
Abstract
Non-Verbal Learning Disability (NVLD) is a neurodevelopmental disorder characterized by deficits in processing visuospatial information but with age-appropriate verbal skills. This cognitive profile has been hypothesized to be associated with atypical white matter, but at the present there is a lack of evidence for this hypothesis. Currently, the condition is not characterized within the main diagnostic systems, in part because no clear set of criteria for characterizing the disorder exists. This report is the first attempt to estimate NVLD prevalence, using two sets of diagnostic criteria, in a large sample of over 11,000 children who were selected without regards to problems of specific nature, either psychological, neurological, physical and/or social. Furthermore, it examined the association between the profile of cognitive abilities and aspects of whole-brain white matter measures in children with and without symptoms associated with NVLD. Participants were drawn from the Adolescent Brain Cognitive Development (ABCD) study, a 10-year longitudinal study of 11,876 children in the U.S. The data used in the present study were drawn from the initial testing point at which the children were 9–10 years old. Prevalence of NVLD based on two distinct sets of criteria, correlations between the measures used to create the criteria, correlations between criteria measures and measures of white matter integrity. The cognitive criteria included measures of visuospatial processing, reading, intelligence and social skills. By varying the cut-offs applied to social skills in conjunction with visuo-spatial difficulties, spared reading skills and intelligence scores, we calculated prevalence for two NVLD groups. White matter characteristics were measures of volume, fractional anisotropy and mean diffusivity. Based on the criteria used, the estimated prevalence of NVLD varied from 1 to 8%. Furthermore, children with NVLD showed a dissociation between measures of visuo-spatial processing not observed in non-NVLD children. At the neurological level, findings provide preliminary evidence of associations between the cognitive profile of NVLD and abnormalities in white matters tracts. The present study documents that exists, within this large non-selected sample, a proportion of youth who show evidence of NVLD. Given those results, it appears essential to establish the best diagnostic criteria, to improve the treatment options and quality of life for children with this disorder.
Similar content being viewed by others

Introduction
The term Non-Verbal Learning disability (NVLD) was first introduced by Johnson and Myklebust in 19671: they described children characterized by difficulties in processing information in the non-verbal domain accompanied by spared verbal abilities. In more recent years, several researchers have studied, in more depth, children with visuospatial processing deficits and examined the possible associations with problems concerning attention, motor, academic and social skills, in the absence of frank neurological symptoms or genetic disorders2,4. There is evidence showing that the difficulties in visuospatial processing interfere with a child’s quality of social, school or life functioning5. In fact, although the core deficits are in visuospatial processing, symptoms can also impact the social domain, especially in relation to non-verbal processing6. In particular, children with NVLD show more severe problems in the visuospatial domain compared to either children with Autism Spectrum Disorder (ASD) or Attention Deficit-Hyperactivity Disorder (ADHD)2,7. These include difficulties with visuospatial working memory8,9, spatial organizational skills and comprehension of spatial descriptions10,11, and nonverbal problem-solving abilities12, all within the context of preserved language abilities.
At the clinical level, despite increased awareness of the characteristics of NVLD derived from research findings, there are currently no “official” diagnostic criteria for NVLD13,14. From a review of the literature, Fisher et al. in 20225 highlighted that the most common criterion used in the past to define NVLD is a discrepancy between verbal and visuospatial intelligence (10 or 15 points between verbal and performance IQ)13. However, this criterion has been criticized by some researchers15,16, since it is not rare to find such a discrepancy in neurotypical children17. Given that NVLD is defined by an impairment in cognitive functioning, more specifically in the realm of visuospatial processing, general heterogeneous consequences for academic achievement and social interactions would be expected. Hence, it could be appropriate not to use the achievement and social measures as a diagnostic criterion. Obviously, which criteria are used (a discrepancy score, or just the level of visuospatial difficulties) will influence estimation of the actual prevalence of NVLD18. These considerations have inspired the current investigation with the goal of exploring the prevalence rates of NVLD depending on different criteria for defining this disorder.
At the neurological level, the cognitive profile observed in NVLD has been explained as resulting from a ‘white matter’ syndrome (term coined by Rourke in 1989)19, indicating that there are damaged or dysfunctional long myelinated white matter fiber tracts in the brain20: these abnormalities have been hypothesized to be mainly located in the right hemisphere. Both animal and human studies point toward the importance of intact white matter for spatial processing21,22, but there are no studies in the literature specifically linking white matter to the cognitive profile of NVLD, probably due to the lack of shared diagnostic criteria, which in turn makes it difficult to find appropriate sample sizes for such studies.
The Adolescent Brain Cognitive Development (ABCD) study represents the largest available dataset of children (over 11,000) tested at 9/10 years old, who will be part of the project until 18 years of age. The ABCD database offers researchers an unprecedented opportunity to: (a) test which criteria and cut-offs are most suitable for identifying the characteristics of NVLD; and (b) investigate the white matter contribution to performance in the visuospatial domain in children with a NVLD profile compared to a control group of children of the same age and thus at a similar stage of development. Although not part of the present report, the longitudinal nature of the ABCD study will allow researchers to follow the developmental trajectory of this population and to further confirm or modify the best criteria for identifying NVLD.
The present study
Given the above considerations, the first goal of the present research was to estimate the prevalence of symptoms associated with a NVLD profile, and to test different criteria in order to investigate which are most informative in describing the population of interest. Surprisingly, considering that the first conceptualization of NVLD was made over 50 years ago, only a few studies have attempted to estimate its prevalence. Moreover, they are generally based on small sample sizes5, on non-representative samples in terms of demographic characteristics, and often were drawn from populations with learning disorders (LD) more generally5 (but see23). A great advantage of the present investigation, compared with the community-drawn sample of Margolis et al.23, is that the sample size is larger, it has broad representation of the US in terms of demographics such as socioeconomic and ethnic backgrounds, and it does not involve children/adolescents with selected problems of specific nature, either psychological, neurological, physical and/or social. For these reasons the present research can yield a more accurate estimation of the prevalence of NVLD.
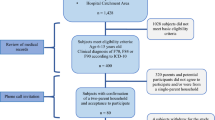
The main aim of the present investigation was to estimate the prevalence of the cognitive profile associated with NVLD following two different sets of criteria. Overall requirements for inclusion as NVLD were the presence of visuospatial processing deficits (equal to/below the 16th percentile), preserved reading decoding (above the 25th percentile), intact total or crystallized intelligence (average or above average), and the absence of symptoms of Autistic Spectrum Disorder (ASD). An additional criterion allowed to distinguish two candidate NVLD groups, one with and the other without regards to social problems. In more detail, (1) the first group was characterized by social abilities above the 85th percentile (with social impairment), while (2) the second NVLD group was estimated without using the social impairment as a criterion. See the defining criteria of the two NVLD groups in Fig. 1 and Table 2.

Representation of the NVLD groups, the cognitive criteria, the estimated prevalence and the relation between subgroups [VS visuospatial, ASD Autism Spectrum Disorder].
The rationale for estimating the prevalence of the NVLD in the ABCD sample with and without regard to social problems is that the scientific community is still debating about the inclusion of this domain as a criterion, with inconsistences concerning the inclusion of social problems as a defining criterion for NVLD13 mainly due to a difficulty in understanding the primary characteristics of NVLD. Moreover, recent evidences are supporting a causal role of the core deficit in the visuospatial domain in explaining the social difficulties5. Another consideration is that having these two NVLD groups represents a possibility for future research to have a comparable set of criteria until a consensus on the diagnostic criteria will be reached.
The second aim of the study was to investigate how measures of visuospatial processing correlate with each other and to other criteria used to define a NVLD profile, in the ABCD sample as a whole and likewise in the two identified NVLD groups. The purpose was to determine whether visuo-spatial abilities seem to cohere or dissociate in different manners in the two samples. In addition, we measured sensitivity and specificity of the visuo-spatial tasks used to identify the deficit in the domain of interest in order to provide an estimation of which task has the potential of becoming a diagnostic tool.
The final goal of the research was to shed more light on the neurobiological underpinnings of NVLD by examining whether there are differences in the relationship between the measures of white matter and visuospatial performance in children with and without an NVLD profile. This endeavor may be critical in identifying unique behavioral and neurobiological features of NVLD that may aid in understanding the etiology of the disorder as well as with regards to clinically-relevant considerations, such as diagnosis and the implementation of effective interventions. In order to gain more insight into the NVLD profile, a correlation analysis was applied also between measures of white matter and performances in the other criteria, that is reading abilities, social skills, fluid, crystallized and total intelligence.
Methods
Sample
The ABCD dataset (release 3.0; https://abcdstudy.org/) includes 11,878 children aged 9–10 years. This is a 10-year longitudinal dataset being collected at 21 sites across the US. Full recruitment details are described in24. It is worth mentioning that participants were drawn from a diverse range of geographic, socioeconomic, ethnic, and health backgrounds meant to be generally similar to that of the US population of 9–10 years old at the initial time point of the study25,26.
Institutional review board approval was obtained for each site before data collection and all parents provided written informed consent in addition to assent from the child participants.
Behavioural measures for the estimation of the prevalence
The following table (Table 1) presents the tasks used as a criterion in the areas of visuospatial processing, intelligence, reading and social skills.
From a parent self-report questionnaire, we have extracted the information about the diagnosis of ASD.
The choice of including the three visuospatial tasks was made because: (a) there are not known diagnostic indices to measure the core deficit of NVLD; (b) the scientific community did not assess yet if the visuo-spatial deficit is just due to the nature of the material presented, thus involving the perceptual processing (as measured by the matrix reasoning test), or due to the recognition of a visuospatial stimulus (as measured by the 0-back), or the manipulation of it (little man task).
The cut-off (16th and 85th percentile) applied to the visuospatial and the social domain in order to identify the deficits was based on both clinical39 and research23,40 practices. Instead, the reasoning behind the choice of the cutoffs applied to reading (25th percentile) and intelligence (50th percentile) was based on the evidence that NVLD children have good reading skills13 and average or above average total and crystallized intelligence13.
Magnetic resonance imaging
The structural MRI measures used in the present study were the following: one anatomical MRI metric, white matter (WM) volume, and two diffusion MRI metrics: fractional anisotropy (FA) and mean diffusivity (MD). WM volume represents the volume in \({{\text{mm}}}^{3}\). FA measures the directionality of water diffusion within brain tissue that is found to be greater in organized WM tracts. MD refers to the rotationally invariant magnitude of diffusion in the brain and its increase is often reported in case of disease41 signaling that pathological processes have affected the structure of white matter and in turn the water motion. Diffusion and anatomical MRI measures were obtained for each hemisphere separately. For a detailed description of the analytic approaches applied to MRI data see26.
Data analysis
The study aimed at estimating the prevalence of the symptoms associated with a NVLD profile and to further explore their neurobiological correlates. First, we set the criteria and identified two different NVLD groups which were differentiated by the cut-offs related to social problems, while keeping constant the criteria applied to visuospatial processing, reading, intelligence and the exclusion of children with a diagnosis of ASD. The 1st NVLD group was estimated with regard to social problems while the 2nd NVLD group was calculated without regard to social problems.
Then we performed three sets of bivariate correlations on the various measures: the first examined the associations of scores between the different behavioral criteria and the second examined the associations between visuospatial performance and white matter measures. The third correlational analysis was applied between white matter measures and the other criteria used to estimate the prevalence of NVLD (reading abilities, social skills, fluid, crystallized and total intelligence). A comparison was made between each correlation observed for the NVLD group with that of the whole ABCD by applying a Z test (Eq. 1) of the difference of the Fisher's Z transformed correlations divided by the standard error of the difference. For sample sizes of n and n2, we found the z of the difference between the z transformed correlations divided by the standard error of the difference of two z scores:
The last set of analysis included the estimation of sensitivity and specificity that in clinical settings is used to estimate the ability of a test to designate individuals with a disease as positive (sensitivity) and the ones without a disease as negative (specificity). This analysis was performed to investigate if there are differences in the sensitivity and the specificity of the three visuospatial tasks. Sensitivity is calculated by dividing the number of estimated true positive (individuals that are found to be NVLD just based of the score of the task considered) and the true positive (number of individuals with the NVLD profile). Specificity is calculated by dividing the estimated true negative (individual without an NVLD profile as defined by the score on the specific task considered) and the true negative (number of individuals without an NVLD profile). This approach was applied only to the NVLD group without regard to social problems (2nd group) since it contains also the sample identified in the group with regard to social problems (1st group). This analysis was performed with the package caret42, specifically with the functions called sensitivity and specificity.
Data analysis was performed in R (v 4.1.0).
Results
Prevalence of NVLD profile in the ABCD sample
The present research used two different sets of criteria (for scores corresponding to percentiles used see S1 in Supplementary materials) to define groups of children presenting symptoms associated with the NVLD profile, as shown in Table 2.
Following these different sets of criteria, the estimated sample sizes of the two groups (Fig. 1) were:
Group 1: 144 children (1.21%),
Group 2: 977 children (8.23%).
Behavioural data
Correlations
The second goal of the present research was to investigate how the measures of visuospatial processing correlated to each other and to other criteria used to select the NVLD profile, in the whole population and in the two identified NVLD groups (Table 3).
The main characteristic that differentiated the NVLD groups from the whole sample was a negative correlation between the mental rotation task and the other two visuospatial tasks, that is matrix reasoning and 0-back. In contrast, in the whole ABCD sample a significant positive correlation was evident between these two tasks and the mental rotation task, consistent with the idea that they measure similar underlying processes related to the visuospatial domain. The NVLD group without regard to social problems was also characterized by a significant negative correlation between the performance on the 0-back task and the scores on the matrix reasoning test that was not present in the whole ABCD sample. Furthermore, the two NVLD groups presented significantly different correlations between scores on the visuospatial tasks compared to the whole sample (as shown in the lower triangle of Table 3; see S2 in Supplementary materials).
Positive correlations between reading skills and the matrix reasoning test were significant in the NVLD group without regard to social problems (group 2), mimicking the results in the overall ABCD sample. Results from the Z-tests highlighted that the two NVLD groups had significantly different correlations between reading and visuospatial abilities compared to the whole ABCD population (see S2 in Supplementary materials for details on statistics).
The scale on social problems extracted from the CBCL (the higher the score, the more pronounced the social problems) was the only measure expected to always be negatively correlated with all the other scores. This held true for the whole ABCD sample. While in the NVLD group without regard to social problems (group 2) we found a significant negative correlation between social problems and the scores on the mental rotation task, that was not found in the other NVLD group in which we used as a criterion social problems on the social subscale of the CBCL. Peculiar to the group 2 were the correlations between visuospatial abilities (measured by matrix reasoning test and 0-back task) and social problems, which were significantly different from the whole sample (see S2 in Supplementary materials for statistics).
There was a positive correlation between the scores on matrix reasoning and total/crystallized intelligence in all the three NVLD groups. In addition, in group 2 there was a significant positive correlation between the fluid component and matrix reasoning, and between total intelligence and the performance on the 0-back task. Furthermore, the same NVLD group without regard to social problems (group 2) presented also a positive correlation between 0-back scores and fluid intelligence, and between the mental rotation task and fluid intelligence. Results of Z-tests indicated that the correlations between performance on thelittle man task and both components of intelligence (in addition to the total score of intelligence) were significantly different between the NVLD groups and the whole ABCD sample (see S2 in Supplementary materials for statistics).
Finally, an unexpected result was found with regards to the correlation between the two components of intelligence within the NVLD groups. It emerged that in the two NVLD groups, the two components of intelligence did not correlate with each other (see S3 in Supplementary materials for statistics).
Sensitivity and specificity of visuo-spatial measures
The sensitivity and specificity were calculated for all the visuospatial tasks considered as a criterion and the following table (Table 4) shows the result of the analysis. These results are presented as percentage of correctly identified sample with an NVLD profile (sensitivity) and percentage of the correctly identified sample without the NVLD profile (specificity).
The analysis highlight that the sensitivity of the little man task is higher than the matrix reasoning and the 0-back task, while all of them have comparable specificity (around 80%).
Correlations between white matter and visuospatial performance
This set of correlational analyses was conducted on white matter measures and performance on visuospatial tasks (Table 5).
In the whole ABCD sample, a significant positive correlation was found between visuospatial processing, as measured by the Little Man task and the 0-back task, and two white matter indices: volume and fractional anisotropy of both hemispheres. A negative correlation was, instead, found between MD and the performance on the Little Man task. The score on the matrix reasoning test was found to be positively correlated with the volume of white matter in both hemispheres and with the fractional anisotropy of the white matter in the right hemisphere.
For the NVLD group 1, performance on the Little Man task was negatively correlated with mean diffusivity of white matter in the right hemisphere. In contrast, no significant correlations were found for NVLD group 2.
A consistent result found in group 2 was between WM Volume in both hemispheres and performance in the three visuospatial tasks: Z-tests indicated significantly different correlations in the NVLD group compared to the ABCD sample. For groups 1 with the social criterion but only for one specific visuospatial task, that is 0-back task. See Supplementary materials for results of Z-test: S3 and S4 respectively for right and left hemispheres).
Correlations between white matter and other cognitive criteria: reading, intelligence and social problems
In order to gain more information about the NVLD profile and its differences compared with the all ABCD sample, a correlational analysis was applied between white matter measures and the other criteria used to estimate the prevalence of NVLD: reading skills, social abilities, fluid, crystallized, and total intelligence. Results are shown in Table 6.
Compared to the all ABCD sample, only group 2, without regard to social problems, showed a significantly different correlation between volume of both hemispheres and all cognitive indices, except for social problems. Furthermore, the NVLD group 2 and the all ABCD sample showed a different correlation between social problems and mean diffusivity of the left hemisphere. See Supplementary materials for results of Z-test: S5 and S6 respectively for right and left hemispheres).
Discussion
Prevalence of the NVLD profile
The first goal of the present investigation was to estimate the prevalence of the NVLD profile in a large, diverse sample of 11,876 North American children aged 9–10 years old. Our multi-pronged approach using two sets of criteria allowed us to identify two groups composed of 1.21% and 8.23% of the total ABCD sample, respectively. Therefore, we can broadly estimate that from 240,000 to 1.9 million children present symptoms associated with NVLD (among 24.5 million 6–11 years-old children estimated in 2019 by the U.S. Census Bureau).
Since group 1 had very strict criteria for both intelligence/reading as well as social problems, it is likely that it did not include all children presenting the overall symptoms associated with NVLD. For instance, from the literature it emerges that social problems are highly variable and not always present/evident, and possibly unspecific to NVLD. In fact, while it has been found that NVLD is associated with increased risk for internalizing psychopathology43, another study found that NVLD was not linked to levels of internalizing psychopathology as rated by the parents44. In addition, two comprehensive reviews45,46 of the literature highlighted that the results on socioemotional functioning in children with NVLD have been inconsistent.
Regarding group 2, it may represent the best definition of NVLD since it is the one better describing this neurodevelopmental condition, i.e., children with a deficit in visuospatial processing, spared verbal intelligence and reading abilities, and with no diagnosis of ASD. The estimation of the prevalence found to be at about 8% is doubled the one found in Margolis et al. (3–4%)23.
This difference between the prevalence rate in the current study and that of Margolis et al.23, could be due to various factors. First, we used consistent criteria throughout the whole sample while Margolis et al. used various samples and measures due to the involvement of 3 different datasets23. Furthermore, in order for our estimation not to be built on the score of single tasks, we also used composite scores for measuring intelligence which are more comprehensive measures of underlying cognitive processes. Second, Margolis et al. employed the discrepancy between verbal and visuospatial measures, whereas we decided not to include it since this approach has been criticized15,16 and it could influence the estimation of the prevalence18. Third, even considering that Margolis et al. used inflation factors weights to account for overrepresentation of the psychiatric disorders in their sample, our estimation was made on the ABCD dataset which not only involved mainly neurotypical children but it is composed by a sample that is more representative of the whole population in terms of geographic, socioeconomic and ethnic backgrounds than that of Margolis et al. Finally, the sample size of the ABCD dataset is considerably larger than the one of Margolis et al. (11 878 vs. 2 596).
Cognitive profile of NVLD
Social and visuospatial domains
The inclusion of social problems as a criterion to estimate the prevalence of NVLD seems to identify a restricted portion of children having deficits in nonverbal abilities. In contrast to Rourke’s cognitive model of NVLD19, recent research highlighted that social problems, while not a primary feature, may still be associated with the disorder13. However, we did not find consistent results on the link between visuospatial abilities and social problems, possibly indicating that there is not a tight association between the two in children with NVLD, even if social problems are used as a criterion. For this reason, we believe that the cut-off criterion of the second group better captures the clinical group of interest, since social problems are not always present and the thresholds imposed to intelligence, reading and visuospatial abilities are likely to reveal the actual difficulties that a child with NVLD has to face.
Among the identified groups presenting the main symptoms associated with NVLD, we found an interesting result that should be taken into account when measuring the performance in the visuospatial domain. The performance in a strictly visuospatial task involving active information manipulation, as in the little an test, should be employed along with other visuospatial tasks. In fact, only the NVLD groups showed a negative correlation between performance on the little man task and the other two visuospatial tests, i.e., matrix reasoning and 0-back tasks. A possible explanation is that NVLD children may try to compensate for their visuospatial deficits with their intact verbal reasoning abilities. Such compensation likely works better for the matrix reasoning and the 0-back task, which mainly involve abstract reasoning, memory and attention, than for the little man task, which likely relies on strategies strictly related to the visuospatial domain47,48. Furthermore, in the NVLD groups, intelligence is correlated with visuospatial performances in all visuospatial tasks except for the little man task, possibly indicating that they cannot use their intact cognitive abilities to perform this task.
Sensitivity and specificity of visuo-spatial tasks
The analysis on sensitivity and specificity of the tasks in the visuo-spatial domain revealed an interesting gap between the visuo-spatial tasks. While there were no differences in the specificity (around 80%), the sensitivity of the little man task (59%) was higher than matrix reasoning (53%) and the 0-back (36%). These results highlight that while all the tasks can accurately identify individuals not having an NVLD profile, only the little man task is sensitive at identifying individuals with an NVLD profile 59% of the time. It should be noted that since none of the tasks are designed to be a normative neuropsychological test. Achieving a sensitivity of 59% makes a promising starting point for developing test tailored to measure the visuo-spatial deficits mainly observed in NVLD.
Intelligence
The two NVLD groups did not show the positive correlation between crystallized and fluid intelligences found in the whole ABCD sample and in the other NVLD group. In fact, this finding indicates that these two components of intelligence are likely independent. It should be noted that theories of intelligence48 assume that the two components develop by mutual interactions and this reciprocal relation is hypothesized to be beneficial for both. Since this interactive process is likely not present in NVLD children, it would be useful to understand how this uncoupling is linked to development of processes such as reading and mathematics. In fact, a recent metanalysis49 highlighted that fluid intelligence and reading/mathematics are able to predict each other over developmental phases. Yet we did not find any significant correlation between reading and fluid intelligence in NVLD groups.
The lack of association between these two facets of intelligence might be helpful as an alternative to using a discrepancy score (generally 10–15 points)13 between verbal and performance IQ in order to study groups with and without a NVLD profile. For instance, by looking at their developmental trajectories, in future studies one could investigate if the lack of correlation between the two components of intelligence is a stable characteristic of this population.
Brain-behaviour linkages
As predicted, associations were found between the NVLD profile and aspects of white matter connectivity in the brain. In NVLD groups 1 (in which social problems serve as a criteria), the lower the performance in visuospatial processing, as measured by the little man task, the higher the mean diffusivity in the right hemisphere. This result indicated that in NVLD a greater disorganization of white matter tracts in the right hemisphere is linked to worse performance in mentally rotating visuospatial materials. Note however that this finding was not replicated in NVLD group 2 and did not extend to the other two tasks measuring visuospatial processing.
When analyzing the differences between correlations in the NVLD groups compared to the whole ABCD sample, the relationship of the visuospatial processing with the volume of the white matter yielded interesting results. In the NVLD group without regard to social problems (i.e., group 2), there was no relationship between visuospatial ability, as measured by all three tasks, and the volume of white matter. This link was significantly different compared to the whole population, in whom the higher the volume, the better the visuospatial performance. In the other NVLD group (i.e., group 1) there were relationships with white matter volume but only for one spatial task, the 0-back task.
Concerning the correlations between white matter measures and social problems, the group without regard to social problems (group 2) showed an interesting result compared to the all ABCD sample. In fact, while the direction of the correlation was negative in both samples, only in the NVLD group we found a significant correlation. The lower the mean diffusivity in the left hemisphere, the greater were the problems in the social domain.
In conclusion, the most relevant finding for the NVLD profile (group 2) in relation to visuospatial performance and white matter measures appeared to be the absence of the significant association found in typically developing children, for whom non-verbal IQ and visuospatial abilities were associated with white matter integrity. We propose that this lack of association may provide an important information regarding the neurobiological basis of the impairments found in NVLD22. This finding represents a first step toward a more sophisticated analysis to model this relationship between white matter and visuo-spatial ability50 and to better test the hypothesis of the relationship between the two20.
Limitations and future directions
The current study is not without limitations. While the sample size was very large, the measurement of visuo-spatial processing skills was restricted, due to the general scope of the ABCD study to test a wide variety of abilities and multiple factors that might influence brain development. In particular, we were not able to include measures assessing visuo-constructive, visuomotor and fine motor abilities which are often used in assessments for NVLD. Therefore, our estimation of 8% (977 children) prevalence of children with a likely diagnosis of NVLD should be taken with caution, while nonetheless pointing to the fact that it will be important to do future research to deepen our knowledge of this neurodevelopmental disorder.
A future goal of this line of research may be to follow the developmental trajectories of children with the NVLD profile in order to investigate how coping strategies may evolve as they grow up, and to find out whether cut-offs and tasks utilized in the present investigation continue to be the best at identifying children with NVLD in transition from middle childhood to the pre-adolescent and adolescent phase. Furthermore, the enormous heterogeneity of the measures present in ABCD protocol will allow researchers to apply other approaches to the study of brain correlates of the NVLD profile, for instance by focusing on specific regions and on other techniques, such as connectivity patterns in networks of interests. Finally, another future direction could be to investigate other weaknesses and strengths that are peculiar of the sample presenting an NVLD profile.
Conclusions
The above limitations notwithstanding, the present research represents the first attempt to estimate the prevalence of NVLD in a large sample of typically developing children. We found that depending on the criteria, the estimated incidence of the profile varied from 1 to 8%. Unlike the ABCD sample as a whole, the NVLD groups showed uncorrelated or negatively correlated performances in the three tasks measuring visuospatial performance indicating that they may apply different strategies to compensate the deficit depending on the demands of the task using visuospatial materials. Moreover, we found that while in typically developing children higher volume of white matter tracts was associated with better visuospatial abilities, children with NVLD did not show this link, bringing support to the notion that an atypical mechanism involving the myelinated tracts, particularly in the right hemisphere, could help to explain the cognitive profile of NVLD.
Data and availability
Data used in the preparation of this article were obtained from the Adolescent Brain Cognitive Development (ABCD) Study (https://abcdstudy.org), held in the NIMH Data Archive (NDA).
References
Johnson, D. J. & Myklebust, H. R. Learning Disabilities**** (Published online, 1967).
Semrud-Clikeman, M., Walkowiak, J., Wilkinson, A. & Christopher, G. Neuropsychological differences among children with Asperger syndrome, nonverbal learning disabilities, attention deficit disorder, and controls. Dev. Neuropsychol. 35(5), 582–600. https://doi.org/10.1080/87565641.2010.494747 (2010).
Mammarella, I. C., Cardillo, R. & Broitman, J. Understanding Nonverbal Learning Disability: A Guide to Symptoms, Management and Treatment 1st edn. (Routledge, 2021).
Fisher, P. W., Reyes-Portillo, J. A., Riddle, M. A. & Litwin, H. D. Systematic review: Nonverbal learning disability. J. Am. Acad. Child Adolesc. Psychiatry 61(2), 159–186 (2022).
Little, L. & Clark, R. R. Wonders and worries of parenting a child with Asperger syndrome and nonverbal learning disorder. MCN Am. J. Matern Child Nurs. 31(1), 39–44 (2006).
Semrud-Clikeman, M., Walkowiak, J., Wilkinson, A. & Minne, E. P. Direct and indirect measures of social perception, behavior, and emotional functioning in children with Asperger’s disorder, nonverbal learning disability, or ADHD. J. Abnorm. Child Psychol. 38(4), 509–519. https://doi.org/10.1007/s10802-009-9380-7 (2010).
Cardillo, R., Vio, C. & Mammarella, I. C. A comparison of local-global visuospatial processing in autism spectrum disorder, nonverbal learning disability, ADHD and typical development. Res. Dev. Disabil. 103, 103682. https://doi.org/10.1016/j.ridd.2020.103682 (2020).
Garcia, R. B., Mammarella, I. C., Tripodi, D. & Cornoldi, C. Visuospatial working memory for locations, colours, and binding in typically developing children and in children with dyslexia and non-verbal learning disability. Brit. J. Dev. Psychol. 32(1), 17–33 (2014).
Mammarella, I. C., Giofrè, D., Ferrara, R. & Cornoldi, C. Intuitive geometry and visuospatial working memory in children showing symptoms of nonverbal learning disabilities. Child Neuropsychol. 19(3), 235–249 (2013).
Mammarella, I. C., Meneghetti, C., Pazzaglia, F. & Cornoldi, C. Memory and comprehension deficits in spatial descriptions of children with non-verbal and reading disabilities. Front. Psychol. 5, 1534 (2015).
Mammarella, I. C. et al. Representation of survey and route spatial descriptions in children with nonverbal (visuospatial) learning disabilities. Brain Cognit. 71(2), 173–179. https://doi.org/10.1016/j.bandc.2009.05.003 (2009).
Schiff, R., Bauminger, N. & Toledo, I. Analogical problem solving in children with verbal and nonverbal learning disabilities. J. Learn. Disabil. 42(1), 3–13. https://doi.org/10.1177/0022219408326213 (2009).
Mammarella, I. C. & Cornoldi, C. An analysis of the criteria used to diagnose children with Nonverbal Learning Disability (NLD). Child Neuropsychol. 20(3), 255–280. https://doi.org/10.1080/09297049.2013.796920 (2014).
Yalof, J. Case illustration of a boy with nonverbal learning disorder and Asperger’s features: Neuropsychological and personality assessment. J. Personal. Assess. 87(1), 15–34 (2006).
Spreen, O. Nonverbal learning disabilities: A critical review. Child Neuropsychol. 17(5), 418–443 (2011).
Poletti, M. A research framework to isolate visuospatial from childhood motor coordination phenotypes. Appl. Neuropsychol. Child. 8(4), 383–388 (2019).
Semrud-Clikeman, M., Fine, J. G., Bledsoe, J. & Zhu, D. C. Magnetic resonance imaging volumetric findings in children with Asperger syndrome, nonverbal learning disability, or healthy controls. J. Clin. Exp. Neuropsychol. 35(5), 540–550. https://doi.org/10.1080/13803395.2013.795528 (2013).
Mammarella, I. C. The importance of defining shared criteria for the diagnosis of nonverbal learning disability. JAMA Netw. Open 3(4), e202559–e202559 (2020).
Rourke, B. P. Nonverbal Learning Disabilities: The Syndrome and the Model (Guilford Press, 1989).
Rourke, B. P. Syndrome of Nonverbal Learning Disabilities: Neurodevelopmental Manifestations 518 (The Guilford Press, 1995).
Gaffan, D. & Hornak, J. Visual neglect in the monkey. Representation and disconnection. Brain 120(9), 1647–1657. https://doi.org/10.1093/brain/120.9.1647 (1997).
Muetzel, R. L. et al. White matter integrity and cognitive performance in school-age children: A population-based neuroimaging study. Neuroimage 119, 119–128 (2015).
Margolis, A. E. et al. Estimated prevalence of nonverbal learning disability among North American children and adolescents. JAMA Netw. Open 3(4), e202551–e202551 (2020).
Garavan, H. et al. Recruiting the ABCD sample: Design considerations and procedures. Dev. Cognit. Neurosci. 32, 16–22 (2018).
Casey, B. J. et al. The adolescent brain cognitive development (ABCD) study: Imaging acquisition across 21 sites. Dev. Cognit. Neurosci. 32, 43–54 (2018).
Hagler, D. J. Jr. et al. Image processing and analysis methods for the Adolescent Brain Cognitive Development Study. Neuroimage. 202, 116091 (2019).
Acker, W. L., & Acker, C. Bexley Maudsley Automated Psychological Screening and Bexley Maudsley Category Sorting Test Manual (NFER-Nelson, for the Institute of Psychiatry, 1982).
Wechsler, D. Wechsler Intelligence Scale for Children—Fourth Edition (WISC-IV) (The Psychological Corporation, 2003).
Chaarani, B. et al. Baseline brain function in the preadolescents of the ABCD Study. Nat. Neurosci. 24(8), 1176–1186 (2021).
Luciana, M. et al. Adolescent neurocognitive development and impacts of substance use: Overview of the adolescent brain cognitive development (ABCD) baseline neurocognition battery. Dev. Cognit. Neurosci. 32, 67–79 (2018).
Gershon, R. C. et al. Language measures of the NIH toolbox cognition battery. J. Int. Neuropsychol. Soc. 20(6), 642–651 (2014).
Carlozzi, N. E. et al. NIH toolbox cognitive battery (NIHTB-CB): The NIHTB pattern comparison processing speed test. J. Int. Neuropsychol. Soc. 20(6), 630–641 (2014).
Tulsky, D. S. et al. NIH Toolbox Cognition Battery (NIHTB-CB): List sorting test to measure working memory. J. Int. Neuropsychol. Soc. 20(6), 599–610 (2014).
Dikmen, S. S. et al. Measuring episodic memory across the lifespan: NIH toolbox picture sequence memory test. J. Int. Neuropsychol. Soc. 20(6), 611–619 (2014).
Eriksen, B. A. & Eriksen, C. W. Effects of noise letters upon the identification of a target letter in a nonsearch task. Percept. Psychophys. 16(1), 143–149 (1974).
Zelazo, P. D. The Dimensional Change Card Sort (DCCS): A method of assessing executive function in children. Nat. Protoc. 1(1), 297–301 (2006).
Achenbach, T. M. The Child Behavior Checklist and related instruments. In The Use of Psychological Testing for Treatment Planning and Outcomes Assessment, 2nd (ed. Erlbaum, L.) 429–466 (Associates Publishers, 1999).
Heaton, R. K. et al. Reliability and validity of composite scores from the NIH Toolbox Cognition Battery in adults. J. Int. Neuropsychol. Soc. 20(6), 588–598 (2014).
Tanner-Eggen, C., Balzer, C., Perrig, W. J. & Gutbrod, K. The neuropsychological assessment of cognitive deficits considering measures of performance variability. Arch. Clin. Neuropsychol. 30(3), 217–227 (2015).
Iverson, G. L. & Karr, J. E. Improving the methodology for identifying mild cognitive impairment in intellectually high-functioning adults using the NIH toolbox cognition battery. Front Psychol. 12, 724888. https://doi.org/10.3389/fpsyg.2021.724888 (2021).
Clark, K. A. et al. Mean diffusivity and fractional anisotropy as indicators of disease and genetic liability to schizophrenia. J. Psychiatr. Res. 45(7), 980–988 (2011).
Kuhn, M. Building predictive models in R using the caret package. J. Stat. Softw. 28, 1–26 (2008).
Pelletier, P. M., Ahmad, S. A. & Rourke, B. P. Classification rules for basic phonological processing disabilities and nonverbal learning disabilities: Formulation and external validity. Child Neuropsychol. 7(2), 84–98 (2001).
Forrest, B. J. The utility of math difficulties, internalized psychopathology, and visual-spatial deficits to identify children with the nonverbal learning disability syndrome: Evidence for a visualspatial disability. Child Neuropsychol. 10(2), 129–146 (2004).
Semrud-Clikeman, M. & Hynd, G. W. Right hemisphere dysfunction in nonverbal learning disabilities: Social, academic, and adaptive functioning in adults and children. Psychol. Bull. 107(2), 196 (1990).
Little, S. S. Nonverbal learning disabilities and socioemotional functioning: A review of recent literature. J. Learn. Disabil. 26(10), 653–665 (1993).
Uttal, D. H., Miller, D. I. & Newcombe, N. S. Exploring and enhancing spatial thinking: Links to achievement in science, technology, engineering, and mathematics?. Curr. Direct. Psychol. Sci. 22(5), 367–373 (2013).
Van Der Maas, H. L. J. et al. A dynamical model of general intelligence: The positive manifold of intelligence by mutualism. Psychol. Rev. 113(4), 842–861. https://doi.org/10.1037/0033-295X.113.4.842 (2006).
Peng, P., Wang, T., Wang, C. & Lin, X. A meta-analysis on the relation between fluid intelligence and reading/mathematics: Effects of tasks, age, and social economics status. Psychol. Bull. 145(2), 189–236. https://doi.org/10.1037/bul0000182 (2019).
Coccaro, A. et al. Resting state dynamic reconfiguration of spatial attention cortical networks and visuospatial functioning in non-verbal learning disability (NVLD): A HD-EEG INVESTIGATION. Brain Sci. 13(5), 731. https://doi.org/10.3390/brainsci13050731 (2023).
Acknowledgements
This study was made possible thanks to a Graduate Fellowship from the Department of Developmental and Social Psychology and the Padua Neuroscience Center, University of Padua to Ambra Coccaro. Data used in the preparation of this article were obtained from the Adolescent Brain Cognitive Development (ABCD) Study (https://abcdstudy.org), held in the NIMH Data Archive (NDA). This is a multisite, longitudinal study designed to recruit more than 10,000 children age 9–10 and follow them over 10 years into early adulthood. The ABCD Study® is supported by the National Institutes of Health and additional federal partners under award numbers U01DA041048, U01DA050989, U01DA051016, U01DA041022, U01DA051018, U01DA051037, U01DA050987, U01DA041174, U01DA041106, U01DA041117, U01DA041028, U01DA041134, U01DA050988, U01DA051039, U01DA041156, U01DA041025, U01DA041120, U01DA051038, U01DA041148, U01DA041093, U01DA041089, U24DA041123, U24DA041147. A full list of supporters is available at https://abcdstudy.org/federal-partners.html. A listing of participating sites and a complete listing of the study investigators can be found at https://abcdstudy.org/consortium_members/. ABCD consortium investigators designed and implemented the study and/or provided data but did not necessarily participate in the analysis or writing of this report. This manuscript reflects the views of the authors and may not reflect the opinions or views of the NIH or ABCD consortium investigators.
Author information
Authors and Affiliations
Contributions
A.C. contributed to study conception, analyzed data, wrote the main manuscript; M.B., I.M. and M.L. contributed to study conception and to the analysis, supervised the project; All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Coccaro, A., Banich, M., Mammarella, I.C. et al. Estimating the prevalence of Non-Verbal Learning Disability (NVLD) from the ABCD sample. Sci Rep 14, 8212 (2024). https://doi.org/10.1038/s41598-024-58639-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-58639-x
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
