
Abstract
Study design:
A formal decision-making and consensus process integrating evidence gathered from preparatory studies was followed.
Objectives:
The aim of this study was to report on the results of the consensus process to develop the first version of a Comprehensive International Classification of Functioning, Disability and Health (ICF) Core Set and a Brief ICF Core Set for individuals with spinal cord injury (SCI) in the early post-acute context.
Setting:
The consensus conference took place in Switzerland. Preparatory studies were performed worldwide.
Methods:
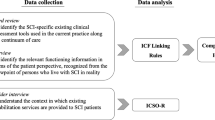
Preparatory studies included an expert survey, a systematic literature review, a qualitative study and empirical data collection involving people with SCI. ICF categories were identified in a formal consensus process by international experts from different backgrounds.
Results:
The preparatory studies identified a set of 531 ICF categories at the second, third and fourth levels. From 30 countries, 33 SCI experts attended the consensus conference (11 physicians, 6 physical therapists, 5 occupational therapists, 6 nurses, 3 psychologists and 2 social workers). Altogether 162 second-, third- or fourth-level categories were included in the Comprehensive ICF Core Sets with 63 categories from the component Body Functions, 14 from Body Structures, 53 from Activities and Participation and 32 from Environmental Factors. The Brief Core Set included a total of 25 second-level categories with 8 on Body Functions, 3 on Body Structures, 9 on Activities and Participation, and 5 on Environmental Factors.
Conclusion:
A formal consensus process-integrating evidence and expert opinion based on the ICF led to the ICF Core Sets for individuals with SCI in the early post-acute context. Further validation of this first version is needed.
Similar content being viewed by others


Introduction
Spinal cord injuries (SCIs) occur unexpectedly. Common activities such as driving a car, diving into a lake or walking downstairs can suddenly result in an injury totally reconfiguring the realities of daily life. Because all organ systems and body functions below the level of the neurological lesion may be affected, SCI often requires major physical, psychological and social adaptations from injured people and their families.1
Timely and appropriate medical and rehabilitative interventions are essential factors affecting functional recovery in traumatic SCI. Following a patient's acute care, early post-acute rehabilitation should be started as soon as possible.2 It aims at improving functional outcomes and tends to hasten and promote improvements in the activities of daily living.3 Reaching this goal, however, requires an in-depth understanding of the broad range and interaction of functional problems people with SCI may experience.
The International Classification of Functioning, Disability and Health (ICF)4 provides a comprehensive and universally accepted framework to classify and describe functioning, disability and health in people with all kinds of diseases or conditions, including SCI. According to the ICF, the problems associated with a disease may involve body functions and body structures and the activities and participation in life situations. Health states and the development of disability are modified by contextual factors such as environmental and personal factors.4 The ICF is structured hierarchically. Categories are divided into chapters, which constitute the first level of precision. Categories on higher levels (for example, third or fourth level) are more detailed. To give an example, the third-level ICF category b7303 Power of muscles in lower half of the body is one element of the second-level category b730 Muscle power functions and is indicated by the last digit ‘3’. The second-level category b730 Muscle power functions is an element of Chapter b7 Neuromusculoskeletal and movement-related functions. Finally, Chapter b7 Neuromusculoskeletal and movement-related functions is part of the ICF component b Body Functions. Supplementary information about the ICF model and structure is provided on the journals website.
Because the ICF can serve as the basis for a comprehensive and detailed understanding of functioning and disability, it is essential in a first step to identify which aspects of functioning and disability in people with SCI should be defined. This process is consistent with the approach that has been followed in other health conditions. Selections of ICF categories relevant for people with a specific health condition, so-called ‘ICF Core Sets’, have already been developed for a number of health conditions.5 However, in SCI different contexts have to be taken into account.
Because an ‘ICF Core Set for Neurological Conditions in the Acute Context’ was already developed6 and is currently being validated, the project aimed at developing ICF Core Sets for SCI for the early post-acute context and for the long-term context.7 The early post-acute context covers the first comprehensive rehabilitation after the acute SCI. The long-term context follows the early post-acute context. This definition was regarded as being applicable throughout the world irrespective of the different health systems. The Core Sets should cover both traumatic and nontraumatic SCI.
The development process of the ICF Core Sets for SCI is divided in a preparatory phase in which information was gathered from different studies and a final consensus conference.7 The objective of this paper was to report on the results of the consensus process-integrating evidence from preparatory studies to develop the Comprehensive ICF Core Set for SCI in the early post-acute context and the Brief ICF Core Set for SCI in the early post-acute context.
Methods
A formal decision-making and consensus process-integrating evidence was gathered from preparatory studies and expert opinion was followed.
Preparatory studies
The conference was based on the data available as on 1 October 2007. The preparatory studies included an empirical data collection applying the second-level ICF categories in 361 people with SCI in clinical rehabilitation from 14 countries, an internet-based expert survey including 144 SCI health professionals worldwide, a systematic literature review on outcomes used in 281 SCI empirical studies and a qualitative study including 21 focus groups with people with SCI from 6 countries. On the basis of these preparatory studies, a preselection of ICF categories was performed using the modified Scree test8 that facilitates priority determination based on a graphical examination of the frequency distribution. The ICF categories most frequently named in all four preparatory studies made up the starting point of the decision-making and consensus process. Details of the preparatory studies are described in the reference publications.9, 10, 11, 12
Recruitment of conference participants
Health professionals who expressed their interest in the project in advance as well as people who were suggested by the project steering committee constituted the pool of potential participants. A total of 154 people (58 physicians, 24 physical therapists, 27 occupational therapists, 23 nurses, 12 psychologists and 10 social workers from 38 countries) made up this pool. Participants were selected randomly under consideration of the profession and the country of origin to assure a most balanced representation of all important health professions and all world regions.
Training and information exchange
During the conference, the first meeting consisted of a 3 h training, in which all participants were familiarized with the ICF framework and classification,4 and were informed about the evidence from the preparatory studies. They were provided with summary sheets containing both the preselected ICF categories and the results of the preparatory studies (see Table 1).
Iterative decision-making process
The ICF Core Set categories were identified in an iterative decision-making process with discussions and voting in working groups and plenary sessions. The process was guided by a member of the ICF Research Branch (AC). In the process, ICF categories that were either clearly relevant or irrelevant according to preset decision rules were excluded from further discussion. The focus on the remaining controversial categories was thereby facilitated. The decision-making process consisted of two major activities.
In the first activity, the participants were asked to select ICF categories to be included in the Comprehensive ICF Core Set, that is, a list of ICF categories long enough to describe the prototypical spectrum of limitations in functioning and health of people with SCI in the early post-acute context, but at the same time short enough to be practical in comprehensive, multidisciplinary assessments.
In the second activity, the participants were requested to select the Brief ICF Core Set from the list of ICF categories included in the Comprehensive ICF Core Set by means of a two-round ranking procedure and a final vote. The Brief ICF Core Set is a list of ICF categories long enough to describe the prototypical spectrum of limitations in functioning and health of people with SCI in the early post-acute context, but at the same time short enough to be practical in clinical studies.
The data resulting from the voting and ranking processes were continuously entered in MS Excel 2003 throughout the conference.
Results
Preparatory studies
In the empirical study, 222 second-level categories were identified. The qualitative study, the expert survey and the systematic review revealed 326, 366 and 424 second-, third- and fourth-level categories, respectively. In total, a list of 273 different second-level categories resulted from the preparatory studies. Using a modified Scree test, we selected the 215 most frequently reported categories.8 The list of ICF categories finally presented at the conference to the participants included 531 ICF categories at the second, third or fourth level (104 on Body Functions, 90 on Body Structures, 220 on Activities and Participation and 117 on Environmental Factors).
ICF consensus conference
The consensus process took place from 15 to 18 November 2007 at the Swiss Paraplegic Research, Nottwil, Switzerland. Thirty-three health professionals (11 physicians with various subspecializations, 6 physical therapists, 5 occupational therapists, 6 nurses, 3 psychologists and 2 social workers) from 30 different countries attended the consensus process for SCI in the early post-acute context. Two of them had an SCI. The decision-making process involved five working groups with six to seven health professionals each. The process was facilitated by the moderator of the plenary sessions (AC) and leaders of the five working groups.
Comprehensive Core Set
Tables 2, 3, 4 and 5 show the ICF categories included in the Comprehensive ICF Core Set. The number of second-, third- and fourth-level categories in the Comprehensive ICF Core Set is 162, with 104 categories on the second level, 49 categories on the third level and 9 categories on the fourth level. The 58 third- and fourth-level categories are a further specification of 14 categories on the second level.
The 162 categories of the Comprehensive ICF Core Set are made up of 63 (38.9%) categories from the component Body Functions, 14 (8.6%) from the component Body Structures, 53 (32.7%) from the component Activities and Participation and 32 (19.8%) from the component Environmental Factors.
All chapters of the component Body Functions are represented in the Comprehensive ICF Core Set. From the component Body Structures Chapter 2 The eye, ear and related structures, Chapter 3 Structures involved in voice and speech and Chapter 5 Structures related to the digestive, metabolic and endocrine systems are not represented in the Comprehensive ICF Core Set. From the components Activities and Participation and Environmental Factors, respectively, all chapters are represented in the Comprehensive ICF Core Set except Chapter 1 Learning and applying knowledge and Chapter 2 Natural environment and human-made changes of environment, respectively.
Brief Core Set
Table 6 shows the second-level ICF categories ordered by rank that were selected for the Brief ICF Core Set. The Brief ICF Core Set includes a total of 25 second-level categories, which represents 24% of all second-level categories that were selected for the Comprehensive Core Set. Eight categories were chosen from the component Body Functions (representing 22% of selected second-level categories in the Comprehensive Core Set), three from Body Structures (representing 33% of selected second-level categories in the Comprehensive Core Set), nine from Activities and Participation (representing 33% of selected second level-categories in the Comprehensive Core Set) and five from Environmental Factors (representing 16% of selected second-level categories in the Comprehensive Core Set).
Discussion
The formal consensus process-integrating evidence from preparatory studies and expert knowledge at the ICF Core Set conference for SCI led to the definition of a Comprehensive ICF Core Set for SCI in the early post-acute context for multidisciplinary assessment and a Brief ICF Core Set for SCI in the early post-acute context for clinical studies.
The 162 categories (104 second-level categories) that were included in the Comprehensive Core Set reflect the numerous functional changes that occur in people with SCI in the early post-acute context. Because the ICF Core Set should be applied for all levels of spinal cord lesions, a wide range of functional problems was included in the Comprehensive Core Set. Despite keeping in mind that the Comprehensive ICF Core Set should include as many categories as necessary to comprehensively describe functioning in patients with SCI, but as few as possible to be practical, the participants frequently felt that a specific description of a problem is necessary. Thus, they included many third-level and even fourth-level categories that provide specifications of second-level categories such as b280 Pain, s120 Spinal cord and related structures or d445 Hand and arm use.
With respect to the four main components of the ICF, the following issues were raised:
About one-half of the second-level ICF categories of the component Body Functions were included in the first vote with a 100% agreement among the participants. These categories address functions typically problematic in people with SCI, such as pain, touch function, blood pressure function, defecation function, urination function, muscle power function and muscle tone function.13, 14, 15
A major point of discussion was the inclusion of the categories b110 Consciousness functions, b114 Orientation functions, b140 Attention functions and b144 Memory functions. These ICF categories were found to be related primarily to comorbid traumatic brain injury16 and consequently were excluded.
The category b126 Temperament and personality functions was discussed controversially and finally included with a high agreement. The most important argument was the participants’ experience that a persons’ personality may influence the rehabilitation and the level of participation in a positive or negative way. On the other hand, the argument came up that a persons’ personality is not influenced by the SCI itself and therefore should not be included in the ICF Core Set. In addition, it was discussed to what extent personality is a persons’ characteristic that should be assigned to the ICF component Personal Factors rather than to Body Functions.
The category b152 Emotional functions was included in the Comprehensive ICF Core Set referring to the high amount of newly injured people who meet the diagnostic criteria for depression.17
The discussion led to an exclusion of b330 Fluency and rhythm of speech functions on the one hand. On the other hand, the participants agreed that problems with voice functions should be addressed in the Comprehensive ICF Core Set using a more general ICF category. Although not included in the list of candidate categories, the ICF category b310 Voice functions was additionally selected and included in the Comprehensive ICF Core Set.
Regarding neuromusculoskeletal functions all candidate categories were included except b720 Mobility of bone functions that overlaps with other already included categories and was regarded as not being primarily important in the early post-acute phase.
The participants decided to include almost all third-level specifications of b730 Muscle power functions. The inclusion of b7201 Power of muscles of one limb was intensively discussed by the participants. Some participants felt that this category could be useful to describe Brown-Séquard syndrome. On the other hand, many participants argued that in the clinical examination all limbs will be screened and therefore this category is already covered by other categories. Finally, all participants agreed to exclude the category.
The selection of all four candidate ICF categories related to functions of skin underlines the importance of impaired skin function and the risk of pressure sores in people with SCI.18
The selection of Body Structures included those structures that are mainly affected by SCI, such as spinal cord, respiratory and urinary systems, upper and lower extremities, trunk, head and neck region, shoulder region and pelvic region and skin.3 The structures of the sympathetic and parasympathetic nervous system were finally excluded because the corresponding body functions are already represented in the Comprehensive ICF Core Set.
A broad range of categories of the ICF component Activities and Participation was selected by the participants reflecting the diversity of problems associated with SCI. The inclusion of many third-level categories of Chapter 4 Mobility highlights the need for a detailed description of mobility problems by health professionals.
The candidate categories addressing education as well as work and employment were predominantly regarded as less relevant for persons with SCI in the early post-acute phase and were excluded from the Comprehensive ICF Core Set. However, some participants reported that aspects of work and employment are addressed very early in SCI rehabilitation in their countries and voted for the inclusion of the category d850 Remunerative employment. Finally, this category was included with an agreement of 59% among the participants.
Regarding Environmental Factors there was a general agreement that the support provided by the family, friends and care providers as well the their attitudes have a considerable impact on the functioning of people with SCI in the early post-acute phase and therefore corresponding ICF categories should be considered in the Core Set.
Although the relevance and applicability specifically of those categories that are assigned to Chapter 5 Services, Systems and Policies may vary across countries and cultures, the participants were able to agree on the most important categories and selected seven categories out of this chapter.
The Brief ICF Core Set includes 25 second-level categories that were selected out of the second-level categories of the Comprehensive ICF Core Set using a two-step ranking procedure and a final cutoff decision. The spectrum and number of ICF categories included in the Brief ICF Core Set seem to fulfill the needs of single health professions who want to get a brief profile of functional problems of a person with SCI. In specific cases when the information provided by categories of the Brief Core Set is not sufficient, additional categories out of the Comprehensive Core Set can be chosen. This method of applying the Brief Core Set can also compensate the loss of presentation of several chapters in the Brief Core Set that is associated with the reduction of the number of categories. Although the chapters of the component Body Functions are represented in the Brief Core Set with only one exception, two or more chapters are not included from the remaining components.
It is striking that the component Activities and Participation is represented by a considerable number of categories that exclusively pertain to Chapter 4 Mobility and Chapter 5 Self-Care. During the ranking procedure, it became clear that it was difficult for the participants to put these categories into a rank order because they were missing arguments for, for example, preferring d550 Eating to d560 Drinking. The idea came up to include these items on the chapter level. The participants who supported this proposal emphasized that other ICF categories with lower rank such as d465 Moving around using equipment could be included in this case. However, other participants pointed out that a judgment on the chapter level would be too unspecific and less useful. Finally, 53% of the participants refused this proposal. As a consequence, d465 Moving around using equipment is not included in the Brief Core Set although wheelchair driving may be an important goal of the early post-acute rehabilitation phase.19
Some more general limitations of the consensus conference should be mentioned. The participants consisted of SCI health professionals of whom two were affected by an SCI. Therefore, a poor representation of consumers could be criticized. Furthermore, the majority of participants came from industrialized countries and as a consequence the perspective of developing countries may not be sufficiently considered in the ICF Core Sets for SCI.
Validation studies will provide further information about the content validity of the ICF Core Sets for SCI. They will also show whether specific subsets of people with SCI, for example those with paraplegia versus tetraplegia or complete versus incomplete lesion will differ. Besides validation, strategies for the implementation of the ICF Core Sets for SCI in clinical practice are currently developed. Using case studies of individuals with SCI, the application of the ICF Core Sets for SCI in rehabilitation practice is presented on website http://www.ICF-casestudies.org. In addition, a handbook for users will be developed. Also, content comparisons of the ICF Core Sets proposed in this paper with other ICF Core Sets, such as the ICF Core Sets for stroke, are being performed. Those comparisons will help to describe the content validity of the different Core Sets. Finally, because the ICF Core Sets for SCI define which areas of functioning should be measured but not how they should be measured, an operationalization of the ICF categories included in the ICF Core Sets for SCI would be useful. The International SCI Data Sets may complement the ICF Core Sets for SCI on this point because they provide specific information about how the relevant information could be assessed.20
In conclusion, a formal consensus process-integrating evidence and expert opinion based on the ICF framework and classification led to the definition of ICF Core Sets for SCI in the early post-acute context. Both the Comprehensive Core Set for multidisciplinary, comprehensive assessment and the Brief Core Set for research and clinical practice are preliminary and need to be tested and validated in the coming years with the ultimate goal of finally defining a universal, valid and accepted tool for clinical practice, clinical studies and health reporting.
Postscript
Professor Haim Ring (Julio Ring), our friend and colleague and author of this paper, died on 15 September 2008. Haim always supported and motivated the process of developing ICF Core Sets. He built bridges among disciplines and health professions. He also brought world regions and countries to work together. We will always be endlessly thankful for having the opportunity of being close to this inspiring spirit.
References
Kennedy P, Lude P, Taylor N . Quality of life, social participation, appraisals and coping post spinal cord injury: a review of four community samples. Spinal Cord 2006; 44: 95–105.
Scivoletto G, Molinari M, Molinari M . Early versus delayed inpatient SCI rehabilitation: an Italian study. Arch Phys Med Rehabil 2005; 86: 512–516.
Sumida M, Fujimoto M, Tokuhiro A, Tominaga T, Magara A, Uchida R . Early rehabilitation effect for traumatic spinal cord injury. Arch Phys Med Rehabil 2001; 82: 391–395.
World Health Organization. International Classification of Functioning, Disability and Health (ICF). WHO: Geneva, 2001.
Cieza A, Ewert T, Üstün B, Chatterji S, Kostanjsek N, Stucki G . Development of ICF Core Sets for patients with chronic conditions. J Rehabil Med 2004; 44: 9–11.
Ewert T, Grill E, Bartholomeyczik S, Finger M, Mokkrusch T, Kostanjsek N et al. ICF Core Sets for patients with neurological conditions in the acute hospital. Disability Rehab 2005; 27: 367–373.
Biering-Sørensen F, Scheuringer M, Baumberger M, Charlifue SW, Post MWM, Montero F et al. Developing core sets for persons with spinal cord injury based on the international classification of functioning, disability and health as a way to specify functioning. Spinal Cord 2006; 44: 541–546.
Zoski K, Jurs S . Priority determination in surveys. An application of the Scree test. Eval Rev 1990; 14: 214–219.
Scheuringer M, Kirchberger I, Boldt C, Hoogland-Eriks I, Rauch A, Velstra I-M et al. Identification of problems in individuals with spinal cord injury from the health professional perspective using the ICF: a worldwide expert survey. Spinal Cord, (submitted).
Post M, Kirchberger I, Scheuringer M, Wollaars MM, Geyh S . Systematic review of concepts used in studies of individuals with spinal cord injury using the International Classification of Functioning, Disability and Health as a reference. Spinal Cord, (submitted).
Kirchberger I, Sinnott A, Charlifue S, Kovindha A, Lüthi H, Campbell R et al. Problems in individuals with spinal cord injury from the consumer perspective: a worldwide qualitative study using the ICF. Spinal Cord, (Submitted).
Kirchberger I, Biering-Sørensen F, Charlifue S, Baumberger M, Campbell R, Kovindha A et al. Identification of problems in individuals with spinal cord injury using the ICF: a worldwide empirical study. Spinal Cord (e-pub ahead of print 15 September 2009).
Lynch AC, Wong C, Anthony A, Dobbs BR, Frizelle FA . Bowel dysfunction following spinal cord injury: a description of bowel function in a spinal cord-injured population and comparison with age and gender matched controls. Spinal Cord 2000; 38: 717–723.
Ullrich PM, Jensen MP, Loeser JD, Cardenas DD . Pain intensity, pain interference and characteristics of spinal cord injury. Spinal Cord 2008; 46: 451–455.
Claydon VE, Steeves JD, Krassioukov A . Orthostatic hypotension following spinal cord injury: understanding clinical pathophysiology. Spinal Cord 2006; 44: 341–351.
Macciocchi SN, Bowman B, Coker J, Apple D, Leslie D . Effect of co-morbid traumatic brain injury on functional outcome of persons with spinal cord injuries. Arch Phys Med Rehabil 2004; 83: 22–26.
Kishi Y, Robinson RG, Forrester AW . Prospective longitudinal study of depression following spinal cord injury. J Neuropsychiatry Clin Neurosci 1994; 6: 237–244.
Fuhrer MJ, Garber SL, Rintala DH, Clearman R, Hart KA . Pressure ulcers in community-resident persons with spinal cord injury: prevalence and risk factors. Arch Phys Med Rehabil 1993; 74: 1172–1177.
Knapik H . The modern rehabilitation of patients with spinal cord injuries. Ortop Traumatol Rehabil 2004; 6: 509–522.
Biering-Sørensen F, Charlifue S, DeVivo M, Noonan V, Post M, Stripling T et al. International spinal cord injury data sets. Spinal Cord 2006; 44: 530–534.
Acknowledgements
This project was funded by Swiss Paraplegic Research, Nottwil, Switzerland. We are grateful for the contributions made by the following experts attending the consensus conference: Lindsay Alford, Lester Butt, Sam S Chan, Guido Deckstein, Wagih El-Masry, Fazlul Hoque, Georgina Ilosvai, Alvydas Juocevicius, Ann-Katrin Karlsson, Shinsuke Katoh, Sanna Koskinen, Klaus Krogh, Jianan Li, Kwan-Hwa Lin, Ana Cristina Mancussi e Faro, Charles Manise, Karen Marshall, Tlhaloganyo Mbalambi, Yuri Moustafaev, Dominick Michael Mshanga, Diana Nix, Ali Otom, Inder Perkash, Kiley Pershouse, Manoj Ranabhat, Gail Richmond, Lalita Thambi, Ha Van Than, Jose M Tormos Munoz, Pat Tracy, Lizelle van der Vyver, Renata Vaughan and Tamara Zamparo. Our special thanks to Monika Scheuringer who was the international coordinator of the preparatory studies for her extraordinary commitment. We thank the working group assistants Jennifer Dunn, Helga Lechner, Hansjörg Lüthi, Joanne Nunnerley and Manuel Zwecker for their support. We also thank Silvia Neubert, Heinrich Gall, Sven Becker, Andreas Leib, Elisabeth Linseisen and Christine Boldt for their invaluable support during the conference.
Author information
Authors and Affiliations
Corresponding author
Additional information
Supplementary Information accompanies the paper on the Spinal Cord website .
Supplementary information
Rights and permissions
About this article
Cite this article
Kirchberger, I., Cieza, A., Biering-Sørensen, F. et al. ICF Core Sets for individuals with spinal cord injury in the early post-acute context. Spinal Cord 48, 297–304 (2010). https://doi.org/10.1038/sc.2009.128
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sc.2009.128
Keywords
This article is cited by
-
A postpartum functional assessment tool for women based on the international classification of functioning, disability and health
BMC Women's Health (2024)
-
Content validity of the Work Rehabilitation Questionnaire (WORQ) for persons with spinal cord injury: A mixed methods study
Spinal Cord (2022)
-
Utilising International Statistical Classification of Diseases and Related Health Conditions (ICD)-10 Australian Modification Classifications of “Health Conditions” to Achieve Population Health Surveillance in an Australian Spinal Cord Injury Cohort
Spinal Cord (2022)
-
Standard set of network outcomes for traumatic spinal cord injury: a consensus-based approach using the Delphi method
Spinal Cord (2022)
-
Recommendations for standards of physiotherapy care following complete traumatic paraplegia in India
Spinal Cord Series and Cases (2020)
