
Abstract
The relationship between cardiorespiratory fitness and arterial compliance in children and adolescents remains controversial. The aim of this study was to assess this association with a quantitative approach. A total of 646 healthy children and adolescents (316 females, age 13.9±2.1 years) were cross-sectionally investigated in seven school settings in and around Munich for their cardiorespiratory fitness and demographic, anthropometric and hemodynamic parameters. Surrogates of arterial stiffness, such as pulse wave velocity (PWV), Augmentation Index normalized to a heart rate of 75 (AI@75), and peripheral and central systolic blood pressures were measured in a supine position using the oscillometric Mobil-O-Graph. Cardiopulmonary fitness was measured by 6-min indoor run tests. After correction for age, sex, body weight, body height, heart rate and mean arterial pressure, controversial findings were produced. PWV increased with higher cardiorespiratory fitness (Beta=0.173; P<0.001), which represented an unfavorable relationship, whereas AI@75 declined with higher cardiorespiratory fitness (Beta=−0.106; P=0.025). Therefore, in contrast to PWV, higher cardiorespiratory fitness seems beneficial for AI@75. The third surrogate of arterial stiffness, central systolic blood pressure, showed no association with cardiorespiratory fitness (Beta=0.066; P=0.052). These controversial outcomes remain almost unchanged when the boys and girls were analyzed separately. Different surrogates of arterial stiffness have different relationships with cardiorespiratory fitness in children and adolescents after correcting for multiple confounders. More research is needed in this field to understand the functioning of the juvenile vessels, and measurements and methodological approaches should be reconsidered.
Similar content being viewed by others

Introduction
Good cardiorespiratory fitness and sufficient physical activity are two of the most effective and simple strategies for the primary prevention of lifestyle diseases such as cardiovascular events, atherosclerosis, obesity, cancer and diabetes.1, 2, 3 Furthermore, a higher cardiorespiratory fitness level has beneficial acute4 and chronic effects on the arterial system and leads to lower arterial stiffness,5 which is determined by the arterial wall structure and is a valid predictor of cardiovascular events.6
The association between higher cardiorespiratory fitness and higher arterial compliance has been well described in adults,5, 7, 8, 9, 10 and some studies propose that this beneficial relationship has its genesis already in early life.11, 12, 13 However, current research in children remains controversial. The Copenhagen Cohort Study of Infant Nutrition and Health11 and the Northern Ireland Young Hearts Project9 found that decreased cardiorespiratory fitness results in stiffer arteries in healthy 10-year-old normal weight children. In contrast, Müller et al.14 found no significant relationship between peak oxygen uptake and arterial stiffness after measuring central systolic blood pressure in children and adolescents. This assumption is supported in other studies.15, 16, 17 Determinants such as body composition (that is, body mass index or body fat), which itself is a strong marker for arterial stiffness and cardiorespiratory fitness,18, 19 may affect cardiorespiratory fitness to a greater extent than cardiorespiratory fitness in children and adolescents.14, 20
A basic, simple and noninvasive method for determining arterial stiffness requires the measurement of surrogates such as pulse wave velocity (PWV), central systolic blood pressure and Augmentation Index (AI).21, 22, 23 After trying to assess the association of cardiorespiratory fitness and arterial stiffness with the qualitative measure of peak oxygen uptake derived from cardiopulmonary exercise testing,14 this study aimed to clarify this question with a quantitative approach by assessing cardiorespiratory fitness with a six-minute run test in a broad school setting.
Methods
Study design
From December 2011 to July 2013, healthy children and adolescents were prospectively recruited in seven school-based settings. The final data collection occurred in four school settings in Munich, Bavaria (integrated and grammar schools), two schools in rural areas of Bavaria (Buxheim and Murnau, Bavaria) and one grammar school in Göttingen (Niedersachsen). The study was conducted in accordance with the Declaration of Helsinki (revision 2008) and was approved by the local ethical board of the Technische Universitat München (project number: 5162/11). Children and adolescents gave written informed consent and agreed to the anonymous publication of their data. Some of the data have recently been published elsewhere.24
Study subjects
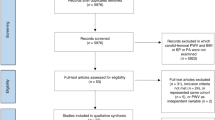
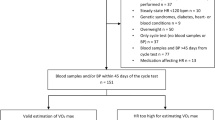
Subjects under 11 or over 18 years were excluded as well as subjects with congenital heart disease or known hypertension, even if treated with antihypertensive medication or other BP-affecting drugs. All subjects underwent a measurement of their demographic, anthropometric, hemodynamic and cardiopulmonary parameters in the same way, with the same methods and the same devices. Examination started with anthropometrics and the assessment of arterial stiffness in the supine position after 5 min rest. Then, a 6-min run test was performed. All examinations occurred at the same day in a regular school gym from 0800 to 1300.
Only subjects achieving a maximum heart rate over 85% during the 6-min indoor run tests were included in the analysis. Additionally, 18 subjects with an on-site measured systolic blood pressure 140 mm Hg or higher were excluded from the analysis because of possible hypertension.
In total, 646 children and adolescents (316 females, age 13.9±2.1 years) were included in the statistical analysis. The characteristics of the study population are displayed in detail in Table 1.
Measurement of anthropometrics and surrogates of arterial stiffness
Body weight (in light sports clothing and without shoes) and height were measured using portable scales and stadiometers (Seca799, MedicalLine, Hamburg, Germany) by trained staff to the nearest of 0.1 kg and 0.5 cm, respectively.
Surrogates of arterial stiffness, such as central systolic blood pressure and pulse wave velocity (PWV) and Augmentation Index normalized to a heart rate of 75 (AI@75), were measured on the left upper arm automatically with the oscillometric cuff-based Mobil–O-Graph (IEM Healthcare, Stolberg Germany) device in a supine position after 5–10 min rest. Subjects were advised to lie down quietly on a sports mat in the gym during measurement. Cuffs were chosen according to the measured left upper arm circumference.25
Central systolic blood pressure, PWV and AI@75 were indirectly estimated with an ARCSolver Algorithmus (Austrian Institute of Technology, Vienna, Austria) based on the recorded brachial pulse waves. That method included the influence of arterial impedance and the aortic hemodynamics using a generalized transfer function and a mathematical model. It is confirmed that this noninvasive cuff-based method strongly correlates with the invasive measurement of central blood pressure.26
Measurement of 6-min indoor run tests
Six-min indoor run tests were used to measure the cardiorespiratory fitness levels of children and adolescents according to the test module by Bös and colleagues.27 In brief, participants ran for 6 min around a 9 × 18 m indoor field (volleyball court) with the aim of going as far as possible. The four angles were tagged by pylons and each lap measured 54 meters. After 6 min, subjects were asked to rest at their final position to record the covered distance by trained staff. Furthermore, heart rate was measured with the ‘Acentas Herzfrequenz Monitoring Team System’ (Acentas GmbH, Hörgertshausen, Germany) throughout the entire run test.
Data analyses
The descriptive data was expressed as mean values and s.d. (mean±s.d.). BMI was calculated by dividing the weight in kilograms by the squared height in meters. The association of surrogates of arterial stiffness (central systolic blood pressure, PWV, AI@75) and cardiorespiratory fitness was assessed using a multivariate linear regression model corrected for mean arterial pressure, heart rate, sex, age, body height and weight for PWV, and central blood pressure. AI@75 was corrected for sex, age, body height and weight only. Gender-specific outcomes are provided in the tables.
All analyses were performed using SPSS 23.0 software (IBM Corp., Armonk, NY, USA). P-values <0.05 in a two-sided analysis were considered significant.
Results
As shown in table 1, the girls were significantly older than the boys (P<0.001), had higher BMI (P=0.002), slower PWV (P=0.024), higher AI@75 (P<0.001) and exhibited a shorter six-minute running distance (P<0.001).
PWV increased with higher cardiorespiratory fitness (Beta=0.173; P<0.001), which represents an unfavorable relationship. On the other hand, AI@75 declined with higher cardiorespiratory fitness (Beta=−0.106; P=0.025). Higher cardiorespiratory fitness seems beneficial for AI@75 in contrast to PWV. There was no association of cardiorespiratory fitness and central systolic blood pressure (Beta=0.066; P=0.052), which was the third surrogate of arterial stiffness measured.
When analyzing the boys and girls separately but including the correction of PWV and central blood pressure for mean arterial pressure, heart rate, sex, age, weight and height (Table 2) and Augmentation Index (AI@75) for sex, age, weight and height (Table 3), those controversial findings remained. Only in the boys did the significant association of AI@75 and cardiorespiratory fitness disappear.
Discussion
This study shows a controversial outcome regarding the associations of arterial stiffness surrogates and cardiorespiratory fitness parameters. In our analysis, all three surrogates of arterial stiffness, central systolic blood pressure, PWV and AI@75, showed opposed findings in a respectably large cohort.
In our qualitative approach using cardiopulmonary exercise testing, we found no association with arterial stiffness in children and adolescents.14 With the quantitative approach, we saw controversial results. While PWV demonstrates a negative relationship to cardiorespiratory fitness, AI turned out to be beneficially associated. However, in both of them, the effect, albeit opposed, was only weak. This poor correlation of cardiorespiratory fitness and distensibility measured by ultrasound was also noted in a large cohort study in young and middle-aged adults.28 In front of this background, it was not surprising that the third surrogate of arterial stiffness, central blood pressure, had no significant relationship with cardiorespiratory fitness.
When reviewing the literature, the controversy between cardiorespiratory fitness and arterial stiffness in children became obvious. Reed and colleagues found a slight association between physical activity and arterial stiffness or compliance in 9- to 11-year-old children. However, the contribution of fitness and other confounders to arterial compliance was low and differed strongly between small and large arterial compliance.16
Interestingly, the results that detect an association are usually mediated by fat intake,11 body height16 or blood pressure.29 Sakuragi and coworkers revealed that arterial stiffness, measured as PWV, depends on body fat and that changes of arterial stiffness and physical fitness are possibly mediated by body fat.12, 30 Only investigations in older subjects, such as young adults and adolescents, verified an inverse relationship between arterial stiffness and cardiorespiratory fitness independent of body mass or body composition.9 Wildman et al.31 showed that an association between higher body weight and increased vascular stiffness exist in adults between 20 and 30 years of age, suggesting that the vascular effects of obesity occur at a very early stage of vascular aging. Even Müller et al.14 highlighted the impact of body weight on the arterial system in a previous investigation. However, stiffening of arteries occurs very slowly in children and adolescents, and this process is difficult to assess in younger subjects.12 At the beginning of adulthood, evidence supports a valid and obviously increased arterial stiffness.5, 7, 8 In early ages, maturity and growth may bias the association of increased arterial stiffness and cardiorespiratory fitness.
However, it could be speculated that cardiorespiratory fitness is not the appropriate measure and more attention should be given to physical activity and the association with arterial stiffness. Ried-Larssen and colleagues found an association between the mean minutes of vigorous physical activity and the metabolic risk z-score in adolescence.17 However, further approaches are needed to fill the knowledge gaps in the field of juvenile vascular functioning and how they interact with measures of exercise capacity.
Finally, there is another shortcoming that should be addressed here. Arterial stiffness is just an umbrella term for many surrogates of arterial stiffness that can be assessed with different devices and methods. Unfortunately, the term arterial stiffness is used interchangeably.32, 33
Applanation tonometry is assumed to be the gold standard, but the hand-held device requires well-trained investigators and frequent use.34 Semi-automatic cuff-based devices use arterial transfer functions of the radial artery waveform to reconstruct the corresponding central pressure waveform with an algorithm.26, 32, 33 However, the validity of this transfer function is also controversial,35 as is the necessity of standardizing Augmentation Index to a heart rate of 75 beats per minute.36 Standardized and uniform measures and devices must be established to resolve the lack of comparability between many different studies. There should be more transparency regarding the algorithms that were used to calculate the recorded brachial pulse waves to central hemodynamics.
Conclusion
Different surrogates of arterial stiffness had different associations with cardiorespiratory fitness in children and adolescents after correction for multiple confounders. More research is needed in this field to understand the functioning of the juvenile vessels, and measurements and methodological approaches should be reconsidered.
Limitations
Oscillometric measurement is an indirect measure of arterial stiffness and not the gold standard.37 However, with regard to methodical issues, no standardization for the measurement of central systolic blood pressure and PWV in children, adolescents and especially obese subjects exists. Therefore, hemodynamic outcomes have been measured differently in several studies due to a lack of comparability. Moreover, in further studies, adjustment for potential confounding variables such as maturation, abdominal and visceral body fat and physical activity in daily life must be taken into account in the hope that uniform associations regarding the different surrogates occur.
References
Ruiz JR, Castro-Pinero J, Artero EG, Ortega FB, Sjostrom M, Suni J, Castillo MJ . Predictive validity of health-related fitness in youth: a systematic review. Br J Sports Med. 2009; 43: 909–923.
Ruiz JR, Huybrechts I, Cuenca-Garcia M, Artero EG, Labayen I, Meirhaeghe A, Vicente-Rodriguez G, Polito A, Manios Y, Gonzalez-Gross M, Marcos A, Widhalm K, Molnar D, Kafatos A, Sjostrom M, Moreno LA, Castillo MJ, Ortega FB group Hs. Cardiorespiratory fitness and ideal cardiovascular health in European adolescents. Heart 2015; 101: 766–773.
Wernhart S, Dinic M, Pressler A, Halle M . [Prevention of cardiovascular diseases through sport and physical activity: a question of intensity?]. Herz 2015; 40: 361–368.
Perdomo SJ, Moody AM, McCoy SM, Barinas-Mitchell E, Jakicic JM, Gibbs BB . Effects on carotid-femoral pulse wave velocity 24 h post exercise in young healthy adults. Hypertens Res 2016; 39: 435–439.
Vaitkevicius PV, Fleg JL, Engel JH, O'Connor FC, Wright JG, Lakatta LE, Yin FC, Lakatta EG . Effects of age and aerobic capacity on arterial stiffness in healthy adults. Circulation 1993; 88 (4 Pt 1): 1456–1462.
Laurent S, Cockcroft J, van Bortel L, Boutouyrie P, Giannattasio C, Hayoz D, Pannier B, Vlachopoulos C, Wilkinson I, Struijker-Boudier H . Expert consensus document on arterial stiffness: methodological issues and clinical applications. Eur Heart J 2006; 27: 2588–2605.
Kingwell BA . Large artery stiffness: implications for exercise capacity and cardiovascular risk. Clin Exp Pharmacol Physiol 2002; 29: 214–217.
Tanaka H, Dinenno FA, Monahan KD, Clevenger CM, DeSouza CA, Seals DR . Aging, habitual exercise, and dynamic arterial compliance. Circulation 2000; 102: 1270–1275.
Boreham CA, Ferreira I, Twisk JW, Gallagher AM, Savage MJ, Murray LJ . Cardiorespiratory fitness, physical activity, and arterial stiffness: the Northern Ireland Young Hearts Project. Hypertension 2004; 44: 721–726.
Thompson PD, Buchner D, Pina IL, Balady GJ, Williams MA, Marcus BH, Berra K, Blair SN, Costa F, Franklin B, Fletcher GF, Gordon NF, Pate RR, Rodriguez BL, Yancey AK, Wenger NK American Heart Association Council on Clinical Cardiology Subcommittee on Exercise R, Prevention, American Heart Association Council on Nutrition PA, Metabolism Subcommittee on Physical Activity. Exercise and physical activity in the prevention and treatment of atherosclerotic cardiovascular disease: a statement from the Council on Clinical Cardiology (Subcommittee on Exercise, Rehabilitation, and Prevention) and the Council on Nutrition, Physical Activity, and Metabolism (Subcommittee on Physical Activity). Circulation 2003; 107: 3109–3116.
Schack-Nielsen L, Mølgaard C, Larsen D, Martyn C, Michaelsen KF . Arterial stiffness in 10-year-old children: current and early determinants. Br J Nutr 2005; 94: 1004–1011.
Sakuragi S, Abhayaratna K, Gravenmaker KJ, O'Reilly C, Srikusalanukul W, Budge MM, Telford RD, Abhayaratna WP . Influence of adiposity and physical activity on arterial stiffness in healthy children: the lifestyle of our kids study. Hypertension 2009; 53: 611–616.
Veijalainen A, Tompuri T, Haapala EA, Viitasalo A, Lintu N, Vaisto J, Laitinen T, Lindi V, Lakka TA . Associations of cardiorespiratory fitness, physical activity, and adiposity with arterial stiffness in children. Scand J Med Sci Sports 2015; 26: 943–950.
Müller J, Meyer J, Elmenhorst J, Oberhoffer R . Body weight and not exercise capacity determines central systolic blood pressure, a surrogate for arterial stiffness, in children and adolescents. J Clin Hypertens 2016; 18: 762–765.
Fernhall B, Agiovlasitis S . Arterial function in youth: window into cardiovascular risk. J Appl Physiol 2008; 105: 325–333.
Reed KE, Warburton DE, Lewanczuk RZ, Haykowsky MJ, Scott JM, Whitney CL, McGavock JM, McKay HA . Arterial compliance in young children: the role of aerobic fitness. Eur J Cardiovasc Prev Rehabil 2005; 12: 492–497.
Ried-Larsen M, Grøntved A, Møller NC, Larsen KT, Froberg K, Andersen LB . Associations between objectively measured physical activity intensity in childhood and measures of subclinical cardiovascular disease in adolescence: prospective observations from the European Youth Heart Study. Br J Sports Med 2014; 48: 1502–1507.
Ferreira I, Twisk JW, van Mechelen W, Kemper HC, Seidell JC, Stehouwer CD . Current and adolescent body fatness and fat distribution: relationships with carotid intima-media thickness and large artery stiffness at the age of 36 years. J Hypertens 2004; 22: 145–155.
Ferreira I, van de Laar RJ, Prins MH, Twisk JW, Stehouwer CD . Carotid stiffness in young adults: a life-course analysis of its early determinants: the Amsterdam Growth and Health Longitudinal Study. Hypertension 2012; 59: 54–61.
Twisk JW, Kemper HC, van Mechelen W . The relationship between physical fitness and physical activity during adolescence and cardiovascular disease risk factors at adult age. The Amsterdam Growth and Health Longitudinal Study. Int J Sports Med 2002; 23 (Suppl 1): S8–14.
McEniery CM, Cockcroft JR, Roman MJ, Franklin SS, Wilkinson IB . Central blood pressure: current evidence and clinical importance. Eur Heart J 2014; 35: 1719–1725.
Roman MJ, Devereux RB, Kizer JR, Lee ET, Galloway JM, Ali T, Umans JG, Howard BV . Central pressure more strongly relates to vascular disease and outcome than does brachial pressure: the Strong Heart Study. Hypertension 2007; 50: 197–203.
Hametner B, Wassertheurer S, Kropf J, Mayer C, Eber B, Weber T . Oscillometric estimation of aortic pulse wave velocity. Blood Press Monit 2013; 18: 173–176.
Elmenhorst J, Hulpke-Wette M, Barta C, Dalla Pozza R, Springer S, Oberhoffer R . Percentiles for central blood pressure and pulse wave velocity in children and adolescents recorded with an oscillometric device. Atherosclerosis 2015; 238: 9–16.
Elmenhorst J, Hulpke-Wette M, Barta C, Dalla Pozza R, Springer S, Oberhoffer R . Percentiles for central blood pressure and pulse wave velocity in children and adolescents recorded with an oscillometric device. Atherosclerosis 2014; 238: 9–16.
Weber T, Wassertheurer S, Rammer M, Maurer E, Hametner B, Mayer CC, Kropf J, Eber B . Validation of a brachial cuff-based method for estimating central systolic blood pressure. Hypertension 2011; 58: 825–832.
Bös KOE, Woll A, Liebisch R, Breithecker D, Kremer B . Das karlsruher testsystem für kinder (KATS-K)–testmanual. Haltung Bewegung 2001; 21: 4–66.
Huynh QL, Blizzard CL, Raitakari O, Sharman JE, Magnussen CG, Dwyer T, Juonala M, Kahonen M, Venn AJ . Vigorous physical activity and carotid distensibility in young and mid-aged adults. Hypertens Res 2015; 38: 355–360.
Li S, Chen W, Srinivasan SR, Berenson GS . Childhood blood pressure as a predictor of arterial stiffness in young adults: the bogalusa heart study. Hypertension 2004; 43: 541–546.
Cruickshank JK, Rezailashkajani M, Goudot G . Arterial stiffness, fatness, and physical fitness: ready for intervention in childhood and across the life course? Hypertension 2009; 53: 602–604.
Wildman RP, Mackey RH, Bostom A, Thompson T, Sutton-Tyrrell K . Measures of obesity are associated with vascular stiffness in young and older adults. Hypertension 2003; 42: 468–473.
Sakuragi S, Abhayaratna WP . Arterial stiffness: methods of measurement, physiologic determinants and prediction of cardiovascular outcomes. Int J Cardiol 2010; 138: 112–118.
Laurent S, Cockcroft J, Van Bortel L, Boutouyrie P, Giannattasio C, Hayoz D, Pannier B, Vlachopoulos C, Wilkinson I, Struijker-Boudier H . Expert consensus document on arterial stiffness: methodological issues and clinical applications. Eur Heart J 2006; 27: 2588–2605.
Van Bortel LM, Duprez D, Starmans-Kool MJ, Safar ME, Giannattasio C, Cockcroft J, Kaiser DR, Thuillez C . Clinical applications of arterial stiffness, Task Force III: recommendations for user procedures. Am J Hypertens 2002; 15: 445–452.
Hope SA, Meredith IT, Cameron JD . Arterial transfer functions and the reconstruction of central aortic waveforms: myths, controversies and misconceptions. J Hypertens 2008; 26: 4–7.
Stoner L, Faulkner J, Lowe A, Lambrick DM, Young JM, Love R, Rowlands DS . Should the Augmentation Index be Normalized to Heart Rate? J Atheroscler Thromb 2013; 21: 11–16.
Van Bortel LM, Laurent S, Boutouyrie P, Chowienczyk P, Cruickshank JK, De Backer T, Filipovsky J, Huybrechts S, Mattace-Raso FU, Protogerou AD, Schillaci G, Segers P, Vermeersch S, Weber T, Artery S, European Society of Hypertension Working Group on Vascular S, Function, European Network for Noninvasive Investigation of Large a. Expert consensus document on the measurement of aortic stiffness in daily practice using carotid-femoral pulse wave velocity. J Hypertens 2012; 30: 445–448.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article

Cite this article
Meyer, J., Elmenhorst, J., Giegerich, T. et al. Controversies in the association of cardiorespiratory fitness and arterial stiffness in children and adolescents. Hypertens Res 40, 675–678 (2017). https://doi.org/10.1038/hr.2017.19
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/hr.2017.19
Keywords
This article is cited by
-
Association of blood pressure, obesity and physical activity with arterial stiffness in children: a systematic review and meta-analysis
Pediatric Research (2022)
-
Combined association of cardiorespiratory fitness and family history of hypertension on the incidence of hypertension: a long-term cohort study of Japanese males
Hypertension Research (2018)
