
Abstract
Study design
A hospital-based retrospective epidemiological study.
Objective
To describe the demographic and epidemiological characteristics of patients with traumatic spinal cord injury (TSCI) in Xi’an to help health-related institutions formulate corresponding measures.
Setting
People with TSCI, all spine centres and orthopaedic centres in Xi’an, China.
Methods
We retrospectively reviewed the medical records of the all spine centers or orthopedic centers in Xi’an according to the International Classification of Disease Version 10 (ICD-10) and diagnostic code of TSCI. Variables included gender, age, medical insurance, etiology, occupation, level of injury, and severity of injury, multiple injury, complication, treatment, and so on.
Results
The study included the medical records of 1730 patients with TSCI from 2014 to 2018. The estimated annual incidence rate increased from 39.0 cases (95% CI, 34.7–43.3 cases) per 1 million persons in 2014 to 43.2 cases (95% CI, 39.0–47.5 cases) per 1 million persons in 2018. The leading cause of TSCI was high falls (35.5%, 614 cases). The most common injury site was the cervical spinal cord, accounting for 55.7% (963 cases). The degree of injury severity with the highest proportion was incomplete tetraplegia (47.2%, 816 cases). In addition, 71.4% (1236 cases) of TSCI cases had spinal fracture or dislocation.
Conclusions
There are specific epidemiological characteristics of TSCI patients in Xi’an, and preventive measures are suggested to be based on the characteristics of the different types of patients with TSCI and focused on high-risk groups.
Similar content being viewed by others
Introduction
Traumatic spinal cord injury (TSCI) is highly disabling. It places a heavy burden on individuals, families and society as a whole because of the labour loss, the need for long-term rehabilitation, the occupation of a large amount of medical resources and expensive medical costs. Developed countries in Europe and the United States have identified the epidemiological characteristics of TSCI patients through large-scale domestic investigations. Although injury prevention initiatives have attempted to reduce the occurrence of TSCI, the incidence and prevalence of TSCI have been increasing, with the annual incidence rate estimated to be 10.4–83 cases per million persons in North America and Western Europe. [1,2,3,4]
In China, studies reported an annual incidence rate of 23.7 per million persons in Tianjin [5] and 60.6 per million persons in Beijing [6]. The epidemiological characteristics of TSCI vary across regions with different economic levels and economic periods. It is of great importance to conduct such epidemiological research at the local population level. Xi’an is the city with the largest population (more than 10 million residents in 2019) and the highest-level economy in northwest China. However, at present, very little is known and has been reported about epidemiological research on TSCI in Xi’an. Therefore, our hospital-based retrospective study aimed to examine the demographics and epidemiological characteristics of patients with TSCI in Xi’an to help health-related institutions develop measures to determine the best allocation of medical resources to ease financial and social burdens.
Methods
Study design and participants
We retrospectively reviewed the medical record data of all spine centres and orthopaedic centres that qualified to treat patients with TSCI in the city from 2014 to 2018 using the International Classification of Diseases Version 10 (ICD-10) and the diagnostic code for TSCI. People who with TSCI live in Xi’an will eventually be referred to these centers due to standardized hierarchical medical system. The cases from these centres are representative of the population of Xi’an. The inclusion criteria were as follows: (1) met the diagnostic criteria for TSCI; (2) newly injured patients; (3) patients admitted to the hospital from January 1, 2014, to December 31, 2018; (4) patient often lives in Xi’an; and (5) in-hospital medical records with complete key information. The exclusion criteria were as follows: (1) patients who died before hospitalization; (2) emergency department patients who were never hospitalized; (3) referrals between hospitals only recorded the first time; and (4) patients undergoing rehabilitation or outpatient follow-up care. For any patient undergoing rehabilitation or post-acute care, we obtained the medical records from the first or major receiving hospital after the injury. The Ethics Committee of Xi’an Honghui Hospital and the ethics committee of each participating centre approved the review process and waived the requirement to obtain patients’ written informed consent. All methods were performed in accordance with the GATHER Statement guidelines.
Data collection
Questionnaires
Referring to the relevant methods of epidemiological research on TSCI globally, experts at Xi’an Honghui Hospital designed a medical record questionnaire based on methods include binary selection and multiple selection to rely on software formatting to collect the data we need. According to the rationality, scientific credibility, necessity and feasibility of the investigation project, multiple rounds of argumentation, modification and field testing were performed until the collected information sufficiently reflected the epidemiological characteristics of TSCI in Xi’an. Then, the final version of the questionnaire was created, and the corresponding database was established.
The following survey indicators were finalized: (1) general information of patients (name, age, sex, ID number, occupation, residence address, medical insurance, telephone number); (2) relevant information regarding the TSCI (date of injury, cause of injury, date of admission, injury level, severity of injury [complete and incomplete injuries, it was judged by investigators according to the description of the sensation and motor dysfunction of the limbs for the first time in the medical records of the patient at the time of admission], with spinal fracture or not); (3) multiple injuries; (4) treatment options (surgery or rehabilitation, surgical procedures and approach); (5) clinical complications over the whole length of a person’s stay [such as pneumonia, bedsores, deep venous thrombosis, etc] and (6) inpatient death and the cause of death. The patients were divided into eight age groups: ≤14, 15–24, 25–34, 35–44, 45–54, 55–64, 65–74, and ≥75-years-old. Occupations were categorized as civil servants, professional technicians, enterprise staff, workers, peasants, students, freelancers, self-employed individuals, unemployed individuals, retired individuals, and all other occupations not classified above. The aetiologies included injuries caused by traffic accidents, sports, low falls (height ≤1 m), high falls (height >1 m), and other causes. The levels of injury were divided into the cervical spinal cord, thoracic spinal cord, and lumbosacral spinal cord. A complete injury was defined as the absence of sensory and motor function in the lowest sacral segments.
Quality control
Experienced investigators were selected to participate in data collection. Relevant personnel were repeatedly trained before data collection, a manual of procedures was distributed, and detailed instructions for administration of the questionnaires and data entry were provided. In the investigation stage, two investigators were assigned to each investigation unit, and they separately extracted and verified the data and signed the questionnaire as the party responsible for the authenticity of the data. Any problems encountered by the investigators during the investigation of medical records was solved through timely discussion and consultation with experts. Strict review of the completed questionnaires and re-examination of unqualified questionnaires was performed to ensure the quality of the data entered. In the data entry phase, a double entry verification system was adopted. After all data were entered, the epidemiologist checked the database data, and the investigator traced the discovered abnormal values back to the paper questionnaire or even the original medical records to determine the source and to correct the error value generated during the data extraction process.
Statistical analysis
We used Epidata software version 3.1 (Epidata Association, Odense, Denmark) for data entry and management and Microsoft Office Excel 2019 to check and save data. Analyses were performed with SAS (version 9.1). The measurement data are expressed by absolute value and mean ± standard deviation and median, and the classification data and ranked data are expressed by absolute value, rate and composition ratio.
Results
General characteristics of patients with TSCI
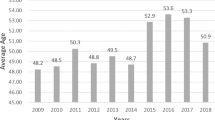
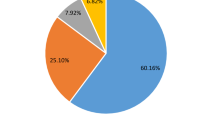
A total of 16 centers in Xi’an were investigated. The study included the medical records of 1730 patients with TSCI from 2014 to 2018; the mean (SD) age of patients was 50.1 ± 14.8 years and a median of 51 years with a male to female ratio of 2.91:1, and males accounted for 74.2%. Although the total number of ward beds in the study hospitals remained unchanged over the study period, the number of TSCI admissions increased (2014: 318, 2015: 336, 2016: 320, 2017: 357, 2018: 399). The highest proportion of TSCIs occurred in the 45–54 age group (28.2%, 487 cases), followed by the 55–65-year-old group (21.3%, 369 cases) and the 55–64-year-old age group (21.3%, 369 cases). The most common occupational groups were peasants and workers, accounting for 60.1% (1041 cases) of the total. Regarding medical insurance, 37.3% (645 cases) of all patients with TSCI had no insurance, and 31.2% (539 cases) used rural cooperative medical care insurance. The length of hospital stay ranged between 1 and 234 days, with a mean length of 17.9 ± 16.6 days and a median of 14 days. The general characteristics are shown in Table 1.
Incidence of TSCI
As shown in Table 2, the estimated annual incidence rate was 39.0 cases [95% CI (Confidence interval), 34.7–43.3 cases] per 1 million persons in 2014 and 43.2 cases (95% CI, 39.0–47.5 cases) per 1 million persons in 2018, with an annual average of 41.0 cases (95% CI, 36.6–45.3 cases) per 1 million persons. The overall crude incidence rates of TSCI were 59.5 (95% CI, 52.2–66.8) and 21.5 (95% CI, 17.0–26.0) per million persons (on average per year) for males and females, respectively. Age-stratified incidence rates showed an increasing trend in the 15–64-year-old age groups among the male population (for instance, an increase from an estimated 58.8 (95% CI, 40.6–77.1 cases) cases/million persons in 2014 to 87.0 (95% CI, 64.8–109.2 cases) cases/million persons in 2018 for the 35–44-year-old age group) and a decreasing trend in the ≥35-year-old age groups among the female population (for instance, a decrease from an estimated 44.3 (95% CI, 27.9–60.6 cases) cases/million persons in 2014 to 20.2 (95% CI, 10.3-30.1 cases) cases/million persons in 2018 for the 45–54-year-old age group). For the overall population, a high rate of decrease in TSCI incidence from 2014 to 2018 was observed in elderly persons (≥65 age groups) (for instance, from 89.6 (95% CI, 63.7–115.4 cases) cases/million persons to 62.3 (95% CI, 44.1–80.5 cases) cases/million persons in the 65–74-year-old age group). Age- and sex-stratified numbers of cases and estimated incidence rates and the population estimates used to calculate incidence rate are provided in the Supplementary online resources.
Aetiology of the injuries
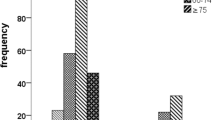
As shown in Fig. 1a, the leading causes of TSCI in Xi’an are high falls (35.5%, 614 cases), traffic accidents (26.6%, 461 cases) and low falls (26.7%, 462 cases). Observing the distribution of the causes of injury (Fig. 1b), we found that in the 15–24-year-old age group, the highest cause was high falls (54.8%, 40 cases), which tended to decrease with increased age. The proportion in the ≥75-year-old age group reached 21.5% (14 cases). The proportion of low falls in the 15–24-year-old age group was 12.3% (9 cases), and the proportion increased with age and reached 50.8% (33 cases) (≥75-year-old age group). The leading cause of injury in patients with incomplete tetraplegia was traffic injury (33.2%, 271 cases), and the leading cause of injury in the remaining group was still high falls (Fig. 1c). The leading cause of injury in patients with injury levels in the cervical spinal cord was traffic accidents (32.3%, 311 cases); in patients with injury levels in the thoracic spinal cord and lumbosacral spinal cord, the leading cause was high falls (47.3% and 50.0%, respectively) (Fig. 1d).

a Bar graph of aetiology for TSCI patients; b distribution of aetiology for TSCI patients by age group, c severity of injury, and d injury level.
Injury level
The most common injury that patients with TSCI suffered was cervical spinal cord injury (SCI) (963 cases), which accounted for 55.7% of all cases, followed by thoracic and lumbar injuries (241 and 526 cases, respectively) (Fig. 2a). There was a tendency for the proportion of cervical SCI to increase with age, and the proportion in the ≥75-year-old age group (73.8%, 45 cases) was the highest. The proportion of lumbosacral SCIs decreased with increasing age and was only 15.4% (ten cases) in the ≥75-year-old age group (Fig. 2b).

a Bar graph of injury level for TSCI patients; b distribution of injury level for TSCI patients by age group.
Severity of injury
The degree of injury severity with the highest proportion in the included TSCI patients was incomplete tetraplegia (47.2%, 816 cases), followed by incomplete paraplegia (30.9%). The proportion of complete injuries (21.8%) was as follows: 8.6% in the cervical spine, 7.2% in the thoracic spinal region, and 6.2% in the lumbar spine.
Level and type of fracture
A total of 71.4% (1236 cases) of TSCI cases had spinal fractures or dislocations. The most common level of fracture that patients with TSCI suffered was cervical (37.1%, 515 cases), followed by lumbosacral and thoracic (34.7% and 28.2%, respectively). The proportion of TSCIs combined with cervical vertebrae fractures in all age groups gradually increased with age, up to 53.3% (≥75-year-old age group), while the proportion of lumbosacral vertebrae fractures gradually decreased with increasing age, with the lowest proportion being 20.0% (≥75-year-old age group) (Fig. 3a). In the cervical spine, the C5 (7.9%, 161 cases) and C6 (10.4%, 211 cases) vertebral bodies were more commonly combined with fractures, and the major fracture type was dislocation. T12 (9.6%, 195 cases) had the highest proportion of fractures in the thoracic spine, and burst fractures were the main fracture type. In the lumbar spine, L1 (14.7%, 299 cases) and L2 (8.1%, 164 cases) were easily combined with fractures, and the fracture type was mainly burst fracture (Fig. 3b).

a Distribution of fracture level for TSCI patients by age group and (b) by type of fracture.
Multiple injuries
With regard to multiple injuries, injuries to the chest (37.6%, 514 cases) accounted for the highest proportion among all TSCI patients, followed by those to the head (33.7%, 460 cases) and limbs (18.8%, 257 cases) (Online Resource 5.3 Fig. 4A). Although there were insufficient data in the ≥75-year-old age group, the distribution of multiple head injuries in the rest of the age groups showed a trend of increasing with age, up to 44.3% (65–74-year-old age group). Multiple limb and pelvic injuries showed a tendency to decrease with increasing age (Online Resource 5.3 Fig. 4B). The distribution of multiple injuries for different causes of injury was also different. The leading site for multiple injuries caused by traffic accidents and low falls was the head (38.2% and 47.1%, respectively). However, in patients experiencing high falls, the site was the head (40.4%) (Online Resource 5.3 Fig. 4C).
Clinical complications
A total of 24.7% (427 cases) of patients with TSCI experienced clinical complications, of which 28.2% (211 cases) had respiratory complications, electrolyte disorders (17.7%, 132 cases) and venous thrombosis (15.1%, 113 cases) (Online Resource 6.3 Fig. 5A). The main clinical complication of injuries at the cervical and thoracic levels was still respiratory distress (31.2% and 31.4%, respectively); however, for injuries at the lumbosacral level, the main complication was venous thrombosis (23.2%) (Online Resource 6.3 Fig. 5B).
Treatment options
A total of 1274 (73.6%) patients underwent surgical treatment, and the main surgical procedure was decompression, fixation and bone graft fusion, occurring in a total of 993 (77.9%) patients (Table 3). Regarding the surgical approach, 381 (29.9%) patients underwent anterior surgery, and 846 (66.4%) patients underwent posterior surgery. A total of 511 (29.5%) patients underwent inpatient rehabilitation.
Death and the cause of death
Thirteen (0.75%) patients died during hospitalization, and the oldest was 89 years old. Of these 13 patients, 76.9% (10 cases) died from respiratory failure. The injury level of 11 (84.6%) dead patients was in the cervical spinal cord, 6 (46.2%) dead patients had experienced high falls, and 5 (38.5%) dead patients had been in traffic accidents.
Discussion
Although many epidemiological articles on TSCI have been published, the advantage of our research is that it is more useful to a more local audience as the main area of difference is in how local factors affect the previously documented epidemiology. To our knowledge, the current study is the first hospital-based retrospective study on TSCI in Xi’an city.
We found that the average age of Xi’an TSCI patients (50.1 ± 14.8) was higher than the global average age of TSCI patients (33 years) [7], which was also higher than the average age of Chinese TSCI patients reported in a previous review [8]. Previous studies have shown that the age of patients with TSCI has a bimodal distribution [9,10,11]; however, this study had a unimodal distribution for age. Most of the injuries were in the 45–54-year-old age group (28.2%, 487 cases), followed by the 55–64-year-old age group (21.3%, 369 cases), which shows that adults are still the main population that has TSCI. We also found that men in Xi’an have a higher risk of suffering from TSCI than women (2.91:1). This is in accordance with a previous study on TSCI conducted in Chongqing [12]. According to other countries’ data, for patients with TSCI, the ratio of males to females was 2.3–2.8:1 in the United States from 1993 to 2012 [3]; in Australia, the ratio from 2002 to 2012 was ~1.5–2.4:1. The main reason is that most women are housewives with low-risk occupations, but men are more likely to engage in high-risk work outdoors [9, 10]. The imbalance between men and women in China may be one of the factors that make the male-female ratio slightly higher than that in other countries.
Moreover, this study revealed that the main aetiologies of TSCI in Xi’an included high falls (35.5%, 614 cases), traffic accidents (26.6%, 461 cases), and low falls (26.7%, 462 cases). A 2011 report from Tianjin [5], a 2017 report from Guangdong [13], and the present study all found that high falls were the leading cause in most cities of China. High falls mainly occur at construction sites, and the Chinese government has increased economic support for the northwestern region in recent years and vigorously pursued infrastructure construction. The construction unit needs to strengthen the individual’s awareness of safety and security, focus on monitoring the safety and quality of production, and provide a safe working environment. Low falls are an important cause of TSCI in Xi’an, and a tendency for them to increase with increased age means that low-energy injuries mainly occur in elderly individuals. Therefore, fall prevention in older people needs more attention than prevention measures for other risk factors. The main cause of injury in patients with incomplete tetraplegia was traffic injury (33.2%, 271 cases), followed by low falls (32.1%, 262 cases). Previous investigations have reported that cervical SCI is most likely to occur when suffering a whiplash injury to one’s neck during a traffic accident or when an elderly person falls, and most cases are incomplete tetraplegia [14]. Our findings that the main cause of injury in patients with cervical SCI was traffic injury (32.3%, 311 cases), followed by low falls (32.1%, 309 cases), demonstrate this.
Cervical injuries were most common, which accounted for 48.7% (963 cases) of the total cases, which is in accordance with a previous study [9, 15, 16]. We found that the proportion of persons with cervical SCI increased significantly with age. The possible reason for this outcome is that degeneration and hyperplasia of the cervical vertebrae are obvious with increasing age. Cervical spinal canal stenosis is caused by disc herniation and ossification of the ligamentum flavum, and the volume of the spinal canal available for compensation is significantly reduced during trauma; thus, even low-energy trauma, such as a low fall, can easily cause damage to the spinal cord. We also found that the proportion of low falls continues to increase with age.
Traumatic spinal cord injury with spinal fracture is more common than without fracture. The C5 and C6 vertebrae were more common in cervical spinal fracture, and the L1 and L2 vertebrae were more common in lumbar spinal fracture, showing a bimodal distribution. This finding is consistent with previous research conclusions [12, 17], but we further studied the types of fractures and found that the most common fracture form of C5 and C6 vertebrae was dislocation and that the fracture types of T12 vertebrae and L1 and L2 vertebrae were mainly burst fractures. We found that the proportion of TSCIs with cervical spine fractures increased with age, and the proportion of lumbosacral fractures decreased with increasing age. This may be because with increasing age, people’s bones gradually become looser, and they are slow-moving, have decreased vision, slow protective responses, etc., which makes it easier to fall. A large number of studies have confirmed that low falls are the most common cause of cervical fractures in elderly patients [18], and in our study, the rising proportion of falls that cause injury with age better explains the above situation. Previous studies have confirmed that fractures in elderly persons mainly occur in the thoracolumbar region, mostly due to osteoporosis combined with low-energy injury. The type of injury is mainly compression and rarely causes damage to the thoracolumbar spinal cord [19]. Therefore, burst fractures of the thoracolumbar spine caused by high energy damage are relatively rare in elderly patients.
In this study, multiple injuries were more common in the chest, but previous research has shown that the main multiple injury site is the head and that the main cause of injury is traffic accidents [11, 20]. Our research also found that high falls are most likely to cause chest injuries, and traffic accidents and low falls are most likely to be involve head injuries. The current results demonstrated that 24.7% (427 cases) of patients with TSCI experienced clinical complications, and the three main complications were respiratory complications (28.2%, 211 cases), electrolyte disorders (17.7%, 132 cases) and venous thrombosis (15.1%, 113 cases). Respiratory complications such as pulmonary infections are the most common complication in TSCI. This finding has become a common consensus.
We found that 1274 (73.6%) patients underwent surgical treatment. The mainstream surgical approach involves decompression, fixation and bone graft fusion. The posterior approach is more common than the anterior approach. Only minority of the TSCI patients (29.5%) received rehabilitation, the following possible reasons were summarized: (1) Medical resources for post-traumatic rehabilitation in Xi’an are still relatively scarce, and only some large trauma centers have rehabilitation departments. (2) Doctors pay more attention to the surgical treatment of spinal cord injury than to rehabilitation. (3) The concept of rehabilitation is relatively backward, still dominated by the concept of rehabilitation of traditional Chinese medicine, with little effect. (4) The surgical treatment of spinal cord injury is expensive, and the heavy economic burden makes patients have to give up rehabilitation treatment. We hope that the Xi’an government will increase its investment in the construction of the system of rehabilitation and attract more professional rehabilitation professionals to improve the current predicament.
In all of the patients included in this study, only 13 patients (0.75%) had in-hospital deaths, with a mean length of 17.8 ± 17.2 days and a median of 14 days, which was significantly lower than the US-reported average in-hospital mortality rate of 7.5% in 2010–2012 [3]. We consider that the death data of this study are heavily influenced by traditional Chinese concepts. For example, for patients with severe TSCI who need to be maintained by a ventilator, family members who choose to give up treatment due to economic burden will maintain the patient’s vital signs until they return home. Outcomes regarding the main causes of death, main causes of injury, and major injury levels for patients who died in-hospital were the same as those in previous studies [20,21,22].
There are some limitations in this study. First, similar to previous studies, our research did not take into account those who died at the scene of the injury or in the emergency department; therefore, the incidence of TSCI may be underestimated. We lost some information because many complications and treatments were not fully diagnosed or recorded in the medical records. This study was a hospital-based descriptive study about TSCI.
The epidemiological characteristics of TSCI described in this study are somewhat different from those described in other countries. High falls were the main cause, and the mean age of patients with TSCI was older than that in other countries. The most frequently reported high-risk occupations in patients with TSCI were peasant and worker. Adult males are still a high-risk group for TSCI. We advocate instituting appropriate preventive policies and taking appropriate measures according to the characteristics of different types of TSCI patients, especially for high-risk groups.
Data availability
The datasets (individual participant level data) generated during and/or analysed during the current study are not publicly available due personal privacy (such as patient name, ID number, home address, telephone number) but are available from the corresponding author on reasonable request. Partial data analysed during this study are included in this published article (and its Supplementary Information files).
References
Lee BB, Cripps RA, Fitzharris M, Wing PC. The global map for traumatic spinal cord injury epidemiology: update 2011, global incidence rate. Spinal Cord. 2014;52:110–6.
Kattail D, Furlan JC, Fehlings MG. Epidemiology and clinical outcomes of acute spine trauma and spinal cord injury: experience from a specialized spine trauma center in Canada in comparison with a large national registry. J Trauma Acute Care Surg. 2009;67:936–43.
Jain NB, Ayers GD, Peterson EN, Harris MB, Leslie M, O'Connor KC, et al. Traumatic spinal cord injury in the United States, 1993–2012. Jama 2015;313:2236–43.
Koskinen EA, Alen M, Väärälä EM, Rellman J, Kallinen M, Vainionpää A. Centralized spinal cord injury care in Finland: unveiling the hidden incidence of traumatic injuries. Spinal Cord. 2014;52:779–84.
Ning G-Z, Yu T-Q, Feng S-Q, Zhou X-H, Ban D-X, Liu Y, et al. Epidemiology of traumatic spinal cord injury in Tianjin, China. Spinal Cord. 2011;49:386–90.
Li J, Liu G, Zheng Y, Hao C, Zhang Y, Wei B, et al. The epidemiological survey of acute traumatic spinal cord injury (ATSCI) of 2002 in Beijing municipality. Spinal Cord. 2011;49:777–82.
Wyndaele M, Wyndaele JJ. Incidence, prevalence and epidemiology of spinal cord injury: what learns a worldwide literature survey? Spinal Cord. 2006;44:523–9. https://doi.org/10.1038/sj.sc.3101893
Chen X, Chen D, Chen C, Wang K, Tang L, Yuzhe Li, et al. The epidemiology and disease burden of traumatic spinal cord injury in China: a systematic review. Chi J Evid Based Med. 2018;18:143–50.
Majdan M, Brazinova A, Mauritz W. Epidemiology of traumatic spinal cord injuries in Austria 2002–2012. Eur Spine J. 2016;25:62–73.
Kang Y, Ding H, Zhou HX, Wei ZJ, Liu L, Pan DY, et al. Epidemiology of worldwide spinal cord injury: a literature review. J Neuroresstoratology. 2018;6:1–9. https://doi.org/10.2147/jn.s143236
Pérez K, Novoa AM, Santamariña-Rubio E, Narvaez Y, Arrufat V, Borrell C, et al. Incidence trends of traumatic spinal cord injury and traumatic brain injury in Spain, 2000–2009. Accid Anal Prev. 2012;46:37–44.
Ning GZ, Mu ZP, Shangguan L, Tang Y, Li CQ, Zhang ZF, et al. Epidemiological features of traumatic spinal cord injury in Chongqing, China. J Am Paraplegia Soc. 2015;39:455–60.
Yang R, Guo L, Huang L, Wang P, Tang Y, Ye J, et al. Epidemiological characteristics of traumatic spinal cord injury in Guangdong, China. Spine 2016;42:E555–E561.
Wang H, Xiang Q, Li C, Zhou Y. Epidemiology of traumatic cervical spinal fractures and risk factors for traumatic cervical spinal cord injury in China. J Spinal Disord Tech. 2013;26:E306–E313.
Ning GZ, Qiang W, Li YL, Feng SQ. Epidemiology of traumatic spinal cord injury in Asia: a systematic review. J Spinal Cord Med. 2012;35:229–39.
Pickett GE, Campos-Benitez M, Keller JL, Duggal N. Epidemiology of traumatic spinal cord injury in Canada. Spine 2006;31:799–805.
Taşoğlu Ö, Koyuncu E, Daylak R, Karacif DY, I˙Nce Z, Yenigün D, et al. Demographic and clinical characteristics of persons with spinal cord injury in Turkey: One-year experience of a primary referral rehabilitation center. J Spinal Cord Med. 2018;41:157–64.
Bub LD, C Craig B, Mann FA, Lomoschitz FM. Cervical spine fractures in patients 65 years and older: a clinical prediction rule for blunt trauma. Radiology. 2005;234:143–9.
Leucht P, Fischer K, Muhr G, Mueller EJ. Epidemiology of traumatic spine fractures. Injury. 2009;40:166–72.
Cynthia T, Jennifer M, Stefan P, Jean-Marc MT. The changing demographics of traumatic spinal cord injury: An 11-year study of 831 patients. J Am Paraplegia Soc. 2014;38:214–23.
Chamberlain JD, Meier S, Mader L, von Groote PM, Brinkhof MWG. Mortality and longevity after a spinal cord injury: systematic review and meta-analysis. Neuroepidemiology 2015;44:182–98. https://doi.org/10.1159/000382079
Derrett S, Beaver C, Sullivan MJ, Herbison GP, Acland R, Paul C. Traumatic and non-traumatic spinal cord impairment in New Zealand: incidence and characteristics of people admitted to spinal units. Inj Prev. 2012;18:343–6. https://doi.org/10.1136/injuryprev-2011-040266
Acknowledgements
We are very grateful to Professor Xiao Qi, an epidemiologist, for providing statistical support for this study.
Funding
This study was supported by the Xi’an Municipal Health Committee (2020yb34), the Science and Technology Commission of Shaanxi (2020SF-187), the Science and Technology Commission of Shaanxi (2018HJCG-08), the National Natural Science Funds (81830077) and the Science and Technology Commission of Xi’an (20YXYJ0011(3)).
Author information
Authors and Affiliations
Contributions
LY and JD reviewed and analysed the data. DH, JD and LY obtained funds and conceived and designed the study. QT, ZZ, YW, HL, YC, CJ, and LB collected the data. DH, BH and LY participated in the critical revision of the manuscript. JD drafted the paper.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
The Ethics Committee of Xi’an Honghui Hospital and the ethics committee of each participating centre approved the review process and waived the requirement to obtain patients’ written informed consent.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
About this article

Cite this article
Du, J., Hao, D., He, B. et al. Epidemiological characteristics of traumatic spinal cord injury in Xi’an, China. Spinal Cord 59, 804–813 (2021). https://doi.org/10.1038/s41393-020-00592-3
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41393-020-00592-3
This article is cited by
-
The impact of COVID-19 and associated lockdowns on traumatic spinal cord injury incidence: a population based study
Spinal Cord (2024)
-
Incidence, prevalence and disability of spinal cord injury in China from 1990 to 2019: a systematic analysis of the Global Burden of Disease Study 2019
European Spine Journal (2023)
