
Abstract
Study design:
One case report of proximal tibia fracture in a patient with incomplete spinal cord injury (SCI) associated with robotic treadmill training.
Objective:
To raise the awareness that bone densitometry may be recommended before starting the robotic treadmill therapy, as well as the active vigilance of symptoms after therapy.
Setting:
Institute of Physical and Rehabilitation Medicine, Lucy Montoro Institute for Rehabilitation, Hospital das Clínicas, School of Medicine, University of São Paulo, São Paulo, Brazil.
Case report:
The patient, female gender, with a fracture of vertebra T12 and arthrodesis from T9 to L1 (American Spinal Injury Association Classification (ASIA-C)). Training on Lokomat consisted of five 30-min weekly sessions, under the supervision of a qualified professional. At the beginning of the 19th session, the patient complained of pain in the anterior region of the left knee. Lokomat and any other body support therapy were discontinued. Magnetic resonance imaging (MRI) evidenced a transverse, oblique, metaphyseal proximal anterior and medial tibial fracture.
Conclusion:
Fractures are among the chronic complications of a SCI, affecting 34% and many times arising from minimal traumas. Lokomat resembles physiological walking, and more studies show its benefits. Many studies encourage the use of robotic devices for the rehabilitation of lower limbs, but there are still several unanswered questions. However, there are not enough studies to show whether there is a higher risk of fracture incidence in patients with osteopenia or osteoporosis who trained on the Lokomat.
Similar content being viewed by others


Introduction
One of the main objectives of the spinal cord injury (SCI) rehabilitation program is the functional locomotion in a wheelchair or standing up.1 As well as the conventional rehabilitation treatment, robotic technologies are becoming more frequent for the treatment of neurological disorders in clinical environments.
Treadmill training with partial weight support opened new perspectives for patients with incomplete SCI. Lokomat (Hocoma, Volketswil, Switzerland) is a mechanical orthosis, linked to the body weight support (BWS) used to reach a reproducible walking standard, with the same rhythm, cadence and kinematic parameters, stimulating the sensorial feedback involved in normal locomotion.2
Case report
The patient, female gender, 43-year old, black, 155 cm in height and 55 kg. She suffered a fall from a height of 3 m in February 2011, with a fracture of vertebra T12 and arthrodesis from T9 to L1. At the Institute of Physical Medicine and Rehabilitation of Hospital das Clínicas, from the University of São Paulo Medical School (IMREA/HC/FMUSP), she was diagnosed with T12 incomplete paraplegia, with motor functions ranging from bilateral grade 3 at L2, bilateral grade 2 at L3 and grade 1 at L5 on the left and partial preservation of sensitive function at L1 to L3 levels (American Spinal Injury Association Classification (ASIA-C)). The patient was restricted to a wheelchair. The first two hospitalization (October, 2001; August, 2012) objectives were training orthostatic, but she had difficulties in adapting with orthoses on parallel bars. As SCI was incomplete, at the third hospital admittance in February 2013, it was decided that she should be training with Lokomat Training on Lokomat consisting of five 30-min weekly sessions. Initially, the device was programmed with a speed of 1.4 km h−1, 100% guiding force and 50% BWS. After 10 sessions, the speed was reduced to 1.2 km h−1 with guiding force varying between 90 and 75% and BWS remaining at 50%. At the beginning of the 19th session in March 2013, the patient complained of pain (visual analog scale: 7) in the anterior region of the left knee. The session was suspended, and the medical team was informed. Lokomat and any other body support therapy were discontinued during the treatment.
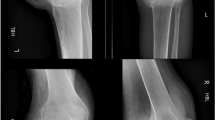
Magnetic resonance imaging (MRI) evidenced a transverse, oblique, metaphyseal proximal anterior and medial tibial fracture, with moderate medullary edema next to it and the related adipose tissues, without deviations, misalignment, fragmentation or impaction (Figure 1). Bone densitometry revealed the following: L3 and L4: T score −1.8; neck of femur right (R): T score −2.1, total femur (R): −2.9; whole body: T score −1.0. Total serum calcium 9.6, ionized serum calcium of 1.34 (unit of measurement), phosphorus 4.0, parathormone of 34 and serum vitamin D level of 11 ng ml−1 (deficiency). Vitamin D deficiency has been associated with decreased muscle mass and strength, osteomalacia, bone pain, osteoporosis and fractures due to impaired balance.3 In this case, the possibility of osteomalacia was discarded. Our patient did not have other symptoms, although osteomalacia is associated with a decrease in bone volume and excess osteoid accumulation. Oral calcium carbonate 500 mg per day and cholecalciferol 7.000 Ui per week were initiated and a single infusion of intravenous zoledronic acid, 4 mg diluted with 100 ml of sodium chloride 0.9%, was administered for osteoporosis management. The medication was well tolerated and the patient had no side effects.

Left knee MRI demonstrates fracture on the proximal anterior and medial tibial region. Black arrow indicates the fracture site.
Discussion
Patients with incomplete SCI with a functional walking prognosis must be emphasized at rehabilitation centers until they achieve their full potential. Lokomat comes close to the normal physiology of the walk, and more studies show its benefits on the rehabilitation of these patients.1
Fractures after SCI affect 34% and often arise from minimal traumas.4 Bone loss may affect any segment but is more intense on immobilized ones and in areas rich in trabecular bone, but new studies illustrated that both trabecular and cortical bone are equally influenced.5 To the best of our knowledge, this is the first report of a proximal tibia fracture during Lokomat training.
According to the manufacturer, the contraindication for this is severe osteoporosis with risk pathologic fractures (T score⩾3) and is not the case of the patient. However, there are not enough studies to show whether there is a higher risk of fracture incidence in patients with osteopenia or osteoporosis who trained on the Lokomat.
Conclusion
Many studies encourage the use of robotic devices for the rehabilitation of lower limbs, but there are still several unanswered questions. Bone densitometry may be recommended before starting the robotic treadmill therapy, as well as the active vigilance of symptoms after therapy. Future studies setting standards to mineral bone density and defining training protocols on Lokomat might avoid this type of complication.
References
Hesse S, Werner C . Connecting research to the needs of patients and clinicians. Brain Res Bull 2009; 78: 26–34.
Dietz V, Harkema SJ . Locomotor activity in spinal cord-injured persons. J Appl Physiol (1985) 2004; 96: 1954–1960.
Visser M, Deeg DJ, Lips P . Low vitamin D and high parathyroid hormone levels as determinants of loss of muscle strength and muscle mass (sarcopenia): the Longitudinal Aging Study Amsterdam. J Clin Endocrinol Metab 2003; 88: 5766–5772.
Lazo MG, Shirazi P, Sam M, Giobbie-Hurder A, Blacconiere MJ, Muppidi M . Osteoporosis and risk of fracture in men with spinal cord injury. Spinal Cord 2001; 39: 208–214.
Edwards WB, Schnitzer TJ, Troy KL . Bone mineral and stiffness loss at the distal femur and proximal tibia in acute spinal cord injury. Osteoporos Int 2014; 25: 1005–1015.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
This work is licensed under a Creative Commons Attribution 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/
About this article

Cite this article
Filippo, T., De Carvalho, M., Carvalho, L. et al. Proximal tibia fracture in a patient with incomplete spinal cord injury associated with robotic treadmill training. Spinal Cord 53, 875–876 (2015). https://doi.org/10.1038/sc.2015.27
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sc.2015.27
This article is cited by
-
Incidental bilateral calcaneal fractures following overground walking with a wearable robotic exoskeleton in a wheelchair user with a chronic spinal cord injury: is zero risk possible?
Osteoporosis International (2020)
-
Dual-energy X-ray absorptiometry and fracture prediction in patients with spinal cord injuries and disorders
Osteoporosis International (2017)
-
Proximal tibia fracture in a patient with incomplete spinal cord injury associated with robotic treadmill training
Spinal Cord Series and Cases (2016)
