
Abstract
Autologous hematopoietic stem cell transplantation (HSCT) has been used to treat severe and refractory autoimmune diseases (ADs) in children and adults for more than 15 years. The aim of this treatment is to restore tolerance through an intense lymphodepleting conditioning, and many patients have achieved lasting remissions. However, HSCT is associated with significant morbidity and mortality and is therefore not yet standard of care. Pre-existing reduced organ function of patients with ADs may increase the organ toxicity of conditioning. In the early post-HSCT phase, bacterial or fungal infections occur and therapy-associated lymphopenia sets patients at risk for reactivation of endogenous viruses and other opportunistic infections. During re-emerging of lymphopoiesis after HSCT, de novo autoimmunity may develop through loss of central or peripheral control mechanisms. Late effects of autologous HSCT (e.g., on the endocrine system) and a potentially increased frequency of secondary malignancies are of concern. The steadily increasing knowledge about specific complications occurring in patients with ADs after HSCT has led to the adaption of treatment protocols and has already reduced toxicity. Further prospective long-term follow-up studies are needed to identify patients at risk for developing serious complications after HSCT.
Similar content being viewed by others
Main
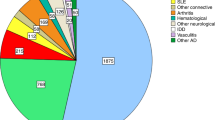
Autologous hematopoietic stem cell transplantation (HSCT) has been used as a treatment for severe and therapy-refractory autoimmune diseases (ADs) for more than 15 years. Experience with this treatment has been gathered in international databases, with the European Bone Marrow Transplantation/European League Against Rheumatism database “Promise” being the largest existing database of transplanted patients with ADs. Promise currently includes data on more than 1,300 such patients from 172 institutions in 27 countries. Additional data stem from case series and phase I and II studies. Most patients reported suffered from multiple sclerosis, systemic sclerosis (SSc), rheumatoid arthritis, systemic lupus erythematosus (SLE), juvenile idiopathic arthritis, and autoimmune cytopenias. In most cases, these patients had a chronic and progressive AD and several lines of established therapies had failed. To date, autologous HSCT has been used as a rescue strategy for patients with an expected poor prognosis and lack of alternative treatment options. In this regard, the reported overall 5-y survival of 85% and a progression-free survival of 43% in a recently published retrospective analysis of 900 patients from the European Bone Marrow Transplantation database are surprisingly positive (1). The rationale for autologous transplantation of children with severe ADs and responses to that treatment has been reviewed recently (2) and are discussed elsewhere in this issue. Results from prospective randomized trials will prove whether in these selected patients HSCT is superior to “standard of care,” if this exists, with respect to efficacy, but as important with respect to side effects. Far less is known regarding the effects of allogeneic HSCT for patients with ADs (3) and experience with the transplantation of mesenchymal stem cells in patients with ADs is only emerging. A possible advantage of allogeneic HSCT over autologous HSCT as treatment for patients with ADs is the fact that a genetically different, presumably nonautoreactive, immune system is transplanted into a host with susceptibility for autoimmunity (4). However, allogeneic HSCT is associated with graft-vs.-host disease, which has been the main hindrance for further investigating this treatment in patients with ADs so far. We therefore focus in this review on complications occurring in patients with ADs during and after autologous HSCT.
HSCT is an invasive procedure associated with severe side effects leading to morbidity and treatment-related mortality (TRM). This issue is the main limitation for the more widespread use of HSCT for patients with ADs.
TRM and nonfatal complications of HSCT have been accepted for patients suffering from malignant diseases. These patients have a high risk of immediate mortality of their disease if untreated. In contrast, most patients with ADs who are eligible for HSCT will not die immediately if not treated. However, in patients having poor prognostic factors, disease-related 5-y mortality may be higher than 30% (5), justifying a more aggressive therapeutic strategy.
To reach the goal of a lower TRM and morbidity, it is important to take a closer look at the complications of HSCT for patients with ADs reported so far and to adapt treatment protocols and patient selection in further trials. Knowledge of the complications and side effects of HSCT stems from cohorts, many including more adult patients than children.
TRM
The TRM of HSCT for patients with ADs depends on the patients’ disease and on conditioning. Patients with SLE, juvenile idiopathic arthritis, and SSc have a higher TRM than patients suffering from other diseases (1). This finding might be explained by the multisystemic nature of these diseases. In recent years, TRM was lower than reported in the early years (e.g., TRM of HSCT for SSc, the second most common indication for HSCT in ADs, was as high as 16% (6) before 2001, and in a later analysis TRM for patients with the same disease was 8.5%) (7). The reduction of TRM has been attributed to better patient selection and to adaption of conditioning regimens. Indeed, a learning curve and experience with these patients contribute to a better outcome. This finding is underlined by the results of the latest analysis of the European Bone Marrow Transplantation database, Promise, that positively correlated the number of patients treated for an autoimmune disease per center with a lower TRM (1). In this study, the overall TRM of the 900 included patients was 5%.
Infectious Complications of HSCT
Autologous HSCT supports the recovery of hematopoiesis in patients with ADs after intense immunosuppressive conditioning. Although the immunosuppressive conditioning aims at lymphodepletion rather than at myelosuppression (in contrast to HSCT for leukemia), transient bone marrow aplasia occurs and a significant proportion of patients develop fever and bacterial infections after HSCT. Moreover, infections were the leading cause of mortality in the latest analysis of the Promise database (1).
In this unique population, pre-existing organ damage due to AD (e.g., pulmonary fibrosis in SSc) may predispose patients to infections after HSCT. Patients with ADs who are eligible for HSCT have often received several lines of immunosuppressive therapies before HSCT, and some ADs are per se accompanied by defects of the immune system (e.g., SLE and complement deficiencies) (8). These factors contribute to the risk of infection after HSCT.
Antithymocyte globulins (ATG) for conditioning and ex vivo selection procedures such as CD34-positive selection of the graft, both often applied in HSCT for patients with ADs, induce severe and lasting immune suppression by enhancing lymphodepletion. The re-emergence of a functional and diverse adaptive immune system can be thus delayed up to years after HSCT (9). Autologous HSCT-induced lymphopenia can be as profound and lasting as in the setting of allogeneic HSCT. In the case of lymphopenia, patients are at risk for reactivation of endogenous viruses and for the occurrence of opportunistic infections. Nash et al. reported on 2 of 56 patients who died from Epstein–Barr virus (EBV)–associated lymphoma after HSCT for ADs. Both received rabbit ATG for conditioning, and lymphocytes in peripheral blood were absent on d +28 after HSCT (10).
In an analysis of 22 juvenile idiopathic arthritis patients who received HSCT, 9 patients developed Varicella zoster virus infection between 1 and 12 mo after HSCT, 4 patients experienced cytomegalovirus (CMV) reactivation, and 1 patient had CMV primoinfection. Two patients died after having developed macrophage activation syndrome, which was related in 1 patient to an EBV infection and in the other patient to a bacterial infection. The conditioning for these patients included ATG and low-dose total body irradiation (11).
EBV-triggered hemophagocytosis may develop after autologous HSCT, even in the absence of lymphocytes in peripheral blood, as has been shown by one patient transplanted for mixed connective tissue disease (12). T-cell responses directed against EBV-derived antigens remain relatively stable during even intense immune suppression (13). Small changes in the conditioning regimen toward a slightly more intense T-cell depletion may therefore rather dramatically increase the risk of loss of control of endogenous herpes viruses. One such procedure is CD 34+ graft selection, which has been proposed to be associated with an increased risk of viral reactivation after HSCT for hematological indications (14). A high rate of virus infections has also been shown among 14 patients who underwent autologous HSCT for severe AD with CD34+ selection of the graft. CMV reactivation was observed in 64% patients and 50% of patients developed a (late) Varicella zoster virus infection (15). Patients with CMV reactivation were pre-emptively treated with gancyclovir and none developed CMV disease. Taken together, lymphodepleting conditioning and CD34+ selection of the graft in the treatment of patients with ADs increase the risk for opportunistic infections; among those, infections with viruses of the herpes family are most often reported. Screening for EBV and CMV replication and careful examination for signs or symptoms of virus-associated disease after HSCT is therefore strongly recommended.
Intense immune suppression (i.e., lymphodepletion) may also impact memory immune responses against vaccines. In an immunological long-term follow-up examination of autologous transplanted SLE patients, significant decreases in protective serum antibody levels for measles, mumps, tetanus toxoid, and diphtheria were observed when tested 1 or 2 years after HSCT (9). Thus, protective long-lived plasma cells in the bone marrow may be deleted by conditioning and patients may be at increased risk of infection, albeit having received vaccination in the past.
Treatment-Associated Toxicity
Toxicity of HSCT depends on conditioning (agents and doses) and on patients’ health before HSCT. The high morbidity and mortality reported in the initial publications on HSCT for ADs have been attributed to the inclusion of patients with advanced diseases with significant organ damage caused by the autoimmune disease. These patients are at an increased risk for developing more severe conditioning-induced complications.
Cardiac Toxicity
Most conditioning regimens contain cyclophosphamide (Cy) and high-dose Cy have been associated with acute cardiotoxicity in the past (16). Cy is assumed to damage endothelium, leading to local inflammation within the myocard. There seems to be a direct correlation between the area under the curve of Cy and cardiotoxicity, whereas the cumulative cardiotoxicity is negligible. With fractionation of Cy doses, cardiotoxicity could be reduced.
Heart involvement is common in patients with severe ADs. In patients with SSc, cardiovascular manifestations are the leading cause of death (17). In SLE, occlusive cardiovascular disease can be present even in young patients (18). Recent data suggest that the incidence of clinically silent heart involvement in these diseases is high (19). Cardiac deaths in patients with SSc associated with HSCT have been reported, which raises the question of whether cardiac toxicity of Cy is related to pre-existing heart disease. Therefore, careful heart examinations including ultrasound and 24-h electrocardiogram (ECG) are performed before HSCT. Dose adaption or substitution of Cy for conditioning in the case of cardiac involvement or implantation of an implantable cardioverter defibrillator in case of ventricular arrhythmias must be considered before HSCT. Close monitoring of these patients during and after HSCT has been recommended (20).
Renal Toxicity
HSCT is associated with significant renal toxicity. This is known for children after autologous HSCT for hematological malignancies, where up to 50% of patients developed renal impairment. Presumably, the use of calcineurin inhibitors and the occurrence of graft-vs.-host disease contribute to the higher incidence of renal impairment after allogeneic HSCT in the same study. Moreover, worsening of renal function after HSCT was associated with mortality (21). Among patients with ADs, those suffering from SSc are at an increased risk for developing renal injury after HSCT. This has been shown by an analysis of 3 US cohorts of 91 patients with SSc who underwent HSCT. Eleven of those developed renal impairment after HSCT. The etiology of renal disease was attributed to scleroderma renal crisis in 6 patients and pre-existing SSc renal disease in 3 patients, and it was uncertain in 2 patients. Eight of the 11 patients died from different causes (22). Angiotensin-converting enzyme inhibitor therapy was given for 10 of 11 patients. Fluid overload, insufficient blood pressure control, toxicity of medication, and irradiation given during HSCT may contribute to this effect.
Toxicity Associated With ATG Administration
ATG consists of polyclonal xenogenic antibodies directed against lymphoid cells. The administration of ATG may therefore cause serious allergic reactions. Premedication with steroids prior to ATG administration is therefore mandatory. With a delay of generally more than 10 d serum sickness, an immune-complex-mediated syndrome has been reported to occur after ATG administration. The disease is a type III hypersensitivity reaction mediated by deposits of circulating immune complexes in small vessels, leading to complement activation and subsequent inflammation. Symptoms are fever, cutaneous eruptions, lymphadenopathy, arthralgias, albuminuria, and nephritis. Serum sickness is an acute self-limited disease (23). More rarely, serum sickness may lead to acute renal failure (24). Other side effects of ATG are induction of intravascular coagulation, hypotension, and liver dysfunction. In a cohort of adult patients who received allogeneic HSCT for different indications, side effects were less frequent if ATG was given over 12 h instead of 4 h and if accompanied by higher doses of steroids (25). ATG has been reported to be associated with an acute respiratory distress syndrome (26).
Granulocyte Colony-Stimulating Factor–Associated Side Effects
Granulocyte colony-stimulating factor (G-CSF) is used for mobilization of hematopoietic stem cells from the bone marrow into peripheral blood. This allows for the collection of stem cells for retransfusion after conditioning. Usually, mobilization is preceded and facilitated by chemotherapy (e.g., Cy). G-CSF administration has been associated with induction of flares of the underlying autoimmune disease) (27,28).
In patients with lung disease and/or lung inflammation, G-CSF may cause an acute respiratory distress syndrome (29) mediated by neutrophils that, following G-CSF administration, migrate in a large numbers into the lung and augment inflammation. Patients with SSc or SLE and lung involvement may be thus at risk for developing pulmonary symptoms after G-CSF given for mobilization.
Secondary ADs Occurring After HSCT
HSCT fundamentally interferes with the immune system. Lymphodepletion is followed by de novo development of T and B cells. As an intended effect, HSCT potentially leads to the re-establishment of tolerance and hence the abrogation of autoimmunity. This can be achieved by restoration of central tolerance or by restoration of peripheral regulatory elements (e.g., regulatory cells). These processes are complex and only partly understood. In the first post-HSCT phase, remaining or transplanted lymphocytes expand in the host in the presence of an excess of growth factors (homeostatic expansion) (30). Later, naive lymphocytes with a broader receptor repertoire emerge. During the whole process, autoreactive clones may escape control and trigger de novo autoimmunity as an unintended effect of HSCT.
Indeed, several types of ADs were observed after both autologous and allogeneic HSCT for different indications (31). Published data stem from isolated case reports or from single-center series of patients with new onset of ADs after HSCT for different diseases. Most frequently, antibody-associated organ-specific ADs such as thyroiditis (32), immune thrombocytopenia, autoimmune hemolytic anemia (33), or myasthenia gravis have been reported (34). In a single-center North American retrospective study (35), 6 of 155 patients with various ADs developed a secondary AD after autologous HSCT, partly related to intense T-cell depletion during conditioning with ATG or alemtuzumab (CD-52 antibodies). Two other cases of SSc patients were studied after HSCT for secondary onset of immune thrombocytopenia, followed by Graves’ disease and SLE with antiphospholipid syndrome in the first one (36) and myasthenia gravis in the other (37).
Because secondary ADs may occur after HSCT for a primary AD, identification of the risk factors is important to improve patient care and may influence outcome after HSCT. We thus recently analyzed the incidence and risk factors for the development of a secondary AD after HSCT in 363 patients reported to Promise (38). Among 363 primary AD patients included from 28 centers in 12 European countries, 32 developed at least one secondary AD after HSCT. The cumulative incidence of secondary AD after HSCT for ADs was 9.8% (±2%) after 5 y. Diagnoses were autoimmune hemolytic anemia (n = 3), acquired hemophilia (n = 3), autoimmune thrombocytopenia (n = 3), antiphospholipid syndrome (n = 2), thyroiditis (n = 10), blocking TSH receptor antibody–associated hypothyroidism (n = 1), Graves’ disease (n = 2), myasthenia gravis (n = 1), rheumatoid arthritis (n = 2), sarcoidosis (n = 2), and psoriasis (n = 1). In this cohort, risk factors for the development of secondary ADs were SLE as primary AD and conditioning with ATG plus CD34+ graft selection. This study and previous single-center case series (39) also suggest that secondary ADs occur more often in younger patients after HSCT. Two patients died of their secondary AD (acquired factor VIII inhibitor, antiphospholipide syndrome). Thus, patients with SLE, younger age at HSCT, or those receiving severe T-cell-depleting conditioning (ATG, alemtuzumab, CD34+ selection) need close monitoring for secondary ADs after autologous HSCT.
Endocrinological Late Effects
Regimen-related infertility may occur after high-dose Cy. Ovarian function after high-dose Cy depends on Cy dose and age of the patient (the younger the patient, the higher the chance to preserve ovarian function). An analysis of 212 patients undergoing allogeneic HSCT for aplastic anemia treated with 200 mg/kg of Cy (the same dose used in HSCT for AD) and ATG showed that at 20 years after HSCT, the probability that a female patient would become pregnant was 47% and the probability that a male patient had fathered a child was 62% of patients among those who did not develop graft-vs.-host disease (40). This analysis did not document what percentage of patients did not wish to get pregnant or to father children. Therefore, it could be speculated that the actual fertility rate is even higher than reported in this cohort. In contrast, total body irradiation used for conditioning induces ovarian failure in nearly all patients (41). Gonadal toxicity accumulates over time; therefore, pretreatment of patients with ADs (e.g., with Cy) must be taken into account.
Younger patients undergoing HSCT should therefore be counseled both before and after HSCT about potential loss of fertility and planning for future pregnancy. Fertility and outcomes of pregnancy after HCT require prospective evaluation.
Allogeneic HSCT in children has been shown to impact growth and thyroid function. Irradiation, the use of busulfan, and graft-vs.-host disease are thought to be associated with growth retardation and hypothyroidism after HSCT (42). In contrast, conditioning for autologous HSCT for patients with ADs uses lower doses of total body irradiation or irradiation-free protocols (43). Growth of children with severe ADs can be delayed through chronic inflammation and through the constant use of steroids. Steroid-free remission of autoimmune disease after HSCT may therefore promote growth catch-up in children (44). Secondary autoimmune thyroiditis occurs after autologous HSCT, especially in severe lymphodepleted patients, and may lead to hypothyroidism.
Malignancies After HSCT
Conditioning for HSCT, pretreatment with alkylating substances, and the AD itself may contribute to an increased risk for the development of malignancies after HSCT in these patients. Cy and irradiation used for conditioning are both known to induce malignancies in a dose-dependent manner. Cy has been associated with bladder carcinoma (45) and the development of hematological malignancies (46). In an analysis of 700 patients with severe aplastic anemia treated with allogeneic marrow transplantation, 23 developed a malignancy 1.4 to 221 mo (median, 91 mo) after transplantation. Five cases were lymphoid malignancies occurring 1.4 to 14.6 mo (median, 3 mo) after transplantation, and 18 were solid tumors presenting 30 to 221 mo (median, 99 mo) after transplantation. Radiation was identified as significant risk factor for the development of a malignancy (47). Similar conditioning protocols have been used in patients with ADs, albeit before autologous HSCT. However, it must be considered that patients with ADs differ from patients with hematological and malignant diseases undergoing HSCT, not only with respect to diagnosis but also with respect to pretreatment before HSCT. In the latest review of the Promise database, 5 of 900 patients who received HSCT for an AD developed a malignancy after transplantation. Diagnoses were acute myeloid leukemia (MS), bronchial carcinoma (SSc), esophageal carcinoma (SSc), refractory anemia with excess of blasts (SLE), and posttransplant lymphoproliferative disease (mixed connective tissue disease) (1). Longer follow-up in prospective trials is needed to identify patients with ADs who are at increased risk for malignancy after HSCT. Regular urine examinations may help to early detect Cy-induced bladder carcinoma.
Outlook
The past 15 years have seen a substantial increase in knowledge of the risks and complications of autologous HSCT for the treatment of patients with severe ADs. Patients, their diseases, and their disease manifestations are heterogeneous. Conditioning aims toward lymphodepletion. This leads to specific and new problems, partly different from what has been described in patients who received HSCT for malignant diseases. Consequently, opportunistic infections and an increased incidence of secondary ADs have been observed. Toxicity of the conditioning regimen depends on patient disease manifestations and thus must be adapted for patients with organ dysfunction. This has been constantly done (e.g., adaption of irradiation protocols to reduce the dose applied to the lungs and kidneys in patients with renal or lung involvement of their ADs) (48).
Critical in respect to outcome after HSCT is the process of patient selection. We have learned that patients with advanced, presumably irreversible, organ damage are at increased risk of developing serious complications following HSCT. It is therefore essential to select those patients for HSCT who suffer from a severe life- or organ-threatening AD, have a poor prognosis, have no advanced organ damage, and do not respond to an established therapy. Figure 1 summarizes factors influencing on complications after HSCT for ADs.

Patient selection criteria, treatment, and procedures and their potential impact on post–hematopoietic stem cell transplantation (HSCT) complications. ATG, antithymocyte globulin; TBI, total body irradiation.
It is possible that with increasing experience with HSCT for patients with ADs, new complications may become apparent. Therefore, all patients should, whenever possible, be treated within prospective protocols looking for side effects. Careful evaluation of organ function before HSCT is advised; after HSCT, follow-up examinations must be adapted to the patient and to the type of conditioning in a standardized form. Results from ongoing phase III studies will help to gain further insights in complications after HSCT and may help to identify patients at risk.
References
Farge D, Labopin M, Tyndall A, et al. Autologous hematopoietic stem cell transplantation for autoimmune diseases: an observational study on 12 years’ experience from the European Group for Blood and Marrow Transplantation Working Party on Autoimmune Diseases. Haematologica 2010;95:284–92.
Milanetti F, Abinun M, Voltarelli JC, Burt RK . Autologous hematopoietic stem cell transplantation for childhood autoimmune disease. Pediatr Clin North Am 2010;57:239–71.
Daikeler T, Hügle T, Farge D, et al.; Working Party Autoimmune Diseases of the EBMT. Allogeneic hematopoietic SCT for patients with autoimmune diseases. Bone Marrow Transplant 2009;44:27–33.
Sykes M, Nikolic B . Treatment of severe autoimmune disease by stem-cell transplantation. Nature 2005;435:620–7.
Fransen J, Popa-Diaconu D, Hesselstrand R, et al. Clinical prediction of 5-year survival in systemic sclerosis: validation of a simple prognostic model in EUSTAR centres. Ann Rheum Dis 2011;70:1788–92.
McSweeney PA, Nash RA, Sullivan KM, et al. High-dose immunosuppressive therapy for severe systemic sclerosis: initial outcomes. Blood 2002;100:1602–10.
Farge D, Passweg J, van Laar JM, et al.; EBMT/EULAR Registry. Autologous stem cell transplantation in the treatment of systemic sclerosis: report from the EBMT/EULAR Registry. Ann Rheum Dis 2004;63:974–81.
Jesus AA, Liphaus BL, Silva CA, et al. Complement and antibody primary immunodeficiency in juvenile systemic lupus erythematosus patients. Lupus 2011;20:1275–84.
Alexander T, Thiel A, Rosen O, et al. Depletion of autoreactive immunologic memory followed by autologous hematopoietic stem cell transplantation in patients with refractory SLE induces long-term remission through de novo generation of a juvenile and tolerant immune system. Blood 2009;113:214–23.
Nash RA, Dansey R, Storek J, et al. Epstein-Barr virus-associated posttransplantation lymphoproliferative disorder after high-dose immunosuppressive therapy and autologous CD34-selected hematopoietic stem cell transplantation for severe autoimmune diseases. Biol Blood Marrow Transplant 2003;9:583–91.
Brinkman DM, de Kleer IM, ten Cate R, et al. Autologous stem cell transplantation in children with severe progressive systemic or polyarticular juvenile idiopathic arthritis: long-term follow-up of a prospective clinical trial. Arthritis Rheum 2007;56:2410–21.
Daikeler T, Tzankov A, Hoenger G, et al. Minimal T-cell requirements for triggering haemophagocytosis associated with Epstein-Barr virus-driven B-cell proliferation: a clinical case study. Ann Rheum Dis 2011;70:1338–9.
Daikeler T, Hoenger G, Oehri I, et al. Dominant Epstein-Barr virus-specific T-cell responses are maintained during moderate and intense immunosuppressive treatment. Ann Rheum Dis 2011;70:395–6.
Holmberg LA, Boeckh M, Hooper H, et al. Increased incidence of cytomegalovirus disease after autologous CD34-selected peripheral blood stem cell transplantation. Blood 1999;94:4029–35.
Kohno K, Nagafuji K, Tsukamoto H, et al. Infectious complications in patients receiving autologous CD34-selected hematopoietic stem cell transplantation for severe autoimmune diseases. Transpl Infect Dis 2009;11:318–23.
Morandi P, Ruffini PA, Benvenuto GM, Raimondi R, Fosser V . Cardiac toxicity of high-dose chemotherapy. Bone Marrow Transplant 2005;35:323–34.
Tyndall AJ, Bannert B, Vonk M, et al. Causes and risk factors for death in systemic sclerosis: a study from the EULAR Scleroderma Trials and Research (EUSTAR) database. Ann Rheum Dis 2010;69:1809–15.
Korkmaz C, Cansu DU, Kasifoglu T . Myocardial infarction in young patients (< or =35 years of age) with systemic lupus erythematosus: a case report and clinical analysis of the literature. Lupus 2007;16:289–97.
Kobayashi H, Yokoe I, Hirano M, et al. Cardiac magnetic resonance imaging with pharmacological stress perfusion and delayed enhancement in asymptomatic patients with systemic sclerosis. J Rheumatol 2009;36:106–12.
Saccardi R, Tyndall A, Coghlan G, et al. Consensus statement concerning cardiotoxicity occurring during haematopoietic stem cell transplantation in the treatment of autoimmune diseases, with special reference to systemic sclerosis and multiple sclerosis. Bone Marrow Transplant 2004;34:877–81.
Caliskan Y, Besisik SK, Sargin D, Ecder T . Early renal injury after myeloablative allogeneic and autologous hematopoietic cell transplantation. Bone Marrow Transplant 2006;38:141–7.
Hosing C, Nash R, McSweeney P, et al. Acute kidney injury in patients with systemic sclerosis participating in hematopoietic cell transplantation trials in the United States. Biol Blood Marrow Transplant 2011;17:674–81.
Chao YK, Shyur SD, Wu CY, Wang CY . Childhood serum sickness: a case report. J Microbiol Immunol Infect 2001;34:220–3.
da Silva PS, Passos RM, Waisberg DR, Park MV . Serum sickness and severe acute renal failure after rabbit antithymocyte globulin treatment in aplastic anemia: a case report. J Pediatr Hematol Oncol 2011;33:43–6.
Pihusch R, Holler E, Mühlbayer D, et al. The impact of antithymocyte globulin on short-term toxicity after allogeneic stem cell transplantation. Bone Marrow Transplant 2002;30:347–54.
Goligher EC, Cserti-Gazdewich C, Balter M, Gupta V, Brandwein JE . Acute lung injury during antithymocyte globulin therapy for aplastic anemia. Can Respir J 2009;16:e3–5.
Snowden JA, Biggs JC, Milliken ST, et al. A randomised, blinded, placebo-controlled, dose escalation study of the tolerability and efficacy of filgrastim for haemopoietic stem cell mobilisation in patients with severe active rheumatoid arthritis. Bone Marrow Transplant 1998;22:1035–41.
Nash RA, Bowen JD, McSweeney PA, et al. High-dose immunosuppressive therapy and autologous peripheral blood stem cell transplantation for severe multiple sclerosis. Blood 2003;102:2364–72.
Karlin L, Darmon M, Thiéry G, et al. Respiratory status deterioration during G-CSF-induced neutropenia recovery. Bone Marrow Transplant 2005;36:245–50.
King C, Ilic A, Koelsch K, Sarvetnick N . Homeostatic expansion of T cells during immune insufficiency generates autoimmunity. Cell 2004;117:265–77.
Daikeler T, Tyndall A . Autoimmunity following haematopoietic stem-cell transplantation. Best Pract Res Clin Haematol 2007;20:349–60.
Carlson K, Lönnerholm G, Smedmyr B, Oberg G, Simonsson B . Thyroid function after autologous bone marrow transplantation. Bone Marrow Transplant 1992;10:123–7.
Sanz J, Arriaga F, Montesinos P, et al. Autoimmune hemolytic anemia following allogeneic hematopoietic stem cell transplantation in adult patients. Bone Marrow Transplant 2007;39:555–61.
Mackey JR, Desai S, Larratt L, Cwik V, Nabholtz JM . Myasthenia gravis in association with allogeneic bone marrow transplantation: clinical observations, therapeutic implications and review of literature. Bone Marrow Transplant 1997;19:939–42.
Loh Y, Oyama Y, Statkute L, et al. Development of a secondary autoimmune disorder after hematopoietic stem cell transplantation for autoimmune diseases: role of conditioning regimen used. Blood 2007;109:2643–548.
Bohgaki T, Atsumi T, Koike T . Multiple autoimmune diseases after autologous stem-cell transplantation. N Engl J Med 2007;357:2734–6.
Deligny C, Clave E, Sibon D, et al. New onset of myasthenia gravis after treatment of systemic sclerosis by autologous hematopoietic stem cell transplantation: sustained autoimmunity or inadequate reset of tolerance? Hum Immunol 2010;71:363–5.
Daikeler T, Labopin M, Di Gioia M, et al.; EBMT Autoimmune Disease Working Party. Secondary autoimmune diseases occurring after HSCT for an autoimmune disease: a retrospective study of the EBMT Autoimmune Disease Working Party. Blood 2011;118:1693–8.
Page KM, Mendizabal AM, Prasad VK, et al. Posttransplant autoimmune hemolytic anemia and other autoimmune cytopenias are increased in very young infants undergoing unrelated donor umbilical cord blood transplantation. Biol Blood Marrow Transplant 2008;14:1108–17.
Deeg HJ, Leisenring W, Storb R, et al. Long-term outcome after marrow transplantation for severe aplastic anemia. Blood 1998;91:3637–45.
Sanders JE, Buckner CD, Amos D, et al. Ovarian function following marrow transplantation for aplastic anemia or leukemia. J Clin Oncol 1988;6:813–8.
Sanders JE, Woolfrey AE, Carpenter PA, et al. Late effects among pediatric patients followed for nearly 4 decades after transplantation for severe aplastic anemia. Blood 2011;118:1421–8.
De Kleer IM, Brinkman DM, Ferster A, et al. Autologous stem cell transplantation for refractory juvenile idiopathic arthritis: analysis of clinical effects, mortality, and transplant related morbidity. Ann Rheum Dis 2004;63:1318–26.
Abinun M, Flood TJ, Cant AJ, et al. Autologous T cell depleted haematopoietic stem cell transplantation in children with severe juvenile idiopathic arthritis in the UK (2000-2007). Mol Immunol 2009;47:46–51.
Talar-Williams C, Hijazi YM, Walther MM, et al. Cyclophosphamide-induced cystitis and bladder cancer in patients with Wegener granulomatosis. Ann Intern Med 1996;124:477–84.
Faurschou M, Sorensen IJ, Mellemkjaer L, et al. Malignancies in Wegener’s granulomatosis: incidence and relation to cyclophosphamide therapy in a cohort of 293 patients. J Rheumatol 2008;35:100–5.
Deeg HJ, Socié G, Schoch G, et al. Malignancies after marrow transplantation for aplastic anemia and fanconi anemia: a joint Seattle and Paris analysis of results in 700 patients. Blood 1996;87:386–92.
Craciunescu OI, Steffey BA, Kelsey CR, et al. Renal shielding and dosimetry for patients with severe systemic sclerosis receiving immunoablation with total body irradiation in the scleroderma: cyclophosphamide or transplantation trial. Int J Radiat Oncol Biol Phys 2011;79:1248–55.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Daikeler, T., Tichelli, A. & Passweg, J. Complications of autologous hematopoietic stem cell transplantation for patients with autoimmune diseases. Pediatr Res 71, 439–444 (2012). https://doi.org/10.1038/pr.2011.57
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/pr.2011.57
This article is cited by
-
Effect of Hematopoietic Stem Cell Transplantation and Post-Transplantation Cyclophosphamide on the Microglia Phenotype in Rats with Experimental Allergic Encephalomyelitis
Archivum Immunologiae et Therapiae Experimentalis (2023)
-
The current standing of autologous haematopoietic stem cell transplantation for the treatment of multiple sclerosis
Journal of Neurology (2022)
-
Autologe hämatopoetische Stammzelltransplantation bei systemischer Sklerose
rheuma plus (2021)
-
In-patient outcomes of Hematopoietic Stem Cell Transplantation in Patients with Immune Mediated Inflammatory Diseases: A Nationwide Study
Scientific Reports (2018)
-
Low toxicity and favorable clinical and quality of life impact after non-myeloablative autologous hematopoietic stem cell transplant in Crohn’s disease
BMC Research Notes (2017)
