
Abstract
Objectives
To compare rates of change in peripapillary retinal nerve fibre layer (pRNFL) and macular ganglion cell-inner plexiform layer (mGCIPL) parameters among different race-ethnicities from a large electronic health record database of subjects with or suspected of glaucoma.
Methods
In this retrospective cohort study, rates of change were obtained using joint longitudinal linear mixed models for eyes with ≥3 visits and ≥1 year of follow-up, adjusting for age, sex, intraocular pressure, central corneal thickness, and baseline pRNFL and mGCIPL thickness. Best linear unbiased predictor estimates of various parameters were stratified by baseline glaucoma severity and analysed by racial-ethnic group.
Results
A total of 21,472 spectral domain optical coherence tomography (OCT) pRNFL scans and 14,431 mGCIPL scans from 2002 eyes were evaluated. A total of 200 (15.6%) and 601 (46.8%) subjects identified as non-Hispanic Black (NHB) and Hispanic, respectively. NHB eyes exhibited faster rates of change in pRNFL among glaucoma suspect (global pRNFL −0.57 ± 0.55 µm/year vs. −0.37 ± 0.62 µm/year among Hispanics, p < 0.001), mild glaucoma (superior pRNFL quadrant −1.20 ± 1.06 µm/year vs. −0.75 ± 1.51 µm/year among non-Hispanic Whites (NHW), p = 0.043), and moderate glaucoma eyes (superior pRNFL quadrant −1.31 ± 1.49 µm/year vs. −0.52 ± 1.26 µm/year among Hispanics, p = 0.003). NHB eyes exhibited faster rates of mGCIPL loss corresponding to pRNFL rates. Global pRNFL and mGCIPL rates were strongly correlated (R2 = 0.70).
Conclusions
Adjusted rates of pRNFL and mGCIPL loss significantly differed between racial-ethnic groups when stratified by glaucoma severity, with faster rates among NHB patients. These differences highlight key racial-ethnic disparities in adjusted rates of glaucoma OCT parameters.
Similar content being viewed by others

Introduction
Glaucoma is a progressive, multifactorial optic neuropathy accompanied by characteristic structural changes and functional visual field loss [1, 2]. It is estimated that nearly 70 million people have been diagnosed with the disease, a number which is expected to increase [3]. Diagnosis and management of glaucoma rely on the detection of disease progression, commonly assessed using standard automated perimetry (SAP) and optical coherence tomography (OCT) [4, 5]. SAP has been used as the main or secondary outcome measures of disease progression in major glaucoma treatment trials [6, 7]. However, structural changes typically precede SAP abnormalities [8]. OCT provides an objective analysis of structural damage to the peripapillary retinal nerve fibre layer (pRNFL) and inner retina in the macula to assess glaucomatous progression. The latter has been described by various parameters such as the ganglion cell layer, ganglion cell complex, and macular ganglion cell-inner plexiform layer (mGCIPL) [9, 10].
Several prospective and retrospective studies have described pRNFL and inner retinal changes in glaucoma patients [9,10,11,12,13]. However, most have focused on smaller populations, suggesting the value of analysing larger clinical databases of patients receiving routine care [9,10,11,12,13,14]. The lack of racial and ethnic diversity in prospective studies restricts their applicability to heterogenous clinical populations [15]. In addition, studies have reported that individuals of African descent have a higher risk of visual impairment from glaucoma compared to those of European descent [16]. However, potential differences in rates of change in OCT parameters between different racial-ethnic groups have not been investigated using a large population receiving routine care.
The purpose of this study was to characterise rates of change in pRNFL and mGCIPL OCT parameters from a large database of glaucoma patients derived from an electronic health record (EHR) system of a tertiary eye care institution that cares for a diverse racial-ethnic population. We aimed to evaluate how jointly modelled rates of pRNFL and mGCIPL parameters differed between racial-ethnic groups when stratified by baseline disease severity and adjusted for key ocular and demographic characteristics.
Methods
The University of Miami institutional review board approved this study (protocol #20191100). However, a waiver for obtaining informed consent was granted due to the retrospective nature of this research. The study adhered to the Declaration of Helsinki and the Health Insurance Portability and Accountability Act.
Inclusion & exclusion criteria
This analysis was a retrospective study of patients from the Bascom Palmer Glaucoma Repository (BPGR). This database contains demographic, exam, imaging, and procedural data of eyes with glaucoma or suspected of having glaucoma examined at the clinical sites of the Bascom Palmer Eye Institute (BPEI), identified using International Classification of Diseases (ICD) codes (Supplementary Table 1) from the electronic health record (EHR) system (Epic Systems, Verona, WI). Patients were all aged 18 years or older at the time of first visit. The BPGR contains data from over 70,000 patients. Tests from any eyes that were diagnosed with exclusionary diagnoses (Supplementary Table 2) were excluded if they followed the first date of any of these diagnoses. All pRNFL and mGCIPL data using the Zeiss Cirrus spectral-domain OCT system were extracted from Zeiss Forum (Carl Zeiss Meditech, Dublin, CA). OCT data were available beginning April 2008. All data available as of February 1, 2022 were collected. For this study, we extracted OCT, demographic, central corneal thickness (CCT), and intraocular pressure (IOP) data from the BPGR.
OCT data preparation
OCT scans were required to have a signal strength of 7 of 10 or greater. Any pRNFL OCT scans with global pRNFL values less than 30 µm or greater than 130 µm were eliminated as similarly completed in prior studies [17]. Based on the expected range of global mGCIPL values [18, 19], mGCIPL OCT scans with global thickness values greater than 105 µm and less than 33 µm were eliminated. In addition, any mGCIPL scans with “xxx” assigned to any sector values were eliminated. Based on the pRNFL “floor” of the Cirrus OCT system [20], eyes that had a global pRNFL thickness <57 µm at baseline were eliminated. Any tests that followed glaucoma surgery (trabeculectomy, aqueous shunt insertion, cyclophotocoagulation – identified by Current Procedural Terminology (CPT) codes 66710, 66172, 0192 T, 66183, 66179, 66180, 66710, and 66711) were excluded.
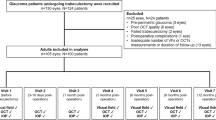
Subjects were required to have ≥ 3 visits with high-quality pRNFL and mGCIPL OCT scans over a minimum of 12 months of follow-up, following the study design of a recent large population study [17]. Only those pRNFL OCT scans that were performed within the same period as the mGCIPL scans were included to evaluate concurrent rates. Only those eyes that had CCT measurements, IOP data, and a 24-2 visual field with false positives < 15% and fixation losses < 33% within 12 months of the first RNFL scan were included. This baseline visual field was used to stage the eye using Hodapp-Anderson-Parrish (HAP) criteria as suspect, mild, moderate, or severe as previously completed [17, 21].
Statistical analysis
We modelled rates of change in pRNFL and mGCIPL parameters using joint longitudinal linear mixed models. Linear mixed modelling has been used extensively in glaucoma research by various groups [5, 14, 21,22,23]. In brief, these models provide improved estimates of rates of change compared to traditional ordinary least squares regression by borrowing strength from population data; eyes with fewer tests borrow strength from the population. These models estimate the average rate of change of a predictor variable as a function of time and includes subject and eye-specific random effects, which function as adjustments to provide unique estimates for each eye. Joint longitudinal modelling has been utilised previously in glaucoma research to model related outcome measures [24, 25]. This approach leads to a shared distribution of random effects for the two predictor variables, thereby reducing the degree of measurement error and thus allowing for an improved assessment of the true relationship between outcome variables [8].
In this study, we modelled anatomically related pRNFL and mGCIPL parameters together in separate joint longitudinal mixed models: the superior pRNFL quadrant was modelled with superior and superotemporal mGCIPL sectors, the inferior pRNFL quadrant was modelled with inferior and inferotemporal mGCIPL sectors, and the temporal pRNFL quadrant was modelled with superonasal and inferonasal mGCIPL sectors. In an alternate model, superonasal and inferonasal mGCIPL sectors were modelled with the superior and inferior pRNFL quadrants respectively, but results were noted to be similar to the original models. Given the lack of an anatomic relationship between macular OCT parameters and the nasal pRNFL quadrant, the latter was modelled alone in a traditional linear mixed model. With respect to global indices, we modelled global pRNFL with global and minimum mGCIPL values. Estimates of rates of change for each of these parameters for individual eyes were obtained from best linear unbiased prediction (BLUP) [7, 25]. Of note, we accounted for inter-eye correlations by clustering measurements by eye. More complex models including nesting within patient did not improve model performance as assessed by Bayesian information criterion and BLUP estimates, and thus the simpler models were utilised.
Extracted demographics included date of birth, sex, self-reported race, and self-reported ethnicity. Age was calculated at the date of the first visit. In accordance with the study design of a recent large population study, patients were grouped as Non-Hispanic White (NHW), Non-Hispanic Black (NHB), Hispanic, or Other based on self-report [26]. Patients that did not identify with the first three categories or declined to answer were classified as Other. Models adjusted for age, sex, CCT, mean IOP, and baseline pRNFL and mGCIPL thickness, which were centred on their respective population means. Only IOP data between the first and last OCT scans were used to calculate mean IOP. Statistical comparisons between rates of racial-ethnic groups were completed using the Kruskal-Wallis rank sum test. Pairwise comparisons were completed using Dunn test with Bonferroni correction for multiple comparisons. P-values presented have been adjusted for multiple comparisons. All analyses were completed in R version 4.2.2 (R Foundation for Statistical Computing, Vienna, Austria).
Results
A total of 2002 eyes from 1284 subjects (mean age 65.9 ± 11.8 years) were included in the study. Most subjects were female (61.8%), and 423 (32.9%) subjects identified as NHW, 200 (15.6%) as NHB, 601 (46.8%) as Hispanic, and 60 (4.7%) as Other (Table 1). Overall, 21,472 OCT pRNFL and 14,431 OCT mGCIPL scans were analysed. Table 2 summarises eye-level characteristics of the cohort, classified by glaucoma severity and racial-ethnic group. Of the 2002 eyes, 1,118 (55.8%) eyes had a normal visual field (and thus were labelled as “glaucoma suspect” in this study), 440 (22.0%) eyes were classified as having mild disease, 237 eyes (11.8%) were classified as moderate, and 207 eyes (10.3%) were identified as having severe glaucoma at baseline. Statistically significant differences (p < 0.001) were observed among the groups for baseline SAP MD, pRNFL thickness, mGCIPL thickness, CCT, and mean IOP (Table 2). However, the effect sizes of these differences were relatively small except for CCT. Follow-up time (mean 3.2 ± 1.0 years) and number of visits per patient (mean 3.8 ± 0.9 visits) were similar between groups (p = 0.13 and p = 0.40 respectively).
Differences in pRNFL rates
Among glaucoma suspects, the mean adjusted rate of change for global pRNFL thickness was −0.44 ± 0.60 µm/year (Table 3 and Supplementary Fig. 1). A statistically significant difference among racial-ethnic groups was noted (p < 0.001). NHB eyes had faster rates of change in global pRNFL compared to Hispanics (−0.57 ± 0.55 µm/year vs. −0.37 ± 0.62 µm/year, respectively, p < 0.001), as well as in the inferior quadrant compared to NHW and Hispanics (−1.22 ± 1.03 µm/year vs. −0.79 ± 0.88 µm/year (NHW) and −0.87 ± 1.10 µm/year (Hispanic); p < 0.001 for both comparisons).
When evaluating eyes with mild glaucoma, the mean adjusted rate of global pRNFL was −0.52 ± 0.66 µm/year (Table 4). A significant difference in the rate of superior pRNFL quadrant change was noted (p = 0.022). NHB eyes demonstrated a significantly faster rate of change compared to NHW eyes in superior quadrant pRNFL (−1.20 ± 1.06 µm/year vs. −0.75 ± 1.51 µm/year, respectively; p = 0.043, Supplementary Fig. 1). In the inferior quadrant, NHB and Hispanic eyes tended to have faster rates compared to NHW eyes (−0.97 ± 1.32 µm/year and −1.04 ± 1.04 µm/year vs. −0.73 ± 0.97 µm/year, respectively), although this trend did not achieve statistical significance (p = 0.066). Global pRNFL rates tended to be faster among Hispanics (−0.59 ± 0.67 µm/year), but this also did not reach statistical significance (p = 0.20).
Among eyes with moderate disease, there was no significant difference in global pRNFL rate (p = 0.60), although NHB eyes tended to have faster rates (Table 5). There was a statistically significant difference in the rate of superior quadrant pRNFL loss (p = 0.006), with NHB eyes having a significantly faster rate compared to Hispanic eyes (−1.31 ± 1.49 µm/year vs. −0.52 ± 1.26 µm/year, p = 0.003; Table 5). No statistically significant differences were noted between racial-ethnic groups among eyes with severe glaucoma (Supplementary Table 3).
Differences in mGCIPL rates
The summary of concurrent changes in mGCIPL parameters classified by racial-ethnic groups are presented in Supplementary Tables 4–7. Among glaucoma suspects, several statistically significant differences were noted between racial-ethnic groups (Supplementary Table 4). NHB eyes presented global mGCIPL rates faster than Hispanics (−0.48 ± 0.31 µm/year vs. −0.40 ± 0.29 µm/year, p = 0.007). In the inferotemporal sector, NHB eyes demonstrated significantly faster rates of change compared to Hispanics and NHW eyes (−0.47 ± 0.31 µm/year, vs. −0.38 ± 0.28 µm/year (Hispanic) and −0.39 ± 0.26 µm/year (NHW), p = 0.010 and p = 0.020 respectively). Statistically significant differences were also noted in the inferior and inferonasal sectors (p = 0.045 and p = 0.007 respectively), although the differences in effect sizes were small.
Among mild glaucomatous eyes, a significant difference was noted in global and inferonasal mGCIPL rates (p = 0.022 and p = 0.012 respectively). Compared to NHW eyes, Hispanic eyes had a faster global rate (−0.53 ± 0.32 µm/year vs. −0.43 ± 0.39 µm/year, p = 0.026; Supplementary Table 5), and inferonasal rate (−0.53 ± 0.33 µm/year vs. −0.41 ± 0.47 µm/year, p = 0.012; Supplementary Table 5). Among eyes with moderate disease (Supplementary Table 6), a significant difference was noted in the superotemporal sector between groups (p = 0.020), with NHB eyes demonstrating a faster rate of loss compared to Hispanics (−0.46 ± 0.24 µm/year vs. −0.34 ± 0.21 µm/year, p = 0.028). No differences were identified in rates of mGCIPL parameters among severe glaucoma eyes (p > 0.05 for all comparisons; Supplementary Table 7).
Relationship between pRNFL and mGCIPL rates
We identified a strong association between global pRNFL and mGCIPL rates of change (R2 = 0.70). When stratified by baseline glaucoma severity (Supplementary Fig. 2), R2 values for relationship between global pRNFL and mGCIPL rates were consistent (glaucoma suspect: R2 = 0.65; mild: R2 = 0.72; moderate: R2 = 0.69; severe: R2 = 0.81). No differences were noted in the strength of the correlation between different racial-ethnic groups (p > 0.05).
Discussion
In this study of a large treated clinical population of subjects with or suspected of glaucoma, we reported significant differences in adjusted rates of change of pRNFL and mGCIPL parameters between various racial-ethnic groups. To our knowledge, this study represents one of the largest analyses of longitudinal SD-OCT data describing both pRNFL and mGCIPL rates among a diverse population of glaucoma patients cared for in routine clinical practice. Of note, Hispanic eyes comprised almost half of the study population, a unique feature in this study. Our study identified faster rates of pRNFL and mGCIPL loss among NHB eyes across most of the spectrum of glaucomatous disease. The lack of any difference in rates among eyes with severe glaucoma may have been due to both smaller sample size and more intense treatment among these subjects. While there was a statistically significant difference in age between groups (Table 1), the estimated rates were adjusted for age as well as other key clinical parameters, such as CCT, IOP, and baseline pRNFL and mGCIPL thickness values. After accounting for these variables, NHB eyes were still noted to have significantly faster rates of pRNFL and mGCIPL loss. Hispanic eyes also tended to have faster rates among certain parameters as well, although most of these comparisons did not reach statistical significance.
Significant differences in mGCIPL rates topographically mirrored areas of significant differences in pRNFL rates in most cases. Among glaucoma suspects, we observed faster thinning in the inferior pRNFL quadrant and inferior/inferotemporal/inferonasal mGCIPL sectors in NHB eyes. Conversely, Hispanics exhibited faster rates in the inferior pRNFL quadrant and inferonasal mGCIPL sector among mild glaucoma eyes, although the former was not statistically significant. Among moderate glaucoma eyes, the superior pRNFL quadrant and supertemporal mGCIPL sector both featured faster rates among NHB eyes. These topographically correlated findings strengthen the likelihood of key differences between racial-ethnic groups.
We observed a strong association between global pRNFL and global mGCIPL rates stratified by glaucoma severity. The correlation coefficient (R2) between pRNFL and mGCIPL was consistent across disease stages, with slightly lower values for earlier disease (Supplementary Fig. 2). The lower correlation coefficient observed among glaucoma suspect eyes could be attributed to early changes occurring in more peripheral regions of the posterior pole, which may not have been captured by the 6x6mm GCIPL cube centred on the fovea. While counterintuitive due to proximity to the RNFL “floor”, the stronger correlation among severe eyes could be explained by our exclusion criteria; we excluded all eyes with a baseline pRNFL thickness <57 µm from the analysis, likely preventing poor correlation due to the “floor effect”. Glaucomatous loss among severe disease is likely to occur closer to the fovea, which is more likely to be captured by the Cirrus GCIPL scan.
Rates of pRNFL loss were generally greater in magnitude than those of mGCIPL, which is likely due to the differences in dynamic range of these tissues. Our finding is similar to previous studies that reported the rate of global pRNFL loss to be significantly faster than global mGCIPL loss [14, 27]. Axons from the inferotemporal, inferior, and inferonasal pGCIPL sectors all enter the optic nerve head primarily in the inferior pRNFL quadrant. Thus, pRNFL loss in this region can be thought of a composite “sum” of the respective mGCIPL losses, likely leading to a faster rate of loss when compared to just one mGCIPL sector. In addition, the Cirrus mGCIPL scan provides data only from a foveal cube, possibly missing macular damage outside of this area. However, those damaged axonal fibres would still be detected on the pRNFL scan. Prior studies have reported similar patterns of sectoral pRNFL and mGCIPL loss but in smaller cohorts of patients [13, 23, 27].
After adjusting for age, sex, CCT, IOP, and baseline thickness, we were impressed that NHB eyes still had significantly faster rates of pRNFL and mGCIPL loss. Numerous studies have demonstrated more progressive glaucomatous disease among Black patients [6, 16, 28, 29]. The Baltimore Eye Survey demonstrated that glaucoma prevalence among individuals of African descent is six times higher than that of the European American population, with a six-fold higher likelihood of glaucoma-related blindness [16]. The younger age of NHB subjects in our study (p < 0.001; Table 1) was also consistent with the findings of the Baltimore Eye Survey, which suggested that glaucoma tends to be diagnosed significantly earlier in the Black population. In a prospective cohort study spanning approximately 3 years and including a total of 528 healthy, glaucoma suspect, and glaucomatous eyes, Bowd et al. reported race-related differences in the rate of change of Bruch Membrane Opening-Minimum Rim Width, but only within the glaucoma suspect group [30]. No significant variation in the rate of change of pRNFL was observed. Notably, the authors did not stratify eyes with overt glaucoma according to the severity of the condition. Additionally, the study only analysed two groups (i.e., European descent and African descent), with a notable difference in the number of eyes included compared to our report. Recently, the investigators of the Primary Open-Angle African American Glaucoma Genetics (POAAGG) study described a median rate of pRNFL loss of −1.60 µm/year among Black subjects, nearly three times higher than a previously reported normal age-related rate of change of −0.52 µm/year [31]. These results are in contrast to the slower rates of pRNFL loss noted in the Duke Glaucoma Registry (−0.76 μm/year) and in the Diagnostic Innovations in Glaucoma Study (−0.98 μm/year), both which were predominantly comprised of White subjects (67.8% and 67%, respectively) [8, 14]. It is important to note that the POAAGG study had a non-comparative design, focusing solely on African American, African descent, or African Caribbean patients. Direct comparisons with other racial and ethnic groups were not made in the study, and the authors did not analyse mGCIPL data, sectoral pRNFL data, or stratify rates based on glaucomatous severity [31]. With respect to rates of OCT parameters among Hispanic patients, we believe that our study represents the first report documenting pRNFL and mGCIPL rates in a large clinical cohort.
Aetiologies for the faster rates of loss among NHB subjects could be related to different factors. A major strength of studying a clinically treated population is analysing the potential impact of non-clinical parameters on testing results, such as poor medication adherence, which are often non-issues in prospective studies due to exclusion criteria. Socioeconomic disparities and differences in access to healthcare have been described to contribute to differences in glaucoma outcomes among racial and ethnic groups [26, 32]. Black patients are more likely to face barriers to care such as lack of insurance, transportation difficulties, limited access to medications, as well as lower adherence to follow-up and treatment regimens, which can negatively impact health outcomes [26, 32, 33]. These disparities, coupled with worse baseline disease at diagnosis and at a younger age, could contribute to faster rates of pRNFL and mGCIPL loss, especially in earlier disease as observed in this study [26, 32]. In contrast, treatment adherence or surgical intervention might be greater in severe glaucoma given the perceptible impact on vision, leading to a non-significant difference in rates (Supplementary Table 3). Addressing these socioeconomic challenges may potentially ameliorate the disparities observed in this study, although further analyses are required as we were unable to distinguish between potential social influences. In addition, genetic differences could predispose NHB eyes to rapid disease progression; for example, the POAAGG study identified potential genetic factors that could contribute to worse disease among Black patients, specifically the TC genotype in a single nuclear polymorphism near the TRIM66 gene [31, 34]. In our study, CCT was significantly lower among NHB eyes (Table 2), potentially suggesting a difference in sclera and lamina cribrosa biomechanics, which may dictate how elevated IOP or IOP fluctuations impact pRNFL and mGCIPL loss. These findings highlight the complex interplay of genetic, ocular, and socioenvironmental factors that may influence the progression of glaucoma and contribute to the observed disparities between racial-ethnic groups [35].
Strengths of this analysis include the study cohort, which consists of a large, clinically treated population with considerable follow-up. Of note, our study population was unique given the substantial representation of Hispanic subjects, accounting for nearly 50%. In addition, the statistical modelling approach of longitudinal joint mixed modelling in this study minimises the degree of measurement error by allowing two associated outcomes to be modelled together. This study was also unique in its modelling of topographically related sections of pRNFL quadrants and mGCIPL sectors. Furthermore, excluding tests conducted after any surgical procedure carried out during the follow-up period enabled a more conservative analysis of the rate of pRNFL or mGCIPL loss, reducing the influence of iatrogenic factors.
Use of EHR data has its inherent limitations, including incorrect ICD or CPT coding. The diagnosis of glaucoma or glaucoma suspect was made based on the clinician’s judgement. In addition, any glaucoma surgeries that occurred outside of BPEI would not have been accounted for when excluding post-intervention tests. Furthermore, certain trends were observed in the data as previously noted, but these differences did not reach statistical significance in our current sample. These trends may represent true differences that would reach statistical significance with a larger sample size. Finally, our clinical population did not have sufficiently large cohorts of other racial-ethnic groups (e.g., Asian or Native American), limiting our conclusions regarding these individuals.
In summary, our analysis of a treated clinical glaucomatous population highlights significant differences in pRNFL and mGCIPL rates across different racial-ethnic groups after stratifying by disease severity. Rates of mGCIPL loss mirrored those of pRNFL, with non-Hispanic Black eyes having faster rates of pRNFL and mGCIPL loss among glaucoma suspect, mild glaucoma, and moderate glaucoma eyes. These findings reflect the importance of considering various aetiologies, such as socioeconomic disparities, that may contribute to these differences in rates of OCT loss among glaucoma patients.
Supplemental material is available at Eye’s website.
Summary
What was known before
-
Differences in rates of change in OCT parameters between diverse racial-ethnic groups have not been investigated using a large population receiving routine care.
What this study adds
-
In this retrospective cohort study including 2002 eyes, non-Hispanic Black eyes featured the highest rates of peripapillary Retinal Nerve Fibre Layer (pRNFL) loss among glaucoma suspect, mild, and moderate glaucoma eyes in a treated clinical population. Global pRNFL and macular Ganglion Cell Inner Plexiform Layer rates were strongly correlated. Racial-ethnic differences must be considered in the management of glaucoma patients, given the potential for a more rapid rate of disease progression within certain groups.
Data availability
The data that support the findings of this study are available from the authors upon reasonable request.
References
Weinreb RN, Aung T, Medeiros FA. The pathophysiology and treatment of glaucoma: a review. JAMA. 2014;311:1901–11.
Gallo Afflitto G, Chou TH, Swaminathan SS, Aiello F, Gedde SJ, Nucci C, et al. Pattern electroretinogram in ocular hypertension, glaucoma suspect and early manifest glaucoma eyes: a systematic review and meta-analysis. Ophthalmol Sci. 2023;3:100322.
Gallo Afflitto G, Aiello F, Cesareo M, Nucci C. Primary open angle glaucoma prevalence in Europe: a systematic review and meta-analysis. J Glaucoma. 2022;31:783–8.
Bradley C, Herbert P, Hou K, Unberath M, Ramulu P, Yohannan J. Comparing the accuracy of peripapillary OCT scans and visual fields to detect glaucoma worsening. Ophthalmology. 2023;130:631–9.
Tatham AJ, Medeiros FA. Detecting structural progression in glaucoma with optical coherence tomography. Ophthalmology. 2017;124:S57–S65.
Gordon MO, Beiser JA, Brandt JD, Heuer DK, Higginbotham EJ, Johnson CA, et al. The ocular hypertension treatment study: baseline factors that predict the onset of primary open-angle glaucoma. Arch Ophthalmol. 2002;120:714–20. discussion 829-30
Swaminathan SS, Jammal AA, Kornmann HL, Chen PP, Feuer WJ, Medeiros FA, et al. Visual field outcomes in the tube versus trabeculectomy study. Ophthalmology. 2020;127:1162–9.
Swaminathan SS, Jammal AA, Berchuck SI, Medeiros FA. Rapid initial OCT RNFL thinning is predictive of faster visual field loss during extended follow-up in glaucoma. Am J Ophthalmol. 2021;229:100–7.
Mohammadzadeh V, Su E, Rabiolo A, Shi L, Zadeh SH, Law SK, et al. Ganglion cell complex: the optimal measure for detection of structural progression in the macula. Am J Ophthalmol. 2022;237:71–82.
Mahmoudinezhad G, Mohammadzadeh V, Martinyan J, Edalati K, Zhou B, Yalzadeh D, et al. Comparison of ganglion cell layer and ganglion cell/inner plexiform layer measures for detection of early glaucoma. Ophthalmol Glaucoma. 2023;6:58–67.
Shin JW, Sung KR, Lee GC, Durbin MK, Cheng D. Ganglion cell-inner plexiform layer change detected by optical coherence tomography indicates progression in advanced glaucoma. Ophthalmology. 2017;124:1466–74.
Lavinsky F, Wu M, Schuman JS, Lucy KA, Liu M, Song Y, et al. Can macula and optic nerve head parameters detect glaucoma progression in eyes with advanced circumpapillary retinal nerve fiber layer damage? Ophthalmology. 2018;125:1907–12.
Lee WJ, Baek SU, Kim YK, Park KH, Jeoung JW. Rates of ganglion cell-inner plexiform layer thinning in normal, open-angle glaucoma and pseudoexfoliation glaucoma eyes: a trend-based analysis. Invest Ophthalmol Vis Sci. 2019;60:599–604.
Hammel N, Belghith A, Weinreb RN, Medeiros FA, Mendoza N, Zangwill LM. Comparing the rates of retinal nerve fiber layer and ganglion cell-inner plexiform layer loss in healthy eyes and in glaucoma eyes. Am J Ophthalmol. 2017;178:38–50.
Berkowitz ST, Groth SL, Gangaputra S, Patel S. Racial/ethnic disparities in ophthalmology clinical trials resulting in US food and drug administration drug approvals from 2000 to 2020. JAMA Ophthalmol. 2021;139:629–37.
Tielsch JM, Sommer A, Katz J, Royall RM, Quigley HA, Javitt J. Racial variations in the prevalence of primary open-angle glaucoma. The Baltimore eye survey. JAMA. 1991;266:369–74.
Jammal AA, Thompson AC, Mariottoni EB, Urata CN, Estrela T, Berchuck SI, et al. Rates of glaucomatous structural and functional change from a large clinical population: the Duke glaucoma registry study. Am J Ophthalmol. 2021;222:238–47.
Mwanza JC, Durbin MK, Budenz DL, Girkin CA, Leung CK, Liebmann JM, et al. Profile and predictors of normal ganglion cell-inner plexiform layer thickness measured with frequency-domain optical coherence tomography. Invest Ophthalmol Vis Sci. 2011;52:7872–9.
Xu X, Xiao H, Guo X, Chen X, Hao L, Luo J, et al. Diagnostic ability of macular ganglion cell-inner plexiform layer thickness in glaucoma suspects. Medicine. 2017;96:e9182.
Mwanza JC, Kim HY, Budenz DL, Warren JL, Margolis M, Lawrence SD, et al. Residual and dynamic range of retinal nerve fiber layer thickness in glaucoma: comparison of three OCT platforms. Invest Ophthalmol Vis Sci. 2015;56:6344–51.
Swaminathan SS, Berchuck SI, Jammal AA, Rao JS, Medeiros FA. Rates of glaucoma progression derived from linear mixed models using varied random effect distributions. Transl Vis Sci Technol. 2022;11:16.
Alencar LM, Zangwill LM, Weinreb RN, Bowd C, Sample PA, Girkin CA, et al. A comparison of rates of change in neuroretinal rim area and retinal nerve fiber layer thickness in progressive glaucoma. Invest Ophthalmol Vis Sci. 2010;51:3531–9.
Miki A, Medeiros FA, Weinreb RN, Jain S, He F, Sharpsten L, et al. Rates of retinal nerve fiber layer thinning in glaucoma suspect eyes. Ophthalmology. 2014;121:1350–8.
Medeiros FA, Zangwill LM, Alencar LM, Sample PA, Weinreb RN. Rates of progressive retinal nerve fiber layer loss in glaucoma measured by scanning laser polarimetry. Am J Ophthalmol. 2010;149:908–15.
Crowther MJ, Lambert PC, Abrams KR. Adjusting for measurement error in baseline prognostic biomarkers included in a time-to-event analysis: a joint modelling approach. BMC Med Res Methodol. 2013;13:146.
Delavar A, Radha Saseendrakumar B, Weinreb RN, Baxter SL. Racial and ethnic disparities in cost-related barriers to medication adherence among patients with glaucoma enrolled in the national institutes of health All of Us research program. JAMA Ophthalmol. 2022;140:354–61.
Nguyen AT, Greenfield DS, Bhakta AS, Lee J, Feuer WJ. Detecting glaucoma progression using guided progression analysis with oct and visual field assessment in eyes classified by International Classification of Disease severity codes. Ophthalmol Glaucoma. 2019;2:36–46.
Leske MC, Wu SY, Hyman L, Nemesure B, Hennis A, Schachat AP, et al. Four-year incidence of visual impairment: Barbados incidence study of eye diseases. Ophthalmology. 2004;111:118–24.
Podgor MJ, Leske MC, Ederer F. Incidence estimates for lens changes, macular changes, open-angle glaucoma and diabetic retinopathy. Am J Epidemiol. 1983;118:206–12.
Bowd C, Zangwill LM, Weinreb RN, Girkin CA, Fazio MA, Liebmann JM, et al. Racial differences in rate of change of spectral-domain optical coherence tomography-measured minimum rim width and retinal nerve fiber layer thickness. Am J Ophthalmol. 2018;196:154–64.
Salowe RJ, Chen Y, Zenebe-Gete S, Lee R, Gudiseva HV, Di Rosa I, et al. Risk factors for structural and functional progression of primary open-angle glaucoma in an African ancestry cohort. BMJ Open Ophthalmol. 2023;8:e001120.
Dreer LE, Girkin C, Mansberger SL. Determinants of medication adherence to topical glaucoma therapy. J Glaucoma. 2012;21:234–40.
Murakami Y, Lee BW, Duncan M, Kao A, Huang JY, Singh K, et al. Racial and ethnic disparities in adherence to glaucoma follow-up visits in a county hospital population. Arch Ophthalmol. 2011;129:872–8.
Kim CD, Gudiseva HV, McGeehan B, Daniel E, Ying GS, Chavali VRM, et al. Association of the SNP rs112369934 near TRIM66 gene with POAG endophenotypes in African Americans. Genes. 2021;12:1420.
Melchior B, Valenzuela IA, De Moraes CG, Paula JS, Fazio MA, Girkin CA, et al. Glaucomatous Visual Field Progression in the African Descent and Glaucoma Evaluation Study (ADAGES): eleven years of follow-up. Am J Ophthalmol. 2022;239:122–9.
Funding
Supported in part by National Institutes of Health/National Eye Institute grant K23 EY033831 (SSS), and American Glaucoma Society Mentoring for the Advancement of Physician Scientists grant (SSS). The funding organisation had no role in the design or conduct of this research.
Author information
Authors and Affiliations
Contributions
G.G.A. was responsible for conducting the preliminary search screening of the literature, writing the final report, creating and updating reference lists, and contributed to the design of the study protocol. SSS was responsible for designing the study protocol, extracting and analysing data, creating figures and tables, and provided feedback on the report.
Corresponding author
Ethics declarations
Competing interests
G.G.A.: none. S.S.S.: Sight Sciences (C), Ivantis (C), Heidelberg Engineering (S), Lumata Health (C, E), Abbvie (C); Topcon (C); National Institutes of Health/National Eye Institute (S).
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Gallo Afflitto, G., Swaminathan, S.S. Racial-ethnic disparities in concurrent rates of peripapillary & macular OCT parameters among a large glaucomatous clinical population. Eye (2024). https://doi.org/10.1038/s41433-024-03103-3
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41433-024-03103-3
