
Abstract
A systematic analysis of the mortality of immigrant residents throughout Italy has never been carried out. The present study aimed to evaluate differences in mortality by immigrant status. A longitudinal study of the Italian resident population (native and immigrants) recorded in the 2011 National Institute of Statistics Census was conducted. This cohort was followed up from 2012 to 2018 until death, emigration, or end of the study period. The exposure variable was the immigrant status, measured through citizenship, dichotomized into Italian and immigrant. The main outcome was overall and cause-specific mortality. Age-standardized mortality ratios (SMRs) were calculated. The SMRs among immigrants were half that of Italians, both for men (SMR 0.52) and women (SMR 0.51), with the lowest SMRs observed for subjects from North Africa and Oceania. For some causes of death, mortality was higher among immigrants: tuberculosis in both men (SMR 4.58) and women (SMR 4.72), and cervical cancer (SMR 1.58), complications of pregnancy, childbirth, and puerperium (SMR 1.36), and homicide (SMR 2.13) for women. A multivariable quasi-Poisson regression analysis, adjusted for age and macro area of residence in Italy, confirmed a lower all-cause mortality for immigrants compared to Italians, both for men (RR 0.46) and women (RR 0.44). Although immigration to Italy is no longer a recent phenomenon, and the presence of immigrants is acquiring structural characteristics, our study confirms their health advantage, with a lower mortality than that of Italians for almost all causes of death and for all areas of origin.
Similar content being viewed by others


Introduction
Many studies have found that immigrants generally have a lower all-cause mortality rate than natives, despite their lower socioeconomic status, a factor associated with poor health status, and their poorer living conditions1,2,3,4,5.
This issue represents an epidemiological paradox that has been typically explained in two ways.
The first explanation, the “healthy-migrant effect,” is based on the hypothesis that, due to the selective migration flows of healthy young people, migrants are healthier than the native people both of the country of origin and of the country of destination1,2,6,7.
The second is the so-called “salmon bias effect,” based on the hypothesis that older, unhealthy immigrants return to their country of origin for “the compulsion to die in one’s birthplace”1,8,9,10,11. In such a case, if deaths occurring in their country of origin are not registered in the mortality statistics of the country of residence, this may result in an artificially low immigrant mortality rate1,7,10,11. Furthermore, the fact that immigrants who returned to their country of origin remain in the demographic registers may determine an overcoverage of this population, meaning that the denominators are artificially inflate. This contributes to explaining the migrant mortality paradox, in particular at peak migration ages13,14,15.
Previous Italian studies found that immigrants showed a lower risk of mortality compared to Italians2,16. A recent study, which investigated the potential contribution of salmon bias effect in Italy, confirmed this finding; an underreporting of the deaths of immigrants who died abroad without an official residence change was observed. However, it was not enough to explain the large difference in mortality rates between immigrants and natives, probably confirming the relevance of the healthy migrant effect2,13,15,16,17,18.
Italy is a country with a short history of immigration, with a significant increase in the number of immigrants since the beginning of twenty-first century, in particular those coming from high migratory pressure countries. The number has doubled in the last 15 years, from 2.4 million people (4.1% of the resident population) in 2005 to 5.0 million (8.5%) in 202019.
Few studies have been published on immigrant mortality in Italy2,16,17,20,21. To our knowledge, only two studies used a longitudinal approach2,17, but one of these was limited to the cohorts of residents of two cities, Turin and Reggio Emilia2.
A longitudinal approach in studies aimed at evaluating differences in mortality between immigrants and natives is useful because immigrants in host countries tend to lose their initial health advantage due to the ageing of the first cohorts, to the cultural and linguistic barriers in accessing health care, and to the acculturation process, leading immigrants to experience life conditions and behaviors similar to those of natives in the lower socioeconomic positions2,22,23.
As great variability in mortality among immigrants by ethnic group, area of residence in the host country, age, cause of death, and length of stay has been observed22,24,25,26,27, a study conducted on a nationwide basis may provide an exhaustive description of these factors.
A systematic analysis of the mortality of immigrants resident throughout Italy has never been carried out. The present study, based on the follow-up of the Italian population recorded in the 2011 Census, aimed to evaluate the differences in mortality by immigrant status in Italy.
Methods
Data sources, study population and design
The study adopted a longitudinal design in which the Italian population recorded in the 2011 Census was considered as the initial cohort. The cohort was conceived within the project "Socioeconomic differences in mortality" (IF IST 2646), as part of the National Statistical Program (PSN), approved by the Italian Data Protection Authority. The database developed by the Italian National Institute of Statistics (Istat) for this project permitted studying the differences in life expectancy and mortality (total and by cause) according to different demographic and socioeconomic characteristics observed in the 15th Census of Population and Housing (2011)28.
The individuals recorded in the 2011 Census and resident in Italy were followed up from 2012 to 2018, until death, emigration, or end of the follow-up, whichever came first, yielding a maximum of 7 years of follow-up. Information on mortality was retrieved from the Causes of Death Register, which annually collects all deaths occurring in Italy, while the Resident Population Register was used to identify any exit from the cohort for emigration. A record linkage, using the fiscal code (a unique personal identification number issued to all residents in Italy at birth or upon request) as linkage key, connected all the archives. The reliability of the fiscal code was very high in all the registers, making it possible to link 97.1% of all deaths among the Census population occurring in Italy in the period 2012–201429. Since there is no reason to believe that the reliability of the fiscal code reported in all registers decreased over the subsequent years, the performance of the record linkage was expected to be equally high.
Istat released a fully anonymised database for this study containing the number of deaths and person-years for the population strata defined through all the variables that were used for the analyses.
Exposure
We considered as exposure immigration status, measured through citizenship, dichotomized in Italian and foreign. All the residents in Italy without Italian citizenship (including stateless) were considered as immigrants. In Italy, immigrants can obtain citizenship by marriage or by application after a period ranging between 3 and 10 consecutive years of legal residence. Moreover, children born in Italy to foreign parents can obtain citizenship after their 18th birthday. For all of these reasons, we considered citizenship the best proxy of immigrant status in Italy, rather than country of birth, at least to assess the most recent immigrations2,30.
Outcome
The present study considered as the main outcome the deaths occurring between 2012 and 2018 in the study population. Overall mortality was analyzed, with a focus on specific causes. The causes of death were classified according to the 10th revision of the International Classification of Diseases and Related Health Problems (ICD-10). Istat has adopted ICD-10 since 2003. Following updates were taken into account in the selection of the causes of death considered for the present analysis. The complete list of causes considered with ICD-10 codes is provided in the “Appendix”2.
Other factors
We considered as potential confounders of the association between citizenship and mortality other demographic and socioeconomic characteristics of the population recorded in the Census: age at death, sex, area of residence in Italy, and area of origin.
Age at death was categorized in six classes (< 15, 15–29, 30–44, 45–64, 65–74, 75 + years old).
The geographic area of residence was categorized on the basis of the classification in five broad areas (macro areas) defined by Istat: North-West (Piedmont, Valle d’Aosta, Lombardy, Liguria), North-East (Trentino-Alto Adige, Veneto, Friuli-Venetia Giulia, Emilia-Romagna), Centre (Tuscany, Umbria, Marche, Latium), South (Abruzzo, Molise, Campania, Apulia, Basilicata, Calabria), and Islands (Sicily and Sardinia).
Countries of origin were categorized as follows, according to the ISTAT classification31, that was partially modified grouping some macro areas: European Union (before 2004), Central-Eastern Europe, other European countries, North Africa, Sub-Saharan Africa, North America, Central-South America, Central-West Asia, East Asia, Oceania, stateless.
Statistical analysis
Baseline sociodemographic characteristics of the cohorts (person years, deaths) were described separately for Italians and immigrants, and the p-value of the differences in the proportion of deaths between the two groups were calculated using Chi-square method.
Crude mortality rates per 100,000 person years were calculated by citizenship, sex, area of origin, and cause of death.
To investigate mortality patterns by area of origin and by cause of death, given the small numbers in some mortality strata, age-standardized mortality ratios (SMRs) were computed using the Italian age-specific mortality rates as standard, and 95% confidence intervals (95% CI) were calculated32.
To evaluate the effect of citizenship on mortality, a multivariable quasi-Poisson regression model for overdispersed count data with log link function33, stratified by sex, was performed, taking into account age at death, and area of residence.
All analyses were performed using SAS® System version 9.3 (2nd release SAS 9.3 TS1M2).
Ethics approval
The cohort was conceived within the project "Socioeconomic differences in mortality" (IF IST 2646), as part of the National Statistical Program (PSN), approved by the Italian Data Protection Authority.
Results
The cohort of Italians and immigrants enrolled in Census 2011 and followed up to 2018 included 59,227,313 subjects, accounting for 398,499,648 person years. Immigrants accounted for 7% of the subjects and for 0.6% of the 4,103,769 deaths observed during follow-up.
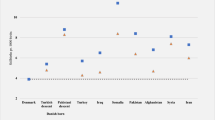
We observed significant (p < 0.001) differences between Italians and immigrants in the distribution of the sociodemographic characteristics (Fig. 1). Compared to Italians, immigrants had a higher proportion of subjects age < 45 years old (78.5% vs 49.4%). Among immigrants the proportion of women (53.3 vs 51.5%) and of residents in Northern Italy (62.6% vs 44.6%) was higher than that of Italians.

Differences between Italians and immigrants in the distribution of the sociodemographic characteristics.
About 50% of all immigrants came from Central-Eastern Europe, followed by North Africa (14.4%) and East Asia (8.5%) (data not shown).
The crude rates showed an excess in mortality for Italians compared to immigrants; in particular, the excess was about tenfold for males and 14-fold for females. When observing the standardized mortality ratios (SMR), we found that mortality among immigrants was half that among Italians, both for men (SMR: 0.52) and for women (SMR: 0.51). Moreover, the SMRs described a lower mortality of immigrants from all macro areas of origin, except for stateless persons, with the lowest SMRs observed for those coming from areas outside Europe, in particular North Africa and Oceania (Table 1).
The multivariable quasi-Poisson regression analysis confirmed, after adjusting for age and macro area of residence in Italy, a lower all-cause mortality for immigrants compared to Italians, both among men (RR: 0.46; 95% CI 0.34–0.63) and women (RR: 0.44; 95% CI 0.33–0.57). No significant difference by macro area of residence in Italy was observed (data not shown).
The SMRs by cause of death showed that in some cases, mortality was higher in immigrants than in Italians, especially among women. Among males (Table 2) tuberculosis was the only cause with an excess in mortality among immigrant men (SMR 4.58); among immigrant women (Table 3), significantly higher mortality compared to the Italians was observed for tuberculosis (SMR 4.73), cervical cancer (SMR 1.58), for complications of pregnancy, childbirth, and puerperium (SMR 1.36), and for homicide (SMR 2.13).
Discussion
Our study found that immigrants resident in Italy had lower all-cause mortality than did Italians, a result that confirms previous results in Italy2 and in other countries24,25,34,35. The mortality advantage of immigrants was more pronounced for those from areas outside Europe, in particular from North Africa and Oceania. In contrast, a higher cause-specific mortality was observed for tuberculosis among immigrants of both sexes and, in immigrant women, for cervical cancer, for causes related to pregnancy, childbirth and puerperium, and for homicide.
The advantage in mortality over Italians may be explained by the “healthy migrant effect” hypothesis, based on the selection for migration of individuals that are healthier than the native people both of the country of origin and of the country of destination1,8,9,10. This effect is evident in particular in the first generations of immigrants2.
Another explanation is the so-called salmon bias effect, the selective remigration of a subsample of unhealthy immigrants to their country of origin when they expect to die shortly. This may result in an artificial underestimation of immigrant mortality rates because deaths occurring in their country of origin are not registered in the mortality statistics of the country of residence, without an official residence change, resulting in these foreign citizens becoming “statistically immortal”1,2,8,10,11,12,13,14.
A recent study conducted in Italy found that, when considering the deaths occurring in the country of origin, this increased the overall mortality rates of immigrants resident in Italy by 18.1% and the age-standardized mortality rate by 23.7%, even if the hypothesized salmon bias effect was not enough to explain the large difference in mortality rates between the two groups of population17.
The lower mortality observed among immigrants concerned all areas of origin, a finding that does not confirm the mortality excess among Sub-Saharan African people observed by a study conducted in the cities of Turin and Reggio Emilia2 and the findings of a study conducted in six European countries, showing a higher all-cause mortality in people from North Africa and Eastern Europe and in women from Sub-Saharan Africa26. However, we observed some differences in mortality between the immigrant areas of origin. In particular, mortality rates were higher in subjects coming from Europe and North America, perhaps due to the greater similarity of their sociodemographic characteristics with the Italian population.
The results of our study highlight that immigrants lose their advantage over Italians for some specific causes of death: tuberculosis and, only among women, for cervical cancer, for complications of pregnancy, childbirth, and puerperium, and for homicide.
The increased mortality for tuberculosis among both male and female immigrants could represent the attenuation of the healthy migrant effect due to more disadvantaged living conditions, inducing a reactivation of latent tuberculosis infection36; confirmation of this seems to be the finding of very few cases of active tuberculosis at the moment of arrival in the host country37. Previous studies reported higher occurrence of tuberculosis among immigrants38,39, suggesting that immigrants arriving in Italy are protected from the most severe consequences of the acute infections acquired in the host country (healthy migrant effect), but are exposed to a higher prevalence of some infections in their country of origin which cause diseases later in life2.
The increased mortality among immigrants for cervical cancer can be explained by the higher prevalence in many of the countries of origin of human papilloma virus (HPV)40, the main cause of cervical cancer. An additional explanation could be lower screening attendance and suboptimal access to cancer treatment2,41,42.
Among women, the mortality excess among immigrants compared to Italians for complications of pregnancy, childbirth, and puerperium is consistent with the results of a large meta-analysis that observed a doubled risk of dying during or after pregnancy for immigrant women in Western European countries when compared with native-born women43. Our findings seem to confirm that maternal and child health represents the main criticality in providing assistance to the foreign population in Italy41,44,45,46.
Moreover, the higher mortality for homicide in immigrant females than in Italian females could be explained by the greater social vulnerability, given factors that are more prevalent in immigrant communities, including social isolation, cultural attitudes, gender roles, and fewer employment options2,24,25,26,47.
We did not find any excess mortality from stomach cancer, contrary to the findings of two systematic reviews48,49 as well as almost all studies. This may be surprising, since stomach cancer is strongly linked with socioeconomic status, and immigrants generally have a lower socioeconomic level than do Italians50. However, Pabla’s extensive systematic review, covering about 40 years, found no Italian or Italian-referenced publication related to stomach cancer among immigrants48. A hypothesis to explain this difference could be the different demographic composition of immigrants in Italy, with a prevalence of communities of European origin, which are less prone to cancers, such as stomach cancer, that are related to infections experienced in early life49.
Strengths and limitations
The study has considerable strengths. First, this is the first study to analyze mortality among immigrants covering the entire resident population in Italy. Its longitudinal approach made it possible to avoid any bias due to the numerator-denominator mismatch in ecological cross-sectional studies and to calculate the exact person-time at risk through a link between individual population records and death registries. Second, to our knowledge, this is the first mortality study based on the whole population of residents in Italy, making it possible to provide a detailed picture of the phenomenon.
However, our study suffers from some limitations. First, like other studies dealing with mortality among immigrants, our study presents the potential bias of unregistered remigration and deaths of immigrants, which may have determined potential overcoverage and salmon bias1,2,8,9,10,11,12,13,14,15,16,17,18. Second, since our study was based on registers of the resident population, immigrants who were undocumented, a particularly vulnerable subpopulation, were not included. However, the percentage of undocumented immigrants in Italy is estimated to be only 0.5% of the total resident population51.
In addition, as shown by Gimeno-Feliu et al.52, the use of citizenship instead of country of birth to define immigrant status, as in our study, can lead to an underestimation of mortality among foreigners compared to natives. This is especially true for individuals who acquired citizenship after a long stay in the country, who are expected to have mortality risks closer to those of natives. Unfortunately, we do not have information in our database on either country of birth or length of stay in Italy.
Conclusions
Although immigration to Italy is no longer a recent phenomenon, and the presence of immigrants is acquiring structural characteristics, our study confirms their health advantage, with lower mortality than that of Italians from almost every cause. This lower mortality in the immigrant population is also observed for all areas of origin. These findings partially differ from a previous Italian longitudinal study and a European study2,26. Future studies could be designed with a nationwide open cohort approach, which is particularly useful for studying an extremely dynamic population such as the immigrant population, taking into account further sources to reduce the potential effects of salmon bias.
Data availability
Statistical analysis were carried out within a research protocol between Istat and INMP, both national public Institute. The database used for the analysis are subject to the legal restrictions established by the European privacy law. The database that support the findings of this study were made available by Istat, but restriction apply to the availability of these data, which were used under license for the current study, and are thus not publicly available. Specific statistical analysis can be requested and agreed with Istat.
References
Abraído-Lanza, A. F., Dohrenwend, B. P., Ng-Mak, D. S. & Turner, J. B. The Latino mortality paradox: A test of the “salmon bias” and healthy migrant hypotheses. Am. J. Public Health 89, 1543–1548. https://doi.org/10.2105/ajph.89.10.1543 (1999).
Pacelli, B. et al. Differences in mortality by immigrant status in Italy. Results of the Italian Network of Longitudinal Metropolitan Studies. Eur. J. Epidemiol. 31, 691–701. https://doi.org/10.1007/s10654-016-0177-z (2016).
Norredam, M., Olsbjerg, M., Petersen, J. H., Juel, K. & Krasnik, A. Inequalities in mortality among refugees and immigrants compared to native Danes—A historical prospective cohort study. BMC Public Health 12, 757. https://doi.org/10.1186/1471-2458-12-757 (2012).
Aldridge, R. W. et al. Global patterns of mortality in international migrants: A systematic review and meta-analysis. Lancet 392, 2553–2566. https://doi.org/10.1016/S0140-6736(18)32781-8 (2018).
Bhopal, R. S. et al. Mortality, ethnicity, and country of birth on a national scale, 2001–2013: A retrospective cohort (Scottish Health and Ethnicity Linkage Study). PLoS Med 15, e1002515. https://doi.org/10.1371/journal.pmed.1002515 (2018).
Razum, O., Zeeb, H. & Rohrmann, S. The ‘healthy migrant effect’—Not merely a fallacy of inaccurate denominator figures. Int. J. Epidemiol. 29, 191–192. https://doi.org/10.1093/ije/29.1.191 (2000).
Kristensen, P. & Bjerkedal, T. Dealing with emigration in cohort studies: Follow-up of mortality and cancer incidence among Norwegians born between 1967 and 1976. Eur. J. Epidemiol. 25, 155–161. https://doi.org/10.1007/s10654-009-9417-9 (2010).
Ruiz, J. M., Steffen, P. & Smith, T. B. Hispanic mortality paradox: A systematic review and meta-analysis of the longitudinal literature. Am. J. Public Health 103, e52-60. https://doi.org/10.2105/AJPH.2012.301103 (2013).
Ullmann, S. H., Goldman, N. & Massey, D. S. Healthier before they migrate, less healthy when they return? The health of returned migrants in Mexico. Soc. Sci. Med. 73, 421–428. https://doi.org/10.1016/j.socscimed.2011.05.037 (2011).
Turra, C. M. & Elo, I. T. The impact of salmon bias on the hispanic mortality advantage: New evidence from social security data. Popul. Res. Policy Rev. 27, 515–530. https://doi.org/10.1007/s11113-008-9087-4 (2008).
Pablos-Méndez, A. Mortality among Hispanics. JAMA 271, 1237 (1994).
Wallace, M. & Kulu, H. Low immigrant mortality in England and Wales: A data artefact?. Soc. Sci. Med. 120, 100–109. https://doi.org/10.1016/j.socscimed.2014.08.032 (2014).
Guillot, M., Khlat, M., Elo, I., Solignac, M. & Wallace, M. Understanding age variations in the migrant mortality advantage: An international comparative perspective. PLoS ONE 13, e0199669. https://doi.org/10.1371/journal.pone.0199669 (2018).
Monti, A., Drefahl, S., Mussino, E. & Härkönen, J. Over-coverage in population registers leads to bias in demographic estimates. Popul. Stud. 74, 451–469. https://doi.org/10.1080/00324728.2019.1683219 (2020).
Wallace, M. & Wilson, B. Age variations and population over-coverage: Is low mortality among migrants merely a data artefact?. Popul. Stud. https://doi.org/10.1080/00324728.2021.1877331 (2021).
Fedeli, U., Ferroni, E., Pigato, M., Avossa, F. & Saugo, M. Causes of mortality across different immigrant groups in Northeastern Italy. PeerJ 3, e975. https://doi.org/10.7717/peerj.975 (2015).
Di Napoli, A. et al. Salmon bias effect as hypothesis of the lower mortality rates among immigrants in Italy. Sci. Rep. 11, 8033. https://doi.org/10.1038/S41598-021-87522-2 (2021).
Puschmann, P., Donrovich, R. & Matthijs, K. Salmon bias or red herring? Comparing adult mortality risks (Ages 30–90) between natives and internal migrants: Stayers, returnees and movers in Rotterdam, The Netherlands, 1850–1940. Hum. Nat. 28, 481–499. https://doi.org/10.1007/s12110-017-9303-1 (2017).
DemoIstat. Demography in figures. National Institute of Statistics. http://demo.istat.it/index.php. (2 Dec 2021 last accessed)
AGENAS. La salute della popolazione immigrata: Il monitoraggio da parte dei Sistemi Sanitari Regionali. 2013. https://www.agenas.gov.it/images/agenas/ricerca/agenas_ccm_corrente_finalizzata/LEA/La%20Salute%20pop%20immigrata/0_La_salute_della_popolazione_immigrata_il_monitoraggio_da_parte_dei_Sistemi_Sanitari_Regionali.pdf. (2 Dec 2021 last accessed)
Martini, A., Chellini, E. & Sala, A. Mortality in immigrants in Tuscany. Epidemiol. Prev. 35, 275–281 (2011).
Lara, M., Gamboa, C., Kahramanian, M. I., Morales, L. S. & Bautista, D. E. Acculturation and Latino health in the United States: A review of the literature and its sociopolitical context. Annu. Rev. Public Health 26, 367–397. https://doi.org/10.1146/annurev.publhealth.26.021304.144615 (2005).
Malmusi, D., Borrell, C. & Benach, J. Migration-related health inequalities: Showing the complex interactions between gender, social class and place of origin. Soc. Sci. Med. 71, 1610–1619 (2010).
Bos, V., Kunst, A. E., Keij-Deerenberg, I. M., Garssen, J. & Mackenbach, J. P. Ethnic inequalities in age- and cause-specific mortality in The Netherlands. Int. J. Epidemiol. 33, 1112–1119. https://doi.org/10.1093/ije/dyh189 (2004).
Regidor, E., de La Fuente, L., Martínez, D., Calle, M. E. & Domínguez, V. Heterogeneity in cause-specific mortality according to birthplace in immigrant men residing in Madrid, Spain. Ann. Epidemiol. 18, 605–613. https://doi.org/10.1016/j.annepidem.2008.04.007 (2008).
Ikram, U. Z. et al. All-cause and cause-specific mortality of different migrant populations in Europe. Eur. J. Epidemiol. 31, 655–665. https://doi.org/10.1007/s10654-015-0083-9 (2016).
Ott, J. J., Paltiel, A. M., Winkler, V. & Becher, H. Chronic disease mortality associated with infectious agents: A comparative cohort study of migrants from the Former Soviet Union in Israel and Germany. BMC Public Health 8, 110. https://doi.org/10.1186/1471-2458-8-110 (2008).
Alicandro, G., Grande, E., Sebastiani, G. & Frova, L. The 2011 Italian census cohort for the study of socioeconomic inequality in mortality. Int. J. Public Health 65, 693–697. https://doi.org/10.1007/s00038-020-01375-6 (2020).
Frova, L., Alicandro, G., Demuru, E. & Sebastiani, G. Integrazione di archivi nazionali per lo studio delle diseguaglianze socioeconomiche nella mortalita in Italia. Istat Working Papers 2019;2/2019. ISBN: 9788845819865
Ministero dell’Interno. Diritti, doveri, identità, partecipazione. Come diventare cittadini italiani. https://www.interno.gov.it/it/temi/cittadinanza-e-altri-diritti-civili/cittadinanza (2 Dec 2021 last accessed)
Istat. Codici delle unità territoriali estere. https://www.istat.it/it/archivio/6747 (2 Dec 2021 last accessed)
Breslow, N. E. & Day, N. E. Statistical Methods in Cancer Research: Volume II—The Design and Analysis of Cohort Studies (International Agency for Research on Cancer, 1987).
Cameron, C. & Trivedi, P. Regression Analysis of Count Data (Cambridge University Press, 1998).
Gadd, M., Johansson, S. E., Sundquist, J. & Wändell, P. Are there differences in all-cause and coronary heart disease mortality between immigrants in Sweden and in their country of birth? A follow-up study of total populations. BMC Public Health 6, 102. https://doi.org/10.1186/1471-2458-6-102 (2006).
Boulogne, R., Jougla, E., Breem, Y., Kunst, A. E. & Rey, G. Mortality differences between the foreign-born and locally-born population in France (2004–2007). Soc. Sci. Med. 74, 1213–1223 (2012).
Baglio, G., Marceca, M. & Tosti, M. E. Il controllo della tubercolosi tra gli immigrati in Italia. Programma Nazionale Linee Guida Salute Migranti (INMP, 2018) (ISBN:9788898544202).
Di Meco, E. et al. Infectious and dermatological diseases among arriving migrants on the Italian coasts. Eur. J. Public Health 28, 910–916 (2018).
Farchi, S., Mantovani, J., Borgia, P. & Giorgi, R. P. Tuberculosis incidence, hospitalisation prevalence and mortality in Lazio, Italy, 1997–2003. Int. J. Tuberc. Lung Dis. 12, 193–198 (2008).
Arshad, S., Bavan, L., Gajari, K., Paget, S. N. & Baussano, I. Active screening at entry for tuberculosis among new immigrants: A systematic review and meta-analysis. Eur. Respir. J. 35, 1336–1345 (2010).
Bruni, L., Albero, G., Serrano, B., et al. ICO/IARC Information Centre on HPV and Cancer (HPV Information Centre). Human Papillomavirus and Related Diseases in the World. Summary Report 22 October 2021. https://hpvcentre.net/statistics/reports/XWX.pdf (2 Dec 2021 last accessed)
Di Napoli, A. et al. Evaluating health care of the immigrant population in Italy through indicators of a nationalmonitoring system. Epidemiol. Prev. 44(5-6S1), 85–93. https://doi.org/10.19191/EP20.5-6.S1.P085.077 (2020).
Petrelli, A. et al. Geographic and socioeconomic differences in Pap test and mammography uptake in Italy: What results from the National Health Interview Survey. BMJ Open 8, e021653. https://doi.org/10.1136/bmjopen-2018-021653 (2018).
Pedersen, G. S., Grøntved, A., Mortensen, L. H., Andersen, A. M. & Rich-Edwards, J. Maternal mortality among migrants in Western Europe: A meta-analysis. Matern. Child Health J. 18, 1628–1638. https://doi.org/10.1007/s10995-013-1403-x (2014).
Petrelli, A. et al. Immigrants’ health and socioeconomic inequalities of overall population residing in Italy evaluated through the Italian network of Longitudinal Metropolitan Studies. Epidemiol. Prev. 43(5-6 Suppl 1), 1–80. https://doi.org/10.19191/EP19.5-6.S1.112 (2019).
Di Napoli, A., Rossi, A., Ventura, M. & Petrelli, A. Sistema di monitoraggio dello stato di salute e di assistenza sanitaria alla popolazione immigrata: risultati anno 2017. Quaderni di Epidemiologia 2021;3. Roma: INMP, 2021. ISBN:9788898544271
Di Napoli, A., Rossi, A., Gaudio, R. & Petrelli, A. Sistema di monitoraggio dello stato di salute e di assistenza sanitaria alla popolazione immigrata: risultati anno 2016. Quaderni di Epidemiologia 2019;2. Roma: INMP, 2019. ISBN:9788898544226
United Nations Office on Drugs and Crime. Global Study on Homicide 2019. Vienna: UNOC, 2019. https://www.unodc.org/documents/data-and-analysis/gsh/Booklet1.pdf (2 Dec 2021 last accessed)
Pabla, B. S., Shah, S. C., Corral, J. E. & Morgan, D. R. Increased incidence and mortality of gastric cancer in immigrant populations from high to low regions of incidence: A systematic review and meta-analysis. Clin. Gastroenterol. Hepatol. 18, 347–359. https://doi.org/10.1016/j.cgh.2019.05.032 (2020).
Arnold, M., Razum, O. & Coebergh, J. W. Cancer risk diversity in non-western migrants to Europe: An overview of the literature. Eur. J. Cancer 46, 2647–2659. https://doi.org/10.1016/j.ejca.2010.07.050 (2010).
Petrelli, A. et al. Italian atlas of mortality inequalities by education level. Epidemiol. Prev. 43(1S1), 1–120. https://doi.org/10.19191/ep19.1.s1.002 (2019).
Centro Studi e Ricerche IDOS. Dossier Statistico Immigrazione 2015 (IDOS, 2015) (ISBN: 9788864800349).
Gimeno-Feliu, L. A. et al. The definition of immigrant status matters: Impact of nationality, country of origin, and length of stay in host country on mortality estimates. BMC Public Health 19, 247. https://doi.org/10.1186/s12889-019-6555-1 (2019).
Acknowledgements
We thank Jacqueline M. Costa for English language editing.
Author information
Authors and Affiliations
Contributions
A.D.N. conceived and designed of the study, contributed to analysis and interpretation of data, and wrote the draft of the article. M.V. contributed to conception and design of the study, was responsible of acquisition of data, performed analysis and contributed to interpretation of data, and drafting the article. E.G. contributed to interpretation of data, and revised the article critically for important intellectual content. L.F. contributed to design of the study, to acquisition and interpretation of data, and revised the article critically for important intellectual content. C.M. contributed to conception of the study, and revised the article critically for important intellectual content. A.P. conceived and designed of the study, contributed to analysis and interpretation of data, and revised the article critically for important intellectual content. All the authors have approved the manuscript before submission, including the order of authors.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Di Napoli, A., Ventura, M., Grande, E. et al. Nationwide longitudinal population-based study on mortality in Italy by immigrant status. Sci Rep 12, 10986 (2022). https://doi.org/10.1038/s41598-022-15290-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-022-15290-8
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
