
Abstract
Study design:
A retrospective hospital-based study.
Objectives:
To describe the epidemiologic features of traumatic spinal cord injury (TSCI) in Anhui Province.
Setting:
Two hospitals within Anhui Province, China.
Methods:
We retrospectively reviewed the hospital records on all patients with TSCI, admitted between 1 January 2007 and 31 December 2010 (n=761). Variables included age, gender, occupation, neurological level, severity of injury, cause and treatment.
Results:
Seven hundred and sixty-one cases of TSCI were identified. Five hundred and eighty eight were males (77.3%) and 173 were females (22.7%), with a mean age of 45 years (s.d.=13, range from 5 to 87). Fall from height was the leading cause of injury (52.6%), followed by transport (21.2%). The neurological lesion levels were cervical (46.3%), lumbosacral (33.3%) and thoracic (20.4%).
Conclusion:
Prevention strategies for TSCI should target 30–60 age group, males, farmers and fall from height. The results of this study will serve as a basis for further studies on TSCI. The prevention strategies and treatment should be designed according to the injury features.
Similar content being viewed by others

Introduction
Traumatic spinal cord injury (TSCI) is a devastating condition and a major cause of disability.1 There is no cure for TSCI just yet. The injury has been put both economic and social burden on patients and their families.2, 3 The estimated annual incidences of TSCI varied from 16 per million to 46 per million in North America and Western Europe.4, 5 Nowadays, there are large numbers of patients with TSCI in Anhui Province, China. Most recent studies have focused on the role of surgical reduction and decompression,6 but analyses on epidemiological features of TSCI in China are minimal, and the prevention efforts and treatment levels are relatively backward. Epidemiologic studies identify high-risk groups and provide useful information for prevention efforts. It is, therefore, imperative to conduct epidemiologic studies of TSCI in order to formulate corresponding intervention strategies to epidemiological features. In this study, we outlined the epidemiological features of TSCI, which included age, gender, cause, occupation, neurological level and severity of injury at admission, treatment and so on. The results of this study will serve as a base for design prevention strategies and epidemiological studies in order to reduce the number of patients with TSCI.
Patients and methods
Anhui is located in eastern China and occupies an area of approximately 140 000 km2. The population is 59.5 million, of which 51.6% are male (from the sixth time population census in 2010).7 There are more than twenty hospitals in the region. The two hospitals cover the whole population in the region and, from incidence in other China studies,8, 9 it is estimated that >20% of people with TSCI are treated in the two hospitals in Anhui Province every year. We identified all cases of TSCI from review of hospital charts by two students, including age, gender, cause, occupation, neurological level of injury, spinal level of injury, American Spinal Injury Association (ASIA) impairment scale (AIS) AIS and treatment. The inclusion criteria for the study were: (1) spinal cord injuries or cauda equina injuries of traumatic origin, and (2) Anhui residency at the time of injury. This study excludes intervertebral disc disease, vertebral injuries in the absence of TSCI and fatally injured persons who were never hospitalized. The inclusion criteria was correspond with the World Health Organization’s International Classification of Diseases, Ninth revision, Clinical Modification diagnostic codes 952 × (spinal cord injury without evidence of spinal bone injury) and 806 × (fracture of vertebral column with spinal cord injury).10 Neurologic deficits were classified according to the level of injury and severity using the AIS for spinal cord injury.11 Seven hundred and sixty one cases were included from two hospitals, admitted between 1 January 2007 and 31 December 2010 in Anhui Province, China.
The quantitative database was set up by using EpiData3.1 (EpiData foreningen (EpiData Association), Odense, Denmark). Data were double entered by two students separately and then cross-checked two times to assure data accuracy of the data. The database was analyzed by using SPSS 12.0 (SPSS Inc., Chicago, IL, USA).
Results
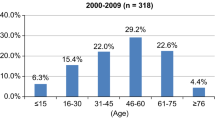
Age and gender
The data of 761 TSCI patients were analyzed. The number has increased in the 4 years (2007:170, 2008:193, 2009:191, 2010:207). Among 761 patients, 588 were males and 173 were females, with a mean age of 45 years (s.d.=13, range from 5 to 87). (Table 1).
Cause of injury
Among males, fall from height was the leading cause of injury in all age groups (Table 2), with a peak in the 31–45 and 46–60 age groups, which was the same to the results among females, but the number of fall from height patients in males was more than those in females in all age groups. Furthermore, fall from height was more likely to result in fracture (based on ICD9 codes 806) in TSCI patients compared with the other etiologies (χ2=18.365, P=0.001, degrees of freedom=4).
Neurological level and severity of injury
The proportion of AIS A among thoracic injury was higher than the proportion among cervical or lumbar injury (Figure 1). The most common fracture levels were at C5, C6, T12, L1 and L2, accounting for 10.6%, 11.2%, 9.4%, 15.9% and 7.8%, respectively, and spinal dislocation occurred mainly in C4/C5, C5/C6 and C6/C7, accounting for 11.9%, 25.0% and 19.6% respectively. The spinal fracture (based on ICD9 codes 806) was significantly associated with severity of injury (χ2=10.947, P=0.012, degrees of freedom =3). AIS A was significantly more common in patients with fracture.

AIS of TSCI classified by neurological level of TSCI.
Concomitant injuries
The detailed review of records showed the most common concomitant injuries were head injuries (66 patients), followed by limb or pelvic fractures (50 patients), fractures of ribs (43 patients), and others such as clavicular fractures, fractures of scapula, sternal fractures and hemopneumothorax (36 patients). Transport, struck by object and fall from height were more likely to result in concomitant injuries in TSCI patients compared with the other causes (χ2=9.934, P=0.042, degrees of freedom=4).
Time and treatment conditions
The time from trauma to admission ranged between 1and 984 h (median=11.5), during this time, some patients may be in an ambulance, and the others may be in other hospitals, which did not have as advanced medical equipments. The length of hospital stay ranged between 1 and 80 days (median=17). Ninety-seven patients received conservative treatment, and 544 patients received surgery treatment, and the other patients left hospital against medical advice. A total of 10 patients died in hospital, and the average time from admission to death was 16 days.
Discussion
To our knowledge, this is the first study on TSCI in Anhui Province from the epidemiological perspective. This study examined the epidemiological characteristics of TSCI over a 4-year period in two hospitals. In this survey, there were 435 farmers and 168 laborers. Their relatively low educational background limited them to do physically demanding work, left them more susceptible to getting TSCI, which may result in the increased number in the 4 years period. Transport, including driving, riding bicycle, was the second most common cause of injury, which is similar to other surveys.12, 8 Conversely, transport was the primary cause in Greece and Canada,13, 14 which could be explained by a lower number of motor vehicles in Anhui Province.
The gender distribution (men/women) of TSCI was 3.4/1, which was similar to other studies, and their gender distribution ranged from 3.0/1–4.8/1.15, 16 It could be explained by risk-taking behaviors men performed. The highest number for both male and female were in 31–45 and 46–60 age groups, whereas the peak age in other reports range from 15 to 30.17, 18 This may be because people in their 15–30s in western countries were more aggressive in sports, and Chinese people in their 31–60s had to bear financial responsibility, so they would work harder than others, which made them easily get TSCI, especially when working on construction areas.
The most common level of fracture seen in our study were at C5–C6 and T12–L2, and spinal dislocation occurred mainly at C4/C5 C5/C6 and C6/C7. So corresponding cervical and lumbosacral neurological level injuries were very high in this survey, which has also been proved by other reports.9, 19 Siebenga et al.20 similarly reported that the majority of the fractures (78%) were seen at the thoracolumbar junction Th11-L2. Although there could have been a higher pressure on these segments than other segments, the thoracolumbar spine proved to be more stable than cervical spine. The proportion of AIS A among thoracic injury was higher than the proportion among cervical or lumbar injury, which may be explained by a thoracic spinal stenosis.
Several limitations need to be discussed. First, China does not currently have a national SCI register system, and there are definitely not enough TSCI epidemiology researches available, and the identification of patients was based on review of hospital charts by two students. Second, our study was retrospective, so at that time registrars may not accurately record the information. Some patients may have received a diagnostic code that did not suggest a TSCI, and some patients with minor neurological deficits may not have been diagnosed. Third, we excluded all fatalities that occurred on the way to hospital. Finally, it is regretful that no follow-up work was done.
DATA ARCHIVING
There were no data to deposit.
References
New PW . Functional outcomes and disability after nontraumatic spinal cord injury rehabilitation: results from a retrospective study. Arch Phys Med Rehabil 2005; 86: 250–261.
Ackery A, Tator C, Krassioukov A . A global perspective on spinal cord injury. J Neurotrauma 2004; 21: 1355–1370.
DeVivo MJ . Causes and costs of spinal cord injury in the United States. Spinal Cord 1997; 35: 809–813.
Cripps RA, Lee BB, Wing P, Weerts E, Mackay J, Brown D . A global map for traumatic spinal cord injury epidemiology: towards a living data repository for injury prevention. Spinal Cord 2011; 49: 493–501.
Wyndaele M, Wyndaele JJ . Incidence, prevalence and epidemiology of spinal cord injury: what learns a worldwide literature survey? Spinal Cord 2006; 44: 523–529.
Fehlings MG, Sekhon LH, Tator C . The role and timing of decompression in acute spinal cord injury: what do we know? what should we do? Spine 2001; 26: S101–S110.
StatisticsAnhui. Statistical Yearbook of Anhui 2011. Statistics Anhui; Anhui, China, 2011.
Li J, Liu G, Zheng Y, Hao C, Zhang Y, Wei B . The epidemiological survey of acute traumatic spinal cord injury (ATSCI) of 2002 in Beijing municipality. Spinal Cord 2011; 49: 777–782.
Ning GZ, Yu TQ, Feng SQ, Zhou XH, Ban DX, Liu Y et al Epidemiology of traumatic spinal cord injury in Tianjin, China. Spinal Cord 2011; 49: 386–390.
Hagen EM, Rekand T, Gilhus NE, Gronning M . Diagnostic coding accuracy for traumatic spinal cord injuries. Spinal Cord 2009; 47: 367–371.
Kirshblum SC, Burns SP, Biering-Sorensen F, Donovan W, Graves DE, Jha A et al International standards for neurological classification of spinal cord injury. J Spinal Cord Med 2011; 34: 535–546.
Hagen EM, Eide GE, Rekand T, Gilhus NE, Gronning M . A 50-year follow-up of the incidence of traumatic spinal cord injuries in Western Norway. Spinal Cord 2010; 48: 313–318.
Divanoglou A, Levi R . Incidence of traumatic spinal cord injury in thessaloniki, greece and stockholm, sweden: a prospective population-based study. Spinal Cord 2009; 47: 796–801.
Pickett GE, Campos-Benitez M, Keller JL, Duggal N . Epidemiology of traumatic spinal cord injury in Canada. Spine 2006; 31: 799–805.
Ahoniemi E, Alaranta H, Hokkinen EM, Valtonen K, Kautiainen H . Incidence of traumatic spinal cord injuries in Finland over a 30-year period. Spinal Cord 2008; 46: 781–784.
Dahlberg A, Kotila M, Leppanen P, Kautiainen H, Alaranta H . Prevalence of spinal cord injury in helsinki. Spinal Cord 2005; 43: 47–50.
Dryden DM, Saunders LD, Rowe BH, May LA, Yiannakoulias N, Svenson LW et al The epidemiology of traumatic spinal cord injury in Alberta, Canada. Can J Neurol Sci 2003; 30: 113–121.
McCammon JR, Ethans K . Spinal cord injury in Manitoba: a provincial epidemiological study. J Spinal Cord Med 2011; 34: 6–10.
Lin CY, Wright J, Bushnik T, Shem K . Traumatic spinal cord injuries in horseback riding: a 35-year review. Am J Sports Med 2011; 39: 2441–2446.
Siebenga J, Segers MJ, Elzinga MJ, Bakker FC, Haarman HJ, Patka P . Spine fractures caused by horse riding. Eur Spine J 2006; 15: 465–471.
Acknowledgements
We thank the First Affiliated Hospital of Anhui Medical University and Anhui Provincial Hospital that allowed us access to patient data, Professor Faming Pan and Professor XiuJun Zhang for help and advice.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article
Cite this article
Wang, H., Yin, Z., Chen, Y. et al. Epidemiological features of traumatic spinal cord injury in Anhui Province, China. Spinal Cord 51, 20–22 (2013). https://doi.org/10.1038/sc.2012.92
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sc.2012.92
Keywords
This article is cited by
-
Epidemiology features of traumatic and non-traumatic spinal cord injury in China, Wuhan
Scientific Reports (2024)
-
Epidemiological features of traumatic spinal cord injury in Wuhan, China
Journal of Orthopaedic Surgery and Research (2023)
-
A systematic review and meta-analysis of the global epidemiology of pediatric traumatic spinal cord injuries
European Journal of Pediatrics (2023)
-
Epidemiological profile of 338 traumatic spinal cord injury cases in Shandong province, China
Spinal Cord (2022)
-
Epidemiological characteristics of spinal cord injury in Northwest China: a single hospital-based study
Journal of Orthopaedic Surgery and Research (2020)
