
Abstract
Workers in the electroplating industry are potentially exposed to a range of hazardous substances including nickel and hexavalent chromium (chromium VI) compounds. These can cause serious health effects, including cancer, asthma and dermatitis. This research aimed to investigate whether repeat biological monitoring (BM) over time could drive sustainable improvements in exposure control in the industry. BM was performed on multiple occasions over 3 years, at 53 electroplating companies in Great Britain. Surface and dermal contamination was also measured, and controls were assessed. Air monitoring was undertaken on repeat visits where previous BM results were of concern. There were significant reductions in urinary nickel and chromium levels over the lifetime of this work in the subset of companies where initially, control deficiencies were more significant. Increased risk awareness following provision of direct feedback to individual workers and targeted advice to companies is likely to have contributed to these reductions. This study has shown that exposures to chromium VI and nickel in the electroplating industry occur via a combination of inhalation, dermal and ingestion routes. Surface contamination found in areas such as canteens highlights the potential for transferral from work areas, and the importance of a regular cleaning regime.
Similar content being viewed by others

INTRODUCTION
Workers in the electroplating industry are potentially exposed to a range of hazardous substances including nickel (Ni) (Ni sulphate and chloride) and hexavalent chromium (chrome VI, Cr VI, chromium trioxide) compounds. These compounds can cause serious health effects, including cancer, asthma and dermatitis.1
Chromium VI is included in the revised Annex XIV to the REACH Regulations. REACH is an European Union regulation concerning the Registration, Evaluation, Authorisation and restriction of Chemicals. Inclusion in this Annex means that in order to continue to use chromium trioxide and other hexavalent chromium compounds after 21 September 2017, an authorisation will be required.2 There are practical problems implementing the substitution of hexavalent chromium (as well as nickel) in some processes used in the electroplating industry. As full process containment is not always practicable, there is consequently a reliance on good working practices, engineering controls and personal protective equipment (PPE) to control worker exposures. A high degree of risk awareness among workers is important in achieving control of exposure.
The principal aim of this research was to investigate whether repeat biological monitoring (BM) over a period of time could be used to drive sustainable improvements in exposure control in the electroplating industry.
BM captures total exposure by all routes,3 and can provide a valuable tool for occupational exposure assessment. BM has demonstrated significant variations in exposure for workers handling 4,4’-methylene-bis-ortho-chloroaniline (MbOCA) performing almost identical work in the same workplace.4, 5, 6 This indicates the pronounced effect that individual working practices can have on exposure. BM provides a feedback loop to workers and managers, and can be used to demonstrate risk reduction by tracking successive results as control improves and exposure reduces. The provision of direct one-to-one feedback of results to individual workers increases risk awareness and supports a culture of good practice to avoid unnecessary exposure.
Soluble chromium and nickel compounds are particularly amenable to exposure assessment using BM.7 Following exposure, the excretion of absorbed chromium and nickel compounds occurs mostly via urine. Urinary levels of chromium and nickel usually reflect recent occupational exposure, and the relatively short initial half-lives allow the effect of improved exposure controls to be quantified in a relatively short time period. Typically, following exposure, chromium is thought to exhibit a tri-phasic half-life with the elimination half-lives of 7 h, 15–30 days and 3–5 years; however, depending on the route of exposure, reported half-lives differ. The elimination of nickel is also dependent on the exposure route and the species of nickel. An initial half-life of at least 17 h (though up to 96 h have been reported8) is thought to be followed by a longer half-life of several weeks. A urinary elimination half-life (for absorbed nickel) of 17–48 h has been reported in a human oral exposure study.9
It is not possible to differentiate between hexavalent and trivalent chromium in urine,10 as once absorbed in the body, chromium compounds are found only in the trivalent form.11 Once absorbed into the bloodstream, hexavalent chromium is rapidly taken up by erythrocytes after absorption and reduced to trivalent chromium inside the red blood cells.
In addition to chromium and nickel, a range of other hazardous substances are handled in the electroplating industry. Some of these, such as cadmium (Cd) compounds and mineral acid (mists), can have serious chronic health effects. Others, such as cyanide compounds, are acutely toxic; however, none of these lend themselves to BM as readily as chromium and nickel. Cadmium, for example, has a half-life in the body of 10–30 years, and body burden increases with age. This makes interpretation of results difficult in an occupational context.
Relevant occupational exposure limits and biological monitoring guidance values (BMGV) are presented in Tables 1 and 2.10, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21
METHODS
Site Work
The research was carried out in collaboration with the Surface Engineering Association (SEA). The SEA has published guidance documents on controlling chromium and nickel exposures, in conjunction with the Health and Safety Executive (HSE).22, 23, 24, 25, 26, 27 Fifty-three sites were visited in GB between 2008 and 2011, the majority of which were SEA members. Sites visited were small to medium sized enterprises, with numbers of employees potentially exposed to chromium and/or nickel ranging between 5 and 40.
Initial Site Visits
The electroplating processes were the main area of interest for this work; however, other processes with exposure potential, such as preparatory work (involving chromium and nickel), maintenance activities, polishing of electroplated items, and ancillary tasks, were also studied. Processes included hard and decorative chrome plating, chrome passivation, chromic anodising, and electrolytic and electroless nickel plating.
During each site visit, information was obtained on relevant work tasks and their associated exposure controls. This included:
-
Management controls (risk assessments, operating procedures, operator training);
-
Engineering controls (containment, local exhaust ventilation (LEV) and general ventilation);
-
PPE programmes;
-
Individual working practices; and
-
Other relevant issues (e.g., use of surfactant in chromium VI tanks).
An assessment of the efficacy of control measures was undertaken, and comprehensive feedback provided to each company.
Biological monitoring
During the initial site visit, workers with exposure potential were invited to take part in the BM programme. At company level, participation rates were greater than 95%, and at individual level within companies, participation rates were 80–90%. Reasons for non-participation were not investigated. The BM programme was conducted in accordance with good practice described in guidance document HSG1673 with written informed consent obtained from individual participants.
Participants undertaking relevant activities undertook BM by providing a single post-shift urine sample on three consecutive working days. Samples were provided using the on-site welfare facilities, into 30 ml polystyrene urine screw-top collection bottles (Sterilin, Newport, UK). Participants were instructed to wash their hands before provision of the sample to minimise the potential for sample contamination.
Participants sealed individual sample bottles inside larger (opaque) bottles. Each participant completed a form for each sample. Details of the work undertaken, along with PPE and respiratory protective equipment (RPE) worn were noted on the form. Each bag, containing the sample and submission form, was posted direct to the laboratory, or on occasions where samples were provided on the same day as the site visit, taken directly to the laboratory by the occupational hygienist undertaking the work.
The samples were analysed for creatinine upon receipt at the laboratory and then stored in a refrigerator until metal analysis was undertaken, normally within 10 working days. Creatinine was determined by an automated alkaline picrate method,28 using an ABX Pentra 400 spectrophotometer (HORIBA ABX UK, Northampton, UK). If time before analysis was anticipated to be greater than 10 days, the samples were frozen. Urine samples were brought to room temperature and mixed on a rotary mixer for a minimum of 20 min. All urine samples and quality control (ClinChek and Bio-Rad) samples were diluted 1 in 20 with an acid diluent. Samples were analysed by inductively coupled plasma-mass spectrometry (ICP-MS) using standard UKAS accredited laboratory methods. The quality control samples were urine-certified reference materials ClinChek Levels 1 and 2 (lot 923 Recipe, Germany) and Lypocheck, urine metals Level 1 (lot 69131 Bio-Rad Laboratories, Hemel Hempstead, UK). All results were within the certified ranges. Based on the overall performance of the certified reference material used as quality control, the measurement uncertainties for chromium were 6.9% at a mean concentration of 9.8 μg/l (n=40) and 4.7% at a mean concentration of 4.7 μg/l (n=180). For nickel, the measurement uncertainties were 5.7% at a mean concentration of 6.1 μg/l (n=85) and 3.4% at a mean concentration of 44.1 μg/l (n=213). These methods are validated by the successful participation in external quality assurance schemes in both the UK (TEQAS) and Germany (GEQUAS).
Additional BM samples were requested approximately 6 and 12 months after feedback had been provided from the initial visit. The repeat exercises tracked exposures over time and assessed the impact of any changes triggered by the initial visit. As with the initial BM exercise, a single post-shift sample was provided on three consecutive working days from the same workers who participated in the initial exercise. The sampling and analysis methodologies were the same as for the initial site visit.
Participants, with a few exceptions (reasons not investigated), provided nine samples over the course of the work, three at the initial site visit, three at 6 months and three at 12 months.
For the 6- and 12-month follow-on exercises, information was requested from each company on actions taken to implement recommendations and any other relevant changes to processes, procedures and control measures since the initial visit.
Comprehensive feedback was provided to all individual participants via a nominated site contact for all BM exercises.
Hand contamination
In many occupational settings, worker hands typically receive the highest level of dermal contamination29 and are most important in terms of transfer of contamination to the mouth.30 Hence, dermal exposure assessment for the project focussed on determining hand contamination.
Various methodologies exist to assess dermal exposure, including the use of tracer chemicals, wipe sampling (of the hands), the use of sampling gloves and handwashing.31, 32, 33 There are limitations on all of these methodologies;31, 34 and hence, the results should be viewed as semi-quantitative only. The measurement of skin contamination is however, still a useful tool in identifying exposure routes.
For this work, skin contamination was measured by hand wash sampling. Only workers who provided BM samples were invited to take part in this exercise. For each sample, the worker’s hand was placed in a polythene bag containing 200 ml of deionised water, and agitated around the hand and wrist area for approximately 30 s. Approximately 20 ml of the resulting solution was decanted into a sample bottle. Left and right hands were sampled separately, and results added together to determine “total” hand contamination. Where possible, samples were taken after a sustained period of work, typically before the main meal break or immediately before the end of the work shift. Workers were asked not to wash their hands before the sampling was performed.
Samples were analysed by inductively coupled plasma-atomic emission spectrometry (ICP-AES).
Surface contamination
An assessment of surface contamination was made in various locations around each site on the initial visit. Ghost WipesTM were used together with, where possible, a 100 mm × 100 mm template, so that a known area could be wiped. For areas where the template could not be used, the area wiped was estimated.35, 36, 37, 38, 39, 40
The locations where wipe sampling was conducted were divided into notionally “clean” areas (canteens, offices, welfare facilities, etc.) and production areas. In general, wipe sampling was conducted where there was the potential for transfer of contamination onto workers skin. Locations commonly sampled included:
-
Production areas
-
Handrails
-
Control panels
-
Workbenches
-
Tool handles
-
-
Clean areas
-
Canteen table surfaces
-
Canteen equipment—microwave controls, tap handles, kettles, interior of food fridges, drinking cups
-
Washroom taps
-
Clean lockers
-
Samples were taken at further locations if they were suspected of being exposure sources. Samples were analysed by ICP-AES.
Air monitoring
Air sampling was not undertaken on initial site visits.
Site Revisits
A proportion of sites were revisited if there were particular concerns, for example, where elevated BM results had been recorded, or if specific tasks were undertaken with the potential for increased airborne contaminants. A more detailed and focussed measurement programme of wipe sampling and/or handwashing was undertaken if dermal exposure was suspected as being significant. If inhalation exposure was thought to be of concern, then air sampling was also conducted.
Air sampling
Air sampling focussed on personal monitoring with samplers mounted in the workers breathing zone. Sampling was conducted to ascertain full shift exposures, and was conducted in accordance with the good practice set out in guidance document HSG173,41 and GB sampling methodology Methods for the Determination of Hazardous Substances (MDHS) 14/3.42 Sampling durations were typically in excess of half the working shift. Where full shift samples were not taken, it was ascertained that the remainder of the shift was similar to that of the monitored period. Samples were taken onto filters mounted in stainless steel cassettes in IOM heads and aspirated at 2 l/min. Table 3 presents the analytical methodology details for the various compounds measured.
Only workers who provided BM samples were invited to take part in this exercise.
Statistical Analysis
For the purposes of statistical analysis, site visits were coded, and workers categorised as being directly or indirectly exposed. Directly exposed workers included:
-
Electroplaters;
-
Workers jigging and carrying out other preparatory work;
-
Site chemists (includes tank sampling and making bulk chemical additions);
-
Maintenance operatives;
-
Polishers.
Other workers who participated in the BM survey, but were not working on a task listed above, were classified as indirectly exposed.
Site visit codes were as follows:
-
Visit 0—initial visit;
-
Visit 1—first revisit;
-
Visit 2—second revisit;
-
Visit 3—6-month follow-on;
-
Visit 4—12-month follow-on;
-
Visit 5—other follow-on.
The BM results were assumed to follow a lognormal distribution, which is typical for occupational exposure data.43, 44, 45 Figure 1 shows an example of how the nickel BM data obtained for this work fits into a lognormal distribution.

Summary of urinary nickel results with fitted lognormal distribution curve.
As several urine samples were collected from workers at various times over the lifetime of the project, a mixed-effect analysis (where statistical models containing both fixed and random effects are fitted) was performed. These include random-effect terms and are appropriate for representing dependent data where observations are taken on related individuals, or over time on the same individual. Correlations between measurements on individuals within the same company were modelled by introducing company effects that were assumed to be random. Correlations between measurements made over time on a worker were modelled by introducing worker effects that were also assumed to be random.
The mixed-effect model was specified on the log scale and was of the form:

where Yijk is the kth observation for the jth worker in the ith company, μ is the mean term, xijkm are the independent variables with associated parameter βm, ci is the random effect for company i, wij is the random effect for the jth worker in the ith company; ɛijk are the normally distributed residual errors.
The βm terms are corrections to the mean (μ) and measure consistent differences in variables such as visit type. In the models for the BM data, the independent variable is the visit type, treated as a factor with six levels associated with each of the six visit codes. By doing so, any significant differences in urinary concentration at subsequent visits can be identified and quantified.
RESULTS
Biological Monitoring
At the majority of sites, there was a combination of different electroplating processes, and workers usually multitasked during a shift. For this reason, it was not possible to assign workers to specific work activities. Statistical analysis was undertaken on all chromium BM results combined, and on all nickel BM results combined.
Most sites were found to be controlling exposure to an adequate standard; this was reflected in the BM results. There was some scope for improvement at these sites, but opportunities to make significant exposure reductions were limited. The summary BM data are presented in Tables 4 and 5.
A subset of 15 companies was identified where the median urinary nickel concentration at the initial visit was above the background level of 10 μmol/mol creatinine. The control deficiencies at these companies were generally more significant; hence, there was more scope for improvement. Control deficiencies included inadequate provision of LEV, over reliance on PPE (including a poor management programme), and poor housekeeping. At these sites, over the lifetime of this project, the BM data for subsets of directly exposed workers revealed:
-
A reduction of 33% (95% CI [13%, 48%]) in urinary nickel for nickel electroplaters; and
-
A reduction of 38% ([95% CI [17%, 54%]) in urinary nickel for other (directly exposed) nickel workers.
Taking a similar approach, a subset of 13 companies was identified where the median urinary chromium concentration at the first visit was above the background level of 3 μmol/mol creatinine. At these sites, over the lifetime of this project, the BM data for subsets of directly exposed workers revealed:
-
A reduction of 23% ([95% CI [6%, 37%]) in urinary chromium for chromium electroplaters; and
-
A reduction of 27% ([95% CI [8%, 43%]) in urinary chromium for all other (directly exposed) chromium workers+.
Note+—BM samples for non-electroplaters were obtained at only 10 of the 13 companies considered for this analysis.
This analysis clearly shows that urinary nickel and chromium levels reduced over the lifetime of the project at companies with the highest exposures at the outset, with exposures better controlled by the end of the research. Many of the changes made at these sites focussed on reducing dermal exposure through improved working methods and housekeeping, supported by well-managed PPE programmes. The measurement results allowed specific problem areas to be targeted at these sites, and provided persuasive evidence to convince some sites to take action.
Hand Contamination
Summary data from the hand wash sampling are presented in Table 6. Statistical analysis shows:
-
A moderate positive correlation between urinary nickel and hand contamination for all directly exposed nickel workers (correlation co-efficient 0.45, P-value (P) <0.0001);
-
A moderate positive correlation between urinary nickel and hand contamination for the subset of nickel electroplaters; (correlation co-efficient 0.43, P<0.0001);
-
A weak positive correlation between urinary nickel and hand contamination for the subset of indirectly exposed nickel workers (correlation co-efficient 0.34, P<0.05);
-
A moderate positive correlation between urinary chromium and hand contamination for all directly exposed chromium workers (correlation co-efficient 0.63, P<0.0001);
-
A strong positive correlation between urinary chromium and hand contamination for the subset of chromium electroplaters (correlation co-efficient 0.71, P<0.0001); and
-
A weak positive correlation between urinary chromium and hand contamination for the subset of indirectly exposed chromium workers (correlation co-efficient 0.13, P=0.49).
The positive correlations between hand contamination and BM results confirm that dermal exposure is significant in terms of contribution to overall systemic dose. This supports observations made during the site visits.
Surface Contamination
Summary data from the surface wipe sampling are presented in Table 7. The measurements show significantly higher contamination in production areas than in “clean” areas ((total) nickel P<0.0001, soluble nickel P<0.0001, chromium P<0.0001).
Although not a direct measure of exposure, surface wipe sampling provides an indication of the potential for dermal exposure. It is unrealistic to expect no measurable surface contamination in production areas; however, these results illustrate the need for good practices to minimise spillage and splashing.
The results of the wipe sampling are more pertinent in “clean” areas, such as canteens.
Statistical analysis revealed:
-
Production areas
-
A moderate positive correlation between surface contamination and hand wash measurements for nickel (correlation co-efficient 0.55, P<0.001); and
-
A weak positive correlation between surface contamination and hand wash measurements for chromium (correlation co-efficient 0.29, P=0.14).
-
-
”Clean” areas
-
A strong positive correlation between surface contamination and hand wash measurements for nickel (correlation co-efficient 0.7, P<0.0001); and
-
A weak, low positive correlation between surface contamination and hand wash measurements for chromium (correlation co-efficient 0.38, P=0.12).
-
The general trend was for a moderate positive correlation between surface wipe and hand wash measurements, more marked for nickel than for chromium. These correlations indicate that surface contamination contributes to workers exposure for both nickel and chromium through hand contamination.
A positive correlation between surface wipes and biological monitoring data can be deduced from the positive correlations between handwashing results and biological monitoring data, and surface wipe and handwashing data.
Air Sampling
Air sampling was conducted at a subset of sites to quantify inhalation exposures. In general, air sampling was performed on revisits where the initial visit had yielded elevated BM results. It is therefore reasonable to assume that exposure controls at these sites were of a lower standard than at other sites visited. Summary data are presented in Table 8.
The measured inhalation exposures for both chromium and nickel were generally below the relevant exposure limits. This is true even in situations where good exposure control practice was not being employed such as in the case of air agitated nickel electroplating baths operated without LEV.22
Statistical analysis shows:
-
A moderate positive correlation between urinary nickel and inhalation exposure (correlation co-efficient 0.56, P<0.01) for nickel workers;
-
A moderate positive correlation between urinary chromium and inhalation (as total chromium) exposure (correlation co-efficient 0.52, P=0.03) for chromium workers; and
-
A moderate positive correlation between urinary chromium and inhalation (as chromium VI) exposure (correlation co-efficient 0.62, P<0.0001) for chromium workers (see Figure 2).
Figure 2 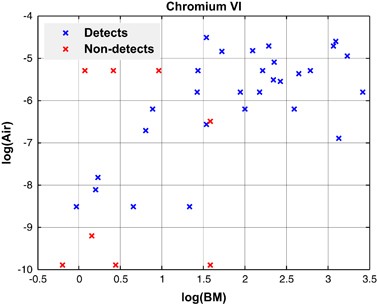
Correlation between inhalation exposure and BM results for chromium VI.

The measured inhalation exposures cannot fully account for the urinary nickel and chromium results.46, 47 If exposure occurred via inhalation alone, then the BM results would have been much lower. This is supported by the conclusions of other researchers,48 indicating that a significant proportion of exposure occurs via ingestion and/or dermal absorption routes.
A communication tool was developed to help workers interpret their BM results by comparing with air monitoring results and relevant exposure limits. This tool used a control banding approach, known as a “traffic light system” (see Table 9).
Exposure Control
A number of exposure control deficiencies were observed during the site visits. Sites were given advice on improving controls in line with principles of the hierarchy of control. Information provided from sites during follow-on exercises revealed some exposure control changes, which reduced exposures.
Although it is possible to conduct decorative chromium plating using chromium III rather than chromium VI (chromium III does not have the potential to cause the same serious health effects), many of the companies visited were still using chromium VI for this purpose.
Air agitation was most commonly used to create movement in nickel plating solutions, and this has a high potential for aerosol emission. Other methods are available to achieve this, including cathode rod movement and eductors, but these were not commonly used. Eductors were only observed in use at a single site. Figure 3 illustrates the effect of removing air agitation from nickel plating tanks and replacing with eductors, at this site, lowering personal exposure to nickel. The results cannot be extrapolated for multiple sites.

Reduction in urinary nickel levels for two electroplaters at a single site, between initial and follow-on work, where air agitation was replaced by eductors.
It was found that 10 of the 15 sites with the highest urinary nickel concentrations were operating nickel tanks without LEV.
All chromium VI electroplating baths were fitted with LEV and/or contained a surfactant. A surfactant is added to a plating bath to reduce mist generation. Perfluorooctane sulphonate (PFOS) was the most common surfactant. Some LEV systems however, did not adequately capture aerosols generated, and some surfactant concentrations were not checked regularly. Tank covers were not common due to frequent tank loading and unloading, and generally only used if electroplating time was significant (i.e., in the case of hard chromium plating, several hours).
Glove selection procedures varied widely from site to site. There was inconsistency in types of gloves used and the management of their use.
RPE was worn at some sites when undertaking bulk additions to tanks or for some maintenance activities. RPE was not used as a control measure for electroplating or any other routine tank side work. Types of RPE ranged from disposable, negative pressure orinasal masks to full face, positive pressure equipment.
DISCUSSION
Exposure Routes
The positive correlations found between the air monitoring and BM results show that inhalation exposure is a significant factor. There were multiple factors contributing to inhalation exposure, dependent on the process.
The positive correlations between hand contamination and BM results show that dermal exposure is a significant factor. Hand contamination is accompanied by the potential for inadvertent ingestion through direct hand to mouth transfer, via food and drink, nail biting or contaminated items such as pens and cigarettes. It is not clear in this instance whether dermal absorption or ingestion is the most significant exposure route, although dermal absorption rates for the relevant metal salts studied in this project are reportedly low.49, 50
The surface wipe data revealed a consistently high proportion of results that demonstrated contamination of “clean” areas as well as production areas. Positive correlations were found between surface and hand contamination results for both nickel and chromium. Although contamination can be expected on surfaces in production areas, workers do not generally expect to receive contamination in clean areas. At several sites, the siting of PPE lockers and the wearing of work-wear at break times were two mechanisms, that explain the spread of contamination into clean areas such as canteens.
Contamination in areas such as canteens was frequent, leading to an increased risk of dermal and ingestion exposure, also increasing the risk of exposure to other, indirectly exposed workers. This exposure route has been previously detailed by other researchers.30 The detection of significant levels of contamination in such areas at some sites is an indication of a failure to prevent the spread of contamination from work areas; and/or provide an effective cleaning regime.
90th percentile guidance values for hand and surface contamination were adopted as a useful risk assessment tool. These values are not health based, but represent levels which companies should normally be able to achieve with good control measures in place. For this work, the 90th percentile concept was used to define a “significant level of contamination”.
Exposure Control
The need for LEV on air agitated nickel tanks is confirmed by the presence of the highest urinary nickel concentrations for sites operating nickel tanks without LEV (see Figure 4), as previously detailed in the literature,22, 51 in order to reduce aerosol emissions.

A comparison of urinary nickel results with the influence of LEV.
Often the hierarchy of control52 was not applied to dermal exposure, and the concept of a safe working distance was not widely understood.53 Gloves were often relied on as a primary barrier against dermal exposure, but these should only be used for splash protection.54 Workers should not immerse gloved hands into plating tanks, or directly handle contaminated items.
The results show that with improved controls and good occupational hygiene practice, reduced exposures can be readily achieved.7
Direct Feedback
The results show significant reductions in urinary nickel and chromium levels for some workers. The use of repeat BM along with targeted advice and direct feedback has provided clear evidence to individuals of their personal exposure in relation to working practices and tasks performed. Figure 5 gives an example of a sustained reduction in exposure for a maintenance worker after an initial set of BM results were reported to the individual. Where appropriate, the hand wash and surface wipe results were used in conjunction with BM results to explain to workers how exposures can occur. Comparisons of (anonymised) results for workers, who undertook the same tasks but had lower results, could be used to identify issues with individual work practices. Anecdotal evidence suggests that such direct feedback is not given when air sampling is conducted, and this may partially explain the positive effect of BM on workers risk awareness.

Reduction in urinary chromium levels for a maintenance worker between initial and follow-on work.
CONCLUSIONS
Exposure to chromium and nickel compounds in the electroplating industry occurs via a combination of inhalation, dermal and ingestion routes. Overall, the directly exposed worker subset of electroplaters had the highest exposure, although other directly exposed worker subgroups, such as maintenance staff, chemists and ancillary workers (e.g., jigging and unmasking of electroplated items), also received elevated exposures. This widespread exposure risk must be taken into account when conducting risk assessments and designing exposure control strategies. Many of the risks can be easily (and cost-effectively) eliminated or controlled.
There were significant reductions in urinary nickel and chromium levels over the lifetime of this work in the subset of companies where initially, control deficiencies were more significant. These have been assisted by a repeat BM programme, provision of direct feedback to individual workers, and targeted advice to individual companies. This suggests that repeat BM over a period of time can help to drive sustainable improvements.
There were multiple sources of dermal exposure. A major source was through poor working practices, and an over reliance of PPE. The hierarchy of control52 should be applied to dermal exposure as well as other routes. There are many cost effective methods that can be implemented to reduce exposures.
Surface contamination in “clean” areas highlights the potential for transferral from the work area and the importance of having a regular cleaning regime in place throughout the workplace. Surface contamination may often lead to dermal and ingestion exposure.
When a good standard of exposure control exists, it is possible to carry out electroplating activities with very little worker exposure. Periodic BM checks have a role to play in maintaining workers risk awareness, facilitating a high level of control.
References
ESIS (European Chemical Substances Information System). Available from: http://esis.jrc.ec.europa.eu/index.php?PGM=cla. Accessed 28 April 2014.
HSE “What is REACH?”. Available from: http://www.hse.gov.uk/reach/whatisreach.htm. Accessed 28 April 2014.
HSE. Health and Safety Guidance, HSG 167. Biological monitoring in the workplace. a practical guide to its application to chemical exposure, 1997. Available from: http://www.hse.gov.uk/pubns/priced/hsg167.pdf. Accessed 3rd March 2014.
HSE. HSE Research Report RR 828 ‘Occupational exposure to MbOCA (4,4’-methylene-bis-ortho-chloroaniline) and isocyanates in polyurethane manufacture’, 2010. Available from: http://www.hse.gov.uk/research/rrpdf/rr828.pdf. Accessed 3 March 2014.
Cocker J, Cain JR, Baldwin P, McNally K, Jones K . A survey of occupational exposure to 4,4’-methylene-bis (2-chloroaniline) (MbOCA) in the UK. Ann Occup Hyg 2009; 53: 499–507.
Keen C, Coldwell M, McNally K, Baldwin P, McAlinden J, Cocker J . A follow up study of occupational exposure to 4,4′-methylene-bis(2-chloroaniline) (MbOCA) and isocyanates in polyurethane manufacture in the UK. Toxicol Lett 2011; 213: 3–8.
HSE. HSE Research Report RR 963. Exposure to hexavalent chromium, nickel and cadmium compounds in the electroplating industry, 2013. Available from: http://www.hse.gov.uk/research/rrpdf/rr963.pdf. Accessed 3 March 2014.
Colli G, Terzi R, Terzi M, Catenacci G . Application of mathematical modelling for assessing the urinary half-times of nickel in stainless steel welders. G Ital Med Lav Ergon 2005; 27: 427–430.
World Health Organization (WHO). Air Quality Guidelines for Europe. WHO Regional Publications, European Series, No. 91, 2nd edn. WHO Regional Office for Europe: Copenhagen. 2000.
HSL. Guidance on Laboratory Techniques in Occupational Medicine. 12th edn, 2013 (in-house).
Langard S, Costa M. Chapter 24 - Chromium. Nordberg GF, Fowler BA, Nordberg M, Friberg LT (eds). Handbook on the Toxicology of Metals. 3rd edn, Elsevier Amsterdam, 1986; ISBN: 978-0-12-369413-3.
HSE, 2011. EH40/2005 Workplace exposure limits. Available from: http://www.hse.gov.uk/pubns/books/eh40.htm. Accessed 25 March 2014.
Recommendation from the Scientific Committee on Occupational Exposure Limits for Nickel and Inorganic Nickel Compounds, SCOEL/SUM/85, June 2011. Available from: http://ec.europa.eu/social/BlobServlet?docId=6935&langId=en. Accessed 25 March 2014.
Recommendation from the Scientific Committee on Occupational Exposure Limits for Chromium Metal, Inorganic Chromium (II) Compounds, and Inorganic Chromium (III) Compounds SCOEL/SUM/50, December 2002. Available from: http://ec.europa.eu/social/BlobServlet?docId=3853&langId=en. Accessed 25 March 2014.
Recommendation from the Scientific Committee on Occupational Exposure Limits: Risk Assessment for Hexavalent Chromium SCOEL/SUM/86, December 2004. Available from: http://ec.europa.eu/social/BlobServlet?docId=3851&langId=en. Accessed 25 March 2014.
ACGIH. Guide to Occupational Exposure Values. ISBN 978-1-607260-49-3. ACGIH: Cincinnati, Ohio, 2012.
ACGIH. TLVs and BEIs Based on the Documentation of the Threshold Limit Values for Chemical Substances and Physical Agents & Biological Exposure Indices. ISBN 978-1-607260-48-6. ACGIH: Cincinnati, Ohio, 2012.
Occupational Safety and Health Administration (OSHA). Occupational Safety and Health Standards Z, Toxic and Hazardous Substances. Standard No. 1910.1026 Appendix A—Chromium VI. Available from: https://www.osha.gov/pls/oshaweb/owadisp.show_document?p_table=STANDARDS&p_id=13096. Accessed 25 March 2014.
OSHA. Nickel, Metal and Insoluble Compounds (as Ni). Available from: https://www.osha.gov/dts/chemicalsampling/data/CH_256200.html. Accessed 25 March 2014.
US Department of Health and Human Services, Public Health Service Agency for Toxic Substances and Disease Registry, 2005. Toxicological profile for Nickel. Available from: http://www.atsdr.cdc.gov/toxprofiles/tp15.pdf. Accessed 25 March 2014.
Cherrie JW, Gorman Ng M, Searl A, Shafrir A, van Tongeren M, Mistry R . Health, socio-economic and environmental aspects of the possible amendments to the EU Directive on the protection of workers from the risks related to exposure to carcinogens and mutagens at work. Hexavalent Chromium, 2011. Available from: http://ec.europa.eu/social/BlobServlet?docId=10158&langId=en. Accessed 28 April 2014.
SEA/HSE Guidance Sheet. Nickel and nickel alloy electroplating operations: controlling the risk of inhaling mist containing nickel. Available from: http://www.hse.gov.uk/surfaceengineering/nickelinhalation.pdf. Accessed 3 March 2014.
SEA/HSE Guidance Sheet. Nickel and nickel alloy electroplating operations: controlling the risk of skin exposure Available from: http://www.hse.gov.uk/surfaceengineering/nickelexposure.pdf. Accessed 3 March 2014.
SEA/HSE Guidance Sheet. Prevention and control of exposure to chromic acid. Available from: http://www.hse.gov.uk/surfaceengineering/chromicacid.pdf. Accessed 3 March 2014.
SEA/HSE Guidance Sheet. Prevention of exposure and control of chromic acid mist. Available from: http://www.hse.gov.uk/surfaceengineering/chromicacidmist.pdf. Accessed 3 March 2014.
SEA/HSE Guidance Sheet. Health surveillance for hexavalent chromium processes. Available from: http://www.hse.gov.uk/surfaceengineering/eh2.pdf. Accessed 3 March 2014.
SEA/HSE Guidance Sheet. Monitoring for electrolytic hexavalent chromium processes. Available from: http://www.hse.gov.uk/surfaceengineering/hexavalentchromium.pdf. Accessed 3rd March 2014.
Cocker J, Mason HJ, Warren ND, Cotton RJ . Creatinine adjustment of biological monitoring results. Occup Med (Lond) 2011; 61: 349–353.
Nicholson PJ, Llewellyn D, English JS. Evidence-based guidelines for the prevention, identification and management of occupational contact dermatitis and urticaria. Contact Dermatitis 2010; 63: 177–186.
Cherrie JW, Semple S, Christopher Y, Saleem A, Hughson G, Phillips A . How important is inadvertent ingestions of hazardous substances at work. Ann Occup Hyg 2006; 50: 693–704.
Brouwer DH, Boeniger MF, Van Hemmen J . Hand wash and manual skin wipes. Ann Occup Hyg 2000; 44: 501–510.
DD CEN/TS 15279:2006 Workplace exposure. Measurement of dermal exposure. Principles and methods. ISBN 0-580-48102-6, British Standards Institution (BSI), 2006.
ISO. ISO/TR 14294 Workplace atmospheres. Measurement of dermal exposure. Principles and methods. ISBN 978-0-580-75356-5, British Standards Institution (BSI), 2011.
Fenske RA . Dermal exposure assessment techniques. Ann Occup Hyg 1993; 37: 687–706.
Wheeler J, Stancliffe J . Comparison of methods for monitoring solid particulate surface contamination in the workplace. Ann Occup Hyg 1998; 42: 477–488.
Stancliffe J, Wheeler J, Dabill D . Monitoring PCB surface contamination using the wipe sampling method. Occup Hyg 1999; 5: 145–166.
Brookhaven Surface Wipe Sampling procedure IH75190 rev18 05/10/11 (recently updated: final rev18). Available from: www.bnl.gov/esh/shsd/sop/pdf/ih_sops/ih75190.pdf. Accessed 25th March 2014.
American Society for Testing and Materials (ASTM) D6966-13. Standard practice for collection of settled dust samples using wipe sampling methods for subsequent determination of metals. Available from: http://www.astm.org/Standards/D6966.htm. Accessed 25 March 2014.
ASTM D7296-12. Standard practice for collection of settled dust samples using dry wipe sampling methods for subsequent determination of beryllium and compounds. Available from: http://www.astm.org/Standards/D7296.htm. Accessed 25 March 2014.
ASTM E1728-10. Standard practice for collection of settled dust samples using wipe sampling methods for subsequent lead determination. Available from: http://www.astm.org/Standards/E1728.htm. Accessed 25 March 2014.
HSE, 2006. HSG173 Monitoring strategies for toxic substances. Available from: http://www.hse.gov.uk/pubns/priced/hsg173.pdf. Accessed 3 March 2014.
HSE, 2000. MDHS 14/3 General methods for the sampling and gravimetric analysis of respirable and inhalable dust. Available from: http://www.hse.gov.uk/pubns/mdhs/pdfs/mdhs14-3.pdf. Accessed 3 March 2014.
Cherrie J, Howie R, Semple S . Monitoring for Health Hazards at Work, 4th edn. ISBN 978-1-4051-5962-3, Wiley-Blackwell: Chichester, UK, 2010.
Ramachandran G . Occupational Exposure Assessment for Air Contaminants. Taylor and Francis Group, ISBN 1-56670-609-2. Taylor and Francis Group: Boca Raton, Florida, 2005.
Gardiner K, Harrington JM . Occupational Hygiene, 3rd edn. ISBN 1-4051-0621-2, 2005. Blackwell Publishing: Malden, Massachusetts, 2005.
DFG. Deutsche Forschungsgemeinschaft List of MAK and BAT Values 2011. DFG. Wiley-VCH: Bonn, Germany, 2011.
American Conference of Industrial Hygienists (ACGIH) Biological Exposure Index (BEI). Chromium (VI), Water-Soluble Fume: BEI®, 7th edn. Documentation ACGIH Publication #7DOC-671, 2004.
Killunen M, Aitio A, Tossavainen A . Occupational exposure to nickel salts in electrolytic electroplating. Ann Occup Hyg 1997; 41: 189–200.
International Programme on Chemical Safety (IPCS). International Programme on Chemical Safety, Environmental Health Criteria 61, Chromium, 1988. Available from: http://www.inchem.org/documents/ehc/ehc/ehc61.htm. Accessed 27 February 2014.
International Programme on Chemical Safety (IPCS). International Programme on Chemical Safety, Environmental Health Criteria 108, Nickel 1988 Available from: http://www.inchem.org/documents/ehc/ehc/ehc108.htm. Accessed 27 February 2014.
The Canning Handbook. Surface Finishing Technology, 23rd edn. ISBN 0-419-12900-6. Canning PLC: Birmingham, UK, 1989.
HSE. Control of substances hazardous to health. The Control of Substances Hazardous to Health Regulations 2002 (as amended). ISBN 978-0-7176-6582-2, 2013. Available from http://www.hse.gov.uk/pubns/priced/l5.pdf. Accessed 10 June 2014.
Sithamparanadarajah R . Controlling Skin Exposure to Chemicals and Wet Work—A Practical Book. British Occupational Hygiene Society, ISBN 978-1-906674-00-7 RMS Publishing: Stourbridge, UK, 2008.
HSE. HSE Research Report RR 1042. Exposure to carcinogens in surface engineering: supplementary report, 2015. Available from: http://www.hse.gov.uk/research/rrpdf/rr1042.pdf. Accessed 4 March 2015.
Acknowledgements
Thanks are given to the Surface Engineering Association (SEA) who partnered the Health and Safety Executive (HSE) in this work and to the companies who were visited as part of the project. This publication and the work it describes were funded by the Health and Safety Executive (HSE). Its contents, including any opinions and/or conclusions expressed, are those of the authors alone and do not necessarily reflect HSE policy.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
About this article

Cite this article
Beattie, H., Keen, C., Coldwell, M. et al. The use of bio-monitoring to assess exposure in the electroplating industry. J Expo Sci Environ Epidemiol 27, 47–55 (2017). https://doi.org/10.1038/jes.2015.67
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/jes.2015.67
Keywords
This article is cited by
-
Sustainability metrics and technical solution derivation for performance improvement of electroplating facilities
Clean Technologies and Environmental Policy (2023)
-
Chromium removal from tannery wastewaters with a strong cation exchange resin and species analysis of chromium by MINEQL+
Scientific Reports (2022)
-
Synergetic Modelling of Energy and Resource Efficiency as well as Occupational Safety and Health Risks of Plating Process Chains
International Journal of Precision Engineering and Manufacturing-Green Technology (2022)
