
Abstract
Purpose
To assess post-operative outcomes following photorefractive keratectomy (PRK) in patients with posterior corneal steepening compared to an age, gender and refraction matched control group.
Methods
A retrospective matched case-control study that analysed outcomes of PRK in eyes with posterior corneal steepening as shown by the Sirius tomography (Sirius, CSO, Italy), versus normal eyes. Both groups were age, gender and refraction matched. Data collected include: demographic data, pre-operative and post-operative refraction, uncorrected distance visual acuity (UDVA) and corrected distance visual acuity (CDVA), maximal ablation depth. Inferior–superior ratio, central corneal thickness (CCT), mean posterior keratometry (K), Baiocchi Calossi Versaci index for the front (BCVf) and back (BCVb) cornea, the symmetry index of front (SIf) and back (SIb) corneal curvature were assessed pre- and postoperatively.
Results
Overall, 89 study eyes and 954 normal myopic eyes were included. Compared to the control group, corneas with posterior steepening demonstrated significantly reduced CDVA (p < 0.0001 and p = 0.007) and lower CCT (p < 0.0001 and p = 0.03), before and following the operation, respectively. Pre-operative BCVf, BCVb, SIf and SIb were significantly higher in corneas with posterior steepening (p < 0.0001) and remained higher following the surgery except for BCVf. Ectasia occurred in one eye (1.1%). The safety and efficacy indices at 12 months were comparable for both groups.
Conclusion
PRK on corneas with posterior steepening results in similar refractive outcomes compared to normal eyes, 1 year following the surgery. Keratectasia is a rare, however a possible complication.
Similar content being viewed by others
Introduction
Refractive surgery on irregular corneas has long been contraindicated due to the post-operative risk of corneal ectasia [1]. Numerous studies have reported ectasia development following photorefractive keratectomy (PRK), though the risk is significantly lower when compared to laser in situ keratomileusis, which involves creating a flap that, as a result, alters the biomechanics of the cornea and renders the cornea more prone to keratectasia [2]. Eyes with posterior steepening as demonstrated by tomography, are a major concern once considered for refractive surgery, however, the risk of operating on those eyes has yet to be established.
Performing surface ablation on eyes with abnormal corneas remains a controversial and challenging issue. Eyes with posterior steepening as demonstrated by tomography, are a major concern once considered for refractive surgery, however, the risk of operating on those eyes has yet to be established.
Nowadays, the diagnosis of suspect and early keratoconus is becoming more precise thanks to the different tomography methods. The combined placido disk and rotating Scheimpflug camera technique, obtains accurate measurements of the whole cornea [3] which have been reported to be highly reproducible and repeatable [4, 5]. Based on posterior corneal characteristics, regularity of the anterior central corneal surface, pachymetry, epithelium thickness and other new indices, subjects that were previously considered normal can now be defined as suspected or early keratoconus [6].
Keratoconus suspects (KCS) display a slightly skewed astigmatism on the anterior surface and markedly asymmetric curvature and abnormal elevation on the posterior corneal curvature [7]. Several studies reported the safety and efficacy of surface ablation in forme fruste, keratoconus suspect and keratoconus eyes. In a prospective non-comparative study, Koller et al. [8] reported the efficacy of customised surface ablation in forme fruste keratoconus. Compared to pre-operative status, a significant reduction of manifest refractive error, corneal irregularity, and ghosting was shown. The 5 year outcomes of PRK in KCS were published by Guedj et al. [9]. The study included 62 eyes and no cases of keratectasia were reported. Khakshoor et al. [10] reported prospectively long-term outcomes of PRK in 38 mild to moderate keratoconus eyes of 21 patients, with predicted post-operative residual central corneal thickness (CCT) ≥400 μm. Mean uncorrected and corrected distance visual acuity (CDVA), spherical equivalent, cylindrical power and keratometry readings were significantly improved at the final endpoint compared to pre operation measurements and no case of ectasia occurred during the follow-up course.
Herein, we report the safety, efficacy, corneal thickness profile, visual and tomography outcomes of PRK for correction of myopia in eyes with suspected early corneal ectatic changes (posterior steepening), compared to normal eyes.
Methods
All data for the study were collected and analysed in accordance with the policies and procedures of the Institutional Review Board of the Barzilai Medical Centre and the tenets set forth in the declaration of Helsinki.
Study participants
This retrospective case-control study included two groups of patients, of various ethnicity groups, who underwent PRK by multiple surgeons between July 2012 and December 2015 at Care-Vision Laser Centres, Tel-Aviv, Israel. The study group consisted of eyes with suspected keratoconus as defined by the Sirius Scheimpflug–Placido corneal tomography (CSO, Costruzione Strumenti Oftalmici, Florence, Italy), and a control group of normal myopic candidates. We included eyes that demonstrate an abnormal posterior cornea based on Baiocchi Calossi Versaci back index (BCVb) and the symmetry index of the back (SIb), but normal anterior corneal indices: Baiocchi Calossi Versaci front index (BCVf) and the symmetry index of the front (SIf). Those eyes were classified by the Sirius as ʻsuspect keratoconus’. The above values’ ranges of normal and suspected corneas were determined based on previous studies [11].
Eyes were considered ʻnormal’ if they had no ocular pathology, no previous ocular surgery and no irregular corneal pattern on Sirius tomography. Inclusion criteria for surgery were: age over 18 years; a stable refraction for at least 12 months; pre-surgical corneal thickness above 450 μm; predicted post-surgical thickness of at least 350 μm; IOP <21 mmHg; a period without wearing contact lenses (more than 2 weeks for rigid contact lenses and more than 4 days for soft contact lenses); and no history of autoimmune disease, diabetes or previous ocular surgery. We included patients with myopia up to −12 D or with a cylinder of up to −6 D. Patients with a follow-up duration of ~12 months were included. Patients with monovision correction were excluded.
Data collection
The medical notes of all eligible patients were reviewed, and the following were extracted: demographic and pre-operative information: age, gender, date of surgery. Intraoperative information: theatre humidity and temperature, optic zone, maximum ablation depth, percent of tissue ablated and the involved eye (right or left). Post-operative collected data included: SE, astigmatism, deviation from target refraction and ectasia development. CDVA, pachymetry, inferior–superior keratometry (K) ratio, BCVf, BCVb, SIf and SIb were noted pre- and postoperatively.
Tomography parameters’ acquisition
Tomography was obtained for all patients pre- and postoperatively using the Sirius Scheimpflug–Placido tomographer (Sirius, CSO, Italy) that combines a monochromatic rotating Scheimpflug camera and a Placido disk. The scanning process acquires a series of 25 Scheimpflug images (meridians) and 1 Placido top-view image to analyse the anterior segment by obtaining 25 radial sections of the cornea and anterior chamber. Anterior surface data from Placido and Scheimpflug images are merged using a proprietary method. All the other measurements for internal structures (posterior corneal curvature, anterior lens surface, and iris) are derived solely from Scheimpflug data. Previous studies have reported the system’s pachymetric and shape measurements (curvature, eccentricity, elevation) to have good repeatability [12].
Measurements were performed by a standard protocol. The patient’s eye was aligned along the visual axis using a central fixation light. The images were obtained with the automatic mode. The system constantly monitored eye movements of the subject, and quality factor was automatically evaluated. In case of a poor-quality scan, artifacts and irregularities (e.g. due to misalignment or blinks during the scan), more shots were performed until a good quality picture was obtained. The patient was excluded if the final scan was of poor quality. Artificial tears were used to allow better acquisition when a difficulty in obtaining the scan was encountered.
Tomographical analysis
The diagnosis of suspected keratoconus was inferred based on measurements obtained by Sirius corneal tomography. The following indices were evaluated: tangential curvature of the anterior and posterior corneal surface; thickness profile; inferior/superior ratio of K; symmetry index of front corneal curvature (SIf) defined as the difference in mean anterior tangential curvature (expressed in dioptres) between two circular zones centred on the vertical axis in the inferior and superior hemispheres. Positive values indicate a steeper inferior hemisphere, whereas negative values indicate a steeper superior hemisphere. Likewise, the symmetry index of back curvature (SIb) is defined as the difference in mean posterior tangential curvature between two circular zones centred on the vertical axis in the inferior and superior hemispheres [13]; BCVf, expressed in micrometres, is a combination of vertical trefoil Z(3,3), vertical coma Z(3,1), horizontal coma Z(3,C1), primary spherical aberration Z(4,0), and 2nd-order vertical coma Z(5,1) coefficients, likewise, a linear combination of Z(3,3), Z(3,1), Z(3,C1), Z(4,0), and Z(5,1) and information about the coma axis on the posterior Zernike decomposition defines the BCVb [13].
The Baiocchi Calossi Versaci index of the front and back, (BCVf) and (BCVb), is a combination of higher order aberrations, that was reported to demonstrate a progressive increase in eyes with suspected keratoconus and keratoconus [11]. Moreover, it can be used to detect the grade of keratoconus as reported by Alio et al. [14]. Surface asymmetry index (SAI) is an average value indicating differences between points spatially located at 180° from 128 equidistant meridians on the front (SAIf) and back (SAIb) surfaces [15]. The SAI of a radially symmetric surface is zero, and this value will increase as the asymmetry is greater, as such in irregular astigmatism of keratoconus eyes. Shetty et al. demonstrated a 100% sensitivity and specificity of BCV and SAI in differentiating between KC and normal eyes [16].
By combining and processing the above parameters, in addition to data regarding steepening and ectasia, the device classifies the eyes into: normal, suspect keratoconus and keratoconus.
Surgical technique
The PRK procedures were performed by five surgeons at the same institution. All patients underwent PRK in a similar manner with residual stromal bed >300 μm in all cases. One drop of a topical anaesthetic (benoxinate hydrochloride 0.4%) was instilled in the conjunctival fornix of the eye prior to the procedure, after which a lid speculum was inserted. Epithelial removal was performed by means of alcohol delamination (20% ethyl alcohol placed on the cornea for 15 s). Following removal of epithelium, the WaveLight® Allegretto Wave® (EX200) excimer laser system was used and after ablation a sponge soaked with 0.02% mitomycin C was placed on the stroma for 20–60 s (depending on the amount of ablation). MMC time is 30, 40 and 60 s for corrections of up to 6 D, between 6 and 8 D and above 8 D correction, respectively. A bandage contact lens was placed after rinsing the mitomycin.
Following the operation, patients were prescribed moxifloxacin 0.5% (q.i.d), dexamethasone 0.1% or fluorometholone 0.1% (q.i.d) and artificial tears (q.i.d).
Follow-up
Patients were examined at the first post-op day and 1 week, 1, 3, 6 and 12 months post operatively and encouraged to return for examination if vision deteriorated at any time after surgery. On post-operative days 1 and 7, we determined UDVA and a slit-lamp inspection was performed. During the following appointments, we performed auto-refractometry, corneal tomography acquired by Sirius tomography, manifest refraction using the fogging technique, uncorrected distance visual acuity (UDVA) and CDVA, applanation tonometry and slit-lamp inspection of the anterior and posterior segments of all the eyes. The average follow- up period was 328.24 ± 197.45 for the suspects group and 334.47 ± 156.67 for the controls.
Statistical analysis
Data were analysed using the SPSS statistical software version 23.0 (SPSS, Cary, NC, USA). When comparing the groups of posterior corneal steepening patients with normal corneas, Student’s T test was utilised for the analysis of continuous data. For the analysis of categorical variables, Chi-Square was used. In all analyses a two-sided P value < 0.05 was considered statistically significant. All presented means are accompanied by their respective standard deviations.
Results
Overall, 89 suspected keratoconus eyes that demonstrated abnormal posterior parameters and 954 normal matched control eyes met the inclusion criteria and were included in the final analysis of this study. Only one eye of each patient was assessed. All surgeries were uneventful and the bandage lens were removed on post-operative days 5–7.
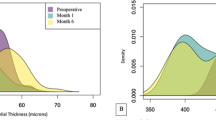
Demographic and pre-operative data are shown in Table 1. At baseline, both arms were age, gender and refraction matched. A statistically significant difference was found in pre-operative CDVA. Compared to the study group, normal eyes demonstrated a better pre-operative CDVA (0.03 ± 0.04 logMAR, Snellen equivalent 20/21 ± 0.4 lines, vs. 0.01 ± 0.05 logMAR, Snellen equivalent 20/20 ± 0.5 lines, p = <0.0001, respectively). Corneal thickness was lower in the study group before and following the operation (Table 2) compared to the normal controls (pre-operative values: 499.26 ± 25.14 and 517.33 ± 36.45, p < 0.0001, respectively. Post-operative values: 430.11 ± 46.52 and 440.92 ± 40.99, p = 0.03, respectively).
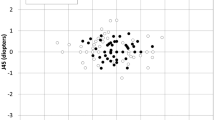
Table 2 presents outcomes at the last follow-up. Post operatively, we found a statistically significant difference between eyes with posterior steepening and the control eyes in terms of CDVA (0.03 ± 0.05 logMAR, Snellen equivalent 20/21 ± 0.5 line, vs. 0.01 ± 0.05 logMAR, Snellen equivalent 20/20 ± 0.5 lines, respectively. P = 0.007). No significant difference was found in post-operative SE, astigmatism and deviation from target refraction. Efficacy was defined as the ratio of post-operative UDVA divided by pre-operative CDVA. Efficacy in eyes with posterior steepening and their matched controls (Fig. 1) did not differ (0.96 ± 0.24 vs. 0.93 ± 0.23, p = 0.264, respectively).

Efficacy index of PRK in corneas with posterior steepening vs. controls.
Safety was calculated by dividing post-operative CDVA by pre-operative CDVA. There were no differences among groups with regards to safety outcomes (Fig. 2) (1.01 ± 0.11 vs. 1 ± 0.13, p = 0.134, for the study and the control groups, respectively).

Safety index of PRK in corneas with posterior steepening vs. controls.
The BCV and SI values are presented in Table 3. Prior to surgery BCVf, BCVb, SIf and SIb were significantly higher among corneas with suspected keratoconus. Following the operation, these parameters remained significantly higher except for the anterior BCV (p = 0.48).
Comparison of the surgically induced changes (ʻpre-op’ minus ʻpost-op’) in BCVf, BCVb, SIf, SIb and inferior–superior ratio of anterior K values between the two groups, yields insignificant differences for each parameter (P > 0.05).
Corneal ectasia was diagnosed if visual acuity was deteriorating and keratometry and SI were increasing. Among the keratoconus-suspect group, one participant (1.1%), has developed corneal ectasia about 27 months following the surgery. Ectasia did not occur in the control group.
Discussion
In the current study, we present the clinical and tomographic outcomes of PRK in eyes diagnosed with suspected keratoconus, compared to normal myopic eyes, and followed up for at least 1 year.
Based on analysis of several morphological maps—thickness, anterior and posterior elevation, anterior and posterior tangential curvature—and through specific indices with normative values, a keratoconus summary is delivered by the Sirius Scheimpflug–Placido disk device, which guides in the diagnosis of suspected and early stages of keratoconus. In our study, we included eyes diagnosed as ʻkeratoconus suspect’ by the instrument, excluding corneas with abnormal anterior indices, therefore, defined as posterior corneal steepening.
At baseline, the mean CDVA of the study group was significantly worse than the normal eyes. A study by Jafri et al. [17] found a significantly higher rate of HOA’s in keratoconus-suspect eyes compared to normal myopic eyes. We assume this is due to the impact of higher order aberrations (HOA’s), induced by the posterior cornea, on visual acuity [18, 19] which might likewise explain the post-surgical outcome of worse CDVA in those subjects.
Corneal thickness was significantly lower in eyes with posterior steepening at baseline and following the surgery, with average residual corneal thickness of 430.11 μm versus 440.92 μm in normal corneas. However, it is uncertain whether a post-surgical mean difference of about 10 μm carries any clinical significance. Safarzadeh and Nasiri [11] and Schlegel et al. [20] reported lower mean central and thinnest pachymetry values in keratoconus-suspect eyes compared to normal eyes. In a non-comparative study, Khashkoor et al. [21] accepted a minimum residual CCT of ≥400 μm as to be safe in mild and moderate keratoconus patients following PRK. In their study, mean follow-up duration was 35 months and no case of ectasia occurred during the follow-up course.
In our study, following PRK, there were no statistically significant differences between the two groups in SE, cylinders and deviation from target refraction. This is consistent with the findings of several studies. Sun et al. [22] reported comparable refractive outcomes of PRK in three patients suspected of keratoconus and a control group. Similarly, Alpins and Stamatelatos [23] reported stable UDVA and CDVA, 1-year after PRK in forme fruste and mild keratoconus with no case of keratoconus progression observed during the follow-up course.
Prior to surgery, eyes with posterior steepening demonstrated higher front and back BCV values compared to normal eyes. Similarly, Fathy et al. [24] found progressive increase in BCVf and BCVb values in suspect keratoconus and keratoconus subjects than normal corneas. Interestingly, the reduction in post-surgical BCVf values were comparable among both groups, demonstrating a favourable effect of the treatment on suspected corneas in terms of HOA’s. The difference in BCVb values remained significant at last follow-up following the operation, however, the surgically induced changes in both BCVf and BCVb were comparable among the groups after the surgery.
The front and back surface asymmetry indices were significantly higher in the study group. However, following the surgery, the difference in the front SAI is almost insignificant (p = 0.04). Furthermore, the surgically induced changes in the front and back SAI, were similar in both groups. The SAI will not be increased by regular astigmatism or centrally located cones but will detect irregular astigmatism and decentred cones [25]. This value will increase as the irregular astigmatism increases or the decentred cone becomes steeper. Consequently, it should act as a disease progression marker.
The inferior/superior keratometry ratio is a value of curvature symmetry, with respect to the horizontal meridian, as the axis of reflection [26]. Li et al. [27] found a statistically significant difference in I–S value between normal and keratoconus suspected eyes. In our study, the surgically induced change in anterior I–S value was comparable between the groups, showing that corneas with posterior steepening initially, did not develop increased anterior inferior steepening post operatively, suggesting corneal stability after surgery.
Given the sensitivity and specificity of the I/S ratio, SAI and BCV parameters in the assessment of ectasia progression, the similar surgically induced changes in both groups suggest corneal stability following PRK in eyes with posterior corneal steepening. To the best of our knowledge, this is the first comparative study to assess BCV and SAI indices following PRK in corneas with abnormal posterior parameters.
All patients received wavefront-optimised treatment. wavefront-optimised treatments take some eye variables into account and use preprogrammed ablation profiles based on population analysis [28]. This technique offers advantages over traditional standard ablation. Wavefront-optimised will minimise the induction of new higher order aberrations, compared to the conventional treatment [29, 30]. Consequently, wavefront-optimised treatment often results in better-quality vision and fewer night vision complaints [31]. However, this method involves increase in ablation depth in the midperiphery of the optical zone [32].
Numerous studies have reported the outcomes of combining PRK with crosslinking (CXL) for corneas with keratoconus and post refractive surgery keratectasia, to halt the ectatic process and enhance functional visual outcomes. Simultaneous topography-guided PRK and CXL was shown to be more effective for visual rehabilitation as compared to CXL alone (Athens protocol) [33]. Studies comparing simultaneous vs. sequential CXL followed by PRK report variable outcomes. Some studies have not found significant difference between the two approaches [34], while others reported superior effect on visual rehabilitation with the same-day PRK and CXL as compared to sequential treatments [35]. Moreover, concurrent laser refractive surgery and CXL (PRK Xtra) has been performed in patients requiring high prescription correction to reduce the incidence of regression [36], thin corneas and corneas that demonstrate subtle changes suspected for early ectasia [37]. The current study excluded thin corneas and any anterior surface abnormalities. More studies are needed in order to assess the long- term outcomes of PRK on corneas with posterior changes only and evaluate the role of combining CXL with PRK.
In our study, one case of ectasia occurred in the study group (1.1%). Adverse events including complications and undesired consequences were not encountered during the follow-up course. In the literature, no cases of ectasia were reported in a study by Guedj et al. [9] who published the 5-year results of PRK in suspected keratoconus eyes. Similarly, no adverse effect of this type of surgery on the cornea and the disease process was observed in Cinnamo et al. [38] and Bilgihan et al. [39] studies. However, Chelala et al. [40] reported two cases of keratoconus progression out of 119 eyes with grade I and II whom ultimately underwent CXL.
This study is subject to certain limitations. Though a large number of eyes were included, one must bear in mind its retrospective nature making it vulnerable to certain biases such as selection bias which we believe was dealt with sufficiently by including all consecutive patients that met the inclusion\exclusion criteria. Regarding the study course, our follow-up is inadequate to evaluate ectasia development, but it is a practical starting point. Several reported cases show development of post-PRK ectasia as late as 5 and even 9 years after PRK [41, 42]. As a result, longer follow-up times are necessary for more accurate assessment of PRK safety in eyes with posterior abnormalities. Keratoconus suspect is an ill-defined entity. Recognising posterior abnormality is difficult as there is a lack of defined threshold criteria and a persistent ambiguity regarding the exact definition of this condition [20, 43]. In our study, we included eyes with normal anterior surface indices, however, posterior surface abnormalities and defined as suspect keratoconus by the Sirius device (combined Scheimpflug camera and Placido disk). This corneal tomography has a software that features a machine-learning classifier, the support vector machine (SVM), which aims to detect the presence of keratoconus or KCS [44]. Based on a study by Arbelaez et al. [45] the classification algorithm of the SVM machine included in the Sirius analyser showed high accuracy, precision, sensitivity, and specificity in discriminating among abnormal eyes, eyes with KC or subclinical KC, and normal eyes, particularly, when data of posterior surface and corneal thickness were included.
In summary, this study found good surgical outcomes for PRK in eyes suspected of keratoconus due to posterior corneal steepening. Differences in post-operative tomography were similar to the control normal myopic eyes. The refractive results at 12 months were excellent, with a mean spherical equivalent close to zero. Yet, a certain risk for post-surgical ectasia development exists. Further studies with longer follow-up periods and a larger sample of candidates are required to determine whether these results are repeatable.
Summary
What was known before
-
Corneal changes suspected for ectasia are relative contraindication for refractive surgery.
-
The outcomes of refractive surgery in corneas with posterior steepening are not well established.
What this study adds
-
PRK is safe to perform in corneas with posterior steepening and suspected for keratoconus.
-
PRK yields excellent refractive outcomes in posteriorly steep corneas.
References
Sorkin N, Kaiserman I, Domniz Y, Sela T, Munzer G, Varssano D. Risk assessment for corneal ectasia following photorefractive keratectomy. J Ophthalmol. 2017;2017:2434830. https://doi.org/10.1155/2017/2434830.
Bühren J, Schäffeler T, Kohnen T. Preoperative topographic characteristics of eyes that developed postoperative LASIK keratectasia. J Refract Surg. 2013;29:540–9. https://doi.org/10.3928/1081597X-20130719-04.
Shetty R, Arora V, Jayadev C, Nuijts RM, Kumar M, Puttaiah NK, et al. Repeatability and agreement of three scheimpflug-based imaging systems for measuring anterior segment parameters in keratoconus. Investig Opthalmol Vis Sci. 2014;55:5263. https://doi.org/10.1167/iovs.14-15055.
Nasser CK, Singer R, Barkana Y, Zadok D, Avni I, Goldich Y. Repeatability of the sirius imaging system and agreement with the pentacam HR. J Refract Surg. 2012;28:493–7. https://doi.org/10.3928/1081597X-20120619-01.
De la Parra-Colín P, Garza-León M, Barrientos-Gutierrez T. Repeatability and comparability of anterior segment biometry obtained by the sirius and the pentacam analyzers. Int Ophthalmol. 2014;34:27–33. https://doi.org/10.1007/s10792-013-9780-0.
Fernández Pérez J, Valero Marcos A, Martínez Peña FJ. Early diagnosis of keratoconus: what difference is it making?. Br J Ophthalmol. 2014;98:1465–6. https://doi.org/10.1136/bjophthalmol-2014-305120.
Klyce SD. Chasing the suspect: keratoconus. Br J Ophthalmol. 2009;93:845–7. https://doi.org/10.1136/bjo.2008.147371.
Koller T, Iseli HP, Donitzky C, Ing D, Papadopoulos N, Seiler T. Topography-guided surface ablation for forme fruste keratoconus. Ophthalmology. 2006;113:2198–202. https://doi.org/10.1016/j.ophtha.2006.06.032.
Guedj M, Saad A, Audureau E, Gatinel D. Photorefractive keratectomy in patients with suspected keratoconus: five-year follow-up. J Cart Refract Surg. 2012. https://doi.org/10.1016/j.jcrs.2012.08.058.
Khakshoor H, Razavi F, Eslampour A, Omdtabrizi A. Photorefractive keratectomy in mild to moderate keratoconus: Outcomes in over 40-year-old patients. Indian J Ophthalmol. 2015;63:157–161. https://doi.org/10.4103/0301-4738.154400.
Safarzadeh M, Nasiri N. Anterior segment characteristics in normal and keratoconus eyes evaluated with a combined Scheimpflug/Placido corneal imaging device. J Curr Ophthalmol. 2016;28:106–11. https://doi.org/10.1016/j.joco.2016.06.003.
Milla M, Piñero DP, Amparo F, Alió JL. Pachymetric measurements with a new Scheimpflug photography-based system: intraobserver repeatability and agreement with optical coherence tomography pachymetry. J Cataract Refract Surg. 2011;37:310–6. https://doi.org/10.1016/j.jcrs.2010.08.038.
Arbelaez MC, Versaci F, Vestri G, Barboni P, Savini G. Use of a support vector machine for keratoconus and subclinical keratoconus detection by topographic and tomographic data. Ophthalmology. 2012;119:2231–8. https://doi.org/10.1016/j.ophtha.2012.06.005.
Alió JL, Shabayek MH. Corneal higher order aberrations: a method to grade keratoconus. J Refract Surg. 2006;22:539–45. http://www.ncbi.nlm.nih.gov/pubmed/16805116. Accessed 23 Jun 2018.
Cavas-Martínez F, De la Cruz Sánchez E, Nieto Martínez J, Fernández Cañavate FJ, Fernández-Pacheco DG. Corneal topography in keratoconus: state of the art. Eye Vis. 2016;3:5. https://doi.org/10.1186/s40662-016-0036-8.
Shetty R, Rao H, Khamar P, Sainani K, Vunnava K, Jayadev C, et al. Keratoconus Screening Indices and Their Diagnostic Ability to Distinguish Normal From Ectatic Corneas. Am J Ophthalmol. 2017;181:140–148. https://doi.org/10.1016/j.ajo.2017.06.031.
Jafri B, Li X, Yang H, Rabinowitz YS. Higher order wavefront aberrations and topography in early and suspected keratoconus. J Refract Surg. 2007;23:774–81. http://www.ncbi.nlm.nih.gov/pubmed/17985796. Accessed 25 Jan 2017.
Applegate RA, Ballentine C, Gross H, Sarver EJ, Sarver CA. Visual acuity as a function of Zernike mode and level of root mean square error. Optom Vis Sci. 2003;80:97–105. http://www.ncbi.nlm.nih.gov/pubmed/12597324. Accessed 26 Jan 2017.
Negishi K, Kumanomido T, Utsumi Y, Tsubota K. Effect of higher-order aberrations on visual function in keratoconic eyes with a rigid gas permeable contact lens. Am J Ophthalmol. 2007;144:924–9.e1. https://doi.org/10.1016/j.ajo.2007.08.004.
Schlegel Z, Hoang-Xuan T, Gatinel D. Comparison of and correlation between anterior and posterior corneal elevation maps in normal eyes and keratoconus-suspect eyes. J Cataract Refract Surg. 2008;34:789–95. https://doi.org/10.1016/j.jcrs.2007.12.036.
Khakshoor H, Razavi F, Eslampour A, Omdtabrizi A. Photorefractive keratectomy in mild to moderate keratoconus: outcomes in over 40-year-old patients. Indian J Ophthalmol. 2015;63:157–61. https://doi.org/10.4103/0301-4738.154400.
Sun R, Gimbel HV, Kaye GB. Photorefractive keratectomy in keratoconus suspects. J Cataract Refract Surg. 1999;25:1461–6. http://www.ncbi.nlm.nih.gov/pubmed/10569160. Accessed 28 Jan 2017.
Alpins N, Stamatelatos G. Customized photoastigmatic refractive keratectomy using combined topographic and refractive data for myopia and astigmatism in eyes with forme fruste and mild keratoconus. J Cataract Refract Surg. 2007;33:591–602. https://doi.org/10.1016/j.jcrs.2006.12.014.
Fathy M, Agooz MHEI, Samman AH, Mostafa EM. Anterior segment characteristics of keratoconus eyes using Scheimpflug-Placido topography. J Clin Res Ophthalmol. 2016;3:003–7. https://doi.org/10.17352/2455-1414.000027.
Wilson SE, Klyce SD. Advances in the analysis of corneal topography. Surv Ophthalmol. 35:269–77. http://www.ncbi.nlm.nih.gov/pubmed/2011820. Accessed 31 Jan 2017.
Kanellopoulos AJ, Asimellis G. Revisiting keratoconus diagnosis and progression classification based on evaluation of corneal asymmetry indices, derived from scheimpflug imaging in keratoconic and suspect cases. Clin Ophthalmol. 2013;7:1539–48. https://doi.org/10.2147/OPTH.S44741.
Li X, Yang H, Rabinowitz YS. Keratoconus: classification scheme based on videokeratography and clinical signs. J Cataract Refract Surg. 2009;35:1597–603. https://doi.org/10.1016/j.jcrs.2009.03.050.
Perez-Straziota CE, Randleman BJ, Stulting DR. Visual acuity and higher-order aberrations with wavefront-guided and wavefront-optimized laser in situ keratomileusis. J Cataract Refract Surg. 2010;36:437–41. https://doi.org/10.1016/j.jcrs.2009.09.031.
Padmanabhan P, Mrochen M, Basuthkar S, Viswanathan D, Joseph R. Wavefront-guided versus wavefront-optimized laser in situ keratomileusis: contralateral comparative study. J Cataract Refract Surg. 2008;34:389–97. https://doi.org/10.1016/J.JCRS.2007.10.028.
Zhou C, Chai X, Yuan L, He Y, Jin M, Ren Q. Corneal higher-order aberrations after customized aspheric ablation and conventional ablation for myopic correction. Curr Eye Res. 2007;32:431–8. https://doi.org/10.1080/02713680701329321.
Schallhorn SC, Tanzer DJ, Kaupp SE, Brown M, Malady SE. Comparison of Night Driving Performance after Wavefront-Guided and Conventional LASIK for Moderate Myopia. Ophthalmology. 2009;116:702–709. https://doi.org/10.1016/j.ophtha.2008.12.038.
Mrochen M, Donitzky C, Wüllner C, Löffler J. Wavefront-optimized ablation profiles: theoretical background. J Cataract Refract Surg. 2004;30:775–85. https://doi.org/10.1016/J.JCRS.2004.01.026.
Kanellopoulos AJ. Ten-year outcomes of progressive keratoconus management with the athens protocol (topography-guided partial-refraction PRK combined with CXL). J Refract Surg. 2019;35:478–83. https://doi.org/10.3928/1081597X-20190627-01.
Abou Samra WA, El Emam DS, Farag RK, Abouelkheir HY. Simultaneous versus sequential accelerated corneal collagen cross-linking and wave front guided PRK for treatment of keratoconus: objective and subjective evaluation. J Ophthalmol. 2016;2016:2927546. https://doi.org/10.1155/2016/2927546.
Kanellopoulos AJ. Comparison of sequential vs. same-day simultaneous collagen cross-linking and topography-guided PRK for treatment of keratoconus. J Refract Surg. 2009;25:S812–8. https://doi.org/10.3928/1081597X-20090813-10.
Tamayo GE. Predictable visual outcomes with accelerated corneal cross-linking concurrent with laser in situ keratomileusis. J Cataract Refract Surg. 2012;38:2206. https://doi.org/10.1016/j.jcrs.2012.10.023. author reply 2207-8.
Sachdev GS, Ramamurthy S, Dandapani R. Comparative analysis of safety and efficacy of photorefractive keratectomy versus photorefractive keratectomy combined with crosslinking. Clin Ophthalmol.2018;12:783–90. https://doi.org/10.2147/OPTH.S156500.
Cennamo G, Intravaja A, Boccuzzi D, Marotta G, Cennamo G. Treatment of keratoconus by topography-guided customized photorefractive keratectomy: two-year follow-up study. J Refract Surg. 2008;24:145–9. http://www.ncbi.nlm.nih.gov/pubmed/18297938. Accessed 29 Jan 2017.
Bilgihan K, Ozdek SC, Konuk O, Akata F, Hasanreisoglu B. Results of photorefractive keratectomy in keratoconus suspects at 4 years. J Refract Surg. 16:438–43. http://www.ncbi.nlm.nih.gov/pubmed/10939723. Accessed 25 Jan 2017.
Chelala E, Rami HEL, Dirani A, Fadlallah A, Fakhoury O, Warrak E. Photorefractive keratectomy in patients with mild to moderate stable keratoconus: a five-year prospective follow-up study. Clin Ophthalmol.2013;7:1923–8. https://doi.org/10.2147/OPTH.S52281.
Kim H, Choi J-S, Joo C-K. Corneal ectasia After PRK. Cornea. 2006;25:845–8. https://doi.org/10.1097/01.ico.0000224634.72309.43.
Spadea L. Collagen crosslinking for ectasia following PRK performed in excimer laser–assisted keratoplasty for keratoconus. Eur J Ophthalmol. 2012;22:274–7. https://doi.org/10.5301/ejo.5000019.
Seiler T, Quurke AW. Iatrogenic keratectasia after LASIK in a case of forme fruste keratoconus. J Cataract Refract Surg. 1998;24:1007–9. http://www.ncbi.nlm.nih.gov/pubmed/9682124. Accessed 2 Feb 2017.
Arbelaez MC, Sekito MB. Screening for subclinical keratoconus. Oman J Ophthalmol. 2013;6:1–2. https://doi.org/10.4103/0974-620X.111891.
Arbelaez MC, Versaci F, Vestri G, Barboni P, Savini G. Use of a support vector machine for keratoconus and subclinical keratoconus detection by topographic and tomographic data. OPHTHA. 2012;119:2231–8. https://doi.org/10.1016/j.ophtha.2012.06.005.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Busool Abu-Eta, Y., Nemet, A., Vainer, I. et al. Outcomes of photorefractive keratectomy in patients with posterior corneal steepening. Eye 35, 2016–2023 (2021). https://doi.org/10.1038/s41433-020-01213-2
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41433-020-01213-2
This article is cited by
-
Factors associated with changes in posterior corneal surface following laser-assisted in situ keratomileusis
Graefe's Archive for Clinical and Experimental Ophthalmology (2023)
