
Abstract
The sense of agency refers to the feeling of initiating and controlling one’s actions and their resulting effects on the external environment. Previous studies have uncovered behavioral evidence of excessive self-attribution and, conversely, a reduction in the sense of agency in patients with schizophrenia. We hypothesize that this apparent paradox is likely to result from impairment in lower-level processes underlying the sense of agency, combined with a higher-level compensational bias. The present study employed three behavioral tasks utilizing the same stimuli and experimental design to systematically evaluate multiple factors that influence the sense of agency, including motor control, sensorimotor processing, and self-attribution. Participants’ real-time mouse movements were combined with prerecorded motions of others in ratios of 30/70, 55/45, or 80/20, with an additional angular bias of either 0° or 90°. Twenty-six patients with schizophrenia and 27 health control volunteers participated in the three tasks. Patients with schizophrenia performed significantly worse in the reaching and control detection tasks than healthy controls. However, their self-attribution in the control judgment task was comparable to that of the healthy controls. Patients with schizophrenia were impaired in motor control components and in the detection of control using sensorimotor information, but their evaluation of agency remained relatively less affected. This underscores the importance of distinguishing between different subcomponents when addressing the abnormal sense of agency in patients with schizophrenia. Subsequent cluster analysis revealed that the combined task performance accurately distinguished between the patients and healthy control participants.
Similar content being viewed by others


Introduction
The subjective feeling of being the originator of our own actions, known as the sense of agency1, plays a crucial role in how we interact with our environment2,3,4,5,6. In everyday life, we may not always consciously regulate our control, yet we typically maintain a robust sense of agency over our actions. However, this is not always the case for patients with schizophrenia. Some patients report feeling in control of events that they did not actually cause7 and sometimes feel a loss of control over their actions or thoughts8.
Previous attempts to understand abnormalities in the sense of agency in schizophrenia involved integrating the comparator model9,10,11,12, which is a widely accepted computational account of motor control13,14. The comparator model posits that humans have a forward model that processes current sensory and action signals (also known as efference copy) to predict subsequent sensory states (sensory consequences). The mismatch between this prediction and the actual sensory feedback, referred to as the prediction error, diminishes the sense of agency. For example, prior studies have revealed that neural signals that generate sensory predictions and are involved in suppressing the sensory consequences of self-generated actions are delayed in schizophrenia patients15,16,17,18,19,20. Furthermore, recent studies using the Bayesian inference framework suggest that an imbalance between the weighting of predictions and sensory input may be the reason for the abnormal sense of agency21,22,23,24,25,26,27,28. Nevertheless, understanding the complexities of the sense of agency in patients with schizophrenia requires a comprehensive approach that considers various components from the sensory-motor level to the cognitive level. However, previous empirical studies have not captured the multiple hierarchical subcomponents at different levels underlying the sense of agency in schizophrenia.
The current study focused on three hierarchical subcomponents of the sense of agency, spanning the sensory-motor level to the cognitive level: motor control, sensorimotor processing, and the self-attribution criterion. We employed three tasks, all using the same experimental design, to investigate these components. First, a reaching task was used to measure motor control when the control of an object was distorted. In this task, the participants moved a dot continuously across a screen. Their control over the dot was disturbed by adding prerecorded motion and angular bias. This task measures how well one can maintain control by adjusting their actions in response to interference. Next, we designed a control detection task to measure the control detection process based on sensorimotor information and a control judgment task to measure self-attribution based on sensorimotor information. In the control detection task, participants moved a mouse freely to trigger the motion of multiple dots on the screen and were tasked with identifying a single target dot over which they had control. This task required the detection of the controls using sensorimotor information (i.e., contingencies between intentional actions and external events) among stimuli29. Specifically, the accurate detection of control among multiple stimuli should not be influenced by the belief in control over the stimuli. Conversely, in the control judgment task, participants were asked to make a binary yes/no judgment regarding whether they felt they had control over a dot on the screen. This task required the interplay of sensorimotor processing and self-attribution criteria, which can be influenced by the belief in control. In addition, the three tasks do not distinctly measure different components underlying the sense of agency. For example, the performance of the control judgment task is likely to partially correlate with the control detection task because both require the processing of sensorimotor evidence. Importantly, by combining these three tasks, we examined the deficits in different hierarchical subcomponents underlying the sense of agency in schizophrenia, such as belief, criterion, and sensitivity. Given that schizophrenia is a complex disease and that compensatory processes are often observed to supplant deficient processes, it is crucial to carefully separate these processes to identify the root causes of abnormalities in the sense of agency.
Methods
Participants
Twenty-six right-handed patients with schizophrenia (nine females and 17 males, aged 26–56 years) and 27 right-handed nonpsychiatric healthy volunteers (nine females and 18 males, aged 24–58 years) were recruited for the present study. All the participants had normal or corrected-to-normal visual acuity. Written informed consent was obtained from all participants prior to the experiments, and they received financial compensation for their participation. Patients with schizophrenia were recruited from Keio University Hospital and Komagino Hospital in Tokyo, Japan. The study was approved by the ethics committees of Keio University Hospital, Komagino Hospital, and the University of Tokyo. An effect size of d = 0.747 was calculated from previously reported results for the duration of false-negative agency judgment between a group of patients with schizophrenia and healthy controls30. Based on this effect size, a sample size of 46 (23 in each group) was sufficient to provide a power of 0.8 (one-tailed independent-groups t-test, α = 0.05) to reveal the difference in self-control detection between the two groups31.
All patients met the criteria of the Diagnostic and Statistical Manual of Mental Disorders-532 for schizophrenia. Symptom severity and classification in the patient group were assessed using the Positive and Negative Syndrome Scale (PANSS)33 for schizophrenia (see Supplementary Material S1 for the sociodemographic data, medication information, and PANSS scores). The exclusion criteria for the study consisted of a history of neurological illness or trauma, nonpsychiatric visual or auditory disorders, a diagnosis of psychosis related to intoxication or organic brain disease, and age below 18 or above 60 years. One patient was excluded from the analysis because of the withdrawal of consent. Two healthy participants were also excluded because they made self-attributions for nearly all trials in the control judgment task, indicating a misunderstanding of the task. This resulted in a final sample of 25 patients and 25 healthy controls matched for dominant hand, age, and sex.
Tasks and procedure
The experimental tasks were conducted using a computer connected to a 17-in. LCD monitor (width 338 × height 270 mm, resolution 1280 × 1024 pixels, refresh rate 60 Hz), a keyboard, and a computer mouse. The experiments were conducted individually in a quiet room. There were three tasks: reaching, control detection, and control judgment (Fig. 1). The order of the three tasks was counterbalanced among the participants.

In the reaching task (A), participants moved the dot to touch a cross by moving the mouse. The cross disappeared and reappeared at a new possible position once it was touched. Participants were instructed to make as many touches as possible in each trial. In the control detection task (B), participants moved the mouse freely for 5 s to trigger the motion of three dots and to identify a target dot that moved in a direction corresponding to the participants’ mouse movement. In the control judgment task (C), participants moved the mouse freely to trigger the motion of the dot for 5 s and made a binary (yes or no) judgment regarding whether they felt they were able to control the movement direction of the dot.
In the reaching task, participants used a mouse to move a dot to touch a cross on the screen (Fig. 1A). The algorithm used to generate the motion of the dot and the experimental conditions were identical to those used in the other two tasks (see below). The onset, offset, and velocity of the dot motion corresponded to the participants’ mouse movement; however, the relationship between the trajectories of the dots and the participants’ mouse movements varied depending on the condition. At the beginning of each trial, a 100-pixel black cross was randomly presented at one of four positions, which were 384 pixels horizontally or vertically away from the center of the screen. A 40-pixel black dot was presented at the center of the screen. Participants were instructed to touch the cross as many times as possible in each trial. The cross disappeared once it was touched by the dot and then appeared at another position out of the three remaining possible positions. Each trial lasted for 5 s from the onset of the first mouse movement. In addition, 20 trials in which participants had full control over the dot (the dot moved in the same manner as the mouse cursor) were added to reduce frustration.
In the control detection task, participants moved the mouse freely for 5 s to detect a target dot over which they had partial control among three dots (Fig. 1B). At the beginning of each trial, three dots appeared on the screen. The initial positions of the dots were randomly generated, ensuring a minimum distance of 200 pixels between the dots and a maximum distance of 250 pixels from the center of the screen. Once the participants started to move the mouse, all the dots began to move. The onset, offset, and velocity of all the dot motions were identical and corresponded to the participants’ mouse movements; however, the relationship between the dots’ trajectories and participants’ mouse movements varied among the three dots. The motion of the target dot contained a certain proportion of the participants’ real-time mouse movements, whereas the other two dots moved in prerecorded trajectories. Five seconds after the onset of mouse movement, the three dots remained on the screen with numbers (1, 2, or 3) near each of them. The participants selected the target dot by stating its number, and the experimenter recorded their responses using a keyboard.
In the control judgment task, participants made a binary yes/no judgment regarding whether they felt they could control the dot’s direction after freely moving the mouse for 5 s (Fig. 1C). At the beginning of each trial, a black 40-pixel dot appeared at the center of the screen and started to move once the participant started to move the mouse. The participants responded by saying ‘yes’ or ‘no’ in Japanese, and the experimenter recorded their responses using a keyboard.
The direction of movement of the (target) dot was generated by combining the participants’ mouse movements and prerecorded trajectories. In each frame, the movement angle of the mouse was calculated from the offset of its position. This angle was combined with the movement angle of a randomly selected trajectory at a certain ratio34. For example, in the 80% control condition, the direction of mouse movement and the prerecorded moving direction were combined in an 80/20 ratio. The position of the dot was calculated using the magnitude of the mouse movement and the generated moving angle. The dot was redrawn at a 60 Hz refresh rate. In each task, the (target) dot contained 30%, 55%, or 80% of the participant’s mouse movements. A 0° or 90° angular bias was applied in the direction of dot movement, resulting in six conditions (3 control levels × 2 angular biases). The three levels of control were selected based on extensive prior research utilizing the same paradigm34,35,36. This selection aims to employ a minimal number of conditions (three) to capture the full psychometric function. A 90° angular bias greatly increases the discrepancy between the dot motion and mouse movement, even when the proportion of one’s own movements is large36. Each condition was repeated 10 times, resulting in 60 trials for each task, except for the reaching task. The reaching task contained 20 additional trials with 100% control and 0° angular bias, resulting in 80 trials. The trial order was randomized for each task and participant. Before each task, the participants practiced one repeat of each condition in randomized order. The tasks were programmed using MATLAB (R2017b, MathWorks) and Psychtoolbox-337. Each task took approximately 10 min. The entire experiment took approximately 45 min for each participant, including instructions, practice, and actual tasks.
Statistical analyses
The number of successful touches on the cross, detection accuracy, and proportion of yes responses were calculated for each condition in the reaching, control detection, and control judgment tasks. The average moving speed of the mouse in each trial was calculated to measure motor control performance. A 2 (group: patients vs. healthy controls) × 2 (angular bias, 0° vs. 90°) × 3 (level of control: 30%, 55%, or 80% of control) mixed-design ANCOVA was conducted on the results of each task with each participant’s average moving speed as a covariate. Two-sided tests were used for all statistics. Bonferroni correction was applied in the case of post hoc multiple comparisons. Finally, the patients and healthy controls were classified using hierarchical clustering analysis. Although diagnosis was not the main purpose of the current study, we believe that the interplay of multiple subcomponents of the sense of agency forms the whole image of an abnormal sense of agency in schizophrenia. Classification combining the results from the three tasks could provide an important understanding of how patients with schizophrenia differ from neurotypical people in terms of the complexity of agency. A cluster was named the patient cluster if it contained more patients or the healthy control cluster if it contained more healthy controls. Euclidean distance and Ward’s method were used for hierarchical clustering.
Results
Reaching task
Performance on the reaching task differed significantly between the schizophrenia and healthy control groups (Fig. 2). The mixed-design ANCOVA revealed significant main effects of group (F(1, 47) = 39.46, p < .001, partial η2 = 0.456), angular bias (F(1, 47) = 437.71, p < .001, partial η2 = 0.902), and level of control (F(2, 94) = 299.79, p < .001, partial η2 = 0.864). Patients with schizophrenia hit fewer targets than did the healthy controls in all conditions. The effect of moving speed was nonsignificant (F(1, 47) = 0.926, p = 0.341, partial η2 = 0.019). Although patients with schizophrenia moved slower in the reaching task, the individual moving speed was unable to solely explain the decreased task performance. Furthermore, there were significant interactions between angular bias and group (F(1, 47) = 30.58, p < 0.001, partial η2 = 0.394), level of control and group (F(2, 94) = 30.58, p < 0.001, partial η2 = 0.394), angular bias and level of control (F(2, 94) = 269.68, p < 0.001, partial η2 = 0.852), level of control and moving speed (F(2, 94) = 4.30, p = 0.007, partial η2 = 0.101), and the three-way interaction (F(2, 94) = 29.49, p < 0.001, partial η2 = 0.386). On the other hand, the covariate, moving speed, was not significantly related to the task performance (F(1, 47) = 0.93, p = 0.341, partial η2 = 0.019). In summary, the results revealed a significant difference in the reaching performance between the patients and the healthy controls, and this group difference cannot be solely explained by the moving speed.

The horizontal axis represents each experimental condition, including the degree of control level and angular bias. The same representation applies to the horizontal axes in Figs. 3 and 4. There were significantly fewer successful touches in the patient group than in the healthy control group. The box plot visualizes the central tendency and dispersion of the data. The central box represents the interquartile range (IQR, the middle 50% of the data). The horizontal line inside the box marks the median. The whiskers represent the smallest and largest values within 1.5 times the IQR from the lower and upper quartiles. Points outside of the whiskers indicate outliers. The same applies for the other box plots in Figs. 3 and 4.
Control detection task
Figure 3 shows detection accuracy in the control detection task for each condition for each group. A mixed-design ANCOVA with the moving speed as a covariate revealed significant main effects of group (F(1, 47) = 6.92, p = 0.011, partial η2 = 0.128) and level of control (F(2, 94) = 27.96, p < 0.001, partial η2 = 0.373). However, the effect of moving speed (F(1, 47) = 3.65, p = 0.062, partial η2 = 0.072), the main effect of angular bias (F(1, 47) = 1.60, p = 0.212, partial η2 = 0.033) were nonsignificant. None of the interactions reached the significance level. In short, the results revealed an overall drop in the ability to detect one’s control among multiple objects in patients with schizophrenia compared to healthy controls, and the moving speed of the mouse was unable to account for the results.

Patients with schizophrenia performed significantly worse than controls in the control detection task.
Control judgment task
Finally, in the control judgment task, the proportion of self-attribution did not differ between groups (Fig. 4). A mixed-design ANCOVA revealed that the main effect of the group was nonsignificant (F(1, 47) = 0.02, p = 0.884, partial η2 < 0.001). The effect of moving speed was also nonsignificant (F(1, 47) = 0.24, p = 0.626, partial η2 = 0.005). The main effects were significant of angular bias (F(1, 47) = 84.93, p < 0.001, partial η2 = 0.644) and level of control (F(2, 94) = 61.59, p < 0.001, partial η2 = 0.567), as was the interaction between angular bias and level of control (F(2, 94) = 21.74, p < 0.001, partial η2 = 0.316). The other interactions were nonsignificant.

There was no significant difference in the self-attribution task between the patient group and the group of healthy controls.
Classification of patients and healthy controls
Figure 5 shows a cluster dendrogram and a summary of the labeling using the results of the three tasks when the number of clusters was set to two. The true positive rate (proportion of correctly labeling patients as patients), false positive rate (proportion of labeling healthy controls as patients), and overall classification accuracy using this dendrogram were 72%, 0%, and 86%, respectively. In addition, although the results of the control judgment task did not reveal significant differences between groups, the overall classification accuracy dropped to 82% if the task was removed from the clustering.

Patients are labeled as 1–25, and healthy controls are labeled as 26–50. Patients who were wrongly classified as healthy controls are marked with red boxes.
Correlations with PANSS scores and treatment doses
Figure 6 shows the correlation between task performance and the PANSS scores33 for patients with schizophrenia. Performance on the reaching task was significantly correlated with PANSS negative score and total score (r = −0.417, p = 0.038; r = −0.413, p = 0.040, respectively). Performance on the control detection task was significantly correlated with PANSS negative score (r = −0.407, p = 0.044). Performance on the control judgment task was not significantly correlated with any category of PANSS scores. In addition, the task performance did not correlate with treatment doses (olanzapine equivalents38) for patients with schizophrenia (for the reaching task, r = −0.001, p = 0.995; for the control detection task, r = 0.172, p = 0.410; for the control judgment task, r = −0.111, p = 0.599).

Each panel shows the plots and linear regression of task performance against each type of PANSS score.
Discussion
Disturbances in the sense of agency, especially concerning one’s own actions and thoughts, are widely recognized as core symptoms of schizophrenia39. However, the overall mechanism by which the sense of agency is disrupted in schizophrenia, which is often reflected in contradictory symptoms, remains unclear. Empirical studies have reported both exaggerated and diminished sense of agency22,40. Controversy remains over whether the prior belief in schizophrenia is too strong41 or too weak27. In this comprehensive study, we used a combination of three behavioral tasks, all of which used a common spatially distorted stimulus, to measure multiple hierarchical subcomponents that might play essential roles in the emergence of a sense of agency: motor control, sensorimotor processing, and self-attribution criteria.
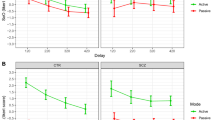
Many studies have reported that patients with schizophrenia show stronger self-attribution than healthy individuals42,43,44,45. For example, patients with schizophrenia give higher agency ratings compared to healthy controls when the events caused by their intentional actions are delayed17,43. Additionally, patients with schizophrenia also show stronger intentional binding effects46. On the other hand, some studies have also reported a weakened sense of agency in patients with schizophrenia30,40. For example, when actual control over a virtual pen was continuously switched on and off, patients with schizophrenia took longer to notice that they had gained control over the virtual pen than healthy controls30. The mechanism of an abnormal sense of agency in schizophrenia is complex, rather than a simple tendency toward either over- or under-self-attribution. It is likely a result of the imbalance between the sensory input and priors47,48,49. In our study, performance on the control detection tasks was significantly worse among patients with schizophrenia, indicating that the ability to detect control based on sensorimotor evidence was impaired in schizophrenia. However, performance in the control judgment task was comparable between healthy controls and patients with schizophrenia. This suggests that patients with schizophrenia conducted self-attribution without sufficient sensorimotor evidence, aligning with the previously reported self-attribution judgment bias. It is important to consider both sensitivity in perceptual processing and judgment bias in schizophrenia. Sensitivity refers to the ability to distinguish between sensory input caused by oneself and others, while judgment bias refers to the tendency to attribute an event to oneself. The combination of these hierarchical components may result in different patterns of results. For example, weakened sensitivity is linked with difficulties in distinguishing self from others. When such weakened sensitivity is combined with a compensatory self-attribution bias (i.e., a belief in control). The judgment bias can vary depending on the task and design of conditions. Abnormal sensitivity in perceptual processing may be more essential for understanding the symptoms of an abnormal sense of agency in schizophrenia22.
Previous studies have demonstrated that patients with schizophrenia exhibit weaker sensory attenuation50,51,52 and stronger intentional binding than healthy controls27,46. Studies using self-reported sense of agency have also indicated abnormal judgment in schizophrenia30,40,41,43,53. However, the apparent paradox of whether patients with schizophrenia have an exaggerated or diminished sense of agency has not been fully resolved22. Findings from the current study showed that patients with schizophrenia displayed a diminished ability to detect control among multiple candidates. These results suggest that even when the self-attribution results did not show significant group differences, distinguishing between sensitivity and judgment bias of sense of agency may reveal important features of the abnormality in schizophrenia54. Patients with schizophrenia likely have weakened sensitivity of the sense of agency. However, when combined with a self-attribution bias, such weakened sensitivity may be compensated. It is important for future studies to distinguish between sensitivity and judgment bias under the abnormal sense of agency in schizophrenia54. A potential reason for the impaired sensitivity of control detecting processes may be deficits in predictive processes, such as delayed corollary discharge16,17,18,19,20 and abnormal action monitoring25,27,40,43,46.
Furthermore, computational psychiatry researchers have suggested that delusions in schizophrenia may stem from an overreliance on prior beliefs and reduced use of sensory evidence28,48. Judgment biases often play a compensatory role when sensorimotor processes are dysfunctional, appearing as a strong belief in control and a lack of update from new sensory evidence when such evidence contradicts their beliefs21,22,28,48. It is not merely a single malfunctioning subcomponent of the sense of agency that is crucial; rather, the interaction among these subcomponents plays a significant role in understanding the abnormalities in the sense of agency associated with schizophrenia. It is worth including more levels of control to further assess the sensitivity and judgment bias of the psychometric function of the sense of agency for patients with schizophrenia in future studies.
Lastly, we observed correlations between the performance of the reaching task and the control detection task with the PANSS negative score, but not with the positive score. Although the delusion of control (measured by the PANSS positive score) is a prominent symptom and is considered to be linked to an abnormal sense of agency in schizophrenia55,56, the relationship between these symptoms and the impaired components underlying the sense of agency may be complex. Decreased sensitivity in the lower-level components of the sense of agency could be combined with higher-level judgment biases as compensation, resulting in varying symptom severity. On the other hand, our results suggest that negative symptoms may be more directly related to impairments in the lower-level components of the sense of agency. A previous study demonstrated a reduced sense of agency in patients exhibiting negative symptoms40. This reduction is considered to be linked to inadequate predictions in the internal model of the sensory-motor system, particularly in patients with predominantly negative symptoms, where compensatory self-attribution bias may be absent. This may explain the observed correlations with only PANSS negative scores in reaching and control detection tasks, where the lower-level components of the sense of agency were evaluated. In contrast, the mechanisms underlying positive symptoms are more complex. Positive symptoms like delusions are processed at the cognitive level of agency attribution bias.
The present study has several limitations. Firstly, patients’ processing speed may be associated with their medication. However, our data showed that treatment doses (olanzapine equivalents38) for patients with schizophrenia were not significantly correlated with task performance. While it is difficult to entirely rule out the potential influence of medication on the patients’ task performance, treatment dosages alone cannot explain the changes in the subcomponents of the sense of agency. Secondly, participants moved the mouse freely during tasks, leading to considerable individual variations in movement patterns and possibly resulting in diverse visual feedback. It would be valuable to further examine different motion strategies within these tasks. Thirdly the control detection task requires visual scanning abilities, which are often impaired in schizophrenia57,58. Future research should also assess this impairment and include it in the analysis. Lastly, the current study conducted a classification analysis and achieved an overall accuracy of 86% using the results from the three behavioral tasks. Previous studies using behaviors such as eye movements and cognitive function tests achieved a similar classification accuracy between patients with schizophrenia and healthy controls (82% for eye movement tests and 81.6% for cognitive function tests)59,60. However, these previous studies involved a much larger sample size. To provide a reliable diagnostic support tool using behavioral tasks for schizophrenia, it is necessary to conduct further experiments with a larger number of samples in future studies.
In summary, our findings suggest that the sense of agency in schizophrenia is not a unitary phenomenon but rather is composed of multiple subcomponents with different levels of impairment. Specifically, we found that sensitivity of the sense of agency, which relies on the detection of sensorimotor regularities, was significantly impaired in patients with schizophrenia. However, after being combined and compensated with the judgment bias, the self-attribution performance did not show significant differences from that of healthy individuals. This distinction between sensitivity and judgment bias offers a deeper understanding of the sense of agency in schizophrenia and could potentially guide future research and therapeutic interventions targeting specific deficits underlying this complex condition. In the future, creating tools to address the abnormal sense of agency in patients with schizophrenia might pave the way for cognitive rehabilitation and the formulation of new treatments.
Data availability
The data from the experimental tasks that support the findings of this study are available on request from the corresponding author, WW. The data are not publicly available due to their containing information that could compromise the privacy of research participants.
References
Gallagher, S. Philosophical conceptions of the self: implications for cognitive science. Trends Cogn. Sci. 4, 14–21 (2000).
Karsh, N. & Eitam, B. I control therefore I do: judgments of agency influence action selection. Cognition 138, 122–131 (2015).
Wen, W. et al. The active sensing of control difference. iScience 23, 101112 (2020).
Wen, W. et al. Perception and control: individual difference in the sense of agency is associated with learnability in sensorimotor adaptation. Sci. Rep. 11, 1–8 (2021).
Wen, W. & Haggard, P. Control changes the way we look at the world. J. Cogn. Neurosci. 30, 603–619 (2018).
Wen, W. & Imamizu, H. The sense of agency in perception, behaviour and human–machine interactions. Nat. Rev. Psychol. 1, 211–222 (2022).
Stanghellini, G. & Monti, M. R. Influencing and being influenced: the other side of ‘bizarre delusions’. 2: clinical investigation. Psychopathology 26, 165–169 (1993).
Schneider, K. Clinical Psychopathology. (Grune and Stratton, 1959).
Blakemore, S.-J., Wolpert, D. M. & Frith, C. D. Central cancellation of self-produced tickle sensation. Nat. Neurosci. 1, 635–640 (1998).
Blakemore, S.-J., Wolpert, D. M. & Frith, C. D. Abnormalities in the awareness of action. Trends Cogn. Sci. 6, 237–242 (2002).
Frith, C. D., Blakemore, S.-J. & Wolpert, D. M. Abnormalities in the awareness and control of action. Philos. Trans. R. Soc. Lond. Ser. B Biol. Sci. 355, 1771–1788 (2000).
Frith, C. D., Blakemore, S.-J. & Wolpert, D. M. Explaining the symptoms of schizophrenia: abnormalities in the awareness of action. Brain Res. Rev. 31, 357–363 (2000).
Miall, R. C. & Wolpert, D. M. Forward models for physiological motor control. Neural Netw. 9, 1265–1279 (1996).
Wolpert, D. M. & Ghahramani, Z. Computational principles of movement neuroscience. Nat. Neurosci. 3, 1212–1217 (2000).
Ford, J. M. & Mathalon, D. H. Anticipating the future: automatic prediction failures in schizophrenia. Int. J. Psychophysiol. 83, 232–239 (2012).
Ford, J. M. & Mathalon, D. H. Efference copy, corollary discharge, predictive coding, and psychosis. Biol. Psychiatry Cogn. Neurosci. Neuroimaging 4, 764–767 (2019).
Koreki, A. et al. Behavioral evidence of delayed prediction signals during agency attribution in patients with schizophrenia. Psychiatry Res. https://doi.org/10.1016/j.psychres.2015.08.023 (2015).
Okimura, T., Maeda, T., Mimura, M. & Yamashita, Y. Aberrant sense of agency induced by delayed prediction signals in schizophrenia: a computational modeling study. Schizophrenia 9, 72 (2023).
Whitford, T. J. et al. Electrophysiological and diffusion tensor imaging evidence of delayed corollary discharges in patients with schizophrenia. Psychol. Med. 41, 959–969 (2011).
Whitford, T. J., Ford, J. M., Mathalon, D. H., Kubicki, M. & Shenton, M. E. Schizophrenia, myelination, and delayed corollary discharges: a hypothesis. Schizophr. Bull. 38, 486–494 (2012).
Edwards, M. J., Adams, R. A., Brown, H., Pareés, I. & Friston, K. J. A Bayesian account of ‘hysteria’. Brain 135, 3495–3512 (2012).
Leptourgos, P. & Corlett, P. R. Embodied predictions, agency, and psychosis. Front. Big Data 3, 27 (2020).
Moore, J. W. & Fletcher, P. C. Sense of agency in health and disease: a review of cue integration approaches. Conscious. Cogn. 21, 59–68 (2012).
Moore, J. W. & Haggard, P. Awareness of action: inference and prediction. Conscious. Cogn. 17, 136–144 (2008).
Sterzer, P., Voss, M., Schlagenhauf, F. & Heinz, A. Decision-making in schizophrenia: a predictive-coding perspective. Neuroimage https://doi.org/10.1016/j.neuroimage.2018.05.074 (2018).
Synofzik, M., Vosgerau, G. & Lindner, A. Me or not me—an optimal integration of agency cues? Conscious. Cogn. 18, 1065–1068 (2009).
Voss, M. et al. Altered awareness of action in schizophrenia: a specific deficit in predicting action consequences. Brain 133, 3104–3112 (2010).
Sterzer, P. et al. The predictive coding account of psychosis. Biol. Psychiatry 84, 634–643 (2018).
Wen, W., Brann, E., Di Costa, S. & Haggard, P. Enhanced perceptual processing of self-generated motion: evidence from steady-state visual evoked potentials. Neuroimage 175, 438–448 (2018).
Werner, J. D., Trapp, K., Wüstenberg, T. & Voss, M. Self-attribution bias during continuous action-effect monitoring in patients with schizophrenia. Schizophr. Res. 152, 33–40 (2014).
Faul, F., Erdfelder, E., Lang, A.-G. & Buchner, A. G. Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 39, 175–191 (2007).
American Psychiatric Association. American Psychiatric Association: Diagnosti c and Statistical Manual of Mental Disorders. (Arlington, 2013).
Kay, S. R., Fiszbein, A. & Opler, L. A. The positive and negative syndrome scale (PANSS) for schizophrenia. Schizophr. Bull. 13, 261–276 (1987).
Wen, W. et al. Categorical perception of control. eNeuro 7, 1–11 (2020).
Nobusako, S. et al. Developmental changes in action-outcome regularity perceptual sensitivity and its relationship to hand motor function in 5–16-year-old children. Sci. Rep. 12, 17606 (2022).
Wen, W. & Haggard, P. Prediction error and regularity detection underlie two dissociable mechanisms for computing the sense of agency. Cognition 195, 104074 (2020).
Brainard, D. H. The Psychophysics Toolbox. Spat. Vis. 10, 433–436 (1997).
Leucht, S., Samara, M., Heres, S. & Davis, J. M. Dose equivalents for antipsychotic drugs: the DDD method. Schizophr. Bull. 42, S90–S94 (2016).
Nielsen, T. I. Volition: a new experimental approach. Scand. J. Psychol. 4, 225–230 (1963).
Maeda, T. et al. Reduced sense of agency in chronic schizophrenia with predominant negative symptoms. Psychiatry Res 209, 386–392 (2013).
Hur, J., Soo, J., Young, T. & Park, S. The crisis of minimal self-awareness in schizophrenia: a meta-analytic review. Schizophr. Res. 152, 58–64 (2014).
Krugwasser, A. R., Stern, Y., Faivre, N., Harel, E. V. & Salomon, R. Impaired sense of agency and associated confidence in psychosis. Schizophrenia 8, 32 (2022).
Maeda, T. et al. Aberrant sense of agency in patients with schizophrenia: forward and backward over-attribution of temporal causality during intentional action. Psychiatry Res. 198, 1–6 (2012).
Schimansky, J., David, N., Rössler, W. & Haker, H. Sense of agency and mentalizing: Dissociation of subdomains of social cognition in patients with schizophrenia. Psychiatry Res. 178, 39–45 (2010).
Tan, D. P. W., Carter, O., Marshall, D. & Perrykkad, K. Agency in schizophrenia and autism: a systematic review. Front. Psychol. 14, 1280622 (2023).
Haggard, P., Martin, F., Taylor-Clarke, M., Jeannerod, M. & Franck, N. Awareness of action in schizophrenia. Neuroreport 14, 1081–1085 (2003).
Powers, A. R., Mathys, C. & Corlett, P. R. Pavlovian conditioning–induced hallucinations result from overweighting of perceptual priors. Science 357, 596–600 (2017).
Fletcher, P. C. & Frith, C. D. Perceiving is believing: a Bayesian approach to explaining the positive symptoms of schizophrenia. Nat. Rev. Neurosci. 10, 48–58 (2009).
Berkovitch, L., Dehaene, S. & Gaillard, R. Disruption of conscious access in schizophrenia. Trends Cogn. Sci. 21, 878–892 (2017).
Hughes, G., Desantis, A. & Waszak, F. Mechanisms of intentional binding and sensory attenuation: the role of temporal prediction, temporal control, identity prediction, and motor prediction. Psychol. Bull. 139, 133–151 (2013).
Näätänen, R. & Kähkönen, S. Central auditory dysfunction in schizophrenia as revealed by the mismatch negativity (MMN) and its magnetic equivalent MMNm: a review. Int. J. Neuropsychopharmacol. 12, 125–135 (2009).
Shergill, S. S. et al. Functional magnetic resonance imaging of impaired sensory prediction in schizophrenia. JAMA Psychiatry 71, 28 (2014).
Franck, N. et al. Defective recognition of one’s own actions in patients with schizophrenia. Am. J. Psychiatry 158, 454–459 (2001).
Wen, W., Chang, A. Y.-C. & Imamizu, H. The sensitivity and criterion of sense of agency. Trends Cogn. Sci. 28, 397–399 (2024).
Bansal, S., Ford, J. M. & Spering, M. The function and failure of sensory predictions. Ann. N. Y. Acad. Sci. 1426, 199–220 (2018).
Picard, F. & Friston, K. Predictions, perception, and a sense of self. Neurology 83, 1112–1118 (2014).
Minassian, A., Granholm, E., Verney, S. & Perry, W. Visual scanning deficits in schizophrenia and their relationship to executive functioning impairment. Schizophr. Res. 74, 69–79 (2005).
Bestelmeyer, P. E. G. et al. Global visual scanning abnormalities in schizophrenia and bipolar disorder. Schizophr. Res. 87, 212–222 (2006).
Fujino, H. et al. Estimated cognitive decline in patients with schizophrenia: a multicenter study. Psychiatry Clin. Neurosci. 71, 294–300 (2017).
Morita, K. et al. Eye movement as a biomarker of schizophrenia: using an integrated eye movement score. Psychiatry Clin. Neurosci. 71, 104–114 (2017).
Acknowledgements
This study was supported by the Japan Society for the Promotion of Science (KAKENHI 24H00707, 19H05729, 21H03780, and 22H04781) and the JST FOREST Program (Grant Number JPMJFR2144).
Author information
Authors and Affiliations
Contributions
H.O.: Conceptualization, Methodology, Data collection, Analysis, Writing—original draft. W.W.: Conceptualization, Methodology, Data collection, Analysis, Writing—original draft. A.C.: Analysis, Writing—original draft. H.U.: Writing—review & editing. T.M.: Conceptualization, Methodology, Writing—original draft.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Oi, H., Wen, W., Chang, A.YC. et al. Hierarchical analysis of the sense of agency in schizophrenia: motor control, control detection, and self-attribution. Schizophr 10, 79 (2024). https://doi.org/10.1038/s41537-024-00512-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41537-024-00512-x
