
Abstract
Frailty as a syndrome of physical decline in late life is associated with adverse health outcomes. Knee osteoarthritis (KOA) could contribute to frailty conditions. The objective of this study was to evaluate the impact of KOA on frailty risk in a Korean National Health and Nutrition Examination Survey (KNHANES) cohort. In this study (N, total = 11,910, age; 64.10 years old [63.94–64.27; mean 95% CI], sex (female, %); 6,752 (56.69)), KOA patients were defined as those with knee joint pain and grade 2 Kellgren–Lawrence (K–L) or more on plain radiographic images who were 40 years old or older in Korean population data of KNHANES. The frailty index was calculated using 46 items related to co-morbidities and laboratory parameters. The impact of KOA on frailty risk was evaluated with logistic regression analyses. The prevalence of KOA patients was 35.6% [95% CI 34.7–36.46]. In polytomous logistic regression, the relative risk ratio (RRR) of KOA was significantly increased in the pre-frail group (2.76, 95% CI 2.30–3.31) and the frail group (7.28, 95% CI 5.90–8.98). RRR of frailty was significantly increased in patients with K–L grade 3 (1.36, 95% CI 1.13–1.63) and K-L grade 4 (2.19, 95% CI 1.72–2.79). Older age, higher BMI, smoking status, alcohol intake, low-income status, higher WBC count, higher platelet count, higher serum creatinine level and low estimated GFR were significantly associated with increased frailty risk. High hemoglobin and regular walking habits were associated with decreased frailty risk in KOA patients. In this large observation population- based survey cohort, KOA is linked to an increased risk of frailty syndrome. We found a significant connection between KOA and frailty syndrome. These results show that we need to think about the overall health of people with KOA and give them special care to prevent frailty syndrome.
Similar content being viewed by others

Introduction
Osteoarthritis (OA) is a common chronic degenerative joint disease, resulting in a diminished ability to adapt to external stressors1,2,3. These stressors could contribute to adverse outcomes including organ damage and mortality risk called frailty syndrome4. Frailty is defined as a biologic syndrome of decreased reserve and resistance to stressors, resulting from cumulative declines across multiple physiologic systems, and causing vulnerability to adverse outcomes3,5. Frailty syndrome known as Fried's frailty phenotype is classically defined as the presence of at least 3 of 5 specific health deficits: unintentional weight loss, exhaustion, low physical activity, slow walking speed, and reduced grip strength3. Fried’s frailty phenotype is classified into three categories based on the number of frailty indicators: robust (n = 0), prefrailty (n = 1 or 2), and frailty (n = 3)3. Any frailty indexes operationalize frailty by counting deficits; the more health deficits an individual has, the frailer they will be—i.e., the more susceptible to adverse health outcomes. The frailty index, calculated as a ratio of deficits present out of the total number of possible deficits, gives a continuous score from total fitness (0) to total frailty (1)6,7.
Several study groups reported the association between the frailty syndrome and OA patients performed by the Fried’s methods. Hip OA is associated with frailty and pre-frailty in older adults in a US cohort study8. Knee OA is closely related to frailty and cognitive frailty conditions in a Thailand and US cohort study9,10.
Recently, the prevalence and clinical features of frailty syndrome in knee OA patients have been studied in several countries. Knee pain could increase the risk of developing prefrailty and frailty11,12.
The prevalence of frailty and pre-frailty is known to be high in knee OA. It is associated with aging, severe knee OA symptoms, malnutrition, physical activity, and functional dependence. The prevalence of cognitive frailty is not uncommon in community-dwelling elderly9,11,13.
However, clinical features and frailty risks in knee OA subjects based on large-scale radiographic studies have not been well reported yet. Thus, the objective of this cross-sectional study was to evaluate the impact of KOA on frailty risk in patients with knee OA patients assessed by radiographic grades in the Korean National Health and Nutrition Examination Survey (KNHANES), a large nationwide population-based survey.
Subjects and methods
Study design, setting, and participants
KNHANES was designed to monitor the health and nutritional status of Koreans since 1998. It is a nationwide cross-sectional survey conducted every year. The KNHANES data were released after anonymization. The study population was not involved in the design of this study. The KNHANES is a nation-wide surveillance system to monitor the health and nutritional status of the general population of South Korea. Each year, representative samples of approximately 10,000 people are selected. Health examination, health interview, and nutritional survey are then conducted. All data are available at https://knhanes.kdca.go.kr/knhanes. The survey was conducted after receiving written informed consent from all study participants.
The study protocol was reviewed and approved by the Institutional Review Board of the Korea Disease Control and Prevention Agency (No: 2013-12EXP-03-5C, 2018–01-03-P-A). The study was performed in accordance with the Declaration of Helsinki.
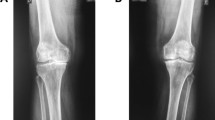
From 2010 to 2013 (i.e. KNHANES IV-1 ~ KNHANES V-3), KNHANES performed the special project for the radiographic studies of knee joints in the subjects aged 40 years and older. Knee OA patients with Kellgren-Lawrence (K-L) grade (possible grade: 0 to 4) of 2 or more (based on plain knee radiographic studies) and knee joint pain were included. We excluded the patients with rheumatoid arthritis in our data processing14.
Frailty index
We developed the frailty index using a cumulative deficit model, including symptoms, signs, abnormal laboratory values, disease status, and disabilities according to the Rockwood clinical frailty scale7. Rockwood’s frailty index was calculated as a ratio of deficits present out of the total number of possible deficits. The index gives a continuous score from total fitness (0) to total frailty (1). This means that the more deficits an individual has, the frailer they are. Our frailty index was constructed based on 46 items from the KNHANES data. These items included comorbidities, functional abilities, signs and symptoms, and laboratory values according to the Rockwood clinical frailty scale6,7. Comorbidities (46 items) included hypertension, pulse irregularity, myocardial infarction, angina pectoris, hypercholesterolemia, decreased high-density lipoprotein, hypertriglyceridemia, dyslipidemia, low vitamin D, diabetes, increased hemoglobin A1c, thyroid disease, dyspnea, bronchial asthma, chronic obstructive pulmonary disease, pulmonary tuberculosis, chronic hepatitis B, chronic hepatitis C, liver cirrhosis, renal failure, history of anemia, stroke, history of arthritis, limitation of motor function, chewing difficulty, weight loss, fatigue, the idea of suicide, decreased mobility, disability of self-care, disability of usual activities, pain/discomfort, anxiety/depressive mood, major depression, smoking status (those who had smoked 100 cigarettes or more in their whole life), current smoking (those who were currently smoking and had smoked 100 cigarettes or more in their whole life), stomach cancer, colon cancer, lung cancer, hepatic cell carcinoma, breast cancer, cervical cancer, and thyroid cancer. We classified subjects into robust (frailty index ≤ 0.10), pre-frail (0.10 < frailty index ≤ 0.21), and frail (frailty index > 0.21) groups6,7.
Statistical analysis
We analyzed the relative risk ratio (RRR; 95% CI) of frailty in control (n = 7670) and KOA subjects (n = 4240) (Fig. 1) by polytomous logistic regression. RRR was adjusted by age, sex, body mass index (BMI), smoking status, alcohol intake, low-income status, hemoglobin (Hb), hematocrit, white blood cell (WBC), platelet (PLT), blood urea nitrogen (BUN), serum creatinine, and estimated glomerular filtration rate (GFR). We analyzed clinical data in KOA subjects by analysis of covariance (ANCOVA) after adjusting for age, sex, and BMI. All statistical analyses were performed using Stata software V.16.0 (StataCorp, 4905 Lakeway Drive, College Station, Texas 77845 USA). Statistical significance was considered when the two-sided p-value was less than 0.05. The prevalence of KOA patients analyzed by estimated proportion (mean and 95% CI).

Case selection flow chart of radiographic study subjects in the Korean National Health and Nutrition Examination Survey (January 2010–December 2013) (Missing values is defined as the data value that is not stored for a variable in the observation of interest).
Results
Study patients
From 44,085 subjects, 17,873 subjects aged ≥ 40 years were chosen. A total of 5,528 patients were excluded due to missing values. After excluding 435 patients with rheumatoid arthritis patients, 11,910 individuals were finally evaluated in this study (Fig. 1). The prevalence of KOA patients was 12.50% [95% CI 11.93–13.10].
Baseline characteristics of study subjects according to three frailty groups are summarized in Table 1.
Relative risk ratios of the frailty and pre-frail group compared to the robust group
RRRs were significantly increased for those with KOA (7.28 [95% CI 5.90–8.98], p < 0.0001), age (1.07 [95% CI 1.06–1.09], p < 0.0001), female gender (2.38 [95% CI 1.71–3.30], p < 0.0001), BMI (1.16 [95% CI 1.14–1.19], p < 0.0001), smoking status (7.66 [95% CI 6.06–9.68] , p < 0.0001), low-income status (1.88 [95% CI 1.61–2.18], p < 0.0001), and WBC (1.30 [95% CI 1.24–1.36] , p < 0.0001) in the frail group compared to the robust group. Significantly decreased RRRs were observed in those with alcohol intake (0.69 [95% CI 0.59–0.81], p < 0.0001), regular walking (0.72 [95% CI 0.62–0.83], p < 0.0001), Hb (0.78 [95% CI 0.74–0.83], p < 0.0001), BUN (0.97 [95% CI 0.96–0.99] , p = 0.001), and estimated GFR (0.97 [95% CI 0.95–0.98], p < 0.0001) in the frail group compared to the robust group (Fig. 2).

The relative risk ratio of demographic and clinical parameters in pre-frailty and frailty status compared to robust status in all radiologic study subjects (N = 11,910) in Korean National Health and Nutrition Examination Survey. BMI body mass index, Hb hemoglobin, Hct hematocrit, WBC white blood cell, PLT platelet, BUN blood urea nitrogen, eGFR estimated glomerular filtration rate.
In the pre-frail group, significant increased RRRs were observed in those with KOA (2.76 [95% CI 2.30–3.31], p < 0.0001), age (1.05 [95% CI 1.04–1.06], p < 0.0001), female gender (1.53 [95% CI 1.18–1.99], p = 0.001), BMI (1.10 [95% CI 1.08–1.12], p < 0.0001), smoking status (3.50 [95% CI 3.00–4.07], p < 0.0001), low-income status (1.28 [95% CI 1.14–1.42], p < 0.0001), WBC (1.14 [95% CI 1.105–1.18], p < 0.0001). Significant decreased RRRs are observed in hemoglobin (0.92 [95% CI 0.88–0.96], p < 0.0001), BUN (0.98 [95% CI 0.97–0.99], p < 0.0001) and estimated GFR (0.98 [95% CI 0.97–0.99], p = 0.001) (Fig. 2).
RRRs of frailty were significantly increased (1.36 [95% CI 1.13–1.63]) in K-L grade 3 subjects. RRRs of prefrailty and frailty were significantly increased (1.36 [95% CI 1.12–1.66] and (2.19 [95% CI 1.72–2.79] respectively) in K-L grade 4 subjects (Fig. 3) when knee radiographic studies were analyzed.

The relative risk ratio of each Kellgren–Lawrence grade of knee joint radiography in pre-frailty and frailty status compared to the robust status. K–L grade Kellgren–Laurence grade, BMI body mass index.
In KOA subjects according to frailty status (robust, pre-frail and frail), age (mean ± SE) (66.66 ± 0.65 years old, 69.43 ± 0.30 and 71.33 ± 0.33, p < 0.001), BMI (mean ± SE) (24.13 ± 0.20 kg/m2, 25.07 ± 0.12 kg/m2, and 25.46 ± 0.16 kg/m2, p < 0.0001) were increased significantly in frailty subjects (Table 2). Smoking status, current smoking, and low-income status were also significantly increased in frailty subjects (Table 2). WBC (mean ± SE) (5.50 ± 0.11(× 103/μL), 5.94 ± 0.07 (× 103/μL) and 6.41 ± 0.09 (× 103/μL), p < 0.0001), PLT (mean ± SE) (246.03 ± 3.83 (× 103/μL), 258.13 ± 2.39 (× 103/μL) and 259.96 ± 3.35 (× 103/μL), p = 0.04), and serum creatinine (0.73 ± 0.01 mg/dL, 0.76 ± 0.01 mg/dL and 0.86 ± 0.02 mg/dL, p < 0.0001) were significantly increased in those with a frailty status (robust, pre-frail and frail) (Table 2). However, Hb (13.53 ± 0.09 g/dL, 13.51 ± 0.05 g/dL and 13.27 ± 0.07 g/dL, p = 0.01) and estimated GFR (CKD-EPI equation) (88.54 ± 0.90 ml/min, 83.89 ± 0.51 ml/min and 76.22 ± 0.72 ml/min, p < 0.0001) were significantly decreased in those with a frailty status (robust, pre-frail and frail) (Table 2).
In addition, we studied serum iron profiles (mean ± SE) in the dataset from 2010 to 2012. It was found that serum iron was decreased in frailty subjects (robust, pre-frail and frail) with KOA (robust, prefrail, and frail) (104.05 ± 3.20 μg/dL, 104.76 ± 1.57 μg/dL and 96.57 ± 1.77 μg/dL, p = 0.0001). Serum ferritin was increased in frailty subjects (robust, pre-frail and frail) with KOA (79.10 ± 6.96 μg/mL, 79.86 ± 3.36 μg/mL and 86.34 ± 4.23 μg/mL, p < 0.0001). Moreover, serum total iron-binding capacity (TIBC) was increased in frailty subjects (robust, pre-frail and frail) with KOA (305.03 ± 3.48 μg/mL, 311.33 ± 1.89 μg/mL and 315.04 ± 2.26 μg/mL, p < 0.0001). These results suggest iron deficiency anemia might be related to frailty status in KOA. The regular walking habit was defined as walking for more than 30 min at a time more than five times a week. The RRR of regular walking habits revealed significant a negative correlation with frailty syndrome (0.72 [95% CI: 0.62–0.83], p < 0.0001) (Fig. 2).
Discussion
In general, decreased BMI is a main feature of the frailty syndrome. This may lead to worsening nutritional status and a decrease in muscle mass, resulting in weight loss and muscle weakness, which are two common indicators of frailty syndrome. Increased BMI is related to the weight-bearing stress and an increased risk of knee osteoarthritis15. Our results revealed that increased RRR of BMI was associated with frailty in knee OA patients (Fig. 2), consistent with a previous study16. In our study, it can be observed that the frequency of normal weight group (Table 1) in the frailty group decreases compared to the robust and pre-frail groups, and that of the overweight group increases relatively. Also, overall distribution of the study subjects according to K-L grade, the frailty status and the BMI status show that the BMI is increased in the frailty group as the K-L grade increases. But that of the overweight group increases as the K-L grade increases (Supplement Fig. 1). These results could show the features of the survived frailty subjects in this study data.
Another previous study has reported that sarcopenic obesity is more closely associated with knee OA than nonsarcopenic obesity13. Sarcopenia may be the common denominator of knee OA and frailty syndrome. Sarcopenic obesity is more closely associated with knee OA than nonsarcopenic obesity, although both groups have equivalent body weights17. This finding supports the importance of the systemic metabolic effect of sarcopenia and sarcopenic obesity on knee OA13,16,17,18. These results suggest that different pathogenesis in knee OA can contribute to the development of frailty syndrome. We cannot analyze the sarcopenia or the sarcopenic obesity by muscle mass or body composite because the data are not available of our analysis dataset.
Kanapuru et al. have reported that lower muscle mass might be a risk factor for knee pain in patients with radiographically mild knee OA, but not in those with radiographically severe OA19. In women, high fat mass and low lower extremity muscle mass are associated with the presence and severity of knee OA20. Lower extremity muscle mass is more closely correlated with knee OA than obesity in women20.
Our results showed leukocytosis and thrombocytosis in KOA were accompanied by the frailty syndrome (Table 2). Furthermore, we observed an increased risk of frailty syndrome related to leukocytosis in KOA (Fig. 2). Previous studies have also reported that leukocytosis, C-reactive protein, and IL-6 levels are associated with normal aging, sarcopenia, and late-life disease (such as cardiovascular diseases)19. Lohman et al. have reported the importance of obesity and increased dietary inflammatory index (DII) in frailty subjects21,22. It has been suggested that inflammatory pathways and disordered coagulation play a role in the pathology of frailty19.
We hypothesized that frailty might also drive OA development by creating an inflammatory environment to interfere with normal tissue health. Molecular and biochemical changes associated with OA might in turn promote frailty, resulting in an exorable deterioration of the joint. Therefore, frailty might be considered an additional risk factor for the development of OA.
Increased serum creatinine and decreased estimated GFR (CKD-EPI equation) reflect a decreased renal function in KOA patients with frailty syndrome (Table 2). Thus, the use of renal toxic agents such as nonsteroidal anti-inflammatory drugs (NSAID) should be cautious in these patients.
Our results revealed that the frequency of regular walking had negative correlations with frailty syndromes (Fig. 2). Our results suggest the need for a long-term, adequately powered, and randomized controlled trial of exercise interventions in knee OA patients for the treatment of frailty in the elderly. Such evidence will greatly support the future design of preventive strategies against disability in older persons.
Conclusion
In this cross-sectional population-based survey cohort, KOA is associated with an increased risk of frailty syndrome. The high K-L grade of KOA is significant the high risk of the frailty syndrome. The patients who had KOA with frailty syndrome are observed increased BMI.
Data availability
The data that support the findings of this study are available from the Korean National Health and Nutrition Examination Survey (KNHANES) but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data are however available from the corresponding authors upon reasonable request and with permission of KNHANES. The data for this study were accessed through the KNHANES homepage (https://knhanes.kdca.go.kr/knhanes/eng/index.do).
References
Salaffi, F., Farah, S. & Di Carlo, M. Frailty syndrome in rheumatoid arthritis and symptomatic osteoarthritis: An emerging concept in rheumatology. Acta Biomed. 91, 274–296. https://doi.org/10.23750/abm.v91i2.9094 (2020).
Salaffi, F., Di Carlo, M., Carotti, M., Farah, S. & Giovagnoni, A. Frailty prevalence according to the survey of health, ageing and retirement in Europe-Frailty Instrument (SHARE-FI) definition, and its variables associated, in patients with symptomatic knee osteoarthritis: Findings from a cross-sectional study. Aging Clin. Exp. Res. https://doi.org/10.1007/s40520-020-01667-0 (2020).
Fried, L. P. et al. Frailty in older adults: Evidence for a phenotype. J. Gerontol. A Biol. Sci. Med. Sci. 56, M146-156. https://doi.org/10.1093/gerona/56.3.m146 (2001).
O’Brien, M. S. & McDougall, J. J. Age and frailty as risk factors for the development of osteoarthritis. Mech. Ageing Dev. 180, 21–28. https://doi.org/10.1016/j.mad.2019.03.003 (2019).
Castell, M. V. et al. Osteoarthritis and frailty in elderly individuals across six European countries: Results from the European Project on OSteoArthritis (EPOSA). BMC Musculoskelet. Disord. 16, 359. https://doi.org/10.1186/s12891-015-0807-8 (2015).
Blodgett, J., Theou, O., Kirkland, S., Andreou, P. & Rockwood, K. Frailty in NHANES: Comparing the frailty index and phenotype. Arch. Gerontol. Geriatr. 60, 464–470. https://doi.org/10.1016/j.archger.2015.01.016 (2015).
Kang, M. G. et al. Association between frailty and hypertension prevalence, treatment, and control in the elderly korean population. Sci. Rep. 7, 7542. https://doi.org/10.1038/s41598-017-07449-5 (2017).
Wise, B. L. et al. Frailty and hip osteoarthritis in men in the MrOS cohort. J. Gerontol. A Biol. Sci. Med. Sci. 69, 602–608. https://doi.org/10.1093/gerona/glt126 (2014).
Wanaratna, K., Muangpaisan, W., Kuptniratsaikul, V., Chalermsri, C. & Nuttamonwarakul, A. Prevalence and factors associated with frailty and cognitive frailty among community-dwelling elderly with knee osteoarthritis. J. Commun. Health 44, 587–595. https://doi.org/10.1007/s10900-018-00614-5 (2019).
Misra, D. et al. Knee osteoarthritis and frailty: Findings from the multicenter osteoarthritis study and osteoarthritis initiative. J. Gerontol. A Biol. Sci. Med. Sci. 70, 339–344. https://doi.org/10.1093/gerona/glu102 (2015).
Bindawas, S. M., Vennu, V. & Stubbs, B. Longitudinal relationship between knee pain status and incident frailty: Data from the osteoarthritis initiative. Pain Med. 19, 2146–2153. https://doi.org/10.1093/pm/pnx296 (2018).
Veronese, N. et al. Pain increases the risk of developing frailty in older adults with osteoarthritis. Pain Med. 18, 414–427. https://doi.org/10.1093/pm/pnw163 (2017).
Yoshimura, N. et al. Prevalence and co-existence of locomotive syndrome, sarcopenia, and frailty: The third survey of research on osteoarthritis/osteoporosis against disability (ROAD) study. J. Bone Miner. Metab. 37, 1058–1066. https://doi.org/10.1007/s00774-019-01012-0 (2019).
Kellgren, J. H. & Lawrence, J. S. Radiological assessment of osteo-arthrosis. Ann. Rheum. Dis. 16, 494–502. https://doi.org/10.1136/ard.16.4.494 (1957).
Blagojevic, M., Jinks, C., Jeffery, A. & Jordan, K. P. Risk factors for onset of osteoarthritis of the knee in older adults: A systematic review and meta-analysis. Osteoarthr. Cartil. 18, 24–33. https://doi.org/10.1016/j.joca.2009.08.010 (2010).
Han, C. D., Yang, I. H., Lee, W. S., Park, Y. J. & Park, K. K. Correlation between metabolic syndrome and knee osteoarthritis: Data from the Korean National Health and Nutrition Examination Survey (KNHANES). BMC Public Health 13, 603. https://doi.org/10.1186/1471-2458-13-603 (2013).
Lee, S., Kim, T. N. & Kim, S. H. Sarcopenic obesity is more closely associated with knee osteoarthritis than is nonsarcopenic obesity: a cross-sectional study. Arthritis Rheum. 64, 3947–3954. https://doi.org/10.1002/art.37696 (2012).
Kim, Y. S. et al. Prevalence of sarcopenia and sarcopenic obesity in the Korean population based on the Fourth Korean National Health and Nutritional Examination Surveys. J. Gerontol. A Biol. Sci. Med. Sci. 67, 1107–1113. https://doi.org/10.1093/gerona/gls071 (2012).
Kanapuru, B. & Ershler, W. B. Inflammation, coagulation, and the pathway to frailty. Am. J. Med. 122, 605–613. https://doi.org/10.1016/j.amjmed.2009.01.030 (2009).
Park, H. M. et al. Decreased muscle mass is independently associated with knee pain in female patients with radiographically mild osteoarthritis: A nationwide cross-sectional study (KNHANES 2010–2011). Clin. Rheumatol. 37, 1333–1340. https://doi.org/10.1007/s10067-017-3942-9 (2018).
Resciniti, N. V., Lohman, M. C., Wirth, M. D., Shivappa, N. & Hebert, J. R. Dietary inflammatory index, pre-frailty and frailty among older US adults: Evidence from the national health and nutrition examination survey, 2007–2014. J. Nutr. Health Aging 23, 323–329. https://doi.org/10.1007/s12603-019-1164-3 (2019).
Lohman, M. C., Resciniti, N. V., Wirth, M. D., Shivappa, N. & Hebert, J. R. Obesity, dietary inflammation, and frailty among older adults: Evidence from the national health and nutrition examination survey. J. Nutr. Gerontol. Geriatr. 38, 18–32. https://doi.org/10.1080/21551197.2018.1552226 (2019).
Acknowledgements
This work was partly supported by the National Resarch Foundation of Korea (NRF) grants funded by the Korea govorment (MSIT; Ministry of Science and ICT) (NRF-2022R1A2C2091831).
Author information
Authors and Affiliations
Contributions
S.J., J.S. contributed to the study design, data interpretation, and writing of the paper. K.S., M.K. contributed to the study design and data interpretation. J.L. contributed to the study design, data interpretation and analysis. As the corresponding author, Y.S. had full access to all the data in the study and was responsible for the decision.to submit this manuscript for publication. All authors reviewed the manuscript. S.J., J.S. contributed equally in this study.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Joo, S.H., Song, J.W., Shin, K. et al. Knee osteoarthritis with a high grade of Kellgren–Lawrence score is associated with a worse frailty status, KNHANES 2010–2013. Sci Rep 13, 19714 (2023). https://doi.org/10.1038/s41598-023-46558-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-023-46558-2
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
