
Abstract
Gait deficits are a common feature of Parkinson’s disease (PD) and predictors of future motor and cognitive impairment. Understanding how muscle activity contributes to gait impairment and effects of therapeutic interventions on motor behaviour is crucial for identifying potential biomarkers and developing rehabilitation strategies. This article reviews sixteen studies that investigate the electromyographic (EMG) activity of lower limb muscles in people with PD during walking and reports on their quality. The weight of evidence establishing differences in motor activity between people with PD and healthy older adults (HOAs) is considered. Additionally, the effect of dopaminergic medication and deep brain stimulation (DBS) on modifying motor activity is assessed. Results indicated greater proximal and decreased distal activity of lower limb muscles during walking in individuals with PD compared to HOA. Dopaminergic medication was associated with increased distal lower limb muscle activity whereas subthalamic nucleus DBS increased activity of both proximal and distal lower limb muscles. Tibialis anterior was impacted most by the interventions. Quality of the studies was not strong, with a median score of 61%. Most studies investigated only distal muscles, involved small sample sizes, extracted limited EMG features and lacked rigorous signal processing. Few studies related changes in motor activity with functional gait measures. Understanding mechanisms underpinning gait impairment in PD is essential for development of personalised rehabilitative interventions. Recommendations for future studies include greater participant numbers, recording more functionally diverse muscles, applying multi-muscle analyses, and relating EMG to functional gait measures.
Similar content being viewed by others

Introduction
Parkinson’s disease (PD) is a multisystem neurodegenerative disease with characteristic features present in both non-motor and motor domains1. The non-motor clinical manifestations include sensory impairments such as pain and tingling, depression, hyposmia and altered executive function2. The main motor symptoms are resting tremor, bradykinesia, rigidity, postural instability and gait disturbance3. This review is concerned with gait dysfunction and therefore will focus on gait and related motor symptoms.
Gait disturbance is characterised by slow shuffling steps4, asymmetry5 and high stride-to-stride variability6,7. The increased energy expenditure associated with dysfunctional gait makes even a short walk a major physical effort8, thereby restricting mobility which impacts on quality of life. Fall risk is higher in people with PD9,10, which imposes a social and economic burden through hospitalisation11 and subsequent health care costs12,13. Dopaminergic treatment may reduce some abnormal gait features such as bradykinesia and rigidity14. However, other characteristics such as gait instability may not respond to dopaminergic therapy in some people with PD due to various factors as outlined in the review by Nonnekes et al.15. Long term treatment is confounded by levodopa-induced dyskinesia, alongside fluctuations in motor response which result in the ‘ON’ and ‘OFF’ states16. Consequently, there is an urgent need to develop novel rehabilitative approaches to gait dysfunction in PD.
Optimal gait is dependent upon the functional integration of motor activity at multiple levels. At the micro level, motor units are recruited according to the ‘size principle’ to ensure graduated contraction and consequentially smooth movement17,18. At the macro level, timings of muscle contractions between synergists, antagonists and muscles acting on ipsilateral and contralateral joints are precisely regulated. This results in an energy efficient, forward propulsion of the individual’s centre of mass whilst maintaining dynamic stability. Complex neuronal networks orchestrate these constantly fluctuating muscle activation patterns. Sensorimotor integration is a key component underpinning effective locomotor neuronal networks. However, in PD, sensorimotor processing is impaired with resultant changes in motor activity patterns during gait19.

Bandpass filtered unrectified EMG signals for tibialis anterior (TA), lateral gastrocnemius (LG), biceps femoris (BF) and rectus femoris (RF) for the right (R) and left (L) legs. Onset of the stance (St) phase of walking for the right leg is indicated by solid vertical lines. Onset of the swing (Sw) phase of walking for the right leg is indicated by dashed vertical lines.
Muscle activity is generally quantitatively assessed by surface or intramuscular electromyography (EMG) which records voltage changes in muscle fibres following stimulation by α-motoneurons. Typical surface EMG signals in a healthy older adult (HOA) of four bilateral lower limb muscles during walking are shown in Fig. 1. Tibialis anterior (TA), biceps femoris (BF) and rectus femoris (RF) are active during the initial loading phase of stance with their corresponding contralateral muscles 180° out of phase. Lateral gastrocnemius (LG), an ankle plantar flexor, is important later in the stance phase for push-off of the foot. TA, an ankle dorsiflexor, is essential for foot clearance during the swing phase. BF contracts again towards the end of the swing phase, decelerating the forward moving leg prior to foot touchdown. Underpinning the timings and magnitude of EMG signals are neural networks. Different characteristics of the EMG signal therefore offer insight into the neural control of locomotion both at the micro and macro level of motor control20,21. Relative timing of motor activity onset may reveal dysfunction of sensorimotor integration. Spectral characteristics of the EMG signal may indicate altered motor unit recruitment strategies22,23 and presence of fatigue24. Multi-muscle EMG analysis and intermuscular coherence may provide information about global control networks25,26.
Studies have found characteristic EMG gait patterns in specific populations. Schmitz et al.27 have reported that HOAs, compared to healthy young controls, displayed greater LG and TA activity during stance and greater coactivation of muscles acting on the ankle joint with larger differences observed in uniarticular muscles such as soleus and vastus lateralis27. Another study observed people with diabetic neuropathy to have earlier onset of activity of soleus (SO), medial gastrocnemius (MG) and semimembranosus/semitendinosus compared to HOA28. Alterations in muscle activity patterns during walking have also been observed in people with transfemoral amputation29 and individuals with cervical spondylotic myelopathy compared to healthy controls30. However, it is not clear what changes occur in muscle activity during walking in people with PD.
Two cardinal motor features of PD likely to leave an imprint on EMG patterns during gait are rigidity and postural instability. Baradaran et al.31 observed that rigidity was associated with changes in cortical/subcortical connectivity including the supplementary motor area to the putamen together with increased excitability of the motor cortex31. One possible functional consequence of this is greater cocontraction of agonist/antagonist muscle groups and less effective recruitment of individual muscles. Manifestation of gait dynamic instability, defined as instability transitioning from one gait phase to another, may be represented by double-support time32 and greater variability of the timing of gait such as stride time33,34. A neural correlate of gait variability is the posterior putamen which is associated with automatic movement and exhibits dysfunction in people with PD35,36,37. Gait variability must necessarily be reflected in variability of EMG signals. EMG parameters may provide a better indicator of neurological dysfunction than current widely used gait parameters.
A limitation of the common gait features extracted from body-worn sensors such as inertial measurement units (IMUs), foot switches, and insole pressure sensors is they lack specificity to PD38. EMG signals differ from kinematic and kinetic features as they are directly linked to the nervous system, via the α-motoneurons. Several studies have reported differences in features of EMG during non-gait motor tasks in people with PD compared to HOAs39,40,41, from which mechanisms of motor control dysfunction in PD have been inferred. Gait dysfunction is a common motor symptom in people with PD, therefore patterns of EMG during gait are expected to differ in people with PD compared to controls. Gait EMG may therefore be a useful tool in detection of PD; however, little information is available about using gait EMG as a biomarker in PD42.
Interpretation of EMG activity is challenging, as there is high intra-individual and inter-individual variability in EMG activity patterns compared to kinematic and kinetic signals29. This is due to numerous muscles performing similar actions across joints, resulting in multiple sets of muscles able to perform a specific motor task rather than a single set, described by Latash43 as the ‘principle of abundance’43. Further compounding the difficulty is the variability of motor symptoms, both at the intra-individual level and inter-individual level. Factors affecting type and severity of motor symptoms include age, the PD phenotype, the stage of PD, type and dosage of medication, responsiveness to medication, and timing of assessment in relation to medication intake44,45.
Interventions targeting gait dysfunction in PD must necessarily modify muscle activity to achieve changes in gait kinematics and kinetics. Levodopa is the first line of treatment recommended for targeting motor symptoms in the early stages of PD46. Deep brain stimulation (DBS) is recommended for patients with advanced PD whose symptoms are not alleviated by pharmaceutical therapy (41). Krack et al.47 have reported improvements in motor function and activities of daily living in patients with PD treated with DBS over a five-year period47. Several studies observed DBS and levodopa-induced comparable improvements in gait parameters such as gait velocity48,49,50,51, step and stride length49,50,51,52, peak of moment and power at hip and ankle49,53,54, and a reduction in double-support time which suggests an improvement in balance and stability52. Levodopa and DBS can be administered individually, but the combination of both treatments have demonstrated a greater improvement in gait parameters, possibly due to working synergistically50,52. However, there are differential effects of DBS and levodopa on gait (for a review see ref. 55), and it is unclear how modification of gait parameters links to the underlying neuromuscular changes.
Understanding the neural mechanisms related to gait dysfunction is essential to improve the effectiveness of interventions, in addition to determining what aspect of the intervention is particularly beneficial. Crucial information regarding the mode of action of therapeutics on neuromuscular control and corresponding kinematics can be obtained by assessing whether they target individual muscles, groups of muscles at the network level, or affect coordination between muscles and limbs. This review will examine the effect of dopaminergic medication and DBS on muscle activity and function.
An essential element of this review is assessing the quality of the studies in terms of external and internal validity. The EMG signal is an indirect measure of muscle activity containing not only the physiological signal but also considerable noise and artefact. It is therefore vital that the EMG signal has been appropriately recorded and processed according to recommended guidelines56.
This review systematically investigates studies that have analysed EMG of lower limb muscles during walking in individuals with PD and HOA. The first aim of this review is to critically evaluate PD-related changes in EMG features during walking. A further aim is to examine the effect of dopaminergic medication and DBS on EMG activity. Understanding how muscle activity contributes to gait impairment in PD and effects of interventions is necessary for the development of personalised, evidence driven rehabilitation techniques and to identify biomarkers which may detect early PD57.
Results
Search yield
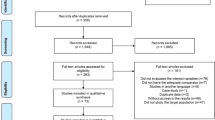
The search strategy yielded 726 studies (Fig. 2) of which 242 duplicates were removed. Studies were screened for titles and abstracts and 46 articles were retrieved for full-text screening. Data were extracted from 17 papers with two papers58,59 reporting on the same study.

The flow chart illustrates how publications were identified and the resulting 17 articles extracted following screening.
Quality assessment
Table 1 lists the overall scores derived from the quality appraisal form (see Supplementary Information) which ranged from 35% to 90% with a median score of 61%. Figure 3 depicts the number of studies scoring for each of the 20 questions. No studies scored on Q9, which related to justification of sample size and only three studies discussed sampling methods (Q9) or attachment of electrodes. Fewer than half of studies clearly outlined their hypotheses (Q7). All studies described patient characteristics (Q1), aims (Q6), main outcomes (Q8), main findings (Q10) and (Q13) validated outcome measures (Q20).

Number of studies from a total of 16 that scored for each of the 20 questions on the quality appraisal form corresponding to external validity, study information, study analysis and EMG recording and processing techniques.
Study protocol
Sample size ranged from nine60,61 to forty62 for individuals with PD and from seven63 to forty62 for healthy aged matched controls. Ages ranged from 58.3 ± 13.5 years64 to 76 ± 6 years60 for individuals with PD and from 58.0 ± 7.6 years64 to 74.4 ± 5.8 years65 for HOA. A greater proportion of males were assessed for the PD groups. Eight studies did not report on gender58,59,63,66,67,68,69,70.
Thirteen lower limb muscles were recorded in the reviewed studies with knee flexors and ankle plantarflexors being most frequently recorded60,61,62,63,64,65,67,70 and only one study measuring hip adductors65 (Fig. 4). Fourteen studies measured muscles bilaterally54,58,59,61,62,63,64,65,66,67,68,69,70,71,72, one study assessed only the right leg60 and one study the most affected leg73.

The chart is normalised to 100% of studies included in this review. The outer ring contains recorded muscles: adductor magnus (AM), biceps femoris (BF), gluteus medius (GM), lateral gastrocnemius (LG), medial gastrocnemius (MG), semimembranosus (SM), semitendinosus (ST), rectus femoris (RF), tibialis anterior (TA), vastus lateralis (VL), vastus medialis (VM). The inner ring contains the functional muscle group.
The EMG recording sessions were all restricted to a gait laboratory. Walking surfaces included level over ground walkways54,62,64,65,66,67,68,69,70,71,73 of lengths between 6 m62,65,67 and 25 m73, motorised treadmills60,66,73, split belt treadmills61,63,70, positive pressure treadmill72, a treadmill simulator73 and body unloading over a treadmill58,59 (Tables 2, 3). A range of walking speeds were investigated including twelve studies at self-selected comfortable walking speed54,60,61,62,64,65,67,68,69,70,71,73 (Tables 2, 3). In the remaining studies, treadmill speeds were set at 0.25–1.0 m/s63, 0.34 ± 0.14 m/s58,59, 0.83 m/s72 and 1.5 m/s66.
Parameters derived from EMG signals included amplitude related measures54,58,62,63,64,65,66,68,70,71,73, duration of activity72, coactivation indices63,67,73, multi-muscle activation61,70, variability60,69 and symmetry69. Amplitude normalisation was applied to the peak value obtained during walking in four studies61,67,70,73 and to the average amplitude in five studies58,59,63,69,71. One study normalised to the 95th percentile of the control group54 and another to maximum isometric voluntary contractions72. Four studies did not report amplitude normalisation methods54,62,64,68.
The number of gait cycles included for analysis ranged from ten58,59,64,65 to a minimum of twenty58,59,63,66. Some studies only described the number of trials54,71 or walking time duration70. Several did not specify the number of cycles60,62,68,69. EMG parameters were evaluated for different phases such as the entire gait cycle, initial/mid/terminal stance and early/late swing.
Muscle activity
Six studies compared differences in lower limb EMG activity patterns during walking between individuals with PD in the ON state and HOA59,62,64,65,66,72. Five studies reported conflicting findings regarding TA activity during walking. Three studies reported a reduction in MG amplitude63,65,66 during stance in individuals with PD. Three studies found differences in proximal muscle activity in the ON state with greater and more prolonged activity of proximal lower limb muscles in people with PD compared to HOA64,65,72. Two studies investigated differences in variability of lower limb muscle activity58,69. BF, TA and MG displayed greater variability in amplitude in individuals with PD compared to HOA, although MG displayed lower timing variability58,69. Three studies assessed multi-muscle activity through analysis of coactivation63,67 or muscle synergies70.
Four studies compared muscle activity during walking in the ON state with activity during the OFF state60,61,64,71. Two studies recorded increased TA activity during late swing/early stance in the ON state64,71. Cioni et al.64 additionally observed increased activity of plantarflexors during late stance64. A decrease in multi-muscle regularity derived from recurrent quantification analysis during the ON state was reported by Pourmoghaddam et al.60. Roemmich et al.61 observed that composition of muscle synergies, not the number of synergies accounting for 95% of variance, differed between the ON and OFF states, with the synergies to which VM and RF had higher weightings accounting for a greater amount of variance in the OFF state compared to the ON state61.
Two studies investigated the effect of DBS on muscle activity, with both applying DBS to the subthalamic nuclei (STN). The TA, MG, SM and RF muscles were reported to increase activation following DBS54,68.
Caliandro et al.71 described that individuals with PD who displayed a reduction in TA activity during initial stance in the OFF state had better motor function (decreased Movement Disorders Society-Unified Parkinson’s Disease Rating Scale III (MDS-UPDRS-III)) in the ON state, compared to individuals who demonstrated no difference in TA activity between ON and OFF71. Arias et al.67 reported no relationship between muscle coactivation and gait kinematics67.
Discussion
To the best of our knowledge, this is the first systematic review to report on EMG in individuals with PD during walking and the effect of dopaminergic therapy and DBS on motor behaviour. Of the sixteen studies identified, the majority reported differences in EMG parameters such as the timing and amplitude of muscle signals and muscle synergies between individuals with PD and HOA. However, in many cases results were conflicting due in part to differing protocols. Only six studies investigated the effect of dopaminergic medication or DBS on EMG activity. Notably, most studies did not relate EMG to gait or clinical measures evaluating motor symptoms severity such as the MDS-UPDRS III, indicating a major limitation in functional interpretation of EMG features and understanding gait in PD. The analysis of EMG signals in isolation without gait kinematics and kinetics or clinical measures restricts its application. Understanding the relationship between muscle activity and gait features will help identify which muscles and activation patterns underpin gait impairment and provide evidence-based support for improving the effectiveness of rehabilitation interventions by targeting specific muscles and muscle groups.
How does PD affect muscle activity?
Although differences were detected between individuals with PD and HOA, there was limited consensus regarding findings, particularly for TA, the most frequently assessed muscle. Cioni et al.64 reported that the TA displayed similar activity patterns in individuals with PD and HOA64. By contrast, Dietz et al.59 observed greater TA activity and Mitoma et al.65 reported less activity in individuals with PD59,65. Jenkins et al.62 found TA peaked later in PD compared to healthy adults62. Albani et al.66 recorded differences in TA in the ON state between freezers and non-freezers with greater activity bilaterally in the swing phase in freezers compared to HOA, whilst non-freezers showed greater activity only in the left TA66. These findings suggest differences in motor control of gait between people who exhibit freezing of gait (FoG) and those who do not freeze. The contradictory findings for TA may be accounted for in part by different processing methods and protocols. Dietz et al.59 and Mitoma et al.65, for example, did not normalise the amplitude of the signals59,65 which precludes comparison of EMG amplitudes between groups (Tables 4, 5). The walking studies were conducted on different surfaces including a level overground walkway and motorised treadmill. Warlop et al.74 reported that treadmill walking differed in individuals with PD compared to overground walking, therefore direct comparison between EMG signals collected on different surfaces may give misleading results74. Another reason for differences in TA activity is the heterogynous nature of PD, with differences in phenotype (tremor-dominant and postural instability and gait disturbance), disease duration, symptom severity and features such as FoG. Functionally, decreased TA activity reduces foot clearance75 and alters foot contact patterns which may influence fall risk. A shorter duration of TA muscle activity occurs prematurely in individuals with PD prior to freezing76.
Studies investigating the activity of MG muscle in individuals provided more conclusive results, with the majority reporting reduced activity in the PD group compared to HOA. As the MG muscle is important for forward propulsion of the body and vertical support77, a decrease in activity may result in reduced gait speed and loss of postural balance along the vertical axis. Three studies reported prolonged increased activity of knee flexors and extensors64,65,72 in individuals with PD. Biomechanically, the enhanced proximal muscle activity may compensate for the reduced function of distal muscles. Greater contraction of the quadriceps during the stance phase will increase extension of the knee, leading to greater stability in this joint during single stance which may compensate for reduced stability at the ankle joint. Greater activity of hamstrings during swing will increase hip extension and knee flexion and may replace some of the foot placement and initial loading role of the distal muscles acting on the ankle joint. Increased muscle activity entails a larger metabolic demand which may limit walking speed and mobility78. Differential compensatory changes in lower limb muscles during walking have been observed in other neurological pathologies such as post-polio syndrome and stroke79,80.
Other EMG measures determined in the reviewed articles included variability, coactivation, muscle synergies and asymmetry. Two studies assessed variability of EMG amplitude and reported greater variability of EMG for proximal and distal muscles58,69. Increased EMG variability suggests decreased automaticity of locomotor control in PD resulting from the dysfunctional putamen81. Clinically, greater gait variability is associated with higher falls risk in individuals with PD and HOA33. However, the relationship between variability and stability is complicated with a certain level of variability essential to enable adaption to perturbations82. There was conflicting evidence regarding changes in coactivation of agonists and antagonists in lower limb muscle pairs during walking in individuals with PD. Dietz et al.63 observed increased coactivation of TA and MG in people with PD during treadmill walking compared to HOA whereas Arias et al.67 reported no difference in coactivation of TA and SO when walking overground63,67. A motorised treadmill can act as an external cue resulting in reduced gait variability and altered coordination of muscles74. Only one study assessed muscle synergies and observed fewer muscle synergies accounting for 95% of variance, altered temporal profiles and a higher percentage of variability accounted for by MG, SM and BF in the PD group compared to HOA70. A reduction in muscle synergies suggests a simpler, possibly less robust, control system83. Miller et al.69 reported higher asymmetry in TA and MG activity in PD compared to HOA69. Motor and gait asymmetry are early features of PD84,85,86. Greater asymmetry is associated with the reduced integrity of callosal sensorimotor regions87 and impairment in sensorimotor integration, in addition to an increased risk of falls88.
How is muscle activity modified by interventions?
Altered contraction of individual muscles and coordination of activity between muscles underpin gait impairment in PD. Interventions targeting gait dysfunction must therefore modify activity of individual muscles and activation patterns. Evidence from the reviewed studies indicate that dopaminergic medication64,71 and STN-DBS54,68 increase the activity of distal lower limb muscles, particularly of the TA muscle. The TA has been reported to have greater projections from the cortex to its motoneurons compared to other lower limb muscles which may account for this muscle being targeted more89. The effect of enhanced muscle contraction, providing there is no increase in the antagonist muscle, is to increase the forces acting about a joint (joint moments). The functional consequence of this is increased angular velocity resulting in increased gait velocity which has been observed to occur following dopaminergic medication and STN-DBS, achieved mainly through longer step length90,91. In individuals with PD, the plantarflexors are impacted more than the dorsiflexors and there is no evidence that the dorsiflexors are weaker in individuals with PD compared to HOA. Increasing disproportionately the activity of the dorsiflexors relative to the plantarflexors will produce an imbalance in forces around the ankle joint with possible associated instability. The effect of STN-DBS on muscle function differs from that of dopaminergic medication as it increases activity of both proximal and distal lower limb muscles. Individuals with PD generally exhibit decreased activity of distal muscles and greater activity of proximal lower limb muscles as outlined in the previous section. A further increase in proximal lower limb muscle due to STN-DBS, may result in imbalance of forces across and between joints and contribute to aggravation of FoG and postural instability which has been reported following STN-DBS92.
Only one study assessed variability of gait EMG following dopaminergic medication. Pourmoghaddam et al.60 observed decreased multi-muscle regularity, determined through nonlinear analysis methods, during the ON state60. This implies increased variability of EMG patterns which could contribute to postural stability not being well controlled by dopaminergic medication, although more evidence is needed in support91. Two studies have reported that step time variability decreased with dopaminergic medication and Gilat et al.93 observed this variability was associated with altered striatal, limbic and cerebellar activity93,94.
Dopaminergic medication and STN-DBS modulate activity of similar brain structures and networks with some differences reported. Evidence indicates that dopaminergic medication and STN-DBS suppress the primary motor cortex (M1)-STN beta band (13–35 Hz) coherence95,96,97,98. Studies investigating cyclical movements of upper and lower limbs have found cortico-muscular beta coherence to be enhanced following dopaminergic medication99,100. STN-DBS has similarly been observed to increase cortico-muscular beta coherence in hand tremor101. Increased cortico-muscular beta band coherence has been linked with greater muscle activity102. Mueller et al.103 additionally reported dopaminergic medication increased connectiveness between the putamen and both the cerebellum and brainstem, with high connectivity correlated with a better motor score (UPDRS-III)103. STN-DBS has also been found to increase activity of motor cortical regions during movement and decrease activity during rest, with lower cortical activity during rest associated with clinical improvement98. These differences in brain targets may account for the varying effects dopaminergic medication and STN-DBS have on gait. In postural studies, dissimilar outcomes have also been reported, with dopaminergic medication increasing postural sway area whereas STN-DBS reduced postural sway area104.
What is the quality of the reviewed studies?
Overall, quality scores were mediocre for both non-intervention and intervention studies. The main points that studies scored low on were sample size justification, electrode placement procedures and signal processing techniques. Individuals with PD exhibit great heterogeneity and generally high inter- and intra- subject gait EMG variability105 necessitating greater sample sizes than for HOA. However, the median sample size was only twenty-two and no study in this review performed power analysis to justify their selection of participant number. Most studies included a greater proportion of males, reflecting the gender bias in PD although some studies did not specify gender. Gender differences in muscle activity during walking have previously been reported106,107 indicating it is an important factor. Only four studies determined electrode location using validated guidelines such as the SENIAM guidelines108. Identification of the optimal electrode site helps ensure the signals with higher signal to noise ratio are recorded from the selected muscle with minimal cross-talk from adjacent muscles109.
Over half of the studies did not report any signal normalisation methods59,60,61,63,65,66,69,70,71. Such normalisation is essential to allow comparisons of EMG between muscles, sessions and participants as factors such as thickness of adipose tissue, presence of oedema and number and orientation of muscle fibres will modify amplitude110,111. Excluding normalisation can invalidate subsequent results.
For the intervention specific studies, all studies excluded reports of adverse events and two studies did not state whether the researchers were blinded from measuring the main outcomes54,68. Reporting of adverse events is crucial for ensuring participant safety and determining potential confounding factors which may influence results interpretation and subsequent intervention development.
Limitations of reviewed studies
A small selection of superficial lower limb muscles was assessed during walking in individuals with PD with certain muscle groups studied less. Information about the contribution of muscles to movement is necessary for understanding compensatory mechanisms resulting in impaired gait and dynamic postural control and for developing interventions. Only one study recorded the hip adductors, a muscle group with a cross-sectional area (CSA), which relates to muscle force, comparable to the CSA of the quadriceps group, and almost three times greater than the CSA of the hamstrings112. This creates a vacuum in our knowledge of motor activity during walking in PD particularly given that mediolateral sway and instability are greater in individuals with PD113. The reviewed studies reported group differences in a wide range of EMG parameters including temporal information (muscle onset/offset), amplitude (root mean square, integrated EMG, mean amplitude of EMG), coactivation indices, synergies, symmetry/variability indices and nonlinear indices. However, spectral characteristics of the EMG signals and intermuscular coherence, which may provide information about motor unit recruitment and neuronal networks controlling muscle activity, were not analysed.
All studies were conducted in a gait laboratory with participants being closely observed whilst walking under constrained conditions. Spatio-temporal measures of gait and by implication muscle activity are modified when gait is observed overtly rather than covertly114. Only single-task walking was generally assessed. However, real-world walking involves additional activities such as walking and turning, varying walking speeds, completing complex visuomotor tasks and talking115,116. As an individual’s EMG profile will vary from day to day117, recording over multiple days and over a longer time period could permit a more accurate appraisal of motor activity to be made and also determine how motor activity changes over time and with disease progression. Repeat measurements are particularly important for individuals with PD as they will exhibit considerable fluctuation in gait depending on their medication regimes.
Thus, the current information regarding EMG activity during gait in PD is restricted in its ability to reflect the complexity of real-life walking and the capacity of the nervous system to integrate multiple neural networks to ensure safe efficient walking and facilitate gait adaptations in response to varying environmental demands. Measurement of muscle activity patterns during real-world gait over longer time periods would capture the specific motor control strategies used under these conditions that would otherwise be confounded by testing in a controlled environment. There are, however, challenges with monitoring free-living EMG, given the high sampling rate needed and low signal to noise ratio compared to wearable sensors such as accelerometers.
Limitations
This systematic review carries the usual limitations regarding restrictions imposed by the nature of literature selection. Only English-language journals were included. Studies involving gait initiation, freezing episodes, running and upper limb muscles/ tasks were excluded as inclusion criteria stipulated only walking tasks. Further studies are required to understand task-based differences in EMG activity between PD and controls as at present there is insufficient evidence in the literature to conduct this type of review.
Recommendations
This review has raised many issues regarding the limitations surrounding our current knowledge of motor activity during walking in individuals with PD. Recommendations for future studies are provided below and divided into points relating to study protocol and data processing.
Protocol considerations for EMG
-
Real-world walking. Investigating gait during real-world activity is desirable to understand motor strategies in a natural environment although current technological limitations make long term recordings challenging.
-
Sample size. Greater numbers of participants and more stride cycles are necessary.
-
Muscle selection. Muscles representing all major muscle groups acting on the ankle, knee and hip joints in the sagittal and coronal planes should ideally be recorded to permit analyses of multi-muscle activation patterns and underlying neural control systems to be undertaken.
-
Electrode placement. A clear statement must be included regarding methods used to identify electrode placement and established guidelines followed.
-
Longitudinal studies. This will inform us how motor patterns change with age and disease progression and help establish EMG characteristics as biomarkers.
-
Additional gait and cortical parameters. Parameters such as joint kinematics and kinetics as well as cortical activity measured with mobile, wireless systems such as functional near infrared spectroscopy or electroencephalography will enable us to relate EMG to gait impairment and cortical processes.
Data analytical considerations for EMG
-
Filtering and normalisation. Appropriate filtering techniques must be performed to ensure signals are physiological and not convoluted by noise. Normalisation techniques must be applied to each muscle for each individual to allow comparisons.
-
Parameter selection. Parameters should be selected that reflect underlying neural control systems, physiology and gait dysfunction. Spectral analysis, nonlinear analysis of variability, and factor analysis methods, such as nonnegative matrix factorisation, may indicate neurophysiological mechanisms. Relating EMG outcome to specific gait functions such as loading, push-off and swing is important for identifying targets for gait rehabilitation in PD.
Conclusion
Results from this review indicate individuals with PD have decreased activity of distal lower limb muscles, specifically plantarflexors, and increased activity of proximal lower limb muscles during walking compared to HOA. Variability of EMG of lower limb muscles during walking is increased in individuals with PD. Dopaminergic medication enhances activity of distal muscles and STN-DBS increases both proximal and distal muscle activity during walking. The effect of further increase in proximal muscle contraction may contribute to FoG and gait instability associated with STN-DBS. There is insufficient evidence to state how changes in muscle activation patterns directly relate to altered temporospatial gait parameters.
The findings from this review highlight the paucity of information regarding how muscles contract during walking in people with PD and how this activity relates to gait impairment. This lack of information about muscle activity is in marked contrast to the wealth of knowledge we have concerning spatio-temporal features of gait or neurodegenerative changes in the brain, requiring invasive techniques. Consequently, although gait impairment is common in PD, we cannot identify which muscles are responsible for slower walking speed or shorter steps, or why falls occur more commonly.
It is not feasible, due to insufficient data, to differentiate individuals with PD from HOA through analysis of muscle activity. Further studies must be undertaken, to enable gait EMG to be employed as a biomarker of PD and to generate personalised rehabilitation techniques targeting dysfunctional muscles. The future challenge is to develop a multi-centre project involving a large cohort of individuals with PD and HOA, which investigates a comprehensive set of muscles and extracts a range of parameters from the EMG over an extended time-period in different settings.
Methods
Search strategy
A literature search was performed in December 2019 to identify relevant articles in the following databases by one author (AI): MEDLINE (1946–2019), Embase (1974–2019), Scopus and Web of Knowledge (Table 6). The search extended back to 1946 to include articles published in the 1960s when surface EMG was first introduced, and patients were first prescribed levodopa.
Four search fields were selected linked with the conjunction ‘’OR”. MESH headings were used for Medline and Embase. Synonyms for each key term were applied. The first search field comprised the measurement technique of interest (EMG) with surface and wire/needle EMG included. The second search field focused on Parkinson’s only, excluding atypical PD and other parkinsonian disorders. The third field consisted of synonyms for walking tasks and gait characteristics. The final search field contained descriptors for the data analysis used (e.g. muscle activation patterns, muscle synergies). The searches from all four databases were combined into a citation manager with duplicates removed. Three authors (AI, AP, LA) screened suitable titles and abstracts. Full text review was performed if the suitability of a paper for inclusion was unclear. Reference lists were manually scanned during full text review to identify relevant articles.
Inclusion and exclusion criteria
Articles recording the EMG signal in individuals with PD during forward, straight line walking were included. Studies which focused on specific phases of walking such as turning, gait initiation and termination or a special type of walk such as backward walking or walking in the Timed Up and Go (TUG) test were excluded. Studies that only analysed static standing, posture and tremor or specific gait events observed in PD such as freezing of gait were excluded. Studies involving groups with pathologies outside of PD were excluded. Dopaminergic studies (ON/OFF) and DBS studies were only included when the EMG signal during a walking task was reported. Only articles written in English were considered. Reviews, abstracts, cohort studies, case studies, editorials, commentaries, discussion papers, conference proceedings and studies lacking full text were excluded. Eligibility and inclusion were determined by three reviewers (AI, AP, LA). Discrepancies were resolved through discussion resulting in a unanimous decision or a majority consensus.
Data extraction
Data extraction forms were created for each study and data were extracted independently by the reviewers (AI, AP, LA). Data extracted includes author, publication date, study aims, participant characteristics, medication state, walking surface, walking task and the key findings from the studies, muscles assessed, electrode placement, signal-processing techniques, EMG outcome measures, gait parameters and the gait duration/length analysed. Data were synthesised and formatted into tables. Tables 2 and 3 list aims, participant characteristics, medication state, walking surface, walking task and the key findings from non-intervention and intervention studies, respectively. Tables 4 and 5 contain EMG related descriptors including muscles assessed, electrode placement, signal-processing techniques, EMG outcome measures, gait parameters and the gait duration/length analysed for non-intervention and intervention studies, respectively.
Quality assessment
A customised quality appraisal form (see Supplementary Information) based on sources addressing the themes in this review was developed. The components of the quality assessment considered both internal and external validity of studies by integrating generic principles of systematic reviews118, intervention studies119,120, reviews assessing EMG and gait121,122 and standardised reporting of EMG data123,124.
External validity considers the applicability and generalisability of the study in other settings and contexts. Themes of external validity included participant characteristics and selection methods. Internal validity refers to the extent of no bias in a study validity and other aspects of research design (e.g. randomisation, blinding, study protocol consistency), and the processing of EMG data. The reviewed studies were divided into two groups: intervention and non-intervention. An additional subset of questions was included to assess the quality of intervention studies only. We defined quality of studies as low (<50%), medium (50–69%) and high (≥70%).
References
Magrinelli, F. et al. Pathophysiology of motor dysfunction in parkinson’s disease as the rationale for drug treatment and rehabilitation. Parkinsons Dis. 2016, 9832839 (2016).
Rodriguez-Oroz, M. C. et al. Initial clinical manifestations of Parkinson’s disease: features and pathophysiological mechanisms. Lancet Neurol. 8, 1128–1139 (2009).
Schrag, A., Ben-Shlomo, Y. & Quinn, N. How common are complications of Parkinson’s disease? J. Neurol. 249, 419–423 (2002).
Knutsson, E. An analysis of Parkinsonian gait. Brain 95, 475–486 (1972).
Amboni, M., Barone, P. & Hausdorff, J. M. Cognitive contributions to gait and falls: evidence and implications. Mov. Disord. 28, 1520–1533 (2013).
Blin, O., Ferrandez, A. M. & Serratrice, G. Quantitative analysis of gait in Parkinson patients: increased variability of stride length. J. Neurol. Sci. 98, 91–97 (1990).
Hausdorff, J. M. Gait dynamics in Parkinson’s disease: common and distinct behavior among stride length, gait variability, and fractal-like scaling. Chaos 19, 026113 (2009).
Nardello, F., Bombieri, F., Tinazzi, M., Schena, F. & Pellegrini, B. Metabolic and kinematic parameters during walking with poles in Parkinson’s disease. J. Neurol. 264, 1785–1790 (2017).
Gray, P. & Hildebrand, K. Fall risk factors in Parkinson’s disease. J. Neurosci. Nurs. 32, 222–228 (2000).
Allen, J. L., McKay, J. L., Sawers, A., Hackney, M. E. & Ting, L. H. Increased neuromuscular consistency in gait and balance after partnered, dance-based rehabilitation in Parkinson’s disease. J. Neurophysiol. 118, 363–373 (2017).
Ashburn, A., Stack, E., Ballinger, C., Fazakarley, L. & Fitton, C. The circumstances of falls among people with Parkinson’s disease and the use of Falls Diaries to facilitate reporting. Disabil. Rehabil. 30, 1205–1212 (2008).
Pressley, J. C. et al. The impact of comorbid disease and injuries on resource use and expenditures in parkinsonism. Neurology 60, 87–93 (2003).
Heinrich, S., Rapp, K., Rissmann, U., Becker, C. & Konig, H. H. Cost of falls in old age: a systematic review. Osteoporos. Int. 21, 891–902 (2010).
Galna, B., Lord, S., Burn, D. J. & Rochester, L. Progression of gait dysfunction in incident Parkinson’s disease: impact of medication and phenotype. Mov. Disord. 30, 359–367 (2015).
Nonnekes, J. et al. Unmasking levodopa resistance in Parkinson’s disease. Mov. Disord. 31, 1602–1609 (2016).
Marsden, C. D. & Parkes, J. D. “On-off” effects in patients with Parkinson’s disease on chronic levodopa therapy. Lancet 1, 292–296 (1976).
Henneman, E., Somjen, G. & Carpenter, D. O. Functional significance of cell size in spinal motoneurons. J. Neurophysiol. 28, 560–580 (1965).
Milner-Brown, H. S., Stein, R. B. & Yemm, R. The orderly recruitment of human motor units during voluntary isometric contractions. J. Physiol. 230, 359–370 (1973).
Lewis, G. N. & Byblow, W. D. Altered sensorimotor integration in Parkinson’s disease. Brain 125, 2089–2099 (2002).
Merletti, R. & Farina, D. Surface Electromyography: Physiology, Engineering and Applications (IEEE Press, Wiley, 2016).
Farina, D., Merletti, R. & Enoka, R. M. The extraction of neural strategies from the surface EMG. J. Appl. Physiol. 96, 1486–1495 (2004).
Pantall, A., Hodson-Tole, E. F., Gregor, R. J. & Prilutsky, B. I. Increased intensity and reduced frequency of EMG signals from feline self-reinnervated ankle extensors during walking do not normalize excessive lengthening. J. Neurophysiol. 115, 2406–2420 (2016).
Wakeling, J. M., Lee, S. S., Arnold, A. S., de Boef Miara, M. & Biewener, A. A. A muscle’s force depends on the recruitment patterns of its fibers. Ann. Biomed. Eng. 40, 1708–1720 (2012).
Merletti, R., Knaflitz, M. & De Luca, C. J. Myoelectric manifestations of fatigue in voluntary and electrically elicited contractions. J. Appl Physiol. (1985) 69, 1810–1820 (1990).
Ivanenko, Y. P., Poppele, R. E. & Lacquaniti, F. Five basic muscle activation patterns account for muscle activity during human locomotion. J. Physiol. 556, 267–282 (2004).
Boonstra, T. W. et al. Muscle networks: connectivity analysis of EMG activity during postural control. Sci. Rep. 5, 17830–17830 (2016).
Schmitz, A., Silder, A., Heiderscheit, B., Mahoney, J. & Thelen, D. G. Differences in lower-extremity muscular activation during walking between healthy older and young adults. J. Electromyogr. Kinesiol. 19, 1085–1091 (2009).
Kwon, O. Y., Minor, S. D., Maluf, K. S. & Mueller, M. J. Comparison of muscle activity during walking in subjects with and without diabetic neuropathy. Gait Posture 18, 105–113 (2003).
Pantall, A. & Ewins, D. Muscle activity during stance phase of walking: comparison of males with transfemoral amputation with osseointegrated fixations to nondisabled male volunteers. J. Rehabil. Res. Dev. 50, 499–514 (2013).
Malone, A., Meldrum, D., Gleeson, J. & Bolger, C. Electromyographic characteristics of gait impairment in cervical spondylotic myelopathy. Eur. Spine J. 22, 2538–2544 (2013).
Baradaran, N. et al. Parkinson’s disease rigidity: relation to brain connectivity and motor performance. Front Neurol. 4, 67 (2013).
Curtze, C., Nutt, J. G., Carlson-Kuhta, P., Mancini, M. & Horak, F. B. Levodopa Is a double-edged sword for balance and gait in people with Parkinson’s disease. Mov. Disord. 30, 1361–1370 (2015).
Hausdorff, J. M., Cudkowicz, M. E. & Firtion, R. Gait variability and basal ganglia disorders: stride-to-S tride variations of gait cycle timing in Parkinson’s disease and Huntington’s disease. Mov. Disord. 13, 428–437 (1998).
Baltadjieva, R., Giladi, N., Gruendlinger, L., Peretz, C. & Hausdorff, J. M. Marked alterations in the gait timing and rhythmicity of patients with de novo Parkinson’s disease. Eur. J. Neurosci. 24, 1815–1820 (2006).
Jankowski, J., Scheef, L., Huppe, C. & Boecker, H. Distinct striatal regions for planning and executing novel and automated movement sequences. Neuroimage 44, 1369–1379 (2009).
Brooks, D. J. et al. Differing patterns of striatal 18F-dopa uptake in Parkinson’s disease, multiple system atrophy, and progressive supranuclear palsy. Ann. Neurol. 28, 547–555 (1990).
Wu, T. et al. Attention to automatic movements in parkinson’s disease: modified automatic mode in the striatum. Cereb. Cortex 25, 3330–3342 (2015).
Horak, F. B. & Mancini, M. Objective biomarkers of balance and gait for Parkinson’s disease using body-worn sensors. Mov. Disord. 28, 1544–1551 (2013).
Flood, M. W., Jensen, B. R., Malling, A. S., Lowery, M. M. & Increased, E. M. G. intermuscular coherence and reduced signal complexity in Parkinson’s disease. Clin. Neurophysiol. 130, 259–269 (2019).
De Michele, G., Sello, S., Carboncini, M. C., Rossi, B. & Strambi, S. K. Cross-correlation time-frequency analysis for multiple EMG signals in Parkinson’s disease: a wavelet approach. Med. Eng. Phys. 25, 361–369 (2003).
Meigal, A. Y. et al. Non-linear EMG parameters for differential and early diagnostics of Parkinson’s disease. Front Neurol. 4, 135 (2013).
Pereira, C. R. et al. A survey on computer-assisted Parkinson’s Disease diagnosis. Artif. Intell. Med. 95, 48–63 (2019).
Latash, M. L. Biomechanics as a window into the neural control of movement. J. Hum. Kinet. 52, 7–20 (2016).
Pagano, G., Ferrara, N., Brooks, D. J. & Pavese, N. Age at onset and Parkinson disease phenotype. Neurology 86, 1400–1407 (2016).
Nieuwboer, A., De Weerdt, W., Dom, R., Bogaerts, K. & Nuyens, G. Development of an activity scale for individuals with advanced Parkinson disease: reliability and “on-off” variability. Phys. Ther. 80, 1087–1096 (2000).
National Institute for Health and Care Excellence. Parkinson’s disease in adults (NICE Guideline 71) (2018). https://www.nice.org.uk/guidance/ng71. Accessed 15 Mar 2020.
Krack, P. et al. Five-year follow-up of bilateral stimulation of the subthalamic nucleus in advanced Parkinson’s disease. N. Engl. J. Med. 349, 1925–1934 (2003).
Stolze, H. et al. Effects of bilateral subthalamic nucleus stimulation on parkinsonian gait. Neurology 57, 144–146 (2001).
Ferrarin, M. et al. Effects of bilateral subthalamic stimulation on gait kinematics and kinetics in Parkinson’s disease. Exp. Brain Res. 160, 517–527 (2005).
Faist, M. et al. Effect of bilateral subthalamic nucleus stimulation on gait in Parkinson’s disease. Brain 124, 1590–1600 (2001).
Blin, O., Ferrandez, A. M., Pailhous, J. & Serratrice, G. Dopa-sensitive and Dopa-resistant gait parameters in Parkinson’s disease. J. Neurological Sci. 103, 51–54 (1991).
Krystkowiak, P. et al. Effects of subthalamic nucleus stimulation and levodopa treatment on gait abnormalities in Parkinson disease. Arch. Neurol. 60, 80–84 (2003).
Ferrarin, M. et al. Quantitative analysis of gait in Parkinson’s disease: a pilot study on the effects of bilateral sub-thalamic stimulation. Gait & Posture 16, 135-148 (2002).
Rizzone, M. G., Ferrarin, M., Lanotte, M. M., Lopiano, L. & Carpinella, I. The dominant-subthalamic nucleus phenomenon in bilateral deep brain stimulation for Parkinson’s disease: evidence from a gait analysis study. Front Neurol. 8, 575 (2017).
Collomb-Clerc, A. & Welter, M. L. Effects of deep brain stimulation on balance and gait in patients with Parkinson’s disease: a systematic neurophysiological review. Neurophysiol. Clin. 45, 371–388 (2015).
Chowdhury, R. H. et al. Surface electromyography signal processing and classification techniques. Sensors (Basel) 13, 12431–12466 (2013).
Sherrington, C. S. The Integrative Action of the Nervous System (Yale University Press, 1920).
Dietz, A. V., Leenders, K. L. & Colombo, G. Leg muscle activation during gait in Parkinson’s disease: influence of body unloading. Electroencephalogr. Clin. Neurophysiol. Suppl. 105, 400–405 (1997).
Dietz, V. & Colombo, G. Influence of body load on the gait pattern in Parkinson’s disease. Mov. Disord. 13, 255–261 (1998).
Pourmoghaddam, A., Dettmer, M., O’Connor, D. P., Paloski, W. H. & Layne, C. S. Identification of changing lower limb neuromuscular activation in parkinson’s disease during treadmill gait with and without levodopa using a nonlinear analysis index. Parkinsons Dis. 2015, 497825 (2015).
Roemmich, R. T., Fregly, B. J. & Hass, C. J. Neuromuscular complexity during gait is not responsive to medication in persons with Parkinson’s disease. Ann. Biomed. Eng. 42, 1901–1912 (2014).
Jenkins, M. E. et al. Plantar cutaneous sensory stimulation improves single-limb support time, and EMG activation patterns among individuals with Parkinson’s disease. Parkinsonism Relat. Disord. 15, 697–702 (2009).
Dietz, V., Ziiistra, W., Prokop, T. & Berger, W. Leg muscle activation during gait in Parkinson’s disease: adaptation and interlimb coordination. Electroencephalogr. Clin. Neurophysiol./Electromyogr. Mot. Control 97, 408–415 (1995).
Cioni, M., Richards, C. L., Malouin, F., Bedard, P. J. & Lemieux, R. Characteristics of the electromyographic patterns of lower limb muscles during gait in patients with Parkinson’s disease when OFF and ON L-Dopa treatment. Ital. J. Neurological Sci. 18, 195–208 (1997).
Mitoma, H., Hayashi, R., Yanagisawa, N. & Tsukagoshi, H. Characteristics of parkinsonian and ataxic gaits: a study using surface electromyograms, angular displacements and floor reaction forces. J. Neurological Sci. 174, 22–39 (2000).
Albani, G. et al. Differences in the EMG pattern of leg muscle activation during locomotion in Parkinson’s disease. Funct. Neurol. 18, 165–170 (2003).
Arias, P., Espinosa, N., Robles-Garcia, V., Cao, R. & Cudeiro, J. Antagonist muscle co-activation during straight walking and its relation to kinematics: insight from young, elderly and Parkinson’s disease. Brain Res. 1455, 124–131 (2012).
Ferrarin, M. et al. Unilateral and bilateral subthalamic nucleus stimulation in Parkinson’s disease: effects on EMG signals of lower limb muscles during walking. IEEE Trans. Neural Syst. Rehabil. Eng. 15, 182–189 (2007).
Miller, R. A., Thaut, M. H., McIntosh, G. C. & Rice, R. R. Components of EMG symmetry and variability in parkinsonian and healthy elderly gait. Electroencephalogr. Clin. Neurophysiol. 101, 1–7 (1996).
Rodriguez, K. L., Roemmich, R. T., Cam, B., Fregly, B. J. & Hass, C. J. Persons with Parkinson’s disease exhibit decreased neuromuscular complexity during gait. Clin. Neurophysiol. 124, 1390–1397 (2013).
Caliandro, P. et al. Levodopa effect on electromyographic activation patterns of tibialis anterior muscle during walking in Parkinson’s disease. Gait Posture 33, 436–441 (2011).
Rose, M. H., Løkkegaard, A., Sonne-Holm, S. & Jensen, B. R. Effects of training and weight support on muscle activation in Parkinson’s disease. J. Electromyogr. Kinesiol. 23, 1499–1504 (2013).
Bello, O., Marquez, G. & Fernandez del Olmo, M. Effect of treadmill walking on leg muscle activation in Parkinson’s disease. Rejuvenation Res. 22, 71–78 (2018).
Warlop, T., Detrembleur, C., Stoquart, G., Lejeune, T. & Jeanjean, A. Gait complexity and regularity are differently modulated by treadmill walking in parkinson’s disease and healthy population. Front Physiol. 9, 68 (2018).
Chen, M. et al. A self-adaptive foot-drop corrector using functional electrical stimulation (FES) modulated by tibialis anterior electromyography (EMG) dataset. Med. Eng. Phys. 35, 195–204 (2013).
Nieuwboer, A. et al. Electromyographic profiles of gait prior to onset of freezing episodes in patients with Parkinson’s disease. Brain 127, 1650–1660 (2004).
Francis, C. A., Lenz, A. L., Lenhart, R. L. & Thelen, D. G. The modulation of forward propulsion, vertical support, and center of pressure by the plantarflexors during human walking. Gait Posture 38, 993–997 (2013).
Pincheira, P. A., Stenroth, L., Avela, J. & Cronin, N. J. Individual leg muscle contributions to the cost of walking: effects of age and walking speed. J. Aging Phys. Act. 25, 295–304 (2017).
Perry, J., Fontaine, J. D. & Mulroy, S. Findings in post-poliomyelitis syndrome. Weakness of muscles of the calf as a source of late pain and fatigue of muscles of the thigh after poliomyelitis. J. Bone Jt. Surg. Am. 77, 1148–1153 (1995).
Nadeau, S., Gravel, D., Arsenault, A. B. & Bourbonnais, D. Plantarflexor weakness as a limiting factor of gait speed in stroke subjects and the compensating role of hip flexors. Clin. Biomech. (Bristol, Avon) 14, 125–135 (1999).
Redgrave, P., Rodriguez, M., Smith, Y. & Rodriguez-oroz, M. C. UKPMC Funders Group Goal-directed and habitual control in the basal ganglia: implications for Parkinson’ s disease. Nat. Publ. Group 11, 760–772 (2010).
Stergiou, N. & Decker, L. M. Human movement variability, nonlinear dynamics, and pathology: is there a connection? Hum. Mov. Sci. 30, 869–888 (2011).
Neptune, R. R., Clark, D. J. & Kautz, S. A. Modular Control Hum. Walk.: A Simul. Study 42, 1282–1287 (2010).
Haas, C. T., Buhlmann, A., Turbanski, S. & Schmidtbleicher, D. Proprioceptive and sensorimotor performance in Parkinson’s disease. Res. Sports Med. 14, 273–287 (2006).
Miller-Patterson, C. et al. Motor asymmetry over time in Parkinson’s disease. J. Neurol. Sci. 393, 14–17 (2018).
Yogev, G., Plotnik, M., Peretz, C., Giladi, N. & Hausdorff, J. M. Gait asymmetry in patients with Parkinson’s disease and elderly fallers: When does the bilateral coordination of gait require attention? Exp. Brain Res. 177, 336–346 (2007).
Fling, B. W., Curtze, C. & Horak, F. B. Gait asymmetry in people with Parkinson’s disease is linked to reduced integrity of callosal sensorimotor regions. Front Neurol. 9, 215 (2018).
Boonstra, T. A., van Vugt, J. P., van der Kooij, H. & Bloem, B. R. Balance asymmetry in Parkinson’s disease and its contribution to freezing of gait. PLoS ONE 9, e102493 (2014).
Brouwer, B. & Ashby, P. Corticospinal projections to lower limb motoneurons in man. Exp. Brain Res. 89, 649–654 (1992).
Roper, J. A. et al. Deep brain stimulation improves gait velocity in Parkinson’s disease: a systematic review and meta-analysis. J. Neurol. 263, 1195–1203 (2016).
Smulders, K., Dale, M. L., Carlson-Kuhta, P., Nutt, J. G. & Horak, F. B. Pharmacological treatment in Parkinson’s disease: Effects on gait. Parkinsonism Relat. Disord. 31, 3–13 (2016).
Cossu, G. & Pau, M. Subthalamic nucleus stimulation and gait in Parkinson’s Disease: a not always fruitful relationship. Gait Posture 52, 205–210 (2017).
Gilat, M. et al. Dopamine depletion impairs gait automaticity by altering cortico-striatal and cerebellar processing in Parkinson’s disease. Neuroimage 152, 207–220 (2017).
Bryant, M. S., Rintala, D. H., Hou, J. G., Collins, R. L. & Protas, E. J. Gait variability in Parkinson’s disease: levodopa and walking direction. Acta Neurol. Scand. 134, 83–86 (2016).
Sharott, A. et al. Dopamine depletion increases the power and coherence of beta-oscillations in the cerebral cortex and subthalamic nucleus of the awake rat. Eur. J. Neurosci. 21, 1413–1422 (2005).
Williams, D. et al. Dopamine-dependent changes in the functional connectivity between basal ganglia and cerebral cortex in humans. Brain 125, 1558–1569 (2002).
Hirschmann, J. et al. Differential modulation of STN-cortical and cortico-muscular coherence by movement and levodopa in Parkinson’s disease. Neuroimage 68, 203–213 (2013).
Alhourani, A. et al. Network effects of deep brain stimulation. J. Neurophysiol. 114, 2105–2117 (2015).
Salenius, S., Avikainen, S., Kaakkola, S., Hari, R. & Brown, P. Defective cortical drive to muscle in Parkinson’s disease and its improvement with levodopa. Brain 125, 491–500 (2002).
Yoshida, T., Masani, K., Zabjek, K., Chen, R. & Popovic, M. R. Dynamic increase in corticomuscular coherence during bilateral, cyclical ankle movements. Front Hum. Neurosci. 11, 155 (2017).
Park, H. et al. Cortico-muscular coherence increases with tremor improvement after deep brain stimulation in Parkinson’s disease. Neuroreport 20, 1444–1449 (2009).
Liu, J., Sheng, Y. & Liu, H. Corticomuscular coherence and its applications: a review. Front. Human Neurosci. 13, https://doi.org/10.3389/fnhum.2019.00100 (2019).
Mueller, K. et al. Modulatory effects of levodopa on cerebellar connectivity in parkinson’s disease. Cerebellum 18, 212–224 (2019).
Rocchi, L., Chiari, L. & Horak, F. B. Effects of deep brain stimulation and levodopa on postural sway in Parkinson’s disease. J. Neurol. Neurosurg. Psychiatry 73, 267–274 (2002).
Herman, T., Weiss, A., Brozgol, M., Giladi, N. & Hausdorff, J. Gait and balance in Parkinson’s disease subtypes: objective measures and classification considerations. J. Neurol. 261, 2401–2410 (2014).
Mengarelli, A. et al. in 37th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC) (IEEE, Milan, Italy, 2015).
Chumanov, E. S., Wall-Scheffler, C. & Heiderscheit, B. C. Gender differences in walking and running on level and inclined surfaces. Clin. Biomech. (Bristol, Avon) 23, 1260–1268 (2008).
Hermens, H. J. et al. European recommendations for surface ElectroMyoGraphy. Roessingh Research and Development, 8–11, https://doi.org/10.1016/S1050-6411(00)00027-4 (1999).
De Luca, C. J. & Merletti, R. Surface myoelectric signal cross-talk among muscles of the leg. Electroencephalogr. Clin. Neurophysiol. 69, 568–575 (1988).
Lehman, G. J. & McGill, S. M. The importance of normalization in the interpretation of surface electromyography: a proof of principle. J. Manipulative Physiol. Ther. 22, 444–446 (1999).
Yang, J. & Winter, D. A. Electromyographic amplitude normalization methods: improving their sensitivity as diagnostic tools in gait analysis. Arch. Phys. Med. Rehabil. 65, 517–521 (1984).
Masuda, K., Kikuhara, N., Takahashi, H. & Yamanaka, K. The relationship between muscle cross-sectional area and strength in various isokinetic movements among soccer players. J. Sports Sci. 21, 851–858 (2003).
Galna, B., Murphy, A. T. & Morris, M. E. Obstacle crossing in Parkinson’s disease: mediolateral sway of the centre of mass during level-ground walking and obstacle crossing. Gait Posture 38, 790–794 (2013).
Robles-García, V. et al. Spatiotemporal gait patterns during overt and covert evaluation in patients with Parkinson’s disease and healthy subjects: Is there a Hawthorne effect? J. Appl. Biomech. 31, 189–194 (2015).
Contreras-Vidal, J. L. & Buch, E. R. Effects of Parkinson’s disease on visuomotor adaptation. Exp. Brain Res. 150, 25–32 (2003).
Wu, T. & Hallett, M. Neural correlates of dual task performance in patients with Parkinson’s disease. J. Neurol. Neurosurg. Psychiatry 79, 760–766 (2008).
Bogey, R., Cerny, K. & Mohammed, O. Repeatability of wire and surface electrodes in gait. Am. J. Phys. Med. Rehabil. 82, 338–344 (2003).
Oxman, A. D. Checklists for review articles. BMJ 309, 648–651 (1994).
Downs, S. H. & Black, N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J. Epidemiol. Community Health 52, 377–384 (1998).
Higgins, J. P. et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 343, d5928 (2011).
Rosa, M. C. N., Marques, A., Demain, S. & Metcalf, C. D. Lower limb co-contraction during walking in subjects with stroke: a systematic review. J. Electromyogr. Kinesiol. 24, 1–10 (2014).
Dobson, F., Morris, M. E., Baker, R. & Graham, H. K. Gait classification in children with cerebral palsy: a systematic review. Gait Posture 25, 140–152 (2007).
Merletti, R. Standards for Reporting EMG Data. J. Electromyogr. Kinesiol. 9, 3–4 (1999).
Hermens, H. J., Freriks, B., Disselhorst-Klug, C. & Rau, G. Development of recommendations for SEMG sensors and sensor placement procedures. J. Electromyogr. Kinesiol. 10, 361–374 (2000).
Acknowledgements
A.I. was financially supported by a Barbour Foundation PhD studentship.
Author information
Authors and Affiliations
Contributions
A.P. was responsible for the conception of the systematic review. A.I. performed the literature search and A.I., L.A. and A.P. screened the articles for eligibility and tabulated relevant information. All authors participated in analysis, checking accuracy, interpretation, and drafting the manuscript. All authors have approved the submitted version.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Islam, A., Alcock, L., Nazarpour, K. et al. Effect of Parkinson’s disease and two therapeutic interventions on muscle activity during walking: a systematic review. npj Parkinsons Dis. 6, 22 (2020). https://doi.org/10.1038/s41531-020-00119-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41531-020-00119-w
