
Abstract
Purpose
To evaluate whether ethnicity affects the risk of full mutation expansion among females heterozygous for FMR1 premutation.
Methods
Women who carry the FMR1 premutation alelle of Jewish origin who underwent fragile X prenatal diagnosis between 2011 and 2018 in two medical centers in Israel were included. The heterozygote women and fetuses were analyzed for the number of CGG repeats and AGG interruptions.
Results
Seven hundred sixty-six subjects were included. Parental ethnicity was fully concordant in 592 cases (Jewish, Ashkenazi, and non-Ashkenazi). Ashkenazi compared with non-Ashkenazi heterozygotes have a significantly higher mean number of CGG repeats (68 ± 8.7, 64 ± 6.4 respectively, P = 0.03) and a lower mean number of AGG interruptions (0.89 ± 0.83, 1.60 ± 1.18 respectively, p = 0.0001). Overall, 56/198 (28.2%) fetuses of Ashkenazi heterozygotes had an expansion to a full mutation compared with 6/98 among the non-Ashkenazi (6.1%) (p = 0.001). Multivariate analysis demonstrated that, in addition to CGG repeats and AGG interruptions (which contributed 68.3% of variance), ethnicity is an independent risk factor for a full mutation expansion (odds ratio [OR] = 2.04, p < 0.001) and accounted for 9% of the variation of a full mutation expansion.
Conclusion
Apart from significant differences regarding the number of CGG repeats and AGG interruptions between Ashkenazi and non-Ashkenazi heterozygotes, ethnicity independently affects the risk of a full mutation.
Similar content being viewed by others
INTRODUCTION
Fragile X syndrome (FXS; MIM 300624) is the most common form of X-linked intellectual and developmental disability, with a prevalence of 1/4,000–5,000 in males and 1/6,000–8,000 in females.1,2,3,4
The syndrome results from a full mutation expansion of a CGG trinucleotide repeat located in the 5’ untranslated region of the fragile X mental retardation (FMR1) gene to more than 200 repeats.5,6,7 Normal range of repeats is 54 CGG repeats or less. Heterozygous individuals for FMR1 premutation have 55–199 CGG repeats but do not have FXS. Heterozygotes are at risk of a full mutation expansion in gametes.8 The greater the number of repeats among these individuals, the higher the risk for a full mutation expansion.
AGG interruptions are normally located within the CGG stretch. These interruptions function as a protective factor decreasing the risk for intergenerational expansion8,9,10,11 and their absence is a risk factor for a full mutation expansion.12 Notably, AGG interruptions were even found among heterozygotes for the FMR1 full mutation also having a high number of CGG repeats.12 However, the rate of full mutation expansion among heterozygotes with more than 90 CGG repeats reaches 100% even in the presence of AGG interruptions.12
During the last several decades, a few worldwide distinct populations have been identified as possessing a unique CGG and AGG pattern. Some studies have demonstrated a minor diversity in the number of CGG repeats, and to a lesser extent in the number AGG interruptions, of unaffected individuals from various populations.4,13,14,15,16 Length differences were also detected among the premutation heterozygotes of different ethnic populations.17
Specifically, Ashkenazi and non-Ashkenazi Jewish populations were recognized as yielding a high rate of individuals who have an FMR1 premutation. Compared with non-Ashkenazi, Ashkenazi women were found to have double the rate of premutation alleles, but only regarding the lower range of premutation (fewer than 60 repeats).18 The number of AGG interruptions among Ashkenazi women was significantly higher compared with non-Ashkenazi, but only in the normal range alleles.18
To date there is no large-scale study that has evaluated the possible effect of additional factors present in the genetic background on the risk of a full mutation expansion.
We assessed the latter possibility in two (Ashkenazi and non-Ashkenazi) genetically isolated Jewish populations and hypothesized that there is a difference in the molecular characterization of the women heterozygous for a premutation allele as well as the rate of full mutation expansion between populations of different ethnic backgrounds.
MATERIALS AND METHODS
Preconception genetic screening in Israel includes FMR1 premutation heterozygosity and is offered and recommended (free of charge) for each woman who wishes to conceive.
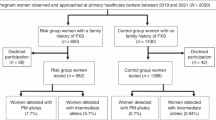
The study population included Jewish females, with FMR1 premutation with 55–199 CGG repeats, who had undergone chorionic villi sampling (CVS) or amniocentesis (AC) during the period of 2011–2018 in two large tertiary medical centers in Israel (Sheba Medical Center, Ramat Gan and Sourasky Medical Center, Tel Aviv), both located in the same geographic area. Females heterozygous for the FMR1 premutation who conceived following in vitro fertilization (IVF) for the purpose of pregestational genetic testing for monogenic disorders (PGT-M) were excluded from this study as well as women with a family or personal history of FXS. Therefore, to avoid selection bias, the included premutation heterozygotes in this study are only those detected through the preconception genetic screening mentioned above.
DNA was extracted by QiaSymphony (Qiagene®) by magnetic beads method or salting-out methods. Long range PCR for FMR1 (Asuragen, TX, USA) was performed to determine the number of CGG repeats and AGG interruptions in all women and fetuses. A detailed molecular characterization has previously been described.12 The number of CGG repeats of the fetus was compared with the maternal allele and an unstable transmission was defined as a change of at least one CGG repeat from mother to offspring.
Ethnic background (Ashkenazi or non-Ashkenazi) was determined by self-report as appeared in the medical records, as the vast majority of the Jewish population in Israel knows its family ethnic origin. The female premutation heterozygotes were divided into two groups according to their Jewish ethnic origin, Ashkenazi or non-Ashkenazi. The Ashkenazi origin was defined as having both parents from Ashkenazi origin (Western, Central, and Eastern Europe descendants) and non-Ashkenazi origin was defined as having both parents from non-Ashkenazi origin. Women who did not provide information on the ethnic origin of both parents were excluded from the study. Women who had unknown ethnic origin, a parents’ nonconcordance for ethnic background, or whose origins were different from these two specific categories (Ashkenazi and non-Ashkenazi) were excluded from the statistical analysis.
Statistical analysis was performed to compare the frequencies of CGG and AGG between Ashkenazi and non-Ashkenazi populations. The number of CGG repeats was considered as a categorical factor by splitting the number of CGG repeats into 11 categories from 55 to 199 where the width of each bin is ten.
Comparison of CGG and AGG values between ethnic groups was performed using Wilcoxon two sample test.
To determine whether ethnicity predicted the outcome measures (full mutation expansion) beyond the mother’s CGG and AGGs, we conducted a series of logistic regression tests using SAS’s PROC LOGISTIC with binomial distribution in two steps. The first step included the mother’s CGG and AGG as predictors and the second step included an additional ethnicity (Ashkenazi vs. non-Ashkenazi) as predictor. Only women with 55–90 CGG repeats were included in the logistic regression as the rate for full mutation expansion above 90 repeats is 100%.
The RsquareV sas macro19 was used to calculate an R-square measure.
Statistical analysis was performed by SAS for Windows version 9.4.
RESULTS
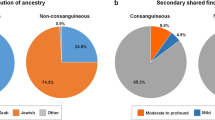
Seven hundred sixty-six women were positive for FMR1 premutation at the Sheba Medical Center and at the Sourasky Medical Center, between 2011 and 2018. Five hundred ninety-two had parents’ concordance for ethnic background, 361 Ashkenazi Jewish (60.9%), and 231 non-Ashkenazi Jewish (39.1%). One hundred and nineteen subjects did not have parents’ concordance for ethnic background, 42 were not from Ashkenazi or non-Ashkenazi origin, and in 13 cases the information regarding the ethnic background was unobtainable.
Three hundred forty-five patients from the Sheba Medical Center were included in the study (215 Ashkenazi Jewish [62.3%], 130 non-Ashkenazi Jewish [37.7%]), and 247 from the Sourasky Medical Center (146 Ashkenazi Jewish [59.1%], 101 non-Ashkenazi Jewish [40.9%]).
A comparison between the study’s populations from the two Medical Centers (Sheba and Sourasky) showed no statistically significant difference regarding the number of CGG repeats, AGG interruptions, and the effect of the ethnic background as an independent risk factor for a full mutation expansion. A total of 568 participants with parents’ concordance underwent CVS/AC during their pregnancy during this period.
The affected allele was transmitted to the fetus in 314/568 (55.3%) of pregnancies and the nonaffected allele was transmitted in 254/568 pregnancies (44.7%) (p = 0.01).
The mean number of CGG repeats among the Ashkenazi heterozygotes for FMR1 premutation was slightly yet significantly higher compared with non-Ashkenazi women (68 ± 8.7, 64 ± 6.4 respectively, p = 0.03, see Table 1). The mean number of AGG interruptions was significantly lower in Ashkenazi women as well (0.89 ± 0.83, 1.60 ± 1.18 respectively; p = 0.0001, see Table 2). Moreover, 128/361 (35.4%) of the Ashkenazi heterozygous for the premutation had no AGG interruptions compared with 47/231 (20.3%) of the non-Ashkenazi women (p = 0.011). Specifically, 19.9% of Ashkenazi participants had 2 AGG interruptions while this rate among non-Ashkenazi women was almost double (36.3%) (Table 2).
The rate of full mutation expansions among the fetuses in which the affected allele was transmitted was 56/198 (28.2%) among the Ashkenazi fetuses and 6/98 among the non-Ashkenazi (6.1%) (p < 0.001) (Fig. 1). The lowest number of CGG repeats that caused a full mutation expansion among Ashkenazi heterozygotes was 62 while among non-Ashkenazi ones this number was 75 repeats. There were no cases of a full mutation expansion among women with two or more AGG interruptions in both ethnic groups (Figs. 1, 2).

The full mutation expansion rate (in percentage of cases) among Ashkenazi heterozygotes’ fetuses are presented according to the number of CGG repeats and AGG interruptions. The number of CGG repeats are binned at groups of 5. Number of CGG interruptions are described as 0 (no interruptions), or 1 (a single interruption). Absence of bars represent no full mutation expansion for the specific group.

The full mutation expansion rate (in percentage of cases) among non-Ashkenazi heterozygotes’ fetuses are presented according to the number of CGG repeats and AGG interruptions. The number of CGG repeats are binned at groups of 5. The number of CGG interruptions are described as 0 (no interruptions), or 1 (a single interruption). Absence of bars represent no full mutation expansion for the specific group.
To test whether ethnic background is an independent risk factor, we performed multivariate analysis using CGG repeats, AGG interruptions, and ethnic background. This model demonstrated that the likelihood of a full mutation expansion significantly rises in each 1-unit increase of CGG (odds ratio [OR] = 1.24, p < 0.001) and significantly decreases in each 1-unit increase of AGG (OR = 0.51, p < 0.001). Overall, heterozygosity for CGG repeats in the premutation range, combined with AGG interruptions, accounted for 68.3% of the variation in a full mutation expansion.
Ashkenazi ethnic background independently increased the risk of a full mutation expansion compared with non-Ashkenazi origin (OR = 2.04, p < 0.001) and accounted for 9% of the variation in full transmission.
A comparison between Ashkenazi and non-Ashkenazi heterozygotes did not demonstrate a significant difference regarding their mean age or the number of pregnancies per woman.
DISCUSSION
This study detected three significant parameters that affect the risk of a full mutation expansion among females who are heterozygous for the FMR1 premutation. Of these, two CGG repeats and AGG interruptions are bona fide factors. However, by focusing on a large genetically isolated population (Jewish of Ashkenazi and non-Ashkenazi origin) the study showed, for the first time, to the best of our knowledge, that ethnic background may contribute to a full mutation expansion among female FMR1 premutation heterozygotes. The ethnicity contribution was still modest compared with the well-known factors being only 9% of the tendency for a full mutation expansion compared with 68.3% of CGG repeats and AGG interruptions.
The difference in CGG repeats we detected between Ashkenazi and non-Ashkenazi women was in concordance with a previous study performed on women with normal and intermediate-range CGG repeats.18 However, while in our previous study we found that Ashkenazi female premutation heterozygotes have a higher number of AGG interruptions,18 our current study revealed that among the premutation range heterozygotes, the number of AGG interruptions is lower among Ashkenazi women compared with non-Ashkenazi women. Of note, the differences in these results may be attributed to the fact that the previous study was a population-based study that included screening thousands of women for the FMR1 premutation, while this study only included women who had already been recognized (due to a screening test or family history) to have a premutation. These data have demonstrated a significant difference between the groups regarding the rate of a full mutation expansion. In addition to the difference in the absolute numbers of CGG repeats between groups, the lowest number of repeats that was associated with a full mutation expansion was lower among the Ashkenazi when compared with non-Ashkenazi women (62 vs. 75). This finding may reflect even more pronouncedly the impact of the ethnic background upon the intergenerational expansion process. In concordance with previous studies,12 we demonstrated that AGG interruptions diminish the risk of a full mutation expansion and that the risk is very minimal among females heterozygous for the premutation with two AGGs or more.
It is not surprising that the ethnic effect was detected among the Jewish population, as this population, especially the Ashkenazi one, was restricted and secluded for many years, decreasing genetic heterogeneity. It is similar to the fact that the BRCA1/2 genes were detected as genetic predisposition genes among the Ashkenazi populace.20,21
These data presented herein suggest the existence of further inherited components affecting the mother-to-offspring transmission process, which are different between individuals and not necessarily related to a specific ethnicity. These factors altogether may explain the variation in the tendency to a full mutation not explained by CGG repeats and AGG interruptions. Indeed, preceding studies demonstrated that haplotype analysis of normal and premutated chromosomes among various populations showed that a substantial proportion of all fragile X chromosomes show linkage disequilibrium with a small subset of DXS548-FRAXAC2-FRAXAC1 haplotypes.22,23,24 These findings are even more pronounced in secluded and genetically isolated populations.25,26
An unusually high incidence of CGG repeat sequences lacking AGG interruptions and significantly higher rate of heterozygosity for intermediate-range and premutation-range alleles were found among the Tunisian and Djerba-origin Jewish population in Israel. These populations have a tendency toward a full mutation expansion, even when compared with other women who are heterozygous for a premutation allele with the same CGG repeat length.27 These unique findings are related to a previously reported haplotype that is believed to account for all observed cases of disease among Tunisian Jewish X chromosomes.27
These findings are in the same line of genetic studies that identified families in which the rate of a full mutation expansion was excessively high, regardless of the CGG repeat number and AGG interruptions.28,29,30 It is possible that these families harbor additional genetic components associated with the expansion, as suggested in our work.
We believe that the Ashkenazi Jewish population is just one example of a secluded population with consequent distinct genetic features that may therefore explain the aforementioned phenomenon. Other populations, families, and individuals may display similar characteristics. It is possible, of course, that while some of these factors increase the risk of a full mutation expansion, some will decrease the risk.
Our findings suggest that the genetic counseling for females heterozygous for FMR1 premutation should put more emphasis upon personal and family history, as well as ethnic background, as these factors are associated with the tendency toward a full mutation expansion among female premutation heterozygotes beyond the CGG repeats and the AGG interruptions. Further research is needed to find the inherited elements that cause the increased risk for a full mutation expansion associated with given origins, haplotypes, and families and to identify other ethnic groups at risk worldwide. Such findings may also help to improve the understanding of the disease biology and maybe detect targetable elements for therapeutic interventions.
In summary, our findings support the hypothesis that there are significant differences regarding the number of CGG repeats and AGG interruptions between different ethnic groups and that there are additional factors that affect the process of intergenerational expansion to a full mutation, apart from the CGG repeats and the AGG interruptions.
Once validated, the supplementation of ethnic background, as well as the specific behavior of the mutation expression in given families, may contribute to precise genetic counseling, providing valuable information and helping identify specific FMR1 premutation heterozygotes at higher risk for instability in future generations.
Data availability
The clinical database that was used for this manuscript is available for sharing upon request.
References
Crawford, D. C., Acuna, J. M. & Sherman, S. L. FMR1 and the fragile X syndrome: human genome epidemiology review. Genet. Med. 3, 359–371 (2001).
De Vries, B. B. et al. Screening and diagnosis for the fragile X syndrome among the mentally retarded: an epidemiological and psychological survey Collaborative Fragile X Study Group. Am. J. Hum. Genet. 61, 660–667 (1997).
Coffee, B. et al. Incidence of fragile X syndrome by newborn screening for methylated FMR1 DNA. Am. J. Hum. Genet. 85, 503–514 (2009).
Hill, M. K., Archibald, A. D., Cohen, J. & Metcalfe, S. A. A systematic review of population screening for fragile X syndrome. Genet. Med. 12, 396–410 (2010).
Oberle, I. et al. Instability of a 550-base pair DNA segment and abnormal methylation in fragile X syndrome. Science. 252, 1097–1102 (1991).
Verkerk, A. J. et al. Identification of a gene FMR-1 containing a CGG repeat coincident with a breakpoint cluster region exhibiting length variation in fragile X syndrome. Cell. 65, 6–15 (1991).
Yu, S. et al. Fragile X genotype characterized by an unstable region of DNA. Science. 252, 1179–1181 (1991).
Nolin, S. L. et al. Fragile X analysis of 1112 prenatal samples from 1991 to 2010. Prenat Diagn. 31, 925–931 (2011).
Yrigollen, C. M. et al. AGG interruptions within the maternal FMR1 gene reduce the risk of offspring with fragile X syndrome. Genet. Med. 14, 729–736 (2012).
Nolin, S. L. et al. Fragile X full mutation expansions are inhibited by one or more AGG interruptions in premutation carriers. Genet. Med. 17, 358–364 (2015).
Nolin, S. L. et al. Fragile X AGG analysis provides new risk predictions for 45–69 repeat alleles. Am. J. Med. Genet. A 161A, 771–778 (2013).
Domniz, N. et al. Absence of AGG interruptions is a risk factor for full mutation expansion among Israeli FMR1 premutation carriers. Front Genet. 9, 606 (2018).
Pastore, L. M., Manichaikul, A., Wang, X. Q. & Finkelstein, J. S. FMR1 C. G. G. repeats: reference levels and race-ethnic variation in women with normal fertility (Study of Women’s Health Across the Nation). Reprod. Sci. 9, 1225–1233 (2016).
Yrigollen, C. M. et al. AGG interruptions and maternal age affect FMR1 CGG repeat allele stability during transmission. J. Neurodev. Disord. 6, 24 (2014).
Genereux, D. P. & Laird, C. D. Why do fragile X carrier frequencies differ between Asian and non-Asian populations? Genes Genet. Syst. 88, 211–224 (2013).
Tzeng, C. C. et al. Prevalence of theFMR1mutation in Taiwan assessed by large-scale screening of newborn boys and analysis of DXS548-FRAXAC1 haplotype. Am. J. Med. Genet. A. 133A, 37–43 (2005).
Owens, K. M. et al. FMR1 premutation frequency in a large, ethnically diverse population referred for carrier testing. Am. J. Med. Genet. A. 176, 1304–1308 (2018).
Weiss, K. et al. Ethnic effect on FMR1 carrier rate and AGG repeat interruptions among Ashkenazi women. Genet. Med. 16, 940–944 (2014).
Zhang, D. A coefficient of determination for generalized linear models. Am. Stat. 71, 310–316 (2017).
Mangold, K. A., Wang, V., Weissman, S. M., Rubinstein, W. S. & Kaul, K. L. Detection of BRCA1 and BRCA2 Ashkenazi Jewish founder mutations in formalin-fixed paraffin-embedded tissues using conventional PCR and heteroduplex/amplicon size differences. J. Mol. Diagn. 12, 20–26 (2010).
Manchanda, R. et al. Population testing for cancer predisposing BRCA1/BRCA2 mutations in the Ashkenazi-Jewish community: a randomized controlled trial. J. Natl Cancer Inst. 107, 379 (2014).
Eichler, E. E. et al. Haplotype and interspersion analysis of the FMR1 CGG repeat identifies two different mutational pathways for the origin of the fragile X syndrome. Hum. Mol. Genet. 5, 319–330 (1996).
Richards, R. I. et al. Evidence of founder chromosomes in fragile X syndrome. Nat. Genet. 1, 257–260 (1992).
Buyle, S. et al. Founder effect in a Belgian-Dutch fragile X population. Hum. Genet. 92, 269–272 (1993).
Haataja, R., Vaisanen, M. L., Li, M., Ryynanen, M. & Leisti J. The fragile X syndrome in Finland: demonstration of a founder effect by analysis of microsatellite haplotypes. Hum. Genet. 94, 479–483 (1994).
Oudet, C., von Koskull, H., Nordstrom, A. M., Peippo, M. & Mandel, J. L. Striking founder effect for the fragile X syndrome in Finland. Eur. J. Hum. Genet. 1, 181–189 (1993).
Falik-Zaccai, T. S. et al. Predisposition to the fragile X syndrome in Jews of Tunisian descent is due to the absence of AGG interruptions on a rare mediterranean haplotype. Am. J. Hum. Genet. 60, 103–112 (1997).
Saldarriaga, W. et al. Genetic cluster of fragile X syndrome in a Colombian district. J. Hum. Genet. 63, 509–516 (2018).
Field, M. et al. Significantly elevated FMR1 mRNA and Mosaicism for methylated premutation and full mutation alleles in two brothers with autism features referred for fragile X testing. Int. J. Mol. Sci. 20, 3907 (2019).
Tabolacci, E. et al. Methylated premutation of the FMR1 gene in three sisters: correlating CGG expansion and epigenetic inactivation. Eur. J. Hum. Genet., 2, 567–575 (2020).
Acknowledgements
This work was partially supported by The Azrieli Foundation Canada–Israel.
Author information
Authors and Affiliations
Contributions
Conceptualization: N.D., S.E., Y.C., Y.Y., S.B.-S. Data curation: N.D., L.R.L. Formal analysis: N.D. Funding acquisition: S.E., H.R.,S.B.-S. Investigation: N.D. Methodology: N.D., L.R.L., M.B., E.P., S.E., S.B.-S. Resources: N.D., Y.Y., L.R.L., D.B.G. Software: N.D. Supervision: Y.C., L.R.L, M.B., E.P., S.B.-S. Validation: N.D., L.R.L. Visualization: N.D., S.B.-S. Writing—original draft: N.D. Writing—review & editing: S.B.-S., S.E., H.R., Y.C., L.R.L.
Corresponding author
Ethics declarations
Ethics declaration
The study was reviewed and approved by the institutional review board (IRB) of both medical centers: IRB 3786-16 SMC (Sheba Medical Center, Ramat Gan, Israel) IRB 0546-09 TLV (Sourasky Medical Center, Tel Aviv, Israel). The data were obtained anonymously from the clinical database. Given the retrospective and aggregative nature of the data, an informed consent was not required by the local IRB committee. All individual-level data, including clinical data, were completely de-identified.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Domniz, N., Levavi, L.R., Berkenstadt, M. et al. Ethnicity has a multiplex impact upon the risk of a full mutation expansion among female heterozygotes for FMR1 premutation. Genet Med 23, 1023–1027 (2021). https://doi.org/10.1038/s41436-020-01089-3
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41436-020-01089-3
