
Abstract
Amyotrophic lateral sclerosis (ALS) is a neurodegenerative rare disease characterized by symptoms and signs in the upper and lower motor neurons, leading to progressive neuro-degeneration and muscle atrophy. Our objective was to analyse the quality of life (QoL) in patients with ALS and compare with general population and with patients with cancer. Prospective study from consecutive ALS patients in one center. In order to assess quality of life, during the first visit three questionnaires were administered: Amyotrophic Lateral Sclerosis Functional Rating Scale (ALSFRS-R), Short Form-36 (SF-36) and EuroQoL 5D (EQ-5D). We compared SF-36 of ALS patients with a reference population (n = 9151), and we compared the EQ-5D index score of ALS patients versus patients with cancer in the same area and in the same period (2015–2018). Between June 2015 and September 2017, 23 were included. The mean age was 65.1 ± 12.6 years and 56.5% were women. Compared with the general population, patients with ALS showed lowest QoL (p < 0.05) in all the dimensions, with a very important impairment in physical function (median: 0; p25-75: 0–10) and physical role (median: 0; p25-75: 0–6.25). In EQ-5D questionnaire, patients with ALS presented an EQ-5D index score of 0.21 ± 0.39 (mean ± standard deviation) with a visual analog scale (VAS) score of 0.32 ± 0.24. Compared with an oncological population, patients with ALS had a worse EQ-5D index score both clinically and statistically (0.21 ± 0.39 vs. 0.77 ± 0.27; p < 0.05). We demonstrate a poorer quality of life in patients with ALS is poor, and clinically and statistically worse than in patients with cancer or general population. New studies need to evaluate the impact of strategies in this population to improve the quality of life.
Similar content being viewed by others

Introduction
Amyotrophic lateral sclerosis (ALS) is a rare neurodegenerative disease with a worldwide incidence of 0.6 and 3.8 per 100, 000 person-years1, 2. ALS is characterized by symptoms and signs of the upper and lower motor neurons, leading to progressive neuro-degeneration and muscle atrophy3. This disease also has a huge impact in the quality of life (QoL) of patients and caregivers4,5,6. Nowadays, one of the aims in patients with ALS is to improve the QoL. The QoL questionnaires are tools that quantify the health-related quality of life. These questionnaires can be generic or specific for a disease and require adaptation and validation. ALS affects the QoL of patients, although the real knowledge of the impact of the disease could be better interpreted if we compare their results with general population and with other well-known diseases. For that reason, we aimed to analyse the QoL in patients with ALS and compare with general population and with patients with cancer.
Material and methods
This is a secondary analysis from a prospective study that evaluated the incidence of venous thromboembolism in ALS patients. The rationale, design and main results of the study were published previously7. The study was approved by the Ethical Committee of the center according to the Spanish Regulatory Authorities (0795-N-14), and each patient provided written informed consent. This work was conducted as per the principles of the Declaration of Helsinki and ICH Guidelines for Good Clinical Practice. All study documents were prepared according to Good Clinical Practice guidelines (CPMP/ICH/135/95). Individual data elements were purposely obtained for this study, anonymized and protected according to the European Union directive 2016/679 of the European Parliament and the European Council, of April 27, 2016. Briefly, consecutive patients with ALS were evaluated followed every 3 months until completing 2 years of follow up. Demographic data and comorbidities were recorded. The objective of this study was to evaluate the QoL in patients with ALS and compare QoL between ALS with two cohort (patients with cancer and general population).
Consecutive patients with ALS according to El Escorial criteria (clinically definite or probable ALS)8, with age > 18 years and with no previous anticoagulant treatment or with previous venous thromboembolism were enrolled from June 2015 to September 2017. In order to assess quality of life, during the first visit, three questionnaires were administered (caregivers helped patients to fill it in when necessary): Amyotrophic Lateral Sclerosis Functional Rating Scale (ALSFRS-R)9, Short Form-36 (SF-36)10 and EuroQoL 5D (EQ-5D)11, 12. ALSFRS-R is a specific questionnaire for ALS validated in Spanish in 20109. This scale is an instrument to measure the progression of the disease in patients with ALS and that assesses the degree of patient´s immobility, the existence and degree of hypersalivation and bulbar involvement where lower scores indicate poorer function. The questionnaires SF-3610 and EQ-5D11, 12 are two generic quality-of-life questionnaires which will allow us to compare the ALS QoL with other groups. SF-36 scale, it’s available and validated in Spanish and reference values are available from the general population10. This questionnaire evaluates 36 items with 8 different dimensions: physical situation, physical role, body pain, general health, vitality, social function, emotional role, and mental health. EQ-5D is a health questionnaire develop by the EuroQol Group which allow to compare different diseases11, 12. This questionnaire allows the calculation of a utility index (UI), which comprises 5 different areas (mobility, self-care, daily activities, pain/discomfort, and anxiety/depression), with a score between 1 (without problem) to 5 (unable to/extreme problems). The responses are combined to obtain a 5-digit number (from 11,111 to 55,555) that summarizes the patient’s health status. This value is subsequently converted into the UI, which may range from 0.208 (worst possible health) to 1.000 (best possible health). The minimally important difference (MID) on the EQ-5D questionnaire for patients with malignancies is 0.06–0.08 UI13.
Statistical analysis
For each QoL questionnaire, the distributions of scores, means, medians, range and standard deviation are presented. In this study, SF-36 questionnaire score was compared with a reference population using a population study performed in 9151 persons older than 18 years old10. Due to the social and media impact of cancer, we decided to compare the EQ-5D index score of ALS patients with patients with cancer (n = 249), taking reference to the work made in the same hospital and same period (2015–2018) by our group14. Statistical significance was considered when p value was < 0.05. Box Plots depicts the median (black line inside the box) and the interquartile range (the edges of the box). Statistical calculations were performed using SPSS, version 20.0 (SPSS Inc. 233 South Wacker Drive, 11th Floor Chicago, IL).
Ethics approval
Study protocol has been approved by the Ethics Committee of Virgen del Rocio Hospital, authorization number 0795-N-14, for protection of human beings involved in biomedical research. All patients provided written consent.
Results
Between June 2015 and September 2017, 44 patients were evaluated, of whom 23 were included in the analysis of QoL. Comparison between clinical characteristics of patients who were included vs. not included is in eTable Supplement 1. In brief, patients who did not participate in the study had similar characteristics although they were younger, with more non-invasive ventilation, supplemental oxygen, cough assist and reduce mobility and wheelchair.
Of 23 patients, mean age was 65.1 ± 12.6 years and 56.5% were women. The median duration of symptom until evaluation was 32.4 months (p25–75: 10.3–47). More than half (60.9%) had reduced mobility and 34.8% needed wheelchair. Out of all the patients studied, 8 presented both spinal and bulbar involvement, while 15 had only spinal involvement (3 of them presenting as flail arms). Two patients had familial ALS, and 19 had sporadic ALS. The functional and clinical status measured by ALSFRS-R questionnaire showed a median of 36 points (p25–p75: 28–38.75) (Table 1). Patients (n = 15) received a disability pension, with the distribution as follows: less than 800 euros per month (n = 1), 800–1500 euros per month (n = 3), and more than 1500 euros per month (n = 11). We obtained data about caregivers for 14 patients, and the relationships were as follows: husband and children (n = 3), wife and children (n = 3), wife (n = 3), nursing home (n = 2), husband (n = 1), children (n = 1), and mother (n = 1). Of all the patients evaluated in our unit, 10 patients (43.5%) were referred to the mental health unit for assessment of anxiety and/or depression. Before being evaluated by the mental health unit, only 4 patients (17.4%) were taking treatment for anxiety and/or depression, and after being evaluated, 11 patients (47.8%) received treatment.
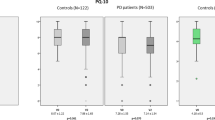
Regarding the SF-36 questionnaire, the median of the physical and mental component was 23.3 (range: 10.7) and 36.5 (range: 51.63), respectively (Fig. 1). When compared with the general population a statistical difference was observed (p < 0.05) in all the dimensions, with a very important impairment in physical function (median: 0; p25–75: 0–10) and physical role (median: 0; p25–75: 0–6.25) (Table 2, Fig. 1). Likewise, in the EQ-5D questionnaire, patients with ALS presented an EQ-5D index score of 0.21 ± 0.39 (mean ± standard deviation) with a visual analog scale (VAS) score of 0.32 ± 0.24. Compared with patients with cancer, patients with ALS had a worse EQ-5D index score both clinically and statistically significant (0.21 ± 0.39 vs. 0.77 ± 0.27; p < 0.05) (Table 2).

Box Plots of SF-36 in patients with amyotrophic lateral sclerosis. The bottom and the top of the box represent first and third quartile, respectively. The line in the center of the box is the median. The extreme of the whisker represents minimum and maximum. Outliers are plotted as individual asterisk.
Discussion
This prospective study showed that ALS is a neurodegenerative disease that significantly affects quality of life. The quality of life of patients with ALS is statistically and clinically worse than in patients with cancer and worse than the general population. Similar studies have addressed this topic although this impact in quality of life were not compared with other disease. A prospective study conducted in 2017 in 23 patients with ALS15 showed that as the disease progresses, the quality of life and functionality of the patients deteriorates. Likewise, a longitudinal prospective study in 36 patients with ALS14 showed the importance of motor disability and its relationship with psycho-emotional pathology such as depression and anxiety.
Our work has several strengths. First, we have collected data about all patients evaluated which allows us to identify different characteristics between the patients who entered in the study versus those who did not participate, which adds value to the internal and external validity of the results. Moreover, patients that decided not to participate in QoL study had more reduce mobility and wheelchair, which probably implies worse quality of life what indicates that our results overestimated quality of life in this population. Second, this study compared QoL in patients with ALS with other population (general population and patients with cancer) which allow us to evaluate the real impact of QoL in ALS.
Regarding limitations of the study. First, we acknowledge the limitation of our small sample size when compared to the number of patients recruited in studies conducted on other pathologies. However, it is crucial to consider that ALS is a rare disease, and the number of patients included in our study is proportionate to what is expected in a reference unit in ALS. Second, it would be interesting to gather data from other tests, such as the Edinburgh Cognitive and Behavioural ALS Screen (ECAS)16, specific questionnaires to evaluate anxiety or depression, or the Milano-Torino Staging (MiToS)17. However, most of these questionnaires are tedious, and patients often become exhausted when completing multiple assessments. We considered the possibility that conducting several tests might discourage patient or family member participation in the study due to the time required. Assessing of these questionnaires and a larger sample size would have allowed us to evaluate variables associated with a worse quality of life. Third, in order to be able to compare several populations, it would have been more appropriate, from a methodological point of view, to evaluate the QoL questionnaires at the same time, and in the context of the same study. Even so, the population with cancer used to compare the QoL came from the same center and was carried out in a similar period.
Conclusions
Quality of life in patients with ALS is poor, and clinically and statistically worse than in patients with cancer or general population. Several strategies should be implemented improve the quality of life of patients with ALS and new studies that evaluate the impact of each of the measures adopted in this population should be done.
Data availability
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- ALS:
-
Amyotrophic lateral sclerosis
- VTE:
-
Venous thromboembolism
- QoL:
-
Quality of life
- EQ-5D:
-
EuroQoL 5D
- PE:
-
Pulmonary embolism
- EFNS:
-
European Federation of Neurological Societies
- HRQoL:
-
Health-related quality of life
- FVC:
-
Forzed vital capacity
- US:
-
Ultrasonography
- V/Q:
-
Ventilation/perfusion
- CT:
-
Computerized tomography
- ALSFRS-R:
-
Amyotrophic Lateral Sclerosis Functional Rating Scale
- SF-36:
-
Short Form-36
- UI:
-
Utility index
- MID:
-
Minimally important difference
- CI:
-
Confidence interval
- VAS:
-
Visual analog scale
References
Longinetti, E. & Fang, F. Epidemiology of amyotrophic lateral sclerosis: An update of recent literature. Curr. Opin. Neurol. 32(5), 771. https://doi.org/10.1097/WCO.0000000000000730 (2019).
Groft, S. C., Posada, M. & Taruscio, D. Progress, challenges, and global approaches to rare diseases. Acta Paediatr. https://doi.org/10.1111/apa.15974 (2021).
Andersen, P. M. et al. EFNS guidelines on the Clinical Management of Amyotrophic Lateral Sclerosis (MALS)—revised report of an EFNS task force. Eur. J. Neurol. 19(3), 360–375. https://doi.org/10.1111/j.1468-1331.2011.03501.x (2012).
Neudert, C., Wasner, M. & Borasio, G. D. Patients’ assessment of quality of life instruments: A randomised study of SIP, SF-36 and SEIQoL-DW in patients with amyotrophic lateral sclerosis. J. Neurol. Sci. 191(1–2), 103–109. https://doi.org/10.1016/S0022-510X(01)00612-8 (2001).
Gauthier, A. et al. A longitudinal study on quality of life and depression in ALS patient-caregiver couples. Neurology 68(12), 923–926. https://doi.org/10.1212/01.wnl.0000257093.53430.a8 (2007).
Galvin, M., Gavin, T., Mays, I., Heverin, M. & Hardiman, O. Individual quality of life in spousal ALS patient-caregiver dyads. Health Qual. Life Outcomes. https://doi.org/10.1186/s12955-020-01551-5 (2020).
Caballero-Eraso, C. et al. Venous thromboembolism in amyotrophic lateral sclerosis. A prospective quasi-experimental study. Thromb. Res. 211, 81–84. https://doi.org/10.1016/J.THROMRES.2022.01.002 (2022).
Brooks, B. R., Miller, R. G., Swash, M. & Munsat, T. L. El Escorial revisited: Revised criteria for the diagnosis of amyotrophic lateral sclerosis. Amyotroph. Lateral Scler. 1(5), 293–299. https://doi.org/10.1080/146608200300079536 (2000).
Campos, T. S. et al. Spanish adaptation of the revised Amyotrophic Lateral Sclerosis Functional Rating Scale (ALSFRS-R). Amyotroph. Lateral Scler. 11(5), 475–477. https://doi.org/10.3109/17482968.2010.489115 (2010).
Alonso, J., Prieto, L. & Antó, J. M. The Spanish version of the SF-36 Health Survey (the SF-36 health questionnaire): An instrument for measuring clinical results. Med. Clin. 104(20), 771–776 (1995).
Group TE. EuroQol—A new facility for the measurement of health-related quality of life. Health Policy 16(3), 199–208. https://doi.org/10.1016/0168-8510(90)90421-9 (1990).
Carr-Hill, R. A. Health related quality of life measurement—Euro style. Health Policy 20(3), 321–328. https://doi.org/10.1016/0168-8510(92)90164-7 (1992).
Simon, A. S., Neary, M. P. & Cella, D. Estimation of minimally important differences in EQ-5D utility and VAS scores in cancer. Health Qual. Life Outcomes. https://doi.org/10.1186/1477-7525-5-70 (2007).
Marin-Barrera, L. et al. A case-control analysis of the impact of venous thromboembolic disease on quality of life of patients with cancer: Quality of life in cancer (QCA) study. Cancers https://doi.org/10.3390/cancers12010075 (2020).
Martínez-Campo, Y. et al. Observational study of patients in Spain with amyotrophic lateral sclerosis: Correlations between clinical status, quality of life, and dignity. BMC Palliat Care. https://doi.org/10.1186/s12904-017-0260-6 (2017).
Abrahams, S., Newton, J., Niven, E., Foley, J. & Bak, T. H. Screening for cognition and behaviour changes in ALS. Amyotroph Lateral Scler. 15, 9–14. https://doi.org/10.3109/21678421.2013.805784 (2014) (Epub 2013 Jun 19).
Chiò, A., Hammond, E. R., Mora, G., Bonito, V. & Filippini, G. Development and evaluation of a clinical staging system for amyotrophic lateral sclerosis. J. Neurol. Neurosurg. Psychiatry. 86(1), 38–44. https://doi.org/10.1136/jnnp-2013-306589 (2015).
Funding
This study was supported by Neumosur (association of pulmonology and thoracic surgery of southern Spain). This association fund the database and statistical analyses. They do not participate in decisions regarding collected data, analyses, article writing and submission. The code of the funding is 1/2014.
Author information
Authors and Affiliations
Contributions
L.J.P. have full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis; Study concept and design: L.J.P., C.C.E.; Acquisition, analysis, or interpretation of data: All authors; Drafting of the manuscript: All authors; Critical revision of the manuscript for important intellectual content: All authors; Statistical analysis: L.J.P.; Study supervision: L.J.P., C.C.E. All patients provided written consent. All authors provided consent to publication.
Corresponding author
Ethics declarations
Competing interests
LJP has received honoraria for presentations from Bayer Hispania, Actelion, Pfizer, Rovi, LEO Pharma, Daiichi Sankyo grants, personal fees and non-financial support from LEO Pharma, Menarini, MSD, and Roche. The rest of authors declare no conflict of interest.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Caballero-Eraso, C., Carrera-Cueva, C., de Benito Zorrero, E. et al. Prospective study to evaluate quality of life in amyotrophic lateral sclerosis. Sci Rep 13, 12074 (2023). https://doi.org/10.1038/s41598-023-39147-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-023-39147-w
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
