
Abstract
Plate fixation is a common treatment option for radial head fractures (RHFs). Due to the benefits of less invasiveness and fewer complications of internal fixation, the application of small-diameter headless compression screws (HCSs) to treat RHFs has become a new trend. This study aimed to compare the mechanical stability of four distinct internal fixation protocols for transversely unstable RHFs via finite element analysis. Using computed tomography data from 10 patients, we developed 40 patient-specific FE models of transversely unstable RHFs fixed by parallel, crossed, and tripod HCSs and mini-T plate (MTP). Under simulated physiological loading of the elbow joint, the construct stiffness, displacement, and von Mises stresses were evaluated and verified by a biomechanical experiment. Under shear loading, the MTP group exhibited lower construct stiffness, larger displacement, and higher Von Mises stress than the HCSs group. The stiffness of tripod HCSs was greater than parallel and crossed screw fixation techniques. There was a strong relationship between apparent bone density and construct stiffness (R = 0.98 to 0.99). In the treatment of transversely unstable RHFs, HCSs have superior biomechanical stability than MTP. The tripod technique was also more stable than parallel and crossed fixation.
Similar content being viewed by others


Introduction
Radial head and neck fractures account for approximately half of all proximal forearm fractures1. Increasing research on the elbow joint has shown that the integrity of the radial head is essential for elbow stability and force transmission2. Open reduction and internal fixation is now the treatment of choice for Mason type II and III radial head fractures (RHFs) with significant displacement or comminution3. Traditional treatments for radial head and neck fractures include k-wires, elastic flexible intramedullary nailing, cannulated screws, biodegradable pins, and various types of plates4,5,6,7. Plates and screws are the most common treatment modality for Mason II RHFs and have been the subject of numerous investigations8. In the treatment of axially unstable RHFs, plate fixation has exhibited generally favorable mechanical stability, according to previous research. However, there is a high incidence of postoperative complications, such as internal fixation failure, deformity recovery, and limitation of forearm rotation9,10. Therefore, researchers have progressively adapted headless compression screws (HCSs) as a less invasive option for the treatment of radial head and neck fractures11.
Small-diameter HCSs have been used to treat radial head and neck fractures for decades. Recently, parallel screws, crossed screws, and tripod techniques for the treatment of radial head and neck fractures have been reported11,12,13. Screw fixation may be a viable alternative to plate fixation due to its favorable outcomes and reduced rate of implant-related complications11,14. However, current retrospective clinical studies have flaws such as small sample size, lack of control, and absence of biomechanical evidence to support the study. Consequently, the purpose of this study was to compare the mechanical properties of 4 distinct fixation methods of HCSs and mini-T plate (MTP) for transversely unstable RHFs using FEA and to provide a theoretical basis for the selection of implant scheme for surgical treatment of RHFs.
Statistical analysis
GraphPad Prism 9 was used for statistical analysis, and the data for each group was expressed as the mean ± standard deviation. The Shapiro–Wilk test was used to test the normality of the experimental data. If the data of each group conformed to a normal distribution, the ANOVA was used to compare the groups, and the LSD-test was used for two-way comparisons between groups; if not, the Kruskal–Wallis test was used to compare the groups, and Bonferroni correction was used for two-way comparisons between groups. Using Pearson correlation analysis, the correlation between apparent bone density and construct stiffness was identified. A p-value less than 0.05 indicated a statistically significant difference.
Results
Construct stiffness
The same tendencies exist in the stiffness results of the FEA and the biomechanical experiment (Fig. 1A and Table 1), and the mean values of stiffness differ by 1 standard deviation between the two sections. The current FE model generates reliable biomechanical results. The MTP group had the lowest stiffness among the four groups and was substantially less stable than the HCSs groups (p = 0.021). The stiffness of the tripod headless compression screws (THCSs) group was the highest among the HCSs groups. Figure 1B displays a strong correlation (R = 0.98 to 0.99) between apparent bone density (ρ) and construct stiffness, as determined by Pearson correlation analysis.

Stiffness results and model validation. (A): Stiffness results of FEA and biomechanical test. (B): Correlation analysis between apparent bone density calculated by HU and construct stiffness.
The maximal displacement of the implants
As depicted in Fig. 2A and Table 1, the MTP group exhibited the greatest MID under shear loading (p = 0.011). In comparison to the MTP group, the MID in the THCSs group exhibited a 64.5% reduction (p = 0.016). Moreover, the THCSs group demonstrated the lowest MID among HCSs groups.

Displacement and stress results for 40 sets of FEA. (A): The maximal implant displacement (MID). (B): The maximum relative displacement of the head-neck fragment (MRD). (C): The maximal implant von Mises stress (MIS). (D): The maximal fracture surface von Mises stress (MFS) (*p < 0.05).
The maximal relative displacement of head-neck fragments
We calculated the MRD based on the terminal position of the paired nodes on the radial head and neck fragments. The MRD was further subdivided into the shear direction (Shear interfragmentary motion, SIM) and the detached direction (Fig. 3). As shown in Fig. 2B and Table 1, the MRD was lowest in the THCSs group. In addition, the MRD of the MTP group was significantly greater than that of the HCSs groups (p < 0.001). The displacement cloud charts indicated a tendency for overturning and displacement of the radial head fragment, and all HCSs groups were significantly more stable than the MTP group.

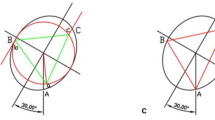
MRD was defined as the vector sum of SIM (Shear interfragmentary motion) and DIM (Detached interfragmentary motion) (displacement cloud chart was magnified by 50 times). (A) and (B) were the distal and proximal fracture surface paired nodes, respectively. The SIM and DIM were obtained by calculating the absolute value of the difference between the final positions of points A and B in the shear and detached directions.
The maximal stress of the implants and fracture end
In the parallel headless compression screws (PHCSs) group, the MIS was located on the screw surface at the fracture line, whereas in the crossed headless compression screws (CHCSs) and THCSs groups, the MIS was concentrated at the screw intersection (Fig. 4). The stress was concentrated at the intersection of the plate and the fracture line. The MIS for each screw group was close to the yield stress and significantly lower (Fig. 2C). Although the MIS of the MTP group was less than the titanium alloy yield stress (900 MPa)15, the risk of failure was substantially greater in comparison to the HCSs groups. The trend of MFS alterations within each group was comparable to that of MIS (Figs. 2D, 4 and Table 1). The MFSs of the PHCSs, CHCSs, and THCSs groups were comparable, whereas the MFSs of the MTP group were greater than those of each HCSs group (p = 0.042). The MTP group had a greater risk of new fractures than each HCS group.

The cloud charts of four internal fixation methods for laterally unstable radial head fractures. A1-A4: MID (mm); B1-B4: MIS (MPa); C1-C4: MFS (MPa).
Discussion
Biomechanical and clinical findings16,17 indicate that the integrity of the radial head positively influences elbow joint stability. The initial phase of fracture healing is especially mechanically sensitive18. By evaluating the movement between fracture fragments, studies have demonstrated that asymmetries in axial or shear motion are detrimental to callus formation and fracture healing19. Consequently, axial and transverse stability of the fracture extremities are essential for fracture healing. Plate fixation has been demonstrated to have sufficient rigidity to sustain axial physiological loading from the elbow joint during the early postoperative period20. Due to the complex morphology of the radial head, however, no single plate can be used to treat all RHFs21. Small-diameter HCSs could potentially address this issue. Biomechanical parameters such as stiffness, MRD, MID, MIS, and MFS have been used to evaluate the biomechanical characteristics of various types of implants22. Therefore, the present study used FEA to compare the biomechanical characteristics of HCSs and MTP for the treatment of RHFs and validated the FEA results using a biomechanical experiment, which provides a theoretical basis for orthopedic surgeons to choose internal fixation, and also helps to explore new techniques for the treatment of radial head fractures23.
Jeffrey et al.24 examined the simulated composite bone model used in biomechanical experiments and validated the dependability of the Synbone brand model results in upper extremity mechanical experiments, confirming that it can be used in place of cadaveric bone for biomechanical experiments. In addition, we have found in clinical practice that transversal displacement of the radial head relative to the neck accounted for the majority of postoperative fixation failures of RHFs. This phenomenon is related to the mechanical transfer characteristics of the elbow joint. The radial head is primarily subjected to shear forces exerted by the ulnar sigmoid notch during anterior–posterior rotation of the forearm25. Because fracture ends compress each other when axial loads are applied, and there are almost no mechanical differences between the groups, the axial compression simulation experiments were unable to demonstrate the variability between the various fixation methods. In addition, torsional loading is unlikely to be the cause of internal fixation failure because the proximal end of the radius is unrestrained26. Therefore, shear pressures were chosen and simulation experiments were conducted based on the radius of patients with varying bone quality. It may be possible to detect subtle differences in the treatment of radial head and neck fractures with various fixation modalities by increasing the sample size.
Structural stiffness is an important indicator for assessing the stability of implants. By quantifying the displacement at the site of load application, the construct stiffness can be accurately calculated27. The FEA and biomechanical experiment results indicated that the shear stiffness of the HCSs group was greater than that of the MTP group. Chen et al.28 discovered through biomechanical experiments that crossed and parallel screws are more resistant to transverse and rotational instability than plates. In addition, this study revealed that the tripod technique is more resistant to transverse instability than the crossed and parallel screws fixation protocols. In the treatment of transversely unstable radial head and neck fractures, the HCSs pass through both fragments, exerting a continuous compressive force on the fracture surface. However, the MTP fixation lacked a rigid connection at the fracture line, which was partially supported by the plate at the fracture end, rendering it significantly more susceptible to shear forces than the HCSs groups. Notable was the fact that the construct stiffness of the fracture model increased with the change in screw configuration and number. By comparing the biomechanical properties of vertical shear fractures in the inner ankle fixed with different screw orientations, Amanatullah et al.29 concluded that when screws were not placed parallel, only the first screw produced a compression effect, and additional non-parallel screws served to stabilize rotation, translation, etc. Therefore, we conclude that the additional HCSs implanted in this study served to resist the transverse instability of the fracture, which was one of the reasons why the shear stiffness was greater in the THCSs group than in the PHCSs group. The strong correlation between apparent bone density calculated from HU values and shear stiffness (Fig. 1) is an intriguing finding that is consistent with previous findings. Previous research has demonstrated that HU values are a reliable indicator of a patient's skeletal mass and fracture risk30,31. In addition, skeletal mass is one of the determinants of structural bone strength32. Haverstock et al.33 calculated bone density by measuring HU values in the region of interest (ROI) of the radial cranium and discovered that fracture risk was elevated in regions with low bone mineral density. In addition to the firm fixation effect of the internal implant, the grade of the bone has a significant impact on the fracture end's stability.
Moderate axial compression strain promotes fracture healing, whereas shearing and separation movements at the fracture site inhibit fracture end healing19,34. The MID of each HCSs group was considerably lower than that of the MTP group, as demonstrated by the results of FEA performed on 40 groups. The displacement cloud charts revealed that the implant displacement distribution was more dispersed in the HCSs group than in the MTP group, where the implants were concentrated at the fracture end of the head fragment. In addition, shear and separation movements were observed in the radial head fragment under shear loading. This trend was most pronounced in the MTP group, as indicated by a higher MRD in the MTP group compared to each HCSs group, similar to the experimental findings of Christina et al.13. Using fresh cadaver bone, they conducted biomechanical experiments to compare the shear stiffness of radial neck fractures fixed with crossed screws to that of radial head plates. It was discovered that the plate group tends to have lower detrimental loads and relative displacement of radial head and neck fragments than the crossed screw group. Differently, we evaluated the inter-fracture strain by normalizing the axial and shear movement between the fracture ends. Additionally, we analyzed parallel, tripod structures based on the crossed screw configuration and discovered that the THCSs group had the highest overall stability among the HCSs groups. All of these results indicate that HCS is superior to MTP for treating radial head and neck fractures. In addition, the tripod fixation modality is advantageous for the treatment of transversely unstable radial head fractures. With the change in screw fixation and the increase in the number of screws, however, the difficulty in fabricating FE and biomechanical models increases, which may make the tripod technique more challenging to perform surgically. However, clinical practice has yet to verify the hypothesis.
Peak VMS has a strong relationship with static yielding and fatigue failure23. In the CHCSs and THCSs groups, the MIS was located at the intersection of the screws, which were smaller than those in the PHCSs group. In the PHCSs and MTP groups, the MIS was located where the fracture line met the implants. In addition, it is noteworthy that the MTP group experienced a more concentrated distribution of stress, which implies a higher risk of failure. Different mechanisms of stress transfer can account for the dissimilar stress distributions in each group. During early function rehabilitation of radial head fracture, a dynamic equilibrium is established between the rigid fixation of the internal implant and the shear loading of the radial head from the ulnar sigmoid notch. The radial head ultimately transmits stress to the bone-implant interface. After transfer to the bone-implant interface, stresses were distributed to the screws in the HCSs groups, preventing radial head detachment and shear motion. As the number of screws and screw configuration changed, the tension dispersion became more pronounced. In the MTP group, the plate tended to deform backward at the attachment point to the fracture line, where it carried the majority of the stress. MFS also adequately described this force transfer mechanism. In each group, the MFS was predominantly concentrated at the bone-implant interface. Notably, the MFS in the MTP group was significantly higher than that of the remaining groups and was close to the yield stress of human bone, which implies that the risk of a new fracture line at the plate-fracture line apposition was considerably higher in the MTP group than in the HCSs group. Under shear loading, at the bone-screw interface of the HCSs groups, new fracture lines appeared. In contrast, in the MTP group, the plate failed at the fracture end with a lower failure force compared to the HCSs groups28.
According to our knowledge, this is the first study to utilize FEA to investigate the biomechanical stability of various HCS implantation techniques and MTP fixation of transversely unstable RHFs. By simulating RHFs with varying bone densities, validating them through biomechanical experiments, and comparing the results to clinical phenomena, the simulation results were made more applicable to the actual clinical situation. However, this study has several limitations. First, the FE model omitted the adjacent results of the radial head and the soft tissues and only considered the shear load on the radial head, which was unable to realistically simulate the stress transmission mode of the elbow joint, resulting in a certain discrepancy between the experimental results. Second, the MTP and HCS models utilized in this research are inadequate to depict all plate and screw varieties. There is a need for additional inquiry into the distinctions between internal fixation techniques. Using synthetic, simulated radius instead of cadaveric specimens to validate the finite element results is also a limitation.
Conclusion
In conclusion, HCSs are more biomechanically stable than MTP for the treatment of transversely unstable radial head and neck fractures. In addition, the tripod technique was the most stable of the screw groups, and all three methods of screw fixation maintained the fracture line's stability. However, the conclusions of this research must be validated by large-scale clinical studies.
Materials and methods
Models establishment
In this study, we retrospectively analyzed the imaging data of 10 patients with radial head and neck fractures. These patients ranged in age from 30 to 72 years, six males and four females, and had no elbow joint trauma or history of osteoarthritis or metabolic bone disease at the time of CT scan. All CT examinations were performed using three multidetector-row CT scanners (SOMATOM SENSATION 64, Siemens Healthcare) with a spatial resolution of 13.7Lp/cm @ 10% MTF. CT images of the healthy elbow joint with a layer thickness of 0.6 mm were saved in digital imaging and communications in medicine (DICOM) format and imported into Mimics 21.0 (The Materialise Group, Leuven, Belgium) to reconstruct patient-specific transversely unstable radial head fracture models. The models were then imported into Geomagic Wrap2021 (Geomagic, Rock Hill, SC, USA) for additional refining. To facilitate subsequent calculations, a 10 cm solid model of the proximal radius was intercepted. According to the osteotomy scheme of Lipman et al.12 10 patient-specific three-dimensional solid models of RHFs were developed in SolidWorks 2021 (DS SolidWorks Corp, Waltham, MA, USA).
Two internal fixation models (3.5 mm HCSs (Arthrex Corporation, Naples, FL), 2.0 mm MTP and corresponding locking screws, (Synthes, Paoli, PA, USA)) were constructed in SolidWorks based on the manufacturer-supplied dimensions. The implant models were implanted into each group of fracture models based on the same criteria as the fixation protocols used in previous studies. In the PHCSs group, two parallel HCSs were implanted at 45° to the radial head axis to fix the fracture model28. In the CHCSs group, two HCSs were placed at intervals of 60° and then crossed to fix the fracture model35. In the THCSs group, three HCSs were implanted separately along the margin of the radial head and disseminated circumferentially around the radial head to form a triangular frame12. The screws were placed 5 mm proximal to the tip of the radial head, with more than 5 mm between each pair36. In the MTP group, the plate was positioned in the safety zone of the radial head and fixed with three proximal and two distal locking screws28. A total of 40 internal fixation models of RHFs were created using the protocol outlined above (Fig. 5). Boolean operations were used to simulate bone loss during drilling and placement of implants during the surgical procedure.

Schematic diagram of four internal fixation methods for laterally unstable radial head fractures. (A): The parallel HCSs group; (B): The crossed HCSs group; (C): The tripod HCSs group; (D): The MTP group.
FE parameter setting
The established fracture models were imported into ANSYS workbench 2020R2 (Ansys, Canonsburg, PA) for further FEA. All fracture models and internal fixation models were presumed to be composed of homogeneous and isotropic linearly elastic materials20. The Hounsfield unit (HU) of cancellous and cortical radius bone was measured separately for each patient using the picture archiving and communication system (Syngo, SIEMENS AG, Germany) following the techniques described in previous studies30,37. Using the following Eqs. 38, the apparent density (ρ), Young's modulus (E), and Poisson's ratio (v) of the radius were assigned based on the Hu value in the CT scans:
All implant models were defined as titanium alloy (Ti-6L-4 V) with a Young's modulus of 110,000 MPa and a Poisson's ratio of 0.3539.
The contact between fracture surfaces and bone and plate was set to be frictional with a friction coefficient of 0.30. Bonded contact was set up between bone and HCSs, and between locking screws and plate40. The model meshed with tetrahedron (C3D10) elements using a mesh size of 0.6 mm, and the number of mesh elements and nodes for all models was shown in Table 2. A grid convergence test revealed that by doubling the mesh density, the von Mises stress (VMS) values of radius and internal fixations increased by no more than 5%, thereby validating the current mesh density. FEA primarily reveals the outcome indicators of the fracture surface and implants; consequently, we enhanced the computational precision by refining the geometry in these regions. Consequently, we established the boundary conditions of the FE models. To maintain consistency with the biomechanical validation experimental conditions, the degrees of freedom along the X, Y, and Z axes for the distal 2.5 mm portion of the RHFs model were set to “0”. A shear load of 50 N was applied from the posterior to the anterior side of the radius to simulate the force from the ulnar sigmoid notch on the radial head during postoperative functional forearm rotation exercise (Fig. 6). Subsequently, parameters including construct stiffness, the maximal implant displacement (MID), the maximal relative displacement of the head-neck fragment (MRD), the maximal implant von Mises stress (MIS), and the maximal fracture surface von Mises stress (MFS) were assessed.

Loading force and fixed support settings for the radial head. (A): A shear load of 50 N was applied from the posterior to the anterior side of the radius to simulate the force from the ulnar sigmoid notch on the radial head during postoperative functional exercise of forearm rotation. (B): The freedom of the distal radial was set to “0” at X-, Y-, and Z-axes.
FEA verification
The proximal 10 cm of 40 identically sized and dense synthetic radii (Synbone 7220, Synbone AG, Switzerland) were used to validate the FEA results through biomechanical testing. Using an oscillating saw, osteotomies were performed at the junction of the radial head and radial neck to simulate transversely unstable RHFs. According to the FE internal fixation scheme, HCSs and MTPs were implanted in each group. The images of each group were subsequently evaluated with a C-arm X-ray machine (Ziehm Solo FD, Ziehm Imaging, Germany) in order to reduce the experimental error induced by surgical manipulation. The distal 2.5 mm portion of the RHFs model was embedded in a wooden block using polymethylmethacrylate (PMMA) and then secured to the universal testing machine platform with a custom clamp. Using an INSTRON universal testing equipment (E3000, INSTRON, USA), shear pressures were applied to the radial head at a rate of 2 mm/min (Fig. 7) from posterior to anterior 28. The experiment was terminated when the radial head displacement reached 2 mm or when the internal fixation failed. The load–displacement curve was recorded, and the construct stiffness of each group was calculated and compared to the FEA outcomes. Model failure was defined as (1) the appearance of new fracture lines in the model other than the original fracture lines; (2) implant failure, such as bending, cutting out, or fracture of implants; (3) shear movement of the radial head exceeding 2 mm; and (4) flattening of the force–displacement curve in the data acquisition system or no significant change in model displacement as the load continued to increase36.

The radial head fracture model was placed on the INSTRON universal testing machine for the biomechanical test.
Ethical approval and consent to participate
The study protocol was reviewed and approved by the Biomedical Research Ethics Committee of West China Hospital, Sichuan University (NO.2023.1115). Considering the retrospective nature of this study, informed consent was waived by the Biomedical Research Ethics Committee of West China Hospital, Sichuan University. All experiments were performed in accordance with relevant guidelines and regulations.
Data availability
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
References
Duckworth, A. D. et al. The epidemiology of radial head and neck fractures. J. Hand Surg. Am. 37, 112–119. https://doi.org/10.1016/j.jhsa.2011.09.034 (2012).
Klug, A., Nagy, A., Gramlich, Y. & Hoffmann, R. Surgical treatment of the radial head is crucial for the outcome in terrible triad injuries of the elbow. Bone Joint J. 102-B, 1620–1628. https://doi.org/10.1302/0301-620X.102B12.BJJ-2020-0762.R1 (2020).
Sun, H., Duan, J. & Li, F. Comparison between radial head arthroplasty and open reduction and internal fixation in patients with radial head fractures (modified Mason type III and IV): a meta-analysis. Eur. J. Orthop. Surg. Traumatol. 26, 283–291. https://doi.org/10.1007/s00590-016-1739-1 (2016).
Wu, P. H., Dixit, A., Kiat Tan, D. M., Shen, L. & Chee, Y. H. Prospective study of surgical fixation of radial head fractures using cannulated headless compression screws for simple and complex radial head fractures. J. Orthop. Surg. (Hong Kong) 25, 2309499017716278. https://doi.org/10.1177/2309499017716278 (2017).
Gao, X., Yin, H. L. & Zhou, G. J. Minimally invasive treatment of mason type II radial head fracture by intramedullary pinning. Orthop. Surg. 11, 879–885. https://doi.org/10.1111/os.12540 (2019).
Tarallo, L., Mugnai, R., Rocchi, M., Capra, F. & Catani, F. Comparison between absorbable pins and mini-screw fixations for the treatment of radial head fractures Mason type II-III. BMC Musculoskeletal Disorders 19, 94. https://doi.org/10.1186/s12891-018-2014-x (2018).
Crönlein, M. et al. Using an anatomically preshaped low-profile locking plate system leads to reliable results in comminuted radial head fractures. Arch. Orthop. Trauma Surg. 137, 789–795. https://doi.org/10.1007/s00402-017-2693-z (2017).
Zwingmann, J. et al. Clinical results after different operative treatment methods of radial head and neck fractures: a systematic review and meta-analysis of clinical outcome. Injury 44, 1540–1550. https://doi.org/10.1016/j.injury.2013.04.003 (2013).
Ruchelsman, D. E., Christoforou, D. & Jupiter, J. B. Fractures of the radial head and neck. J. Bone Joint Surg. American 95, 469–478. https://doi.org/10.2106/JBJS.J.01989 (2013).
Burkhart, K. J., Wegmann, K., Müller, L. P. & Gohlke, F. E. Fractures of the radial head. Hand Clin. 31, 533–546. https://doi.org/10.1016/j.hcl.2015.06.003 (2015).
Demiroglu, M. et al. Results of screw fixation in Mason type II radial head fractures. Springerplus 5, 545. https://doi.org/10.1186/s40064-016-2189-2 (2016).
Lipman, M. D., Gause, T. M., Teran, V. A., Chhabra, A. B. & Deal, D. N. Radial head fracture fixation using tripod technique with headless compression screws. J. Hand Surg. Am. 43(575), e571-575.e576. https://doi.org/10.1016/j.jhsa.2018.03.009 (2018).
Gutowski, C. J., Darvish, K., Ilyas, A. M. & Jones, C. M. Comparison of crossed screw versus plate fixation for radial neck fractures. Clin. Biomech. (Bristol, Avon) 30, 966–970. https://doi.org/10.1016/j.clinbiomech.2015.07.001 (2015).
Model, Z., Merchan, N., Rozental, T. D. & Harper, C. M. Outcomes of radial head fractures treated with the “tripod technique”. J. Hand Surg. Am. 47, 581–582. https://doi.org/10.1016/j.jhsa.2021.06.014 (2022).
Bolzoni, L., Ruiz-Navas, E. M. & Gordo, E. Evaluation of the mechanical properties of powder metallurgy Ti-6Al-7Nb alloy. J. Mech. Behav. Biomed. Mater. 67, 110–116. https://doi.org/10.1016/j.jmbbm.2016.12.005 (2017).
Kastenberger, T. et al. Clinical and radiological outcome of Mason-Johnston types III and IV radial head fractures treated by an on-table reconstruction. J. Orthop. Surg. Res. 17, 503. https://doi.org/10.1186/s13018-022-03394-w (2022).
Miyamura, S., Lans, J., Murase, T., Oka, K. & Chen, N. C. Degenerative changes in the elbow joint after radial head excision for fracture: quantitative 3-dimensional analysis of bone density, stress distribution, and bone morphology. J. Shoulder Elbow Surg. 30, e199–e211. https://doi.org/10.1016/j.jse.2020.09.035 (2021).
Klein, P. et al. The initial phase of fracture healing is specifically sensitive to mechanical conditions. J. Orthop. Res. 21, 662–669 (2003).
Elkins, J. et al. Motion predicts clinical callus formation: construct-specific finite element analysis of supracondylar femoral fractures. J. Bone Joint Surg. Am. 98, 276–284. https://doi.org/10.2106/jbjs.O.00684 (2016).
Rebgetz, P. R., Daniele, L., Underhill, I. D., Öchsner, A. & Taylor, F. J. A biomechanical study of headless compression screws versus a locking plate in radial head fracture fixation. J. Shoulder Elbow Surg. 28, e111–e116. https://doi.org/10.1016/j.jse.2018.10.008 (2019).
Burkhart, K. J., Nowak, T. E., Kim, Y.-J., Rommens, P. M. & Müller, L. P. Anatomic fit of six different radial head plates: comparison of precontoured low-profile radial head plates. J. Hand Surg. Am. 36, 617–624. https://doi.org/10.1016/j.jhsa.2010.12.028 (2011).
Lewis, G. S., Mischler, D., Wee, H., Reid, J. S. & Varga, P. Finite element analysis of fracture fixation. Current Osteoporosis Rep. 19, 403–416. https://doi.org/10.1007/s11914-021-00690-y (2021).
Lewis, G. S., Mischler, D., Wee, H., Reid, J. S. & Varga, P. Finite element analysis of fracture fixation. Curr. Osteoporos. Rep. 19, 403–416. https://doi.org/10.1007/s11914-021-00690-y (2021).
Reed, J. D., Stanbury, S. J., Menorca, R. M. & Elfar, J. C. The emerging utility of composite bone models in biomechanical studies of the hand and upper extremity. J. Hand Surg. Am. 38, 583–587. https://doi.org/10.1016/j.jhsa.2012.12.005 (2013).
Wagner, F. C. et al. Biomechanical dynamic comparison of biodegradable pins and titanium screws for operative stabilization of displaced radial head fractures. Proc. Inst. Mech. Eng. H 234, 74–80. https://doi.org/10.1177/0954411919884794 (2020).
Giffin, J. R., King, G. J. W., Patterson, S. D. & Johnson, J. A. Internal fixation of radial neck fractures: an in vitro biomechanical analysis. Clin. Biomech. (Bristol, Avon) 19, 358–361 (2004).
Wee, H., Reid, J. S., Chinchilli, V. M. & Lewis, G. S. Finite Element-derived surrogate models of locked plate fracture fixation biomechanics. Ann. Biomed. Eng. 45, 668–680. https://doi.org/10.1007/s10439-016-1714-3 (2017).
Chen, H. et al. Comparison of three different fixation constructs for radial neck fractures: a biomechanical study. J. Orthop. Surg. Res. 12, 175. https://doi.org/10.1186/s13018-017-0680-2 (2017).
Amanatullah, D. F., Khan, S. N., Curtiss, S. & Wolinsky, P. R. Effect of divergent screw fixation in vertical medial malleolus fractures. J. Trauma Acute Care Surg. 72, 751–754. https://doi.org/10.1097/TA.0b013e31823b8b9f (2012).
Schreiber, J. J., Gausden, E. B., Anderson, P. A., Carlson, M. G. & Weiland, A. J. Opportunistic osteoporosis screening - gleaning additional information from diagnostic wrist CT scans. J. Bone Joint Surg. Am. 97, 1095–1100. https://doi.org/10.2106/JBJS.N.01230 (2015).
Viveen, J. et al. Regional differences in the three-dimensional bone microstructure of the radial head: implications for observed fracture patterns. Arch. Orthop. Trauma Surg. 142, 165–174. https://doi.org/10.1007/s00402-020-03665-3 (2022).
Gebauer, M. et al. Microarchitecture of the radial head and its changes in aging. Calcified Tissue Int. 86, 14–22. https://doi.org/10.1007/s00223-009-9304-0 (2010).
Haverstock, J. P. et al. Regional variations in radial head bone volume and density: implications for fracture patterns and fixation. J. Shoulder Elbow Surg. 21, 1669–1673. https://doi.org/10.1016/j.jse.2012.07.002 (2012).
Claes, L. E. & Meyers, N. The direction of tissue strain affects the neovascularization in the fracture-healing zone. Med Hypotheses 137, 109537. https://doi.org/10.1016/j.mehy.2019.109537 (2020).
Smith, G. R. & Hotchkiss, R. N. Radial head and neck fractures: anatomic guidelines for proper placement of internal fixation. J. Shoulder Elbow Surg. 5, 113–117 (1996).
Shi, X. et al. Effect of different orientations of screw fixation for radial head fractures: a biomechanical comparison. J. Orthop. Surg. Res. 12, 143. https://doi.org/10.1186/s13018-017-0641-9 (2017).
Phillips, A., Burton, N. J., Warren-Smith, C. M., Kulendra, E. R. & Parsons, K. J. Topographic bone density of the radius and ulna in greyhounds and labrador retrievers with and without medial coronoid process disease. Vet Surg. 44, 180–190. https://doi.org/10.1111/j.1532-950X.2014.12294.x (2015).
Reina-Romo, E., Rodríguez-Vallés, J. & Sanz-Herrera, J. A. In silico dynamic characterization of the femur: physiological versus mechanical boundary conditions. Med. Eng. Phys. https://doi.org/10.1016/j.medengphy.2018.06.001 (2018).
Zhang, H., Lin, K.-J., Liu, P.-Y. & Lu, Y. Finite element analysis of coronoid prostheses with different fixation methods in the treatment of comminuted coronoid process fracture. J. Orthop. Traumatol. 23, 56. https://doi.org/10.1186/s10195-022-00675-2 (2022).
Lv, M. L. et al. Biomechanical analysis of a novel double-point fixation method for displaced intra-articular calcaneal fractures. Front. Bioeng. Biotechnol. 10, 791554. https://doi.org/10.3389/fbioe.2022.791554 (2022).
Funding
This work was supported by the 2023 Natural Science Foundation of Sichuan Province (grant no.2023NSFSC1490), and the 2023 Key research and development project of Sichuan Province (grant no.2023YFS0504).
Author information
Authors and Affiliations
Contributions
LY and XZ contributed equally to this work. LY and XZ designed the study, analyzed the study data, and drafted the manuscript. ZZ and JL corrected the study data and searched the relevant literature. ZX revised the manuscript and supervised the study. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Yang, L., Zhang, X., Zhong, Z. et al. Patient-specific finite element analysis of four different fixation methods for transversely unstable radial head fractures. Sci Rep 14, 21134 (2024). https://doi.org/10.1038/s41598-024-70602-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-70602-4
Keywords
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
