
Abstract
This review article systematically reviews the use of Patient Reported Outcome Measures (PROMs) in Vitreoretinal surgery, with the aim of recommending a preferred PROM-tool for use in clinical practice. Vitreoretinal surgery lags behind other ophthalmic subspecialties in the adoption of PROMs as a core outcome measure of success post-operatively. Current outcomes rely heavily on post-operative Best Corrected Visual Acuity (BCVA) and anatomical success on imaging modalities such as Ocular Coherence Tomography (OCT), despite the link between each of these measures and patient satisfaction being uncertain. We systematically reviewed the available literature in March 2021, in accordance with PRISMA guidelines, searching six databases: MEDLINE, EMBASE, Web of Science, APA PsycINFO, SCOPUS and Cochrane Library. Critical appraisal of PROM-tools was facilitated using the COnsensus-based Standards for the selection of health Measurement INstruments (COSMIN) risk of bias checklist. We identified 14 eligible original research papers that used PROMs as a primary or secondary outcome of success post-operatively in patients having undergone vitreoretinal surgery. Eight different generic and vision-related PROM-tools were identified as being used in vitreoretinal studies, none of which were vitreoretinal-disease-specific. Our review article considers whether generic-health PROMs (e.g., EQ5D) or vision-related PROMs (e.g. NEI VFQ-25) are precise or responsive enough following vitreoretinal surgery to have a meaningful impact on clinical or research practice. We also consider the importance of standardisation of clinical outcomes in vitreoretinal clinical trials.
摘要
本文系统回顾了由患者报告的结局量表 (PROMs) 在玻璃体视网膜手术中的应用, 旨在为临床实践推荐首选的PROM量表。在采用PROMs作为评价手术成功的核心结局指标这方面, 玻璃体视网膜手术落后于其他眼科亚专业的手术。目前, 玻璃体视网膜手术的预后评价主要依赖于术后最佳矫正视力 (BCVA) 和成像方面的解剖成功率 (相干光断层扫描技术), 尽管这些指标与患者满意度之间的关联尚不清楚。我们根据PRISMA指南, 对2021年3月现有的文献进行了系统综述, 共检索了6个数据库: MEDLINE、EMBASE、Web of Science、APA PsycINFO、SCOPUS和Cochrane Library。我们基于COnsensus标准, 选择健康测量量表 (COSMIN) 偏倚风险检查表对PROM量表进行了严格评估。我们筛选了14篇符合条件的原始研究, 这些研究将PROMs作为玻璃体视网膜手术成功的主要或次要结局评价指标。8种不同的通用的以及和视觉相关的PROM量表被确定用于玻璃体视网膜研究, 但都不具有玻璃体视网膜疾病的特异性。本文探究了玻璃体视网膜术后, 全身健康相关的PROMs (如EQ5D) 或视觉相关的PROMs (如NEI VFQ-25) 是否能做到精确评估或足够灵敏, 从而对临床试验或研究转化产生有意义的影响。我们还讨论了玻璃体视网膜临床试验中临床结果标准化的重要性。
Similar content being viewed by others
Introduction
Patient reported outcome measures (PROMs) are a key part of how healthcare is funded, provided, and managed. It represents a paradigm-shift in placing the patient at the centre of their care, as patients are best placed to judge how effective their treatment is for them [1]. PROM-tools are a series of standardised and validated questions to gain patient’s perspective of their own health. The purpose of PROMs is to obtain patients’ own assessment of their health and health-related quality of life (HR-QOL). The responses can be gathered by clinicians to influence decision-making in healthcare [2].
PROM development is difficult; the questions chosen must discriminate between clinically distinct groups, be responsive enough to detect clinically important changes over time, demonstrate test-retest validity; all whilst being short enough to administer in a busy clinical environment [3]. The three main psychometric concepts used for item development in PROMs include classic test theory (CTT) [4], item response theory (IRT) [5]; and Rasch measurement theory (RMT) [6]. In essence, QOL instruments are assessed for validity (the concept to be measured is assessed by the instrument), reliability (any significant results obtained are repeatable) and responsiveness (captures clinically useful changes over a period of time). Robust psychometric testing of a questionnaire is always required in the target population and in a new cultural setting [7, 8].
PROMs can be generic or disease-specific. Generic PROMs measure general health so that changes in health can be compared across different patients, conditions and population groups. These generic instruments measure health in terms of the ability to function or enjoy life. The most common of these include the EuroQol Five Dimensions questionnaire (EQ-5D) [9] or Short-Form 36 (SF-36) [10]. These generic PROMs can yield a health utility score, often on a scale of 0–1, whereby one represents perfect health and 0 is equivalent to death. Scores can be used to calculate Quality Adjusted Life Years (QALYs) [1].
Generic PROMs are useful in comparisons across diseases and populations, while disease-specific PROMs are usually more sensitive to clinically meaningful changes in disease-related characteristics. Both generic and disease-specific PROMs are recommended to be used in conjunction [11]. No single instrument is the ‘gold standard’ for measuring patient status, each measure different dimensions of health, use different levels of scoring and reference different time periods [12]. In Ophthalmology, various PROM-tools have been used to measure HR-QOL as well as Vision-Related Quality of Life (VR-QOL) [13].
Vitreoretinal surgery, as defined by BEAVRS, [14] (British & Eire Association of Vitreoretinal Surgeons) is the subspecialty of ophthalmic surgery treating diseases of the vitreous and retina. Vitreoretinal surgery can be extremely effective at restoring vision, but clinical outcomes can be unpredictable and the surgery itself is not without risks and side effects. Important decisions need to be made by patients and their clinicians when deciding on treatments. The correct decision for one patient may be radically different from another highlighting the importance of patient-centred care.
Current practices which guide surgical treatments rely on objective measurements of visual acuity and anatomical features, for example, on Ocular Coherence Tomography (OCT). It is widely recognised that these outcomes do not always correlate well with patient satisfaction [3, 15, 16]. PROMs in everyday practice have the ability to narrow the gap between the clinician’s and patient’s view and help tailor treatment plans to meet the patient’s preferences and needs’ [17]. PROMs also have an important and growing role in clinical trials and research; a number of health agencies, such as the National Institute for Health and Care Excellence advocate the use of PROMs to demonstrate the cost-effectiveness of new drugs or treatments [1].
This review article aims to identify and critically evaluate PROMs used in Vitreoretinal surgery. The authors consider the implementation of any identified PROM-tools and to outline any difficulties with their use.
Methods
A systematic review of the literature was performed on multiple databases; MEDLINE, EMBASE, Web of Science, APA PsycINFO, SCOPUS and Cochrane Library, without restrictions on publication date but limited to the English language only (as resources to ensure robust translation to address cross-culturally validity issues were not available). A snowballing citation search was subsequently performed and supplemented by a search of the grey literature. The initial search was carried out in February 2021 and then updated in March 2021. The search was completed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) guidelines, and followed a thorough search, with relevant MeSH terms, on all six databases (see Supplementary Information).
Deduplicated citations were exported to Covidence (Covidence systematic review software, Veritas Health Innovation, Melbourne, Australia), where title and abstract screening was completed by two researchers, (AY and AD). Any conflicts were discussed with a third reviewer (TS) to reach a consensus. The full-text articles were imported to Covidence for full-text screening. The researchers employed the strict inclusion and exclusion criteria as summarised in Table 1. Published conference abstracts were excluded in this systematic review.
Abstracts were reviewed independently by two researchers (AY, AD) to determine the eligibility based on the inclusion and exclusion criteria outlined in Table 1. Any conflicts were discussed individually to reach a consensus, with intervention of a third reviewer (TS) if still not resolved. The full papers were then obtained and imported onto Covidence for full-text screening and data extraction. Full text articles that did not meet the inclusion criteria were excluded (see Supplementary Information). The researchers used an agreed data extraction template, focussing on instrument description and measurement properties (Table 2). Data was extracted on details regarding study type, population size and PROM-specific details (PROM instruments used, concepts, scoring, response, mode and timepoints PROMs administered, etc.). Different versions of the same instrument reported in different publications were counted as one (i.e., language adapted). If major modifications were made, they were classed as a different instrument.
Two reviewers (AY, AD) completed the quality assessment, and the results are summarised in Table 3. The COnsensus-based Standards for the selection of health Measurement INstruments (COSMIN) Risk of Bias checklist [18,19,20] was used to assess the individual measurement properties and then consequently the overall methodological quality. This tool was designed to critically appraise studies evaluating the use of PROMs and their assessment in a systematic review, and therefore used in this review. Items on the checklist included ten domains; PROM development, content validity, structural validity, internal consistency, cross-cultural validity, reliability, measurement error, criterion validity, hypothesis testing for construct validity and responsiveness (see Supplementary Information for further explanation of domains). The checklist rates items based on a 4-point scale; “very good”, “adequate”, “doubtful” or “inadequate”. The overall quality of a study was determined by the mean score attributing 4 points for “very good”, 3 for “adequate”, 2 for “doubtful” and 1 for “inadequate”. Some fields were not applicable to the PROM-tool in question and are recorded in grey shading in Table 3.
Results
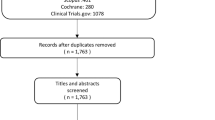
The combined database and grey literature search and yielded a total of 1313 citations, with 358 duplications removed. Exact numbers of each screening stage can be found in Fig. 1. Two reviewers (AY, AD) independently screened 955 article abstracts against the clearly defined eligibility criteria (Table 1). Where abstracts alone were insufficient to determine eligibility, full texts were obtained resulting in 34 full-text articles. 60% (n = 12) of the full text research articles were excluded since the intervention described in the studies included combined VR surgery, most commonly cataract surgery with VR surgery. Full texts articles excluded, with reason are included in Appendix 1. A total of 14 studies were included for qualitative synthesis and reviewed for data extraction and quality assessment, presented in Table 2 and Table 3, respectively.

PRISMA Diagram; Flowchart of Study Identification and Selection. (PROMs: Patient Reported Outcome Measures).
Of the 14 eligible studies included in out review, eight different PROM-tools were identified as being used to evaluate HR-QOL or VR-QOL in patients after vitreoretinal surgery. No VR-specific PROM-tools were found. The majority of studies focused on RD (n = 8), with fewer studies in ERM (n = 3), MH (n = 2) and vitrectomy for diabetic retinopathy (n = 1). More than one different PROM tools were used in 21% (n = 3) of the studies. Vision-specific instruments were the most commonly used measure, with the National Eye Institute Visual Function Questionanire-25 (NEI VFQ-25) identified as the most widely used tool (n = 8). One study reports the use of the NEI VFQ-13 [21], a modified version of the NEI VFQ-25. The Chinese Version Low-Vision Quality of Life Questionnaire (CVLQOL) was another VR-QOL measure (n = 1).
Generic PROM-tools measuring HR-QOL included the SF-36 (n = 3), Hospital Anxiety and Depression Scale (HADS) (n = 2), EQ-5D (n = 1), Diabetic-Specific Quality of Life Scale (DSQL) (n = 1), and Subjective QoL Assessment Questionnaire (n = 1).
PROM instruments that had be translated for use in their respective populations (n = 7), reported reliably translated and validated versions of the instrument. Table 2 summarises the characteristics of the instruments identified in this systematic review.
Vision-related instruments
The NEI VFQ-25 was the most commonly used PROM of all the studies. Developed from a multi-condition focus group process in the USA, it has been adopted internationally and translated to various languages including, French, German, Italian, Spanish, Chinese, Greek and Portuguese [22]. This review identified its use translated from its original language into four different languages: Dutch, German, Japanese and Chinese. The NEI VFQ-25 has also been validated to measure QOL across many ocular diseases [23], such as age-related macular degeneration [24], glaucoma [25] and cataract [26]. This review found the NEI-VFQ-25 was used for studies in RD (n = 4), MH (n = 2), and ERM (n = 2).
A short version NEI VFQ-13 was used by Potic et al. to measure VR-QOL in patients requiring surgery for RD in a prospective cohort study [21]. The study validated it’s modified PROM using Rasch analysis [27]. The shortened version included seven items of the short version of the visual function scale (SVFVS) and six items of the short version of the socioeconomic scale (SVSES), with same scales used as the original NEI VFQ-25.
The Chinese Version Low-Vision Quality of Life questionnaire (CVLQOL) developed by Zou et al. assessed the multidimensional VR-QOL of patients with retinal detachment [28]. This included 25 closed-ended visual functioning items classified into four subscales, graded on an ordinal scale from five (no problems due to vision) to one (great difficulties due to vision). The four subscales included: (1) general vision and lighting, (2) mobility, (3) psychological adjustment and (4) reading, fine work and activities of daily living.
Generic instruments
Our review identified three studies which implemented the SF-36 PROM-tool in vitreoretinal disease. The SF-36 contains 11 items in six domains, including general health and symptoms, role limitations, social functioning, vitality, and mental health. Two studies used the Hospital Anxiety and Depression Scale (HADS), which covers emotional well-being. We found one study which used the EQ-5D, which includes five questions on mobility, self-care, usual activities, anxiety/depression, and pain/discomfort. The scores for each question can be translated to an overall utility state, based on published value sets validated for each country [29]. It has been widely used as a HR-QOL measure since its inception almost three decades ago by the EuroQol Group.
The Diabetic-Specific Quality of Life Scale (DSQL) has been identified as an appropriate diabetic-specific tool, measuring the physical, psychological, and social impacts of diabetic disease on an individual’s health. Although validated in a type-1 diabetic-specific population in Germany [30], Yu et al. [31] found the DSQL to correlate with improved summary SF-36 scores after surgical intervention for diabetic retinopathy but acknowledge its’ sensitivity to symptomatic changes in diabetic retinopathy is yet be verified.
Koriyama et al. [32] developed their own subjective assessment questionnaire which they implemented in their cohort of patients undergoing scleral buckling for retinal detachment. Quality of Life assessment was a secondary outcome in this study. The authors of this review could not find prior published work attesting to its development or validation and consequently found their questionnaire had inadequate methodological quality according to the COSMIN Risk of Bias criteria checklist used in this review.
All of the generic instruments identified were not developed for ocular disease and thus not validated for the common indications of VR surgery but have been validated against classical test theory.
Mode and timepoints of administration
Across all studies, questionnaires were either self-completed on paper (n = 7) or the questions were interview-administered (n = 2). Yu et al. [31] performed a mixed mode of either questionnaires sent by post, or interviews conducted over the phone depending on patient preference. Four studies did not report mode of administration.
Timepoints of questionnaires varied across all studies, most commonly completed at baseline/preoperatively and at least once post-operatively. Four studies did not complete a pre-operative/baseline assessment of quality of life, all of which were for RD surgery. All authors cited this was due to the rapid-onset nature and urgent need for treatment.
Zou et al. [28] had the longest duration to follow up (three years) measured once pre-operatively and repeated three times post-operatively, at three months, one year, and three years after retinal detachment surgery. One study asked patients to complete the questionnaire two years post-operatively and five studies 1-year post-operatively.
Across all studies, PROM instruments were administered at a maximum of three different timepoints post-intervention; once (n = 8), twice (n = 3) and three times (n = 3). The most measured timepoint was three months post-operatively (n = 8) followed by at both 6 and 12 months (n = 6).
Risk of bias across studies
The COSMIN Risk of Bias checklist [18] was developed through an international Delphi study consensus to facilitate critical appraisal of patient-reported outcome measure-tools (PROM-tools) and enable the selection of high-quality instruments for a specific purpose. The validated and standardised nature of this tool explains its increasing use in systematic reviews of PROMs [33].
Based on the COSMIN criteria and 4-point rating scale (outlined in Table 3), no studies were deemed of overall “very good” methodology according to their individual domains. The reliability of only two studies were deemed adequate [28, 34], and the measurement error was ‘very good’ in two studies [35, 36]. Content validity could only be rated in five of the 14 studies, as most failed to comment on patients’ perspective of the comprehensibility and relevance of the instrument. However, even these studies failed to assess content validity. Generally, as most studies did not report the patient burden of PROMs to their patient populations, this systematic review found little evidence on the acceptability of PROMs for vitreoretinal patients undergoing surgery.
The measurement of structural validity of studies included queries regarding the developmental model of the instrument (Rasch, CTT, IRT), appropriateness of the model to the research question, and if the sample size was adequate. Assessment could not be made for structural validity in 57% (n = 8) of the studies, either because it was not reported, or most commonly due to the small sample size. Almost all studies recognised their small statistical power as a limitation to ascertain significant differences.
The quality of PROM development was adequate in only one study (Potic et al., 2021) [21], as the authors describe the use and validation of their modified version of the NEI VFQ-25.
This was the only study of the identified articles that used a modified version of an existing PROM tool; therefore this was the only study which considered validation of their PROM tool (NEI VFQ-13) in their article.
Discussion
This review aimed to identify PROMs assessing QOL in VR surgery, evaluate how they are administered and recommend, if possible, suitable PROM-tools for routine clinical use in patients undergoing VR surgery.
Context and characteristics of PROMs
Across 14 eligible studies, eight PROMs were identified: three vision-related, five generic items, but no PROMs were VR-specific. The most common instrument to quantitatively assess VR-QOL was the NEI-VFQ-25.
Although, generic PROM-tools have a number of advantages, they may lack sensitivity in ocular disease [37]. Measuring vision-related QOL (VR-QOL) provides a greater indication on the effect of the ocular disease or treatment on a patient’s overall quality of life. This review found that vision-related PROMs are more responsive to changes in health and better correlate with other clinical parameters, compared with generic PROMs. Okamoto et al. [35] showed a significant correlation of post-operative NEI VFQ-25 scores with the severity of metamorphopsia and best corrected visual acuity (BCVA) for epiretinal membranes. Similarly, Ng et al. [38] shows NEI VFQ-25 scores positively correlating with metamorphopsia, BCVA, colour vision and stereopsis in patients with RD surgery. A positive correlation was also seen with the NEI VFQ-13 scores and BCVA by Potic et al. [21]. Contrastingly, a negative correlation between NEI VFQ-25 scores with metamorphopsia was found by Lina et al. [39] in patients who underwent RD surgery.
Though most of the generic PROMs showed a continually improved score of quality in life of patients after surgery at different timepoints, they either did not measure or prove statistical correlation with vision-specific clinical parameters. Generic PROMs have the advantages of allowing comparison across populations, and for the calculation of QALYs, but lack sensitivity versus disease-specific questionnaires. BCVA is accepted as a major determinant of VR-QOL and ophthalmologists use it as one of the most essential clinical parameters to evaluate success of vitreoretinal surgery [40, 41]. The studies in this review most commonly measured vision as clinical indication of progress after intervention, however BCVA alone is insufficient to explaining many aspects of visual function [42]. Though not considered specifically in this review, a number of previous works have proposed that it is best corrected visual acuity (BCVA) in either the better-seeing eye(BSE), or indeed worse-seeing eye(WSE), that more closely correlates with QOL [43].
It is also important to note that ocular dominance was not assessed in any of the studies which is important as it can be a major determinant of VR-QOL in uniocular diseases [44]. Many VR conditions present uniocularly, and symptoms can vary based on dominance with compensation of visual function by the fellow eye [45].
Vitreoretinal surgery itself is complex and where interventions such as epiretinal membrane peel, macular hole surgery or repair of retinal detachments can significantly improve visual acuity, other vision-related symptoms may be equally, if not more, important to the patient. Ng et al. [38] described visual acuity itself as being inadequate as an indicator of quality of life, but considered the importance of also considering metamorphopsia, aniseikonia and colour vision in patients who had undergone retinal detachment repair. Furthermore, in a prospective cohort study, van de Put et al. [46] found that whilst the incidence of metamorphopsia is high in patients after retinal detachment surgery, the degree of metamorphopsia was often mild and may not interfere with patient-reported QOL metrics to a significant degree. Hence simply considering the presence or absence of metamorphopsia may be too simplistic in the ideal PROM-tool for vitreoretinal surgery.
Furthermore, a recent large prospective patient-cohort study reported that the use of a metamorphopsia-specific patient questionnaire, as compared to a generic symptom-based assessment completed by the clinician, yielded more frequent reports of metamorphopsia in vitreoretinal macular traction [47]. It also concluded that the severity of metamorphopsia acts as a predictor of VR-QOL. It could be postulated that inclusion of questions specifically enquiring about symptoms of metamorphopsia in a VR-specific PROM, which is absent in current PROM tools, is important in predicting VR-QOL after VR surgery. It is therefore likely that there are several specific VR-related clinical symptoms that bear an impact on patient’s QOL after VR surgery [48,49,50,51], suggesting the need for a VR-specific PROM-tool.
This systematic review reiterates the lack of research around PROMs in VR surgery; no VR-specific PROM-tools were identified. The majority of PROM studies were in RD surgery (n = 8) and fewer studies in ERM (n = 2), MH (n = 2) and post-vitrectomy for diabetic retinopathy (n = 1). The authors felt the more insidious vitreoretinal pathologies, such as ERM and MH, for which surgery is likely elective were severely under-represented in the literature on PROMs. This is surprising as it is in these conditions where the decision to proceed with surgery is less clear cut versus surgical emergencies such as retinal detachment. Patient-reported outcome measures are arguably more important in these conditions, where a detailed consideration of patient’s disease burden, psychosocial and functional impacts and expectations from surgery must be considered.
In terms of constructs across all PROMs, the most measured was general HR-QOL and the most common domain assessed was emotional well-being. The most common instrument to quantitatively assess the VR-QOL was the NEI-VFQ-25. Although, based on Rasch analysis, Pesudovs et al. [27] reported several fundamental issues with this questionnaire. To remediate the problems discovered, the authors created a short form NEI VFQ-13 with two short forms; SFVFS and SFSES which Potic et al. [21] have deemed the most suitable for RD, after producing the most statistically robust results using this instrument. However, an even shorter version is available, NEI VFQ-11, developed using IRT. This was created and validated in Japan, with the researchers describing a decrease in burden on patients due to the short nature of the instrument [52].
Method and timepoints of administration
Patient acceptance and adherence is an important consideration of the ideal PROM-tool, not least in a population who are likely to suffer visual impairment. The mode of administration is a key determinant of patient adherence and completion rate. The studies in the review used paper-based methods most frequently, however, electronic or online administration is reported to increase patient adherence [53]. This also avoids manual data entry which could be less time-consuming for clinicians and more cost effective in the long term.
Seven of the 14 identified studies had questionnaires which were self-administered by patients and therefore susceptible to common method bias, a limitation recognised in all of these studies. Common method bias describes a variation, even upwardly biased in some cases, in responses caused by the instrument rather than the actual predispositions of the respondents [54]. Zou et al. [28], administered their PROM-questionnaire through a clinician-directed interview. Despite this being delivered by a skilled interviewer, who was not connected to the research study, face-to face interviews carry with it the possibility of interviewer bias [55].
There was little homogeneity regarding the timepoints of questionnaire administration, inhibiting quantitative analysis between studies. The most measured timepoint was 3 months post-operatively (n = 8) followed by at both 6 and 12 months (n = 6). Eight of the studies in this review administered the questionnaire exclusively at or after 12 months post-operatively. Smretschnig et al. [56] found that QOL generally improves in the 3 to 12 months’ postoperatively, possibly plateauing after this time period. Van de Put et al. [46] report significantly higher QOL composite scores 12 months after surgery for RD. Tracking patient outcomes over time can help evaluate which post-operative interventions are most effective and may facilitate modifying interventions [57].
Overall, there is no consensus amongst researchers as to the most appropriate timepoints of PROM administration. We feel further work is needed in tracking QOL over time post-operatively to recommend standardised outcome timepoints. Standardisation between studies will permit higher-level evidence such as meta-analysis to guide future resource allocation and best-practice guidelines.
Choosing the ideal PROM-tool for vitreoretinal disease
The ideal PROM-tool is able to distinguish clinically useful changes in ocular condition whilst being short and simple enough to complete in a busy clinical environment. Inclusion of disease-specific domains may allow the PROM-tool to be responsive-enough to help guide and monitor treatments. Similarly, generic PROM-tools such as those discussed earlier in this review can allow the comparison of PROMs between different populations and diseases and therefore be useful in calculating QALYs. This has useful research implications and is particularly useful for clinical trials and economic evaluation. In reality, it is likely therefore that a combination of PROM-tools should be used.
Following COSMIN methodology, it is difficult to formulate a recommendation on the most suitable PROM-tool for vitreoretinal surgery. We have discussed methodological shortcomings and the limited validation of the identified PROM-tools for a VR-specific subset of conditions and patients. A large proportion of identified studies did not disclose any statement on financial conflict of interest (n = 4, 29%). Whilst it is acknowledged in these cases, there may not have been a relevant disclosure to make, a short statement clarifying this would reassure any critical appraiser. Furthermore, a key element of PROMs are how well they are accepted by patients, as ultimately patients must be willing and able to relay their thoughts and opinions regarding their condition. We feel it is essential that PROM studies include some analysis of acceptability to patients and the ease of administration. PROM-tools have the potential to bridge the gap between a clinician’s and patient’s understanding of treatment success. Ideally PROMs should therefore be co-developed by patients and clinicians to ensure acceptability and ease of use. Choosing the best PROM tool takes healthcare one step closer to discover the patient voice in Ophthalmology [58].
There are a few limitations of this systematic review. We felt quantitative analysis in terms of meta-analysis was unfeasible and of limited value to the end-clinician, given, the significant heterogeneity of PROM-tools used, their differing timepoints of administration and often lack of baseline PROM-assessment prior to undergoing vitreoretinal surgery. This literature search focused on medical databases which included only peer-reviewed articles and hence has the potential to miss relevant but possibly less robust non-peer-reviewed literature. Our systematic review protocol was not pre-registered in a publicly available registry, which in theory could introduce bias in the conduct and reporting of the systematic review. Furthermore, an aim of this review was to recommend a PROM tool for use in VR surgery, which could not be done with confidence due to the lack of robust studies identified. We found very few studies reporting data on acceptability or the patient perspective on the relevance of PROMs in terms of clarity, structure or ease of use. This data is valuable, particularly considering this cohort of patients are likely to have visual disturbance and therefore, a time-consuming and difficult questionnaire would be logistically challenging to implement. Greatest progress, in terms of developing and validating PROMs and introducing standardised outcome measures into RCTs, has been made in other Ophthalmic subspecialties such as in ‘Low Vision’ and glaucoma [59], but vitreoretinal surgery, at present, lags behind.
Conclusion
This review identified a general lack of research in PROMs for vitreoretinal surgery, lagging behind a number of other ophthalmic subspecialties. Of the fourteen identified studies, no vitreoretinal disease-specific PROM tools were identified. The majority of studies used either generic PROM-tools such as EQ5D or vision-related PROM-tools such as the NEI VFQ-25. We have considered their applicability to a vitreoretinal cohort of patients and feel these instruments would benefit from further psychometric testing and standardised implementation across larger clinical trials. A confident recommendation for a preferred PROM-tool for use in vitreoretinal surgery could therefore not be made due to the lack of robust studies in the current literature. There is a need for further PROM-work in developing and validating vitreoretinal-specific PROM tools. There is also a need for standardisation of core outcomes for vitreoretinal surgery, of which PROMs should be an integral part. This is essential to guide future randomised-controlled trials in vitreoretinal surgery and permit higher levels of evidence such as meta-analysis to inform clinical best-practice.
Summary
What was known before
-
Vitreoretinal surgery can be extremely effective at restoring vision, but clinical outcomes can be unpredictable, and these outcomes do not always correlate well with patient satisfaction.
-
Patient reported outcome measures (PROMs) put the patient at the centre of their care and are increasingly important to justify the provision and funding of healthcare resources.
-
Many ophthalmic subspecialties and medical specialties have developed and validated disease-specific PROM-tools to guide standardised core outcomes of success after treatment.
What this study adds
-
This is the first systematic review to review the current literature on the use of PROMs specifically in vitreoretinal surgery.
-
Vitreoretinal surgery lags behind other ophthalmic subspecialties in the adoption of PROMs as a core outcome of success after surgery. No vitreoretinal disease-specific PROM-tools were identified.
-
There was significant heterogeneity in the implementation of generic and vision-specific PROM-tools; timepoints of administration and lack of baseline measurements inhibited quantitative comparison across studies. Further work is needed to develop and validate a robust vitreoretinal-specific PROM-tool in an effort to standardise core outcome sets for vitreoretinal surgery.
Data availability
All data generated or analysed during this study are included in this published article [and its supplementary information files].
References
Devlin NJ, Parkin D, Browne J. Patient-reported outcome measures in the NHS: new methods for analysing and reporting EQ-5D data. Health Economics. 2010;19:886–905.
Weldring T, Smith SMS. Patient-reported outcomes (PROs) and patient-reported outcome measures (PROMs). Health Serv Insights. 2013;6:61–8.
Braithwaite T, Calvert M, Gray A, Pesudovs K, Denniston AK. The use of patient-reported outcome research in modern ophthalmology: impact on clinical trials and routine clinical practice. Patient Relat Outcome Meas. 2019;10:9–24.
Novick MR. The axioms and principal results of classical test theory. Journal of Mathematical Psychology. 1966;3:1–18.
Chang C-H, Reeve BB. Item response theory and its applications to patient-reported outcomes measurement. Evaluation & the Health Professions. 2005;28:264–82.
Andrich D. Rating scales and Rasch measurement. Expert Review of Pharmacoeconomics & Outcomes Research. 2011;11:571–85.
Margolis MK, Coyne K, Kennedy-Martin T, Baker T, Schein O, Revicki DA. Vision-specific instruments for the assessment of health-related quality of life and visual functioning: a literature review. Pharmacoeconomics. 2002;20:791–812.
Guillemin F, Bombardier C, Beaton D. Cross-cultural adaptation of health-related quality of life measures: literature review and proposed guidelines. J Clin Epidemiol. 1993;46:1417–32.
Brooks R. EuroQol: the current state of play. Health Policy. 1996;37:53–72.
Ware JE Jr, Sherbourne CD. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med Care. 1992;30:473–83.
Clark MJ, Harris N, Griebsch I, Kaschinski D, Copley-Merriman C. Patient-reported outcome labeling claims and measurement approach for metastatic castration-resistant prostate cancer treatments in the United States and European Union. Health and quality of life outcomes. 2014;12:104.
Fryback DG, Palta M, Cherepanov D, Bolt D, Kim J-S. Comparison of 5 health-related quality-of-life indexes using item response theory analysis. Med Decis Making. 2010;30:5–15.
Khadka J, McAlinden C, Pesudovs K. Quality assessment of ophthalmic questionnaires: review and recommendations. Optom Vis Sci. 2013;90:720–44.
British and Eire Association of Vitreoretinal Surgeons. What is VR surgery? 2022 [06/03/2022]. Available from: https://beavrs.org/what-is-vr-surgery.
Lundström M, Wendel E. Assessment of vision-related quality of life measures in ophthalmic conditions. Expert Review of Pharmacoeconomics & Outcomes Research. 2006;6:691–724.
Scott IU, Smiddy WE, Feuer W, Merikansky A. Vitreoretinal surgery outcomes: results of a patient satisfaction/functional status survey. Ophthalmology. 1998;105:795–803.
Nelson EC, Eftimovska E, Lind C, Hager A, Wasson JH, Lindblad S. Patient reported outcome measures in practice. Bmj. 2015;350:g7818.
Mokkink LB, de Vet HCW, Prinsen CAC, Patrick DL, Alonso J, Bouter LM, et al. COSMIN Risk of Bias checklist for systematic reviews of Patient-Reported Outcome Measures. Qual Life Res. 2018;27:1171–9.
Prinsen CAC, Mokkink LB, Bouter LM, Alonso J, Patrick DL, de Vet HCW, et al. COSMIN guideline for systematic reviews of patient-reported outcome measures. Qual Life Res. 2018;27:1147–57.
Terwee CB, Prinsen CAC, Chiarotto A, Westerman MJ, Patrick DL, Alonso J, et al. COSMIN methodology for evaluating the content validity of patient-reported outcome measures: a Delphi study. Qual Life Res. 2018;27:1159–70.
Potic J, Bergin C, Giacuzzo C, Konstantinidis L, Daruich A, Wolfensberger TJ. Application of modified NEI VFQ-25 after retinal detachment to vision-related quality of life. Retina. 2021;41:653–60.
Kovac B, Vukosavljevic M, Djokic Kovac J, Resan M, Trajkovic G, Jankovic J, et al. Validation and cross-cultural adaptation of the National Eye Institute Visual Function Questionnaire (NEI VFQ-25) in Serbian patients. Health and Quality of Life Outcomes. 2015;13:142.
Mangione CM, Lee PP, Gutierrez PR, Spritzer K, Berry S, Hays RD. Development of the 25-item National Eye Institute Visual Function Questionnaire. Archives of Ophthalmology. 2001;119:1050–8.
Orr P, Rentz AM, Margolis MK, Revicki DA, Dolan CM, Colman S, et al. Validation of the National Eye Institute Visual Function Questionnaire-25 (NEI VFQ-25) in age-related macular degeneration. Invest Ophthalmol Vis Sci. 2011;52:3354–9.
Nassiri N, Mehravaran S, Nouri-Mahdavi K, Coleman AL. National Eye Institute Visual Function Questionnaire: usefulness in glaucoma. Optom Vis Sci. 2013;90:745–53.
Wan Y, Zhao L, Huang C, Xu Y, Sun M, Yang Y, et al. Validation and comparison of the National Eye Institute Visual Functioning Questionnaire-25 (NEI VFQ-25) and the Visual Function Index-14 (VF-14) in patients with cataracts: a multicentre study. Acta Ophthalmol. 2021;99:e480–8.
Pesudovs K, Gothwal VK, Wright T, Lamoureux EL. Remediating serious flaws in the National Eye Institute Visual Function Questionnaire. J Cataract Refract Surg. 2010;36:718–32.
Zou HD, Zhang X, Xu X, Liu HY, Bai L, Xu X. Vision-Related Quality of Life and Self-Rated Satisfaction Outcomes of Rhegmatogenous Retinal Detachment Surgery: 3-Year Prospective Study. Plos One. 2011;6:e28597.
Devlin NJ, Brooks R. EQ-5D and the EuroQol Group: past, present and future. Appl Health Econ Health Policy. 2017;15:127–37.
Bott U, Mühlhauser I, Overmann H, Berger M. Validation of a diabetes-specific quality-of-life scale for patients with type 1 diabetes. Diabetes Care. 1998;21:757–69.
Yu Y, Feng L, Shao Y, Tu P, Wu HP, Ding X, et al. Quality of life and emotional change for middle-aged and elderly patients with diabetic retinopathy. Int J Ophthalmol. 2013;6:71–4.
Koriyama M, Nishimura T, Matsubara T, Taomoto M, Takahashi K, Matsumura M. Prospective study comparing the effectiveness of scleral buckling to vitreous surgery for rhegmatogenous retinal detachment. Japanese journal of ophthalmology. 2007;51:360–7.
Kandel H, Khadka J, Lundström M, Goggin M, Pesudovs K. Questionnaires for measuring refractive surgery outcomes. J Refract Surg. 2017;33:416–24.
Hillier RJ, Felfeli T, Berger AR, Wong DT, Altomare F, Dai D, et al. The Pneumatic Retinopexy versus Vitrectomy for the Management of Primary Rhegmatogenous Retinal Detachment Outcomes Randomized Trial (PIVOT). Ophthalmology. 2019;126:531–9.
Okamoto F, Okamoto Y, Hiraoka T, Oshika T. Effect of vitrectomy for epiretinal membrane on visual function and vision-related quality of life. American Journal of Ophthalmology. 2009;147:869–74.
Ternent L, Vale L, Boachie C, Burr JM, Lois N. Cost-effectiveness of internal limiting membrane peeling versus no peeling for patients with an idiopathic full-thickness macular hole: results from a randomised controlled trial. British journal of ophthalmology. 2012;96:438–43.
Donovan JL, Brookes ST, Laidlaw DA, Hopper CD, Sparrow JM, Peters TJ. The development and validation of a questionnaire to assess visual symptoms/dysfunction and impact on quality of life in cataract patients: the Visual Symptoms and Quality of life (VSQ) Questionnaire. Ophthalmic Epidemiol. 2003;10:49–65.
Ng H, Vermeer KA, van Meurs JC, La Heij EC. Visual acuity inadequately reflects vision-related quality of life in patients after macula-off retinal detachment surgery. Invest Ophthalmol Vis Sci. 2020;61:34.
Lina G, Xuemin Q, Qinmei W, Lijun S. Vision-related quality of life, metamorphopsia, and stereopsis after successful surgery for rhegmatogenous retinal detachment. Eye. 2016;30:40–5.
Kobayashi M, Iwase T, Yamamoto K, Ra E, Murotani K, Terasaki H. Perioperative factors that are significantly correlated with final visual acuity in eyes after successful rhegmatogenous retinal detachment surgery. PLoS One. 2017;12:e0184783. e
Miskala PH, Hawkins BS, Mangione CM, Bass EB, Bressler NM, Dong LM, et al. Responsiveness of the National Eye Institute Visual Function Questionnaire to changes in visual acuity: findings in patients with subfoveal choroidal neovascularization-SST Report No. 1. Arch Ophthalmol. 2003;121:531–9.
Subhi Y, Henningsen G, Larsen CT, Sørensen MS, Sørensen TL. Foveal morphology affects self-perceived visual function and treatment response in neovascular age-related macular degeneration: a cohort study. PLoS One. 2014;9:e91227.
Hirneiss C. The impact of a better-seeing eye and a worse-seeing eye on vision-related quality of life. Clin Ophthalmol. 2014;8:1703–9.
Waheed K, Laidlaw DAH. Disease laterality, eye dominance, and visual handicap in patients with unilateral full thickness macular holes. British Journal of Ophthalmology. 2003;87:626–8.
Chua PY, Sandinha MT, Steel DH. Idiopathic epiretinal membrane: progression and timing of surgery. Eye. 2021;36:495–503.
van de Put MA, Vehof J, Hooymans JM, Los LI. Postoperative metamorphopsia in macula-off rhegmatogenous retinal detachment: associations with visual function, vision related quality of life, and optical coherence tomography findings. PLoS One. 2015;10:e0120543.
Patel PJ, Steel DH, Hirneiß C, Brazier J, Aly A, Lescrauwaet B, et al. Patient-reported prevalence of metamorphopsia and predictors of vision-related quality of life in vitreomacular traction: a prospective, multi-centre study. Eye. 2019;33:435–44.
Kinoshita T, Imaizumi H, Okushiba U, Miyamoto H, Ogino T, Mitamura Y. Time course of changes in metamorphopsia, visual acuity, and OCT parameters after successful epiretinal membrane surgery. Investigative Ophthalmology & Visual Science. 2012;53:3592–7.
Gupta B, Sivaprasad S, Wong R, Laidlaw A, Jackson TL, McHugh D, et al. Visual and anatomical outcomes following vitrectomy for complications of diabetic retinopathy: the DRIVE UK study. Eye (Lond). 2012;26:510–6.
Unsal E, Cubuk MO, Ciftci F. Preoperative prognostic factors for macular hole surgery: Which is better? Oman J Ophthalmol. 2019;12:20–4.
Hirata N, Iwase T, Kobayashi M, Yamamoto K, Ra E, Terasaki H. Correlation between preoperative factors and final visual acuity after successful rhegmatogenous retinal reattachment. Scientific Reports. 2019;9:3217.
Fukuhara S, Wakita T, Yamada M, Hiratsuka Y, Green J, Oki K. Development of a short version of the visual function questionnaire using item-response theory. PLoS One. 2013;8:e73084.
AHRQ Methods for Effective Health Care. In: Gliklich RE, Dreyer NA, Leavy MB, editors. Registries for Evaluating Patient Outcomes: A User’s Guide. Rockville (MD): Agency for Healthcare Research and Quality (US); 2014.
Conway JM, Lance CE. What reviewers should expect from authors regarding common method bias in organizational research. Journal of Business and Psychology. 2010;25:325–34.
Jelin E, Wisløff T, Moe MC, Heiberg T. Psychometric properties of the National Eye Institute Visual Function Questionnaire (NEI-VFQ 25) in a Norwegian population of patients with neovascular age-related macular degeneration compared to a control population. Health and quality of life outcomes. 2019;17:140.
Smretschnig E, Falkner-Radler CI, Binder S, Spörl J, Ristl R, Glittenberg C, et al. VISION-RELATED QUALITY OF LIFE AND VISUAL FUNCTION AFTER RETINAL DETACHMENT SURGERY. Retina. 2016;36:967–73.
Basch E, Abernethy AP. Commentary: encouraging clinicians to incorporate longitudinal patient-reported symptoms in routine clinical practice. J Oncol Pract. 2011;7:23–5.
Dean S, Mathers JM, Calvert M, Kyte DG, Conroy D, Folkard A, et al. “The patient is speaking”: discovering the patient voice in ophthalmology. British Journal of Ophthalmology. 2017;101:700–8.
Robertson AO, Tadić V, Rahi JS. Attitudes, experiences, and preferences of ophthalmic professionals regarding routine use of patient-reported outcome measures in clinical practice. PLoS One. 2020;15:e0243563.
Author information
Authors and Affiliations
Contributions
AY was responsible for designing the review protocol, writing the protocol and report, conducting the search, screening potentially eligible studies, extracting and analysing data, interpreting results, updating reference lists and creating’Summary of findings’ tables. AY, AD were responsible for screening potentially eligible studies. MS contributed to writing the report, extracting and analysing data, interpreting results and creating’Summary of findings’ tables. TS contributed to the design of the review protocol and arbitrating potentially eligible studies. TS and DS provided feedback on the report.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Yoganathan, A., Sandinha, T., Shamdas, M. et al. Patient-reported outcome measures in vitreoretinal surgery: a systematic review. Eye 37, 391–401 (2023). https://doi.org/10.1038/s41433-022-02073-8
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41433-022-02073-8
