
Abstract
Study design:
Case report.
Objective:
To describe a rare case of paraplegia in a patient with Scheuermann's disease and dysplastic thoracic spinous processes.
Setting:
Spinal Cord Injury Center, Orthopaedic University Hospital Heidelberg, Heidelberg, Germany.
Clinical presentation:
The authors report on a 15-year-old boy with progressive incomplete spastic paraplegia presenting segmental dysplastic thoracic spinous processes and Scheuermann's disease. The magnetic resonance imaging showed a kyphotic angulation at T 5/6 and signs of myelopathy. Hypoplastic thoracic processes and hypoplastic paraspinal muscles in the upper thoracic spine were observed intraoperatively. In this case, dorsoventral stabilization from T 4–7 was performed and the neurological outcome improved at follow-up (6 months).
Conclusion:
Paraplegia can be accelerated in patients with Scheuermann's disease, severe kyphotic angulation and dysplastic posterior elements. After operative treatment, neurological recovery and a normal walking pattern were shown.
Similar content being viewed by others

Introduction
Sharp-angle kyphosis may be congenital, traumatic, degenerative, infectious or iatrogenic in origin.1 A short-segmented thoracic kyphosis and Scheuermann's disease can lead to progression in the angulation of the hyperkyphotic segment and constitutes a weak point for spinal cord compression, which is multifactorially influenced. We present a rare case of progredient spastic paraplegia in a 15-year-old boy with Scheuermann's disease associated with a short-segmented kyphotic angulation.
Case report
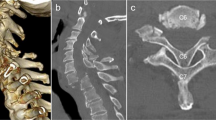
A 15-year-old boy in good health, who had had a minor trauma (sledge accident) with contusion of his back 18 months ago, was admitted to our hospital with progressive sensorimotor deficits in his left leg that began 3 months ago. The boy reported that while he was sitting on the sledge, he glided backwards and fell on his back. There were no neurological signs present immediately after this trauma. On admission, the patient reported a progressive disturbance of equilibrium with a tendency to stumble, as well as rapid fatigue during physical activity. At birth (31st week of gestation) his mother suffered from HELLP (haemolysis-elevated liver enzymes-low platelet count) syndrome and prenatal asphyxia necessitated artificial ventilation for 3 days. Physical examination found a sharply wedged kyphotic deformity of the upper thoracic spine with a fixed, short-segmented gibbus, a left convex thoracic scoliosis and a hyperlordosis of the lumbar spine. The initial neurological examination revealed an incomplete paraplegia with a neurological level at T5 (ASIA D). Routine haematological and electrolyte investigations were normal. X-rays showed a sharp and short-segmented kyphosis with the apex located at T5–6 and a sagittal angle from T3–8 of 65°. Computerized tomography scanning showed osteochondrotic, signs irregularities of the T4, 5 and 6 endplates with trapezoid deformity of the vertebral bodies, decreased vertebral disc height comparable with Scheuermann's disease and flattened hypoplastic spinous processes from T4–7 (Figure 1). Additional information from the magnetic resonance imaging showed a ventral tensed spinal cord above the apex of the kyphosis at T5–6 corresponding to the neurological findings (Figures 2a and b). The urodynamic examination revealed a hyposensitive, normotonic bladder with normocontractile detrusor muscle activity and a residual urine volume of 200 ml. The patient underwent osteodiscectomie T5–6 and ventral stabilization accompanied by dorsal spondylodesis T4–7 (Expedium Titan, Depuy Spine, Johnson & Johnson, Kirkel-Limbach, Germany). Intraoperatively, the incidental finding of hypoplastic spinous processes T4–7 measuring 1 cm, as well as hypoplastic paraspinal muscles in the upper thoracic vertebral spine was confirmed. The patient's progress was uncomplicated and mobilization was allowed without orthosis. The neurological examination revealed ASIA D and normal bladder function. Although the thoracic kyphotic angle (63°) showed only slight improvement at the 6 months follow-up, the sensomotoric function was maintained (Figure 3).

Sagittally formatted computerized tomography of the kyphotic upper thoracic spine shows pronounced irregularities of multiple thoracic endplates, wedge-shaped appearance of T5, disc space narrowing and a compensatory osseous hypertrophy of the anterior rim of T6. Flattened spinous processes are also shown (□).

(a) Magnetic resonance imaging (MRI): T2 weighted image of the thoracic spinal cord detects a high signal focus in the myelon (←) at T5/6 level, representing focal myelopathy. Wedge-shaped vertebrae at the mid-thoracic region are shown. (b) MRI: T1 weighted image of the thoracic vertebral column shows marked endplate irregularities with wedge-shaped deformity of the T5- and T6-vertebrae, representing Scheuermann' s disease.

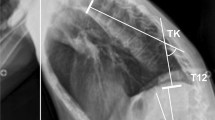
Postoperative radiographies at 6 months follow-up with recovery of neurological impairment and normal walking pattern.
Discussion
Absence of posterior elements of the spine can be a normal variant or an indication of a destructive process. Downey et al.2 presented four cases of congenital absence of the posterior elements in the thoracolumbar spine using computerized tomography scanning. Most of them presented with absences or partial absences of laminae, pedicles or facets. A congenital variant seemed to be excluded after review of the patient's childbirth and the absence of other risk factors apart from HELLP syndrome of the mother.
This case report shows structural consequences of Scheuermann's disease in a young patient with increase of a short-segmented kyphotic angulation during growth and resulting paraplegia. Hypoplastic spinous processes and paraspinal muscles at the upper thoracic spine can therefore be regarded as possible consequences of Scheuermann's disease. Failure of formation produces an average progression of 7° angulation a year and wedging vertebrae in Scheuermann's disease 2° a year.3 The trauma 15 month before the manifestation of neurological deficits could have contributed to the acceleration of flexion myelopathy of the thoracic spine with increased pressure at the anterior part of the vertebral body, kyphotic angulation and traction of the spinal cord as described by Fujibayashi et al.4 If Scheuermann's disease with a sharp-wedged kyphotic angulation occurs, attention should be paid on sensorimotor deficits. On the other side, Masini and Maranhão1 pointed out that the degree of angulation affects the vascularization of the spinal cord with the consequence of venous stasis. In an animal model that compared spinal cord compression and kyphotic deformity, Shimizu et al.5 found histological changes of the spinal cord associated to both, continuous mechanical compression and vascular changes. The combination of Scheuermann's disease with a short-segmented thoracic gibbus may influence the progression of kyphosis with a potential harm for developing myelopathic complications and subsequent paraplegia (Table 1).
Conflict of interest
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
References
Masini M, Maranhão V . Experimental determination of the effect of progressive sharp-angle spinal deformity on the spinal cord. Eur Spine J 1997; 6: 89–92.
Downey EF, Whidden SM, Brower AC . Computed tomography of congenital absence of posterior elements in the thoracolumbar spine. Spine 1986; 11: 68–71.
Hefti F . Kongenitale Fehlbildungen an der Wirbelsäule. Orthopäde 2002; 31: 34–43.
Fujibayashi S, Neo M, Nakamura T . Flexion myelopathy of the thoracic spine. Case report. J Neurosurg Spine 2007; 6: 68–72.
Shimizu K, Nakamura M, Nishikawa Y, Hijikata S, Chiba K, Toyama Y . Spinal kyphosis causes demyelination and neuronal loss in the spinal cord: a new model of kyphotic deformity using juvenile Japanese small game fowls. Spine 2005; 30: 2388–2392.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Putz, C., Stierle, I., Grieser, T. et al. Progressive spastic paraplegia: the combination of Scheuermann's disease, a short-segmented kyphosis and dysplastic thoracic spinous processes. Spinal Cord 47, 570–572 (2009). https://doi.org/10.1038/sc.2008.133
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sc.2008.133
