A DAP12-mediated pathway regulates expression of CC chemokine receptor 7 and maturation of human dendritic cells. J. Exp. Med. 194, 1111–1122 (2001).
Allcock, R. J. N., Barrow, A. D., Forbes, S., Beck, S. & Trowsdale, J. The human TREM gene cluster at 6p21.1 encodes both activating and inhibitory single lgV domain receptors and includes NKp44. Eur. J. Immunol. 33, 567–577 (2003).
Su, L. et al. Dynamic changes in serum soluble triggering receptor expressed on myeloid cells-1 (sTREM-1) and its gene polymorphisms are associated with sepsis prognosis. Infect. Genet. Evol. 39, 1833–1843 (2012).
Liu, F. et al. TREM1: A positive regulator for inflammatory response via NF-κB pathway in A549 cells infected with Mycoplasma pneumoniae. Biomed. Pharmacother. 107, 1466–1472 (2018).
Mohamadzadeh, M. et al. Activation of triggering receptor expressed on myeloid cells-1 on human neutrophils by Marburg and Ebola viruses. J. Virol. 80, 7235–7244 (2006).
Denner, J. et al. Modulation of cytokine release and gene expression by the immunosuppressive domain of gp41 of HIV-1. PLoS ONE 8, e55199 (2013).
Dang, J. et al. Zika virus depletes neural progenitors in human cerebral organoids through activation of the innate immune receptor TLR3. Cell Stem Cell 19, 258–265 (2016).
Ruiz-Pacheco, J. A. et al. TREM-1 modulation during early stages of dengue virus infection. Immunol. Lett. 158, 183–188 (2014).
da Silva-Neto, P. V. et al. Strem-1 predicts disease severity and mortality in covid-19 patients: Involvement of peripheral blood leukocytes and mmp-8 activity. Viruses 13, 1–17 (2021).
Gonzales, J. R., Gröger, S., Haley, G., Bödeker, R. H. & Meyle, J. The interleukin-4 -34TT and -590TT genotype is correlated with increased expression and protein production in aggressive periodontitis. Mol. Immunol. 47, 701–705 (2010).
Jia, Y., Xie, X., Shi, X. & Li, S. Associations of common IL-4 gene polymorphisms with cancer risk: A meta-analysis. Mol. Med. Rep. 16, 1927–1945 (2017).
Gonzalez-Hormazabal, P. et al. Polymorphisms PSCA rs2294008, IL-4 rs2243250 and MUC1 rs4072037 are associated with gastric cancer in a high risk population. Mol. Biol. Rep. 47, 9239–9243 (2020).
Rabelo, K. et al. Zika induces human placental damage and inflammation. Front. Immunol. 11, 1–15 (2020).
Vinhaes, C. L. et al. Newborns with Zika virus-associated microcephaly exhibit marked systemic inflammatory imbalance. J. Infect. Dis. 222, 670–680 (2020).
Naveca, F. G. et al. Analysis of the immunological biomarker profile during acute Zika virus infection reveals the overexpression of CXCL10, a chemokine linked to neuronal damage. Mem. Inst. Oswaldo Cruz 113, 1–13 (2018).
Chaudhary, V. et al. Selective activation of type II interferon. J. Virol. 91, 1–17 (2017).
Liu, M. et al. CXCL10/IP-10 in infectious diseases pathogenesis and potential therapeutic implications. Cytokine Growth Factor Rev. 22, 121–130 (2011).
Chiang, S. & Ubogu, E. E. The role of chemokines in Guillain–Barré syndrome. Muscle Nerve 48, 320–330 (2013).
Remick, D. G. Interleukin-8. Crit. Care Med. 33, 466–467 (2005).
Hull, J., Thomson, A. & Kwiatkowski, D. Association of respiratory syncytial virus bronchiolitis with the interleukin 8 gene region in UK families. Thorax 55, 1023–1027 (2000).
Ohyauchi, M. et al. The polymorphism interleukin 8–251 A/T influences the susceptibility of Helicobacter pylori related gastric diseases in the Japanese population. Gut 54, 330–335 (2005).
Chen, C. H. et al. Association between interleukin-8 rs4073 polymorphism and prostate cancer: A meta-analysis. J. Formos. Med. Assoc. 119, 1201–1210 (2020).
Li, C.-H. et al. Association of interleukin-8 promoter genotypes with Taiwan lung cancer risk. Anticancer Res. 42, 1229–1236 (2022).
Noah, T. L. et al. Nasal cytokine production in viral acute upper respiratory infection of childhood. J. Infect. Dis. 171, 584–592 (1995).
Minashkin, M. M. et al. The role of genetic factors in the development of acute respiratory viral infection COVID-19: Predicting severe course and outcomes. Biomedicines 10, 549 (2022).
Askar, E., Ramadori, G. & Mihm, S. Toll-like receptor 7 rs179008/Gln11Leu gene variants in chronic hepatitis C virus infection. J. Med. Virol. 82, 1859–1868 (2010).
Acknowledgements
The authors thank the staff, donors and patients at the University Hospital of the Federal University of Sergipe, Brazil who contributed to this study.
Funding
This work was supported by the following grants: FINEP (Financiadora de Estudos e Projetos), grant number 0116005600. Authors CNOS and JAC has received a fellowship from Coordenação de Aperfeiçoamento de Pessoal de Nível Superior - Brasil (CAPES). Author LSM receive a fellowship from Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPQ). Authors ARJ, RPA and MMT are scientists sponsored by CNPQ.
Author information
Authors and Affiliations
Contributions
CNOS developed and performed experiments and wrote the manuscript. CNOS and LSM analyzed and interpreted data. ABLF, AJBB, RLSP clinically characterized patients for the study. CNOS, JCA, AMS recruited the clinical cohort for the study. CAS helped to perform the patient’s laboratorial diagnostic, including DENV IgG and ZIKV IgG ELISA. JVC helped in gathering information from patients. MMT helped prepare the manuscript. RPA and ARJ conceived and designed the study and helped to write the manuscript. PLS and ARJ supervised the research and contributed equally to the study. All the authors discussed the results and commented on the manuscript. All authors have agreed for publication.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Santos, C.N.O., Magalhães, L.S., Fonseca, A.B.d. et al. Association between genetic variants in TREM1, CXCL10, IL4, CXCL8 and TLR7 genes with the occurrence of congenital Zika syndrome and severe microcephaly. Sci Rep 13, 3466 (2023). https://doi.org/10.1038/s41598-023-30342-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-023-30342-3
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
