
Abstract
Sarcopenia has been associated with several conditions relevant to obstructive sleep apnea (OSA), such as aging and obesity, but a direct relationship between OSA and skeletal muscle alterations has not been identified. This study investigated associations between computed tomography (CT)-measured skeletal muscle indices and OSA severity. Analyzed were 334 patients who underwent polysomnography to diagnose OSA. Lumbar skeletal muscles were assessed with CT for the skeletal muscle mass index (SMI, cross-sectional area, normalized for height squared) and skeletal muscle density (SMD, fat infiltration). The apnea-hypopnea index (AHI) correlated positively with the SMI and negatively with SMD in both men and women. The AHI was weakly associated with SMI only in men (β = 0.11, P = 0.017) after adjustment for the body mass index (BMI) (BMI: β = 0.61, P < 0.001 in men, β = 0.65, P < 0.001 in women). The association of AHI and SMD was not significant after adjustment for BMI (BMI: β = −0.42, P < 0.001 in men, β = −0.64, P < 0.001 in women). Severity of OSA correlated with increases in skeletal muscle mass rather than muscle depletion and skeletal muscle adiposity. These associations were limited compared with the stronger associations between obesity and skeletal muscles.
Similar content being viewed by others

Introduction
Sarcopenia is the loss of systemic skeletal muscle mass accompanied by decreased strength and function1. Sarcopenia has been of increasing interest because skeletal muscle depletion has been observed in several conditions such as aging, chronic obstructive pulmonary disease (COPD), metabolic syndrome, and cancer2,3,4,5,6. In fact, decreased skeletal muscle mass assessed by computed tomography (CT) and other measures was a significant predictor of overall survival of patients with cancer and COPD4,7,8. These findings suggest that skeletal muscle changes can reflect the systemic effects and burdens of chronic diseases. In addition, low skeletal muscle density (SMD) values on CT indicated fat infiltration into muscles and was associated with muscle dysfunction, aging, and obesity2,3,9,10. Thus, these CT measurements (mass volume and density) can be useful for assessment of different changes in skeletal muscles (depletion and fat accumulation) and could be associated with various conditions and their consequences.
Obstructive sleep apnea (OSA) is a common sleep disordered breathing condition. OSA has significant effects on various organ systems such as the cardiovascular (hypertension; ischemic heart disease), endocrinal (glucose intolerance; dyslipidemia), and central and sympathetic nervous systems (cognitive impairment; sympathetic activation)11. Among these comorbidities associated with OSA, hypertension, and diabetes are also associated with sarcopenia12. Given the wide range of the systemic impact of OSA, OSA can also profoundly affect skeletal muscles in the whole body. In addition, OSA was associated with ageing and obesity13, both of which were reported to be accompanied by skeletal muscle depletion and fat accumulation on CT measurements2,3. These findings suggest a possible association between OSA and skeletal muscles in the entire body. However, the direct relationship between OSA and skeletal muscle indices has not been investigated with the exception of one study that used the bioimpedance method14.
Thus, in this study, we aimed to investigate the relationship between OSA severity and skeletal muscle mass and density. We hypothesized that more severe OSA should be associated with greater losses of total skeletal muscle mass and increases in fat accumulation in muscles. CT and magnetic resonance imaging (MRI) are gold standards for estimating skeletal muscle mass3, and CT measurements at the lumbar level have been used as a surrogate marker for whole body skeletal muscle volume7,15,16. Therefore, using abdominal CT images taken to evaluate visceral fat accumulation and to diagnose visceral fat obesity, we assessed lumbar skeletal muscles quantitatively in patients suspected to have OSA as the representatives of total skeletal muscles. We then analyzed the associations among CT indices of skeletal muscles, OSA parameters, and other confounders such as body adiposity and self-reported physical activity.
Results
Baseline characteristics of study patients
During the study period, 740 patients underwent polysomnography (PSG), and finally data on 334 patients were analyzed (Fig. 1). Of 334 patients included in the analysis, 12 (3.6%), 61 (18.3%), 105 (31.4%), and 156 (46.7%) had no (AHI < 5), mild (5 ≤ AHI < 15), moderate (15 ≤ AHI < 30), and severe OSA (AHI ≥ 30), respectively. Table 1 shows the baseline characteristics and skeletal muscle parameters of study patients according to sex. This comparison revealed that OSA was significantly more severe in the men than in the women, and the skeletal muscle mass index (SMI), SMD and subcutaneous fat area (SFA) index were significantly higher in the men than in the women (SMI, 52.5 ± 8.4 vs. 42.6 ± 7.5 cm2/m2; SMD, 35.8 ± 6.5 vs. 30.0 ± 7.8 cm2/m2; SFA index, 47.6 ± 22.1 vs. 76.6 ± 43.5 cm2/m2, all P < 0.001). Neither the BMI nor visceral fat area (VFA) index differed between the men and women.

Flowchart of patient participation. PSG, polysomnography; CT, computed tomography; OSA, obstructive sleep apnea.
Relationships between SMI and OSA, physical activity, and obesity
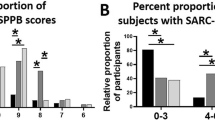
Given the significant gender differences in OSA severity and the skeletal muscle parameters, the relationships between skeletal muscle parameters and other clinical parameters were analyzed in men and women separately, as reported in previous studies4,7,15,16,17,18,19. Correlations between the SMI and clinical variables are shown in Table 2. The SMI was significantly correlated with AHI in both men and women (r = 0.35, P < 0.001, and r = 0.24, P = 0.019, respectively) (Fig. 2a,b).

Correlation between AHI and the SMI or SMD. (a) Correlation between AHI and SMI in men. (b) Correlation between AHI and SMI in women. (c) Correlation between AHI and SMD in men. (d) Correlation between AHI and SMD in women. AHI, apnea-hypopnea index; SMI, skeletal muscle mass index; SMD, skeletal muscle density.
Results of the multivariate regression analysis of predictors for the SMI are shown in Table 3. Because there was strong collinearity between the BMI and the SFA index in men and women and between the BMI and VFA index in women, BMI (Table 3, model 1) and both the VFA index and SFA index (Table 3, model 2) were entered into the model separately. After adjusting for age and BMI, the AHI was significantly positively related to SMI in men (β = 0.11, P = 0.017), but the BMI was more strongly associated with the SMI in both sexes (Table 3, model 1). Fat mass was also associated with the SMI (Table 3, model 2). Even when we included the physical activity index as a covariate, the results were almost the same (Table 3, model 3). When CT90 or 3%ODI was chosen as a parameter of OSA severity instead of the AHI, 3%ODI was significantly positively related to the SMI in men (β = 0.12, P = 0.014), but CT90 was not (Supplementary Table S1).
Relationships between SMD and OSA, physical activity, and obesity
Table 2 shows the correlations between SMD and clinical variables. The SMD was significantly correlated with the AHI in both men and women (r = −0.15, P = 0.025, and r = −0.29, P = 0.005, respectively) (Fig. 2c,d).
Results of the multivariate regression analysis of predictors for SMD are shown in Table 4. As with the SMI, BMI (Table 4, model 1) and both the VFA index and SFA index (Table 4, model 2) were entered into the model separately. After adjusting for covariates, the AHI was not related to SMD in either model. However, age, BMI, VFA index, and SFA index were independently associated with SMD in both sexes. When CT90 or 3%ODI was chosen as a parameter of OSA severity instead of the AHI, neither CT90 nor 3%ODI was related to SMD (Supplementary Table S2).
Discussion
To the best of our knowledge, this is the first study to investigate the relationship between OSA severity and skeletal muscle mass and density as assessed by CT. In a relatively large cohort of patients suspected to have OSA, the AHI significantly and positively correlated with the SMI in both men and women. After adjustment for covariates, the association of the AHI with the SMI remained significant but was much weaker than that of the BMI in men; however, the association was not significant for women. The AHI was significantly and negatively correlated with SMD in men and women, but this association did not persist in either men or women after adjustment for other confounders.
We hypothesized that the severity of OSA negatively correlates with the SMI. However, our results were contrary to this hypothesis, showing that OSA was associated with an increased skeletal muscles mass in both men and women. Previously, the BMI was reported to be positively correlated with AHI20 and SMI7. Results of our multivariate analysis suggested that BMI was the strongest contributor to the SMI in our cohort. On the other hand, the independent association of OSA with the SMI was limited although statistically significant after adjustment for the BMI and age. This limited association of OSA with the SMI remained the same even when considering the effect of daily exercise. Similar results were obtained when VFA and SFA indices for the severity of obesity were entered into the analysis instead of the BMI. Taken together our findings suggested that skeletal muscle mass is mainly a reflection of body size and the severity of obesity in OSA patients.
The positive correlation between OSA severity and the SMI was contrary to the negative correlation observed with other chronic diseases such as cancer, chronic heart failure, and COPD. In those diseases, skeletal muscle depletion has been associated with the disease burden, probably through cachexia or systemic exhaustion caused by the disease. In lung, gastrointestinal, or skin cancer, decreased skeletal muscle mass was associated with impaired physical function and poor survival7,21. In chronic heart failure, skeletal muscle depletion has been related to reduced exercise capacity and the advancement of the disease22. In COPD, decreased skeletal muscle mass was associated with spirometric measurements indicating impaired lung function and poor survival8,23. Compared to these exhaustive diseases, OSA may have only a small role in skeletal muscle alterations, and the BMI and obesity may have much stronger relationships with the condition of skeletal muscles.
The severity of OSA was negatively correlated with SMD, suggesting that more severe OSA was associated with greater fat accumulation in muscles. This finding was consistent with our hypothesis, although the association was not independent from obesity. Obesity was shown to be a major confounder in the relationship between OSA and other conditions24. OSA was also reported to be associated with liver and visceral fat accumulation25,26, although the associations were much weaker than those between BMI and adiposity. Similarly, our results indicated that the relationship between OSA and adipose accumulation in skeletal muscles might be largely mediated by obesity.
Interestingly, some associations of OSA with skeletal muscle indices were different between men and women. For women, age and obesity (BMI and body fat indices) could account for all of these associations, while the AHI was independently associated with skeletal muscle mass only in men. Associations of OSA with BMI and adiposity were reported to differ between men and women. Women with OSA had a higher BMI than men with OSA of the same severity, suggesting that the impact of obesity could be greater in women27. The association of OSA with abdominal fat accumulation was stronger in men than in women, while obesity had a stronger association with abdominal fat in women26,28. These previous findings may be consistent with our results on skeletal muscle because obesity, rather than OSA, had a stronger link with adiposity in women than in men, although the mechanisms of sex differences relevant to OSA have not been elucidated.
Several limitations of this study should be mentioned. First, this was a cross-sectional study of an Asian population. Thus, because of its cross-sectional design our study could not reveal the causative relationship between skeletal muscle changes and OSA. In addition, we did not have CT measurements after continuous positive airway pressure (CPAP) therapy. A prospective longitudinal study of patients on CPAP therapy may clarify the impact of OSA on skeletal mass. Also, anthropometric values differ among ethnic groups13,29. Ethnic cohorts other than Asians should be studied. Second, skeletal muscles were assessed only in the lumbar region. A significant correlation between lumbar muscle mass measured by CT and MRI and total skeletal muscle volume assessed by dual-energy X-ray absorptiometry and MRI was reported15,30. Several studies evaluated skeletal muscles using CT images at the lumbar level as a surrogate marker for total skeletal muscle volume7,16,18,31,32. In addition, we showed a strong correlation between CT-measured skeletal muscle mass at the third lumbar vertebra and bioelectrical impedance analysis (BIA)-measured skeletal muscle mass of the whole body (Supplementary Figure S1). On the other hand, upper airway dilator muscle dysfunction has a specific role in the pathogenesis of OSA33. Hypoglossal nerve stimulation to dilator muscles has been proposed as a novel therapeutic option for OSA34. Thus, upper respiratory muscle changes may have different associations with OSA from other skeletal muscle changes, although we do not have data on upper airway muscles for analysis. The relationships between upper respiratory muscle changes and OSA should be addressed in future studies. Third, physical activity was assessed by questionnaires in this study, the results of which might be different from those obtained by objective measurements.
In conclusion, the severity of OSA did not correlate with skeletal muscle depletion. Conversely, patients with more severe OSA had a larger mass of skeletal muscles than those with less severe OSA even after adjustment for the strong effect of obesity, although this association was weak and limited to men. The severity of OSA was associated with low SMD, suggesting fat infiltration into skeletal muscles; however, this relationship was not independent from obesity. To clarify the roles of skeletal muscles in the pathogenesis of OSA and its consequences, these limited associations between OSA and skeletal muscle indices should be re-examined in future studies of other cohorts.
Methods
Patients
We retrospectively examined data on consecutive patients who underwent diagnostic full overnight PSG at the Sleep Unit of Kyoto University Hospital between January 2010 and December 2012. All had been referred to our sleep unit under suspicion of OSA with symptoms such as daytime sleepiness or habitual snoring. Inclusion criteria were age between 40 and 85 years, and no prior diagnosis of or treatment for OSA. Exclusion criteria were as follows: no CT scan, sleep disordered breathing other than OSA, steroid use, systemic inflammatory disease (i.e., connective tissue diseases), and malignancy. The Kyoto University Graduate School and Faculty of Medicine Ethics Committee approved this study (R0480) and waived the requirement for written informed consent from participants due to the study’s retrospective nature. All the performances were in accordance to the Declaration of Helsinki. Patient information was anonymized and de-identified prior to analysis.
Polysomnography
The diagnosis of OSA was confirmed by overnight PSG (SomnoStar pro, Cardinal Health, Dublin, OH, USA or Alice 4, Philips Respironics, Inc., Murrysville, PA, USA) as previously described35. Apnea was defined as the continuous cessation of airflow for at least 10 s and hypopnea was defined as a reduction in airflow by nasal pressure ≥50% lasting at least 10 s accompanied by a decrease in SpO2 ≥3% and/or associated with arousal. Apnea-hypopnea index (AHI) values were calculated as the number of episodes of apnea and hypopnea per h over total sleep time.
Physical activity
We assessed self-reported physical activity with questionnaires on frequency and time spent on three levels of physical activity. Three levels were vigorous (jogging, swimming, strenuous sports, bicycling on hills), moderate (housework, ballroom dancing, golf, bicycling on level ground, regular walking), and light (office work, strolling, personal care)36. Average intensity of activity was defined using metabolic equivalents (MET, kcal·kg−1·body weight·h−1) as follows: 9 METs for vigorous, 6 for moderate, and 3 for light37. The amount of physical activity (kcal/w) was calculated by multiplying the corresponding MET values by time spent and body weight, and summing up the values. The summed physical activity values were defined as the physical activity index. Also, the maximum intensity of physical activity (vigorous, moderate, light, or no activity) was used as the parameter of physical activity.
Measurement of skeletal muscle and visceral and subcutaneous adipose tissue
Patients who agreed to our recommendation underwent an abdominal CT within 30 days of the diagnostic PSG before starting CPAP therapy. Unenhanced transverse CT was performed with an Aquilion 64 CT system (Toshiba Medical Systems Corporation, Tochigi, Japan). In this study, CT images of 7 mm slices were used for the analysis of skeletal muscle area and muscle density.
For skeletal muscle, two consecutive transverse CT images extending from the third lumbar vertebrae in the inferior direction were assessed, then averaged. Skeletal muscle tissues quantified included the psoas, erector spinae, quadratus lumborum, transversus abdominus, internal and external obliques, and rectus abdominus. Images were analyzed with a workstation (AZE VirtualPlace 99, AZE of America, Ltd., Irvine, CA, USA). Skeletal muscle was identified and quantified by Hounsfield Unit thresholds of −29 to +150. Cross-sectional area for muscle was normalized for height in meters squared (cm2/m2) and described as the SMI4,7,15,16,18,19,31,32. SMD, which was studied as a correlate of muscle density determined by CT38, was reported for the entire muscle area at the third lumbar vertebra7,18. The intraclass correlation coefficients for the SMI and SMD from 50 random subset samples were both >0.95.
The lumbar skeletal muscle area was shown to be strongly correlated with the whole skeletal muscle mass15,30. To determine whether SMI at the third lumbar vertebra is valid as a surrogate index for total skeletal muscle volume, we investigated the association between SMI and the whole body skeletal muscle mass obtained from BIA in another cohort of OSA patients (n = 68). For BIA, patients were assessed in the supine position by a body composition analyzer (InBody S20; Biospace, Seoul, Korea). Appendicular skeletal muscle mass (ASM) normalized for height in meters squared was used as an indicator of total skeletal muscle volume39. SMI was strongly correlated with ASM/height2 (r = 0.804, P < 0.001, Supplementary Figure S1).
For the VFA and SFA, CT images at the level of the umbilicus were assessed40. VFA and SFA were quantified with the same workstation mentioned above and as previously described26. VFA and SFA were both normalized for height in meters squared (cm2/m2) and described as the VFA index and SFA index, respectively.
Statistical analysis
To evaluate the clinical features of each sex, we classified the participants into men and women. All values were expressed as means ± standard deviations, percentages, or medians [interquartile range] unless stated otherwise. Continuous variables were compared using an unpaired Student’s t test or Mann-Whitney U test, as appropriate. Categorical variables were compared using a chi-squared test or Fisher’s exact test, as appropriate. To analyze the correlation between the severity of OSA and the SMI or SMD, Pearson or Spearman rank correlation coefficients were calculated for each sex, as appropriate. To test our hypothesis that SMI and SMD were associated with the severity of OSA, we performed a multivariate regression analysis for each sex. As covariates for SMI, we included age, BMI, and the physical activity index, which were shown to be associated with muscle mass4,7,15,16,19,32,41, and the VFA index, SFA index, and AHI, the latter of which is usually taken as a parameter of OSA severity. As covariates for SMD, we included age, BMI, VFA index, and SFA index, which were associated with muscle density7,17,18,38, and AHI. When multiple independent variables had strong collinearity (r >0.70), one was selected. In the sample size calculation, when the effect size was 0.15, the statistical power level was 0.8, the number of predictors was 4, and the probability level was 0.05, the minimum required sample size for multiple regression analysis was 84. During 2010–2012, the number of eligible female patients was 95 and that of male patients was 239. Thus, we decided to include all consecutive patients during this period. Two-tailed P value < 0.05 was deemed statistically significant. All statistical analyses were performed using JMP 11.2.0 software (SAS Institute Inc., Cary, NC, USA).
Data availability
The datasets analyzed during the current study are available from the corresponding author on reasonable request.
References
Rosenberg, I. H. Sarcopenia: origins and clinical relevance. J. Nutr. 127, 990s–991s (1997).
Volpato, S. et al. Prevalence and clinical correlates of sarcopenia in community-dwelling older people: application of the EWGSOP definition and diagnostic algorithm. J. Gerontol. A Biol. Sci. Med. Sci. 69, 438–446, https://doi.org/10.1093/gerona/glt149 (2014).
Cruz-Jentoft, A. J. et al. Sarcopenia: European consensus on definition and diagnosis: Report of the European Working Group on Sarcopenia in Older People. Age Ageing 39, 412–423, https://doi.org/10.1093/ageing/afq034 (2010).
Baracos, V. E., Reiman, T., Mourtzakis, M., Gioulbasanis, I. & Antoun, S. Body composition in patients with non-small cell lung cancer: a contemporary view of cancer cachexia with the use of computed tomography image analysis. Am. J. Clin. Nutr. 91, 1133s–1137s, https://doi.org/10.3945/ajcn.2010.28608C (2010).
Lu, C. W. et al. Sarcopenic obesity is closely associated with metabolic syndrome. Obes. Res. Clin. Pract. 7, e301–307, https://doi.org/10.1016/j.orcp.2012.02.003 (2013).
Ischaki, E. et al. Body mass and fat-free mass indices in COPD: relation with variables expressing disease severity. Chest 132, 164–169, https://doi.org/10.1378/chest.06-2789 (2007).
Martin, L. et al. Cancer cachexia in the age of obesity: skeletal muscle depletion is a powerful prognostic factor, independent of body mass index. J. Clin. Oncol. 31, 1539–1547, https://doi.org/10.1200/jco.2012.45.2722 (2013).
Tanimura, K. et al. Quantitative Assessment of Erector Spinae Muscles in Patients with Chronic Obstructive Pulmonary Disease. Novel Chest Computed Tomography-derived Index for Prognosis. Ann Am Thorac Soc 13, 334–341, https://doi.org/10.1513/AnnalsATS.201507-446OC (2016).
Aubrey, J. et al. Measurement of skeletal muscle radiation attenuation and basis of its biological variation. Acta Physiol (Oxf) 210, 489–497, https://doi.org/10.1111/apha.12224 (2014).
Goodpaster, B. H. et al. Attenuation of skeletal muscle and strength in the elderly: The Health ABC Study. J Appl Physiol (1985) 90, 2157–2165 (2001).
Jordan, A. S., McSharry, D. G. & Malhotra, A. Adult obstructive sleep apnoea. Lancet 383, 736–747, https://doi.org/10.1016/s0140-6736(13)60734-5 (2014).
Han, P. et al. The increased risk of sarcopenia in patients with cardiovascular risk factors in Suburb-Dwelling older Chinese using the AWGS definition. Sci. Rep. 7, 9592, https://doi.org/10.1038/s41598-017-08488-8 (2017).
Chen, X. et al. Racial/ethnic differences in the associations between obesity measures and severity of sleep-disordered breathing: the Multi-Ethnic Study of Atherosclerosis. Sleep Med. 26, 46–53, https://doi.org/10.1016/j.sleep.2015.06.003 (2016).
Kosacka, M., Korzeniewska, A. & Jankowska, R. The evaluation of body composition, adiponectin, C-reactive protein and cholesterol levels in patients with obstructive sleep apnea syndrome. Adv Clin Exp Med 22, 817–824 (2013).
Mourtzakis, M. et al. A practical and precise approach to quantification of body composition in cancer patients using computed tomography images acquired during routine care. Appl Physiol Nutr Metab 33, 997–1006, https://doi.org/10.1139/h08-075 (2008).
Hanai, T. et al. Sarcopenia impairs prognosis of patients with liver cirrhosis. Nutrition 31, 193–199, https://doi.org/10.1016/j.nut.2014.07.005 (2015).
Sabel, M. S. et al. Sarcopenia as a prognostic factor among patients with stage III melanoma. Ann. Surg. Oncol. 18, 3579–3585, https://doi.org/10.1245/s10434-011-1976-9 (2011).
Antoun, S. et al. Skeletal muscle density predicts prognosis in patients with metastatic renal cell carcinoma treated with targeted therapies. Cancer 119, 3377–3384, https://doi.org/10.1002/cncr.28218 (2013).
Prado, C. M. et al. Prevalence and clinical implications of sarcopenic obesity in patients with solid tumours of the respiratory and gastrointestinal tracts: a population-based study. Lancet Oncol. 9, 629–635, https://doi.org/10.1016/s1470-2045(08)70153-0 (2008).
Pillar, G. & Shehadeh, N. Abdominal fat and sleep apnea: the chicken or the egg. Diabetes Care 31(Suppl 2), S303–309, https://doi.org/10.2337/dc08-s272 (2008).
Bye, A. et al. Muscle mass and association to quality of life in non-small cell lung cancer patients. Journal of cachexia, sarcopenia and muscle 8, 759–767, https://doi.org/10.1002/jcsm.12206 (2017).
Fulster, S. et al. Muscle wasting in patients with chronic heart failure: results from the studies investigating co-morbidities aggravating heart failure (SICA-HF). Eur. Heart J. 34, 512–519, https://doi.org/10.1093/eurheartj/ehs381 (2013).
McDonald, M. L. et al. Quantitative computed tomography measures of pectoralis muscle area and disease severity in chronic obstructive pulmonary disease. A cross-sectional study. Ann Am Thorac Soc 11, 326–334, https://doi.org/10.1513/AnnalsATS.201307-229OC (2014).
Romero-Corral, A., Caples, S. M., Lopez-Jimenez, F. & Somers, V. K. Interactions between obesity and obstructive sleep apnea: implications for treatment. Chest 137, 711–719, https://doi.org/10.1378/chest.09-0360 (2010).
Toyama, Y. et al. Impact of Obstructive Sleep Apnea on Liver Fat Accumulation According to Sex and Visceral Obesity. PLoS One 10, e0129513, https://doi.org/10.1371/journal.pone.0129513 (2015).
Harada, Y. et al. Differences in associations between visceral fat accumulation and obstructive sleep apnea by sex. Ann Am Thorac Soc 11, 383–391, https://doi.org/10.1513/AnnalsATS.201306-182OC (2014).
Yukawa, K. et al. Gender differences in the clinical characteristics among Japanese patients with obstructive sleep apnea syndrome. Chest 135, 337–343, https://doi.org/10.1378/chest.08-1414 (2009).
Simpson, L. et al. Sex differences in the association of regional fat distribution with the severity of obstructive sleep apnea. Sleep 33, 467–474 (2010).
Yamagishi, K. et al. Cross-cultural comparison of the sleep-disordered breathing prevalence among Americans and Japanese. Eur. Respir. J. 36, 379–384, https://doi.org/10.1183/09031936.00118609 (2010).
Shen, W. et al. Total body skeletal muscle and adipose tissue volumes: estimation from a single abdominal cross-sectional image. J Appl Physiol (1985) 97, 2333–2338, https://doi.org/10.1152/japplphysiol.00744.2004 (2004).
Tan, B. H., Birdsell, L. A., Martin, L., Baracos, V. E. & Fearon, K. C. Sarcopenia in an overweight or obese patient is an adverse prognostic factor in pancreatic cancer. Clin. Cancer Res. 15, 6973–6979, https://doi.org/10.1158/1078-0432.ccr-09-1525 (2009).
Moisey, L. L. et al. Skeletal muscle predicts ventilator-free days, ICU-free days, and mortality in elderly ICU patients. Crit. Care 17, R206, https://doi.org/10.1186/cc12901 (2013).
Javaheri, S. et al. Sleep Apnea: Types, Mechanisms, and Clinical Cardiovascular Consequences. J. Am. Coll. Cardiol. 69, 841–858, https://doi.org/10.1016/j.jacc.2016.11.069 (2017).
Strollo, P. J. et al. Upper-airway stimulation for obstructive sleep apnea. N. Engl. J. Med. 370, 139–149, https://doi.org/10.1056/NEJMoa1308659 (2014).
Murase, K. et al. Association between plasma neutrophil gelatinase associated lipocalin level and obstructive sleep apnea or nocturnal intermittent hypoxia. PLoS One 8, e54184, https://doi.org/10.1371/journal.pone.0054184 (2013).
Morimoto, T. et al. Gender differences in effects of physical activity on quality of life and resource utilization. Qual. Life Res. 15, 537–546, https://doi.org/10.1007/s11136-005-3033-2 (2006).
Ainsworth, B. E. et al. Compendium of physical activities: an update of activity codes and MET intensities. Med. Sci. Sports Exerc. 32, S498–504 (2000).
Goodpaster, B. H., Kelley, D. E., Thaete, F. L., He, J. & Ross, R. Skeletal muscle attenuation determined by computed tomography is associated with skeletal muscle lipid content. J Appl Physiol (1985) 89, 104–110 (2000).
Chen, L. K. et al. Sarcopenia in Asia: consensus report of the Asian Working Group for Sarcopenia. J. Am. Med. Dir. Assoc. 15, 95–101, https://doi.org/10.1016/j.jamda.2013.11.025 (2014).
Yoshizumi, T. et al. Abdominal fat: standardized technique for measurement at CT. Radiology 211, 283–286, https://doi.org/10.1148/radiology.211.1.r99ap15283 (1999).
Chien, M. Y., Kuo, H. K. & Wu, Y. T. Sarcopenia, cardiopulmonary fitness, and physical disability in community-dwelling elderly people. Phys. Ther. 90, 1277–1287, https://doi.org/10.2522/ptj.20090322 (2010).
Acknowledgements
The authors thank K. Ueda, Y. Ishikawa, A. Ishii, Y. Masuda, Y. Narita and R. Imai (Department of Clinical Laboratory, Graduate School of Medicine, Kyoto University) for analyzing polysomnographic data. The authors also thank N. Kimura, S. Tamura and T. Toki (Department of Respiratory Care and Sleep Control Medicine, Graduate School of Medicine, Kyoto University) for their support for this clinical research.
Author information
Authors and Affiliations
Contributions
Contribution to the study design: T. Matsumoto, K.T., K.C.; Collection of data: T. Matsumoto, K.T., R.T., T. Minami, K.M., M.I., T. Handa, T.O., T. Hirai, K.C.; Analysis and interpretation of data: T. Matsumoto, K.T., R.T., K.M., K.C.; Drafting the manuscript: T. Matumoto, K.T., R.T., K.C.; Critical revision for intellectual content: T. Matsumoto, K.T., R.T., T. Minami, K.M., M.I., T. Handa, T.O., T. Hirai, K.C.; Approval of the final version of manuscript: T. Matsumoto, K.T., R.T., T. Minami, K.M., M.I., T. Handa, T.O., T. Hirai, K.C.
Corresponding author
Ethics declarations
Competing Interests
Dr. Takeshi Matsumoto reports grants from japan Foundation for Neuroscience and Mental Health, during the conduct of the study. Dr. Kiminobu Tanizawa reports grants from the Japanese Ministry of Education, Culture, Sports, Science and Technology (16K09534), during the conduct of the study; grants from Philips-Respironics, grants from Teijin Pharma, grants from Fukuda Denshi, grants from Fukuda Lifetec Keiji, outside the submitted work. Drs. Kimihiko Murase, Morito Inouchi, and Toru Oga reports grants from Philips-Respironics, grants from Teijin Pharma, grants from Fukuda Denshi, grants from Fukuda Lifetec Keiji, outside the submitted work. Dr. Kazuo Chin reports grants from the Japanese Ministry of Education, Culture, Sports, Science and Technology (17H04182), grants from the Intractable Respiratory Diseases and Pulmonary Hypertension Research Group, the Ministry of Health, Labor and Welfare, Japan, grants from the Japan Vascular Disease Research Foundation, grants from Health, Labour and Welfare Sciences Research Grants, Research on Region Medical, grants from Japan Agency for Medical Research and Development under Grant Number JP17ek0210096, during the conduct of the study; grants and personal fees from Philips-Respironics, grants and personal fees from Teijin Pharma, grants and personal fees from Fukuda Denshi, grants and personal fees from Fukuda Lifetec Keiji, grants from KYORIN Pharmaceutical Co., Ltd, grants from Nippon Boehringer Ingelheim Co., Ltd, grants and personal fees from GlaxoSmithKline, personal fees from MSD, personal fees from Resmed, personal fees from Astellas Pharma, personal fees from Eisai Co., Ltd., outside the submitted work. Drs. Ryo Tachikawa, Takuma Minami, Tomohiro Handa, and Toyohiro Hirai declare no potential conflict of interests.
Additional information
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Matsumoto, T., Tanizawa, K., Tachikawa, R. et al. Associations of obstructive sleep apnea with truncal skeletal muscle mass and density. Sci Rep 8, 6550 (2018). https://doi.org/10.1038/s41598-018-24750-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-018-24750-z
This article is cited by
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
