
Abstract
Study design:
Literature review.
Objectives:
To map traumatic spinal cord injury (TSCI) globally and provide a framework for an ongoing repository of data for prevention.
Setting:
An initiative of the ISCoS Prevention Committee.
Methods:
The results obtained from the search of Medline/Embase using search phrases: TSCI incidence, aetiology, prevalence and survival were analysed. Stratification of data into green/yellow/red quality ‘zones’ allowed comparison between data.
Results:
Reported global prevalence of TSCI is insufficient (236–1009 per million). Incidence data was comparable only for regions in North America (39 per million), Western Europe (15 per million) and Australia (16 per million). The major cause of TSCI in these regions involves four-wheeled motor vehicles, in contrast to South-east Asia where two-wheeled (and non-standard) road transport predominates. Southern Asia and Oceania have falls from rooftops and trees as the primary cause. High-fall rates are also seen in developed regions with aged populations (Japan/Western Europe). Violence/self-harm (mainly firearm-related) was higher in North America (15%) than either Western Europe (6%) or Australia (2%). Sub-Saharan Africa has the highest reported violence-related TSCI in the world (38%). Rates are also high in north Africa/Middle East (24%) and Latin America (22%). Developed countries have significantly improved TSCI survival compared with developing countries, particularly for tetraplegia. Developing countries have the highest 1-year mortality rates and in some countries in sub-Saharan Africa the occurrence of a spinal injury is likely to be a fatal condition within a year.
Conclusion:
Missing prevalence and insufficient incidence data is a recurrent feature of this review. The piecemeal approach to epidemiological reporting of TSCI, particularly failing to include sound regional denominators has exhausted its utility. Minimum data collection standards are required.
Similar content being viewed by others


Introduction
The last prior international comparisons of the literature was performed in 2004 by Ackery et al.1 and in 2006 by Wyndaele2 and this review builds on that body of work, updating it to the present day and adding a review of aetiology where available.
Our ability to review and analyse large quantities of data is influenced by the format in which those data are presented—in text format, in the form of tables of data or in graphical formats. Mackay3 and Rosling (http://www.gapminder.org/) have shown the value of enhanced mapping techniques in the portrayal of health data of national and international significance. We believe that these techniques can be employed usefully in directing our prevention efforts, ensuring that they are appropriate to each region or country. This report suggests a data repository structure, which allows for simple conversion to a graphical, easily interpretable map of global trends in spinal cord injury (SCI), which can be easily updated and published as a living document through the ISCoS website. As such, it will be open for future contributions of published and unpublished data.
This project is part of a worldwide SCI mapping project, which is being undertaken by the Prevention Committee of ISCoS and aims to:
-
1
Inform the ISCoS Prevention Committee for coordination of future prevention strategies.
-
2
Provide data to stakeholders seeking information to support injury prevention (specifically to inform regional or national SCI prevention programs).
-
3
Provide a platform for development of specific tools to facilitate injury prevention and encourage uniformity of data collection.
-
4
Create partnerships within ISCoS to facilitate development of strategies for primary and secondary prevention of SCI.
-
5
Provide the structure for an ongoing data repository.
It is intended that this work continue as an ongoing review, which will be open to contributions of published and unpublished data to assist the ISCoS Prevention Committee and other organisations in the task of SCI prevention.
Materials and methods
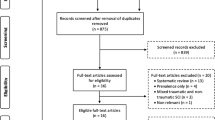
The literature search of Wyndaele2 was repeated without date or language restriction using search phrases (exploded): ‘Epidemiology of SCI’, ‘Prevalence of SCI’, ‘Incidence of SCI’ through Medline and Embase. This search yielded 1872 articles. These articles and abstracts were screened and added to our reference library. Reference lists of global incidence of Wyndaele2 and Ackery et al.,1 the prevalence article by Blumer and Quine4 and the articles about non-traumatic SCI from New and Sundararajan5 were also reviewed as well as conference proceedings. A review of available SCI mortality data was also conducted.
World Health Organisation (WHO) regions were used for analysis so that countries, which are epidemiologically similar to others in the region, could be compared. The regions and the countries within were chosen using mortality estimates from the WHO and the United Nations and other country-specific factors such as income and number of hospitals.6
The authors decided on the most representative study for each country by reviewing the methodology, population covered and the time period of data collection. Preference was given to the more recent studies, which provided national statistics and aetiological data. Median data values were calculated for multiple studies of individual countries and global regions.
Information used in constructing global regions and country maps was divided into three broad categories to allow comparison between information of variable quality (Box 1).
Maps using SCI incidence and aetiological data were developed for WHO regions and countries within these regions using mapping and graphical techniques developed by Myriad Editions (http://www.myriadeditions.com/health) (Figures 1 and 2).

Global mapping of spinal cord injury from traumatic causes by WHO regions 1959–2008.

Global mapping of spinal cord injury from traumatic causes by country 1959–2008.
Results
A total of 377 records were reviewed after a screen of abstracts. Two unpublished additional data sources were received (Vietnam and Saudi Arabia) and conference proceedings data from two countries were also included (western Norway, Iceland).
Green or yellow zone data was only available for North America (USA and Canada), Australia and Western Europe (Denmark, Greenland, Iceland, Sweden, Ireland and Germany).
Discussion
In a 2004 epidemiological review of SCI, Ackery and colleagues noted the need for standardised reporting of SCI, as did Wyndaele in a 2006 review. Ackery et al. noted that countries with similar economies tended to have similar injury patterns; Wyndaele also observed the need for improved registration, whereas Ackery suggested that a role existed for the involvement of international organisations in injury prevention of SCI: we echo these opinions and suggest minimal standards and a possible mechanism for reporting. At a minimum, traumatic and nontraumatic SCI statistics should be separately reported and the current International Standards data sets should be employed.1, 2, 7
Most clinicians are aware of the need to report their local statistics for incidence and prevalence of SCI, but may lack the tools or financial resources to undertake this task. Failure to refer patients with SCI to a specialised centre makes this task more difficult unless national or regional reporting is routinely occurring using internationally accepted data standards through an injury registry. The absence of national reporting, illustrated by the many ‘red-zone’ areas in the global maps makes it difficult to determine valid population denominators and even small area variation, helpful in determining prevention strategies.
Prevalence of SCI globally
Insufficient data exist to derive a global prevalence for SCI. Detailed prevalence data are summarised in Table 1. The range of reported global prevalence is between 236 and 1009 per million. Missing prevalence data for major populations is stark. Asian countries, particularly China and India are not appropriately represented, with available Asian statistics likely underestimating the overall prevalence within this populous region. No published data exists for Africa or South America. The differing methodologies used to derive prevalence statistics has previously been observed by Wyndaele.2 Global and country-specific prevalence data comparisons should be made with caution because of different methods of derivation, dates of publication and other factors such as mortality rates.
Asia, South and South-East
Prevalence data only exists for the Kashmir region in India8 and Vietnam,9 with a prevalence of between 236–464 per million traumatic SCI.
Australasia
Prevalence data, available only for Australia, ranges between 370 in 1987 and 681 per million in 1998.10, 11, 12
Western Europe
Two countries only have reported prevalence data: Finland 280 per million13 and Iceland 316 per million.14
North America, high income
USA (721–1009 per million, with a median of approximately 853 per million).15, 16, 17, 18, 19
Canadian data is estimated at approximately 1173 per million (assuming a population of 30.7 million).20
Incidence of traumatic SCI globally
The most representative incidence statistic for each country within WHO regions is presented (http://iscos.org.uk/page.php?content=57, Table 2) along with aetiology data where possible. Trends and statistical outliers in aetiology within a region are identified. Unfortunately the lack of standardised reporting of aetiology data reduces the ability of this data to contribute to specific injury prevention strategies or hypotheses. Increasing familiarity with and adherence to the International Classification of the External Cause of Injury (ICECI) should increase our understanding of injury patterns and our ability to reduce the incidence of traumatic SCI (and other injuries).
Incidence data was interpretable only for the green and yellow zone regions of north America, Western Europe and Australia. North America (39 per million) had more than twice the incidence of Australia (15 per million) and Western Europe (16 per million) The major cause of SCI in these regions is road traffic accidents primarily four-wheeled motor vehicles. Violence/self-harm was higher in North America (15% of which almost all were firearm-related injuries) than either Western Europe (6%) or Australia (2%). Western Europe had the highest rate of falls (37%) followed by Australia and North America (29 and 20%, respectively). This may be related to Western Europe having a comparatively older population than both Australia and North America (population >60 years: 23.9, 18.9 and 18%, respectively).21 Mortality rates after SCI across these regions were low. Median values were calculated from information contained in http://www.iscos.org.uk/ (Table 2) and http://www.iscos.org.uk/ (Table 3).
Red zone incidence data, although presented in the tables, are not analysed or interpreted as comparisons between regions and countries would be misleading.
Asia Pacific, high income
Japan, on the basis of a nation-wide survey, had an incident rate of 40.2 per million.22 Japanese studies by Shingu22 and Ide23 had higher rates of tetraplegia than experienced in other countries, possibly because of reporting bias, to high-quality emergency retrieval and health care. A higher than usual proportion of falls (42%) is probably related to an aged population at time of injury, given Japan has an extremely aged population with 29.7% of people being aged 60 years or over, based on 2009 statistics. Overall, one-third of falls were on level ground. After the age of 50 years, high falls declined and falls on level ground continued to increase.22, 21
Asia, East
Taiwan had an incident rate of 18.8 per million (70% of possible SCI cases from centres throughout Taiwan).24 Land transport accounted for 49% of SCI in the general population. The incidence of SCI was higher in geriatric (age greater than 65) population (47.5 per million) with a higher proportion of tetraplegic patients in this group. Within the geriatric population, 62% of the SCI were as a result of falls. Chen25 provided the only recent aetiology data.
There were no published incidence data for mainland China.
Asia, South
Land transport-related SCI is reported to be much lower than European countries; falls predominate within southern Asia. The highest percentage of falls was in Pakistan 82%, particularly off trees and rooftops.26 Data from Bangladesh also had high number of falls (63%), out of which 43% of the falls involved falls from trees and 20% while carrying heavy loads.27 Mukhida28 provided statistics for people in Nepal under the age of 19, in which 61% of SCI was due to falls (mainly from rooftops as opposed to trees in the rest of the region).
Incidence data are inadequate for this region.
Asia, South-east
Vietnam: unpublished calculated incidence data from Weerts9 underestimates the actual incidence because of the lack of a national data registry. In Vietnam and Thailand (Weerts,9 Kovindha,29 and Parajareya30), transport caused about 47% of reported cases of SCI and the largest proportion of transport-related accidents were due to motorcycles (which includes non-standard transport types such as Jitneys). Factors contributing to the high rates of motorcycle accidents are: motorcycles are the major mode of transportation, they transport heavy loads, have multiple passengers (often more than two people) and travel on poor road infrastructure.
Australasia
The aetiological causes were similar in both Australia and New Zealand,31, 32 with the highest land transport-related SCI due to motor vehicles (predominantly four or more wheels) in Australia and in New Zealand. Sports/recreational injuries were about 3% greater, proportionally, in New Zealand. In New Zealand, rugby was responsible for 8% of the sports-related injuries. In both countries, falls accounted for about one-quarter to one-third of SCI cases. Incidence data was not compared, as the published New Zealand Statistics did not come from a national spinal or population register.
Europe, Central
Regional data was only available for Poland (Poznan)33 and Romania (Bucharest).34 The reference article for Central Europe is Romania, which extrapolates the SCI incidence of Bucharest to the entire population of Romania (red zone data). The main aetiology of SCI in Poland and Romania is transportation. There was a high proportion of falls from carts in Romania. Both Poland and Romania are among the top six (EU25, European) countries with the highest standardised death rate for transport-related mortality (Belanger).35
Europe, Eastern
Estonian data and regional data for Russia were only available.36, 37, 38 The main aetiology of SCI in Estonia and Russia (Novosibirski and Saint Petersburg) were falls (median 40%) and land transport (median 25%).
Europe, Western
From the most recent data from countries with national statistics: Denmark (9.2 per million), Finland (13.8 per million), France 19.4 per million, Germany 10.7 per million, Greece 33.6 per million, Greenland 26 per million, Iceland 20 per million, Ireland 13.1 per million, Italy 19 per million, Israel 15.9 per million, Netherlands 7.5 per million, Norway 4.5 per million, Spain 8.1 per million, Switzerland 15 per million The median for the Western Europe region is 14.4 per million. (median values were calculated from information contained in http://www.iscos.org.uk/, Table 2.)
Transport injuries were mostly in a similar order throughout the Western European countries.
Where identified, these are mostly motor vehicle, four-wheeled transport injuries, followed by motorcycles. Bicycle injuries were also represented in Netherlands, Greece, Denmark and Ireland (descending proportionate order).
Transport-related SCI are over represented in Greece and Italy, which also have high standardised death rate s for transport-related mortality (Belanger35). There were proportionately slightly higher rates of motorcycle injuries in Greece and Italy compared with other western European countries. The papers identified risk-taking behaviour in young males in Greece as well as a destructive driving culture and a need for effective road safety programs (Divanoglou39). Pagliachi40 comments on young Italian males, poor seatbelt use (22% of people injured in car collisions used seatbelts), travelling during the summer weekends and the use of alcohol and drugs. Presumably, inter-related to this is an issue of legislative enforcement. Education and prevention programs in both regions were identified as being in urgent need.
Falls-related SCI rates are high in Western Europe (17–49%, median 32%). Europe has one of the highest proportions of older persons (age>60 years) in the world41 and this is likely to contribute to high-fall rates for many years.
Attempted suicide-related SCI in Western Europe varied between 1 and 26%, with a median value of 8%. There appeared to be a relationship between high-suicide rates and Scandinavian countries (with the exception of Switzerland), with the five highest rates (in high to low order) being Greenland (26%), Switzerland (9%), Sweden (9%), Denmark (8%) and Finland (7%).13, 39, 42, 43, 44
SCI in Greenland is marked by the highest attempted suicide rate in Western Europe (26%). The Pedersen report42 notes that six out of every seven suicide attempts in Greenland were jumps from buildings. SCI in this area is also characterised by high levels of accidental gunshot injury (15%), mostly due to hunting. Greenland also had low-land transport rates (4%), with all of these being motorcycle injuries. Relatively, high numbers of skiing accidents (4%) were also seen in this region. Approximately, 50% of SCI in Greenland occurred under the influence of alcohol.
Horse riding-related injuries were highest in Ireland (4%),45 Sweden (3%)46 and Iceland (of the sports-related injuries, horse riding was the single largest cause, but no percentage was provided).47
Latin America, Tropical
Statistics were only available for Brazil.48, 49, 50, 51 Rates of SCI resulting from violence-related gun shots were high (27–37%, median 30%). Regional data that involved a major urban centre recorded higher gunshot-related injuries. Land transport was a common cause (27–42%, median 35%). Aetiology for land transport, where available, (for example, San Paulo) was mostly four-wheeled vehicles followed by motorcycles. Diving into shallow water was an issue reported by Campos da Paz.51
North Africa, Middle East
Land transport accidents were high (49%), but subcategories for these accidents were unavailable for Turkey.52 In Jordan, 44% of the land-transport accidents were mostly four-wheeled vehicles and involved high speed and lack of seatbelts. In Jordan, drinking and driving was not considered a common occurrence because of the adherence to Muslim beliefs (Otom53). SCI from falls, particularly falls from heights were common in Turkey (37%). These were mostly falls from trees and from rooftops (People sleep on rooftops in summer when it is hot) and these falls tend to involve children and the elderly. Accidental gunshot injuries were high in Jordan (26%) and in the paper were partly attributed to guns being fired into the air as a cultural tradition, particularly in rural areas, as well as mishandling of guns. Unpublished data was available for Saudi Arabia (Alshahri54). The high rate of transport-related injury (85%) is striking, mostly as a result of accidents involving four-wheeled vehicles. The male preponderance for SCI is likely enhanced by the lack of female drivers within the road system in Saudi Arabia.
North America, high income
National incidence data were available for Canada (Rick Hansen Spinal Cord Injury Register20) 35 per million and USA (30–40 per million, median 38.4).16, 19, 55, 56
Within Canada, nationally, land transport-related SCI was 47% with the following regional data ranges: low (34% (Toronto)) (35% (S/W Ontario )) to high (56% (Alberta)). Falls accounted for 17% of SCI, with sports and recreation being 7%.20
Within USA, land transport-related SCI is the most common cause of SCI (48%, NSCISC,56 most recent national data). Burney57 provided the most detailed aetiology data, that is, overall, land transport, 52% of out of which most were four-wheeled vehicles (40%), followed by motorcycles (7%).
Violence-related data in the USA is high by global comparisons (14% NSCISC,56 most recent national data). Burney57 provided the most detailed aetiology data. Overall, violence provided 15% of the aetiology in the USA and, of the violence-related injuries, 14% were gunshot related and 1% stabbings.
The most recent national data for falls-related SCI is 23% (NSCISC56). Regional data was fairly close to the National figure.
Hawaii has a higher incidence of diving-related SCI (12%) when compared with the rest of the USA (Goebert58). In other USA regional data reports, diving-related SCI ranged from 3 to 6% (Griffin,59 Kraus,60 Price,61 Acton,62 Thurman63 and Calancie64).
Oceania
Fiji Islands: (Maharaj65) Main aetiology are falls (39%), a high proportion being falls out of trees followed by sports and recreation 28% (a quarter of which arose from rugby and 1 in 20 from diving). Land transport was not particularly high at 25%.
Sub-Saharan Africa, Southern
The main aetiologies are land transport and violence in these regions. In South Africa, land transport ranged proportionally from a low of 28% in the southern Transvaal to a high of 34% in the Cape Province.66, 67 In Zimbabwe, land transport accounted for half of the SCI cases.68 Violence-related SCI in South Africa was higher than in Zimbabwe (25% in Cape Province, 61% in Johannesburg and 62% in the southern Transvaal compared with 15% in Zimbabwe). In the Cape Province and Johannesburg, gunshots predominated (40 and 35%, respectively).67, 69 Stabbings were lower and ranged between 22 and 26% in these two South-African regions. In southern Transvaal and Zimbabwe, gunshots were proportionally lower, 2 and 4%, respectively. Falls were proportionally low in both countries (South Africa 3–12% and 17% in Zimbabwe).
Sub-Saharan Africa, West
Most of the published aetiological data are from regions in Nigeria (Iwegbu70 Zaria region, Igun71 Plateau State, Obalum72 Lagos, Solagberu73 Ilorin, Nwankwo74 and Nwadinigwe75 Enugu, and Olasode76 Ile-Ife) and Sierra Leone (Gosselin77).
In general, the numbers of SCI cases treated annually in Nigeria and Sierra Leone are quite low (ranging from 5 to 33 cases annually (median 15 cases) for Nigeria and about eight cases annually in Sierra Leone. As reported by most of the above authors, this is because of the high mortality rate during patient retrieval by untrained first responders and the lack of specialised or adequately resourced treatment centers, particularly outside of large population centres like Lagos.
Aetiologically, land transport (ranging from 57 to 89%) and falls (ranging from 8 to 24%) accounted for about 84% of the SCI cases in Nigeria and 92% of the cases in Sierra Leone. Almost all falls in Nigeria and Sierra Leone were from trees.
In this region, very little SCI incidence data have been published.
Survival of SCI globally
Long-term longitudinal data (10-year mortality) are only available for those countries with established SCI registries such as the USA (16.2%, Krause: Southeast region78), Canada (10.7%: Hu, Manitoba region.79) and Australia (14.3%, O’ Connor80).
Developed countries have significantly improved survival data compared with undeveloped countries. There has been a dramatic improvement in survival over the last 40 years in developed countries. Tetraplegics have lower survival rates than paraplegics; however, in developed countries, this gap has narrowed considerably. Soden et al.81 projected from New South Wales (Australian) data that the mean life expectancy of SCI compared with the underlying Australian population was approximately 70% of normal for complete tetraplegia and 86% of normal for complete paraplegia.
Developing countries have the highest 1-year mortality rates and in some countries in sub-Saharan Africa, the occurrence of a spinal injury is likely to be a fatal condition within a year. In Sierra Leone (2002–2004) after 28 months, 20 patients (83%) out of an initial cohort of 24 were dead and the remaining 4 were lost to follow-up. Nigeria (1996–2001) had a 1-year mortality rate of 34.3%.75 South Africa and Zimbabwe reported a 1-year mortality rate of 13% and 49%, respectively.67, 68
Epidemiological data standards for TSCI
The piecemeal approach to the reporting of SCI epidemiological statistics, and in particular reporting of data without a sound regional denominator, has exhausted its utility. We propose the following standards:
-
1
Authors should provide a clear description of the population being surveyed.
-
2
Data should be reported using the International Standards core data set as a minimum.7
-
3
Traumatic and non-traumatic SCI data should be clearly distinguished
-
4
The aetiology of traumatic SCI should ideally be described using the ICECI or other standardised aetiological classification. Software, which integrates the ISCoS core data set with the ICECI as well as ICECI training tools and videos are available at zero cost at http://www.iscos.org.uk/page.php?content=20).
-
5
Annual reports of national statistics should be published on the internet in a searchable manner.
-
6
The International Spinal Cord Society and other relevant organisations should explore options for a centralised data repository and/or related links to facilitate injury prevention planning. The tabulations and a summary form for data submissions are available on the ISCoS website. We welcome submissions of unpublished or published data from the Spinal Cord readership to produce an annual electronic update.
Conclusions
Assimilation of data, assessing significance and determination of a course of action can be greatly facilitated by mapping techniques, which allow complex data to be used quickly and intuitively by clinicians and the makers of policy. We believe that future efforts should not only address reporting deficiencies but also the manner of publication to improve the comparability of available information. Eventually, comparisons should extend to prevention methodology and allow more rapid global learning about what works and why, as well as provide policy traction for advocates of injury prevention.
The ISCoS Prevention Committee is supporting the standardisation of traumatic injury reporting by a process of incremental validation and the release of free software tools developed by this team to allow all countries (particularly red zone countries) to access the types of injury reporting available in green and yellow Zone global precincts. Our current software allows participants to combine ISCoS core data set reporting with injury coding through the ICECI. An Asian Spinal Cord Network version has been developed, translated into Vietnamese and is being piloted in Vietnam. A Chinese version is now underway.
From the standpoint of injury prevention, these tools surpass the constructs used in the established green/yellow zone databases as they allow multi-axial analysis of data and are more amenable to interpretation through injury matrices.82, 83 Start-up collaborations can be facilitated by request to the corresponding author.
Incidence and Survival Data
These tables are extensive and are available through an online repository at ISCoS.
Supplementary Table 2: incidence and aetiology of traumatic SCI by region and author(s) of published data (http://iscos.org.uk/page.php?content=57).
Supplementary Table 3: survival of SCI (1-year and 10-year mortality) by region and author(s) of published data (http://iscos.org.uk/page.php?content=57).
References
Ackery A, Tator C, Krassioukov A . A global perspective on spinal cord injury epidemiology. J Neurotrauma 2004; 21: 1355–1370.
Wyndaele M, Wyndaele JJ . Incidence, prevalence and epidemiology of spinal cord injury: what learns a worldwide literature survey? Spinal Cord 2006; 44: 523–529.
Mackay J, Mensah G . The Atlas of Heart Disease and Stroke. Myriad Editions, published by the World Health Organization 2004, ISBN 92 4 156276 8.
Blumer CE, Quine S . Prevalence of spinal cord injury: an international comparison. Neuroepidemiology 1995; 14: 258–268.
New PW, Sundararajan V . Incidence of non-traumatic spinal cord injury in Victoria, Australia: a population-based study and literature review. Spinal Cord 2008; 46: 406–411.
Harvard University, Institute for Health Metrics and Evaluation at the University of Wasington, Johns Hopkins University, University of Queensland, World Health Organization (WHO), Geneva, Switzerland. Operations Manual, final draft, January 20. In, 2009.
DeVivo M, Bierring-Sørensen F, Charlifue S, Noonan V, Post M, Stripling T, Wing P . International Spinal Cord Injury Core Data Set. Spinal Cord 2006; 44: 535–540.
Razdan S, Kaul RL, Motta A, Kaul S, Bhatt RK . Prevalence and pattern of major neurological disorders in rural Kashmir (India) in 1986. Neuroepidemiology 1994; 13: 113–119.
Weerts E . Final reporting of project outcomes Spinal Cord Injury care and Orthopedic workshop. Handicap International, Hanoi, Vietnam, 2009.
Walsh J . Costs of spinal cord injury in Australia. Paraplegia 1988; 26: 380–388.
O’Connor PJ . Prevalence of spinal cord injury in Australia. Spinal Cord 2005; 43: 42–46.
Yeo JD, Walsh J, Rutkowski SB, Soden RJ, Craven ML, Middleton JW . Mortality following spinal cord injury. Spinal Cord 1998; 36: 329–336.
Dahlberg A, Kotila M, Leppanen P, Kautiainen H, Alaranta H . Prevalence of spinal cord injury in Helsinki. Spinal Cord 2005; 43: 47–50.
Knutsdottir S . Spinal cord injuries in Iceland 1973–1989. A follow-up study. Paraplegia 1993; 31: 68–72.
Harvey C, Rothschild BB, Asmann AJ, Stripling T . New estimates of traumatic SCI prevalence: a survey-based approach. Paraplegia 1990; 28: 537–544.
Lasfargues JE, Custis D, Morrone F, Carswell J, Nguyen T . A model for estimating spinal cord injury prevalence in the United States. Paraplegia 1995; 33: 62–68.
Kurtzke JF . Epidemiology of spinal cord injury. Exp Neurol 1975; 48 (3, Part 2): 163–236.
DeVivo MJ, Fine PR, Maetz HM, Stover SL . Prevalence of spinal cord injury: a reestimation employing life table techniques. Arch Neurol 1980; 37: 707–708.
Stover SL, Fine PR . The epidemiology and economics of spinal cord injury. Paraplegia 1987; 25: 225–228.
Rick Hansen Spinal Cord Injury Register. Spinal Cord Injury Facts and Statistics: Canada, 2006.
United Nations: Department of Economic and Social Affairs PD. World Population Ageing 2009. United Nations: New York, 2009.
Shingu H, Ohama M, Ikata T, Katoh S, Akatsu T . A nationwide epidemiological survey of spinal cord injuries in Japan from January 1990 to December 1992. Paraplegia 1995; 33: 183–188.
Ide M, Ogata H, Tokuhiro A, Takechi H . Spinal cord injuries in Okayama prefecture: an epidemiological Study ‘88-‘89. J UOEH 1993; 15: 209–215.
Chen CF, Lien IN . Spinal cord injuries in Taipei, Taiwan, 1978–1981. Paraplegia 1985; 23: 364–370.
Chen HY, Chen SS, Chiu WT, Lee LS, Hung CI, Hung CL et al. A nationwide epidemiological study of spinal cord injury in geriatric patients in Taiwan. Neuroepidemiology 1997; 16: 241–247.
Raja IA, Viohra AH, Ahmed M . Neurotrauma in Pakistan. World J Surgery 2001; 25: 1230–1237.
Hoque MF, Grangeon C, Reed K . Spinal cord lesions in Bangladesh: an epidemiological study 1994–1995. Spinal Cord 1999; 37: 858–861.
Mukhida K, Sharma MR, Shilpakar SK . Pediatric neurotrauma in Kathmandu, Nepal: implications for injury management and control. Childs Nerv Syst 2006; 22: 352–362.
Kovindha A . A retrospective study of spinal cord injuries at Maharaj Nakorn Chiang Mai Hospital, during 1985–1991. Chiang Mai Med Bull 1993; 32: 85–92.
Pajareya K . Traumatic spinal cord injuries in Thailand; an epidemiologic study in Siriraj Hospital, 1989–1994. Spinal Cord 1996; 34: 608–610.
Cripps R . Spinal cord injury, Australia, 2006–07. In: Injury Research and Statistics Series Number 48 Cat. no. INJCAT 119.. AIHW: Adelaide, 2008.
Dixon GS, Danesh JN, Caradoc-Davies TH . Epidemiology of spinal cord injury in New Zealand. Neuroepidemiology 1993; 12: 88–95.
Jankowski R, Zukiel R, Nowak S, Czekanowska-Szlandrowicz R, stachowska-Tomczak B . Vertebral column and spinal cord injuries: isolated and concomitant with multiple injury. Chir Narz Ruchu Ortop Pol 1993; 58: 353–359.
Soopramanien A . Epidemiology of spinal injuries in Romania. Paraplegia 1994; 32: 715–722.
Belanger F, Ung A-B, Falzon A . Transport-related deaths in an enlarged European Union. Institut de veille sanitaire: Saint-Maurice, 2008.
Sabre L, Linnamagi U, Derrik G, Rekand T, Asser T, Korv J . Traumatic spinal cord injuries in Estonia from 2003 to 2007. In: ISCoS. University of Tartu: Florence, 2009.
Silberstein B, Rabinovich S . Epidemiology of spinal cord injuries in Novosibirsk, Russia. Paraplegia 1995; 33: 322–325.
Kondakov EN, Simonova IA, Poliakov IV . The epidemiology of injuries to the spine and spinal cord in Saint Petersburg. Zhurnal Voprosy Neirokhirurgii Imeni N—N—urdenko 2002; 2: 50–53.
Divanoglou A, Levi R . Incidence of traumatic spinal cord injury in Thessaloniki, Greece and Stockholm, Sweden: a prospective population-based study. Spinal Cord 2009; 47: 1–6.
Pagliacci MC, Celani MG, Zampolini M, Spizzichino L, Franceschini M, Baratta S et al. An Italian survey of traumatic spinal cord injury. the gruppo italiano studio epidemiologico mielolesioni study. Arch Phys Med Rehabil 2003; 84 (September): 1266–1275.
World Population Ageing 2009, United Nations: Department of Economic and Social Affairs, Population Division, New York, ESA/P/WP/212 December, 2009, pp. 1–66.
Pedersen V, Muller PG, Biering-Sorensen F . Traumatic spinal cord injuries in Greenland 1965–1986. Paraplegia 1989; 27: 345–349.
Gehrig R . Statistics of acute paraplegia and tetraplegia on a natonal scale, Switzerland 1960–1967. Paraplegia 1988; 6: 93–95.
Biering-Sorensen F, Pedersen V, Clausen S . Epidemiology of spinal cord lesions in Denmark. Paraplegia 1990; 28: 105–108.
O’Connor RJ, Murray PC . Review of spinal cord injuries in Ireland. Spinal Cord 2006; 44: 445–448.
Augutis M, Levi R . Pediatric spinal cord injury in Sweden: incidence, etiology and outcome. Spinal Cord 2003; 41: 328–336.
Knutsdottir S, Thorisdottir H . Epidemiology of spinal cord injuries in Iceland 1973–2008. In: ISCoS Conference Proceedings, 48th ISCoS Annual Scientific Meeting, Florence, Italy, 21–24th October, 2009. Abstract number P47, p.224. (http://www.iscos2009.com/Docs/Book_of_abst.pdf).
Brasil AVB, Coelho DG . The neurological outcome of acute spinal cord injury in a neurosurgical hospital of a developing country. Spinal Cord 1998; 36: 353–356.
Greve J . Epidemiology from the developing world: what we have, what we need—Brazil. In. Medical School Of the University of Sao Paulo, Sao Paulo, Brazil, 2009, pp 1–8.
Barros F, Taricco MA, Oliveira RP, Greve JM, Santos LC, Napoli MM . Epidemiological study of patients with spinal cord injuries. Rev hosp Fac Med S Paulo 1990; 45: 123–126.
Campos da Paz A, Beraldo PSS, Almeida MCRR, Neves EGC, Alves CMF, Khan P . Traumatic injury to the spinal cord. Prevalence in Brazilian hospitals. Paraplegia 1992; 30: 636–640.
Karacan I, Koyuncu H, Pekel O, Sumbuloglu G, Kirnap M, Dursun H et al. Traumatic spinal cord injuries in Turkey: a nation-wide epidemiological study. Spinal Cord 2000; 38: 697–701.
Otom AS, Doughan AM, Kawar JS, Hattar EZ . Traumatic spinal cord injuries in Jordan—an epidemiological study. Spinal Cord 1997; 35: 253–255.
Alshahri S . Traumatic spinal cord injury in Saudi Arabia: an epidemiological study. Unpublished work, 2010.
Ditunno JF, Formal CS . Chronic spinal cord injury. New Engl J Med 1994; 330: 550–556.
National Spinal Cord Injury Statistical Centre Birmingham Alabama. Spinal Cord Injury Facts and Figures at a Glance. Alabama, USA, 2008.
Burney RE, Maio RF, Maynard F, Karunas RB . Incidence, characteristics, and outcome of spinal cord injury at trauma centers in North America. Arch Surg 1992; 128: 596–599.
Goebert DA, Ng MY, Varney JM, Sheetz DA . Traumatic spinal cord injury in Hawaii. Hawaii Medical Journal 1991; 50: 44–50.
Griffin MR, O’Fallon WM, Opitz JL, Kurland LT . Mortality, survival and prevalence: traumatic spinal cord injury in Olmsted County, Minnesota, 1935–1981. J Chron Dis 1985; 38: 643–653.
Kraus JF, Franti CE, Riggins RS, Richards D, Borhani NO . Incidence of traumatic spinal cord lesions. J Chron Dis 1975; 28: 471–492.
Price C, Makintubee S, Herndon W, Istre GR . Epidemiology of traumatic spinal cord injury and acute hospitalization and rehabilitation charges for spinal cord injuries in oklahhoma, 1988–1990. Am J Epidemiol 1994; 139: 37–47.
Acton PA, Farley T, Freni LW, Ilegbodu VA, Sniezek JE, Wohlleb JC . Traumatic spinal cord injury in Arkansas, 1980–1989. Arch Phys Med Rehabil 1993; 74: 1035–1040.
Thurman DJ, Burnett CL, Jeppson L, Beaudoin DE, Sniezek JE . Surveillance of spinal cord injuries in Utah, USA. Paraplegia 1994; 32: 665–669.
Calancie B, Molano MR, Broton JG . Epidemiology and demography of acute spinal cord injury in a large urban setting. J Spinal Cord Med 2005; 28: 92–96.
Maharaj JC . Epidemiology of spinal cord paralysis in Fiji: 1985–1994. Spinal Cord 1996; 34: 549–559.
Hart C, Williams E . Epidemiologyof spinal cord injuries: a reflection of changes in South African society. Paraplegia 1994; 32: 709–714.
Key AG, Retief PJM . Spinal cord injuries: an analysis of 300 new lesions. In: International Medical Society of Paraplegia: Annual Scientific Meeting. Tel-Aviv: Paraplegia, 1968, pp 243–249.
Levy LF, Makarawo S, Madzivire D, Bhebhe E, Verbeek N, Parry O . Problems, struggles and some success with spinal cord injury in Zimbabwe. Spinal Cord 1998; 36: 213–218.
Velmahos GC, Degiannis E, Hart K, Souter I, Saadia R . Changing profiles in spinal cord injuries and risk factors influencing recovery after penetrating injuries. J Trauma 1995; 38: 334–337.
Iwegbu CG . Traumatic paraplegia in Zaria, Nigeria: the case for a centre for injuries of the spine. Paraplegia 1983; 21: 81–85.
Igun GO, Obekpa OP, Ugwu BT, Nwadiaro HC . Spinal injuries in the Plateau State, Nigeria. East Afr Med J 1999; 76: 75–79.
Obalum DC, Giwa SO, Adekoya-Cole TO, Enweluzo GO . Profile of spinal injuries in Lagos, Nigeria. Spinal Cord 2009; 47: 134–137.
Solagberu BA . Spinal cord injuries in Ilorin, Nigeria. West Afr J Med 2002; 21: 230–232.
Nwankwo OE, Katchy AU . Outcome of a 12-week programme for management of the spinal cord injured with participation of patient's relations at Hilltop Orthopaedic Hospital, Enugu, Nigeria. Spinal Cord 2003; 41: 129–133.
Nwadinigwe CU, Iloabuchi TC, Nwabude IA . Traumatic spinal cord injuries (SCI): a study of 104 cases. Niger J Med 2004; 13: 161–165.
Olasode BJ, Komolafe IE, Komolafe M, Olasode OA . Traumatic spinal cord injuries in Ile-Ife, Nigeria, and its environs. Tropical Doctor 2006; 36: 181–182.
Gosselin RA, Coppotelli C . A follow-up study of patients with spinal cord injury in Sierra Leone. Int Orthop 2005; 29: 330–332.
Krause JS, Zhai Y, Saunders LL, Carter RE . Risk of mortality after spinal cord injury: an 8-year prospective study. Arc Phys Med Rehabil 2009; 90 (October): 1708–1715.
Hu R, Mustard CA, Burns C . Epidemiology of incident spinal fracture in a complete population. Spine 1996; 21: 492–499.
O′Connor PJ . Survival after spinal cord injury in Australia. Arch Phys Med Rehabil 2005; 86: 37–47.
Soden RJ, walsh J, Middleton JW, Craven ML, Rutkowski SB, Yeo JD . Causes of death after spinal cord injury. Spinal Cord 2000; 38: 604–610.
Lee BB, Cripps RA, Woodman RJ, Biering-Sørensen F, Wing P, Campbell R et al. Development of an international spinal injury prevention module: application of the international classification of external cause of injury to spinal cord injury. Spinal Cord 2010; 48: 498–503.
Barnett DJ, Balicer RD, Blodgett D, Fews AL, Parker CL, Links JM . The application of the Haddon matrix to public health readiness and response planning. Environ Health Perspect 2005; 113: 561–566.
Acknowledgements
We would like to thank Mr Obayd Marial, Mr Adam Rutkowski and Mr Jason Chuang for their generous assistance with translation, and Dr Saaide Alshahari for providing Saudi-Arabian unpublished data. We would also like to thank members of the ISCoS prevention committee and the ISCoS membership for their continuing enthusiasm. Dr Lee and Myriad Mapping were funded by the Prince of Wales Hospital Training, Education and Study Leave fund (New South Wales Department of Health, Australia). Claire Weeks was instrumental in putting together the team for this report.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Additional information
Supplementary Information accompanies the paper on the Spinal Cord website
Supplementary information
Rights and permissions
About this article
Cite this article
Cripps, R., Lee, B., Wing, P. et al. A global map for traumatic spinal cord injury epidemiology: towards a living data repository for injury prevention. Spinal Cord 49, 493–501 (2011). https://doi.org/10.1038/sc.2010.146
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sc.2010.146
Keywords
This article is cited by
-
Incidence and mortality of spinal cord injury from 2008 to 2020: a retrospective population-based cohort study in the Piedmont Region, Italy
Spinal Cord (2023)
-
Single-cell RNA sequencing in orthopedic research
Bone Research (2023)
-
Factors associated with neuropathic pain in Colombian patients with spinal cord injury of traumatic origin: case–control study
Spinal Cord Series and Cases (2022)
-
Epidemiology of traumatic spinal cord injury: a large population-based study
Spinal Cord (2022)
-
Clinical and demographic predictors of symptoms of depression and anxiety in patients with spinal cord injury
Spinal Cord (2022)
