
Abstract
The COVID-19 pandemic has disrupted lives and the economy, reminding the global community of the devastating health and economic impacts of uncontrolled infectious disease. It has affected how and where people live, work, shop, and play, and exposed our cities’ vulnerabilities, leading to calls for a health lens to be applied in designing, approving, and evaluating city plans. Socioeconomic, spatial and health inequities have been amplified, particularly for those living in inadequate or poorly designed housing, neighbourhoods, and cities. Hence, city mayors have committed to ‘build back better’ with all daily living amenities within a 15-min walking or cycling trip. Designed well, these cities have the potential to be healthier, more sustainable, equitable, and resilient. Yet their delivery requires a rethink of city planning. Drawing on lessons from the COVID-19 pandemic, we argue that to reduce the risk of future pandemics, we must mitigate climate change, limit urban expansion, and use nature-based solutions to protect natural habitats and biodiversity. We then explore how healthy, sustainable, and resilient 15-minute cities could be planned to reduce emissions and ensure our cities are more resilient in the event of future crises. Given that higher density housing underpins the success of 15-minute cities, we also examine how to create more resilient housing stock, through well-implemented health-supportive apartment design standards. Finally, we argue that to achieve all this, cross-sector leadership and investment will be vital.
Similar content being viewed by others

Introduction
The foundations of contemporary town planning, civil engineering and public health were built on the leadership of social reformers in the late 19th century, advocating comprehensive interventions to curb morbidity and mortality associated with people living in overcrowded, unsanitary, and polluted industrialising cities1,2,3. Integrated infrastructure and policy interventions provided access to clean water and sanitation and improved housing conditions, the latter by requiring minimum lot sizes and separating noxious land uses from residential areas4. Prompted by 20th century infectious disease epidemics, further improvements to higher density housing were achieved through regulations promoting natural light, ventilation and space5,6. Hence, in many cities – particularly those in higher income countries with well-implemented environmental health programs – infectious, waterborne and respiratory diseases have appeared to be largely tamed, and the associated morbidity and mortality prevented or controlled.
The COVID-19 pandemic has challenged this assumption7. Over three years into the pandemic, there have been over 600 million confirmed cases of COVID-19, and over 6.4 million deaths globally8. Irrespective of a city’s location or wealth, COVID-19 has disrupted lives and the economy, reminding the global community of the devastating human health and economic impacts of uncontrolled infectious disease7. Socioeconomic inequities have been amplified, particularly for those living in inadequate or poorly designed housing, neighbourhoods and cities6,9. The pandemic has affected how and where people live, work, shop and play, and exposed our cities’ vulnerabilities, with calls for a health lens to be applied to planning, approving and evaluating city plans6,10,11. Moreover, as human health is underpinned by eco-system health, COVID-19 has highlighted the need for the integrated, unifying and balanced approach to promoting health known as ‘One-Health’, that aims to optimise the health of people, animals and the environment12.
Given current and future global challenges confronting urban populations, planning cities to mitigate and adapt to future pandemics, climate change, and disasters must be a priority. The impacts of the pandemic have highlighted the need for cities to be resilient and designed to support urban dwellers to withstand future shocks9. Consistent with the World Health Organization’s concept of ‘One-Health’12, the UN Habitat13 defines a resilient city as one that ‘assesses, plans and acts to prepare for and respond to hazards - natural and human-made, sudden and slow-onset, expected or unexpected’ in ways that can protect and enhance people’s lives. This paper explores what lessons can be applied from this 21st century pandemic, to create healthy, sustainable, resilient cities in the future?6
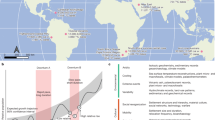
To address this question, we draw on a slightly modified framework of the pathways through which city planning impacts health, recently published in The Lancet Global Health series on urban design, transport and health (see Fig. 1)14. This comprehensive framework was developed in response to the significant interrelated challenges confronting cities in the 21st century including population growth, rapid urbanisation, traffic congestion, rising non-communicable disease rates, transport-related air and noise pollution, climate change and biodiversity loss14,15. It takes a systems approach to city planning16 and considers the integrated upstream policies and interventions needed to optimise compact urban development that fosters human, ecosystem and planetary health. Compact urban development intensifies the use of space within a city through higher density housing in walkable neighbourhoods with mixed land use, public open space and efficient multi-modal transport infrastructure17. Done well, compact urban development fosters healthy and sustainable lifestyles. Done poorly, it can expose residents to individual, social and environmental risks, and impedes human, eco-system, and planetary health outcomes.

Modified from14 with new pathway indicated in green.
This framework is relevant to both non-communicable and communicable disease risks14 and could usefully guide policies to create resilient cities that protect residents’ health in the event of future crises. Rather than focussing on one sector, it addresses the upstream multi-sector ‘causes of the causes’ of poor health and environmental outcomes and proposes the need for integrated cross-sector planning and interventions. Hence, this paper applies and expands the framework to highlight the role city planning could and should play in promoting healthy and sustainable lifestyles in the post-COVID-19 era, by mitigating future crises (e.g., preventing future novel infectious diseases)11,18, creating built environments that support citizens to endure periods of lockdown and/or quarantine, and minimising the social, economic and health inequities that COVID-19 made so apparent.
This paper begins by exploring how the COVID-19 pandemic exposed the vulnerabilities of our cities for health and wellbeing; before considering the city planning features and lessons that could be applied to ensure future cities are designed to protect the health of all citizens in the event of a pandemic or other future crises.
The impact of the COVID-19 pandemic on city dwellers
COVID-19 spread quickly throughout urban areas, particularly amongst the more vulnerable, and those living in crowded and poorly ventilated housing7,14,19,20. Without vaccines to protect citizens from serious illness, hospitalisation and death, governments worldwide introduced basic public health and social measures (PHSM) (e.g., handwashing, mask wearing, physical distancing and quarantine). In many cases, mandatory city-wide lockdowns restricted movement outside the home to essential activities such as food shopping, outdoor exercise and recreation, medical care and caregiving, and study or work that could not be done at home. Those classified as ‘essential’ workers, often disproportionately residing in disadvantaged neighbourhoods21, remained mobile across the city, increasing their risk of infection and transmission within and outside the home, particularly for those living in crowded households19.
Densely populated cities increase social interactions in public places and hence, potential exposure to infectious diseases. Initially, population density was implicated in accelerating disease transmission10. However, subsequent studies have challenged this assumption, observing that once strict PHSM were enforced, irrespective of the level of density, it was overcrowded living conditions22 and intra-urban mobility23, particularly by public transport10, that affected disease transmission and hospitalisation, rather than density-levels per se24,25. Indeed, some of the densest cities globally successfully curbed transmission by strictly enforcing PHSM10,26,27.
Nonetheless, as lockdowns were extended, the challenges of living, working, and studying in poorly designed housing, with insufficient or inflexible space, or in neighbourhoods that lacked key local infrastructure, such as green spaces or shops, increased social isolation and affected mental health18. This prompted an exodus to outer suburban and regional areas26, placing pressure on housing affordability and local infrastructure, and displacing lower income households, particularly in regional cities28. If unchecked post-pandemic, this trend could exacerbate the urban sprawl already rife across many cities26, and widen socioeconomic inequities28.
Working from home was enabled by digital technology that saw telecommuting for office workers become normalised. With most people working and studying from home, commuting and private motor vehicle use plummeted, and cities worldwide saw rapid declines in traffic, greenhouse gas emissions and air and noise pollution25. This was fortuitous because studies subsequently found an increased risk of COVID-19 transmission for those exposed to air pollution25,29. Air pollution is already the 4th leading cause of global mortality and morbidity14, causing almost 9 million premature deaths annually30.
When exercise and essential errands were the only permitted activities outside the home, access to local shops and services and public open space were vital, and there were calls for more road space to be allocated to commerce, active transport and recreation to enable physically distanced circulation in the public realm31. This prompted a proliferation of ‘pop-up’ bicycle lanes in cities worldwide, providing opportunities for safe physically distanced travel32, particularly when people were fearful of disease transmission when using public transport. Such was the importance of cycling as a safe, effective and reliable form of recreation and transportation, cities such as Copenhagen classified bicycle shops as ‘essential services’31,32. The preference for walking and cycling during lockdowns highlighted ‘that non-motorised transportation systems are more resilient during pandemics’25, and must be prioritised post-pandemic, to create more resilient cities. Indeed, with more people working from home and spending more time in their neighbourhoods, urban dwellers and decision-makers alike began to appreciate the importance of living locally, with local access to shops, services, public open spaces, and multi-modal transport systems.
Lessons for city planning
So, what lessons can we take from this experience, to protect urban dwellers during future pandemics or other crises? Here we reflect on and apply the Fig. 1 framework for creating healthy, sustainable, and resilient cities post-pandemic. First, we consider how city planning could mitigate future pandemics by reducing the impacts of urban development on natural habitats and avoiding biodiversity loss and climate change. Second, we explore how creating 15-minute cities that enable local living and sustainable mobility would reduce transport-related emissions and mitigate climate change while also enabling urban dwellers to adapt when confronted with a crisis, such as a pandemic. Finally, given higher density housing underpins achieving 15-minute cities, we consider how to ensure that higher-density housing is health-supportive, particularly in the event of a crisis.
Protecting habitats and reducing biodiversity loss
Urban expansion is threatening biodiversity by ‘polluting, degrading and fragmenting habitat and displacing endemic species with introduced ones’ (p e923)14. The pandemic has been a timely reminder of the interconnection between humans and nature, given COVID-19 is a probable zoonotic disease that transferred to humans from an animal source33. Established socioecological models of health situate ecosystems and nature as fundamental determinants of healthy urban populations2,34. Emerging infectious diseases are a growing global health concern35, driven by biodiversity loss, which increases interaction and disease ‘spill over’ between species33,36. Once a new disease has appeared, crowded urban areas are perfect environments for transmission. Conversely, intact ecosystems reduce the risk of pathogen emergence and transmission among humans and animals35,36.
To prevent future epidemics and pandemics, policies that foster nature-based solutions are needed (see Fig. 1). This includes curbing urban expansion to reduce biodiversity loss and human activity encroaching into wildlife habitats, and biodiversity-sensitive urban design. Economic activity and resource use in cities also needs to limit environmental alterations and biodiversity loss well beyond urban boundaries, from pollution, deforestation, agriculture, resource mining and climate change14,33,37.
Climate change exacerbates the risk of infectious disease emergence and spread (including zoonotic, vector-borne, and water-borne disease) due to ecosystem disruption and the increased frequency and intensity of extreme weather and disasters (e.g., heatwaves, flood, bushfires)33,35,38. Exposure to multiple disasters, such as a heatwave or flood during a pandemic, has compounding impacts on health and inequities20,39,40. Transitioning to zero-emission cities is therefore imperative for disaster mitigation, and preventing the health impacts of climate change.
The COVID-19 pandemic brought a short-term dividend of reduced air pollution and emissions in cities, but these climate benefits need to be sustained and accelerated in the longer-term20. Cities also need to minimise impacts of climate-change related disasters, especially for vulnerable populations who are less able to adapt and respond. Key components of disaster risk minimisation are development controls in areas prone to disasters such as fire or flood, and provision of resilient infrastructure and housing that can withstand extreme weather14,38.
Policies that foster nature-based solutions and promote urban greening to integrate and protect nature within urban areas, not only make cities and neighbourhoods more desirable, but also have co-benefits for biodiversity, wildlife corridor protection, climate change adaptation, and resilience to urban heat, which impacts human health14,25,41. Well-designed urban green spaces played a vital role in urban resilience during the COVID-19 pandemic, enabling socially distanced outdoor recreation and contact with nature, with multiple population health benefits25,42. Thus, the size and equity of access to biodiverse green spaces and tree canopy cover should be key city planning considerations, along with biodiversity-sensitive design principles14. Planning resilient 15-minute cities post-pandemic is an opportunity to embrace the close connection between planetary and human health, and adopt an integrative approach to economic recovery and urban policy that safeguards biodiversity and ecosystems33.
Enabling local living through 15-minute cities
Healthy and sustainable cities are underpinned by compact urban development that enables citizens to undertake daily activities locally using active forms of transport14. Yet for decades, low-density car-centric planning has dominated the design of cities worldwide, robbing residents of the health and other benefits afforded by active transport access to local amenities43. As the impacts of the pandemic became apparent, Moreno et al.32 and others6,9,10,25,43,44,45, have argued for a rethink of city planning to reduce inequities and ensure that urban dwellers’ basic needs - working, commerce, healthcare, education and entertainment - can be met locally by walking, cycling or micro-mobility. Indeed, with more people now working from home enabled by digital tools and infrastructure, the importance of local neighbourhoods for fulfilling daily needs has re-emerged. For example, C40, the global network of city Mayors, has committed to ‘build back better’ by creating 15-minute cities that support local living and prioritise active, sustainable mobility with co-benefits for reducing urban inequities, improving public health, and climate change mitigation46. Creating ‘cities of villages’ could make cities more resilient to future pandemics, enabling residents to adapt and thrive during lockdowns and potentially reducing geographic spread of disease associated with mobility22.
However, transitioning to 15-minute cities will require a new typology in the way cities are structured25,32, focussing on decentralised47, ‘proximity-based’ planning where all basic services required for daily living are available within 15 min by walking or cycling9,44. Moreno et al.32 have argued that achieving the 15-minute city requires a focus on four Ds: Density (i.e., ensuring sufficient population to make shops, services and public transport viable, but as discussed below, this must be done well to protect the health and wellbeing of residents), Destination Proximity (i.e., creating a city of short-distances where shops and services are within a walkable catchment), Diversity (i.e., of housing to achieve increased population density and social diversity, and diversity of destinations to make local living achievable) and Digitalisation (i.e., access to high-quality digital infrastructure that enables more people to work from home at least on some days of the week48).
All these Ds are vital. In addition to Moreno et al.’s 4Ds (three were already in our framework; and we added their Digitalisation), we include four regional intervention Ds (Destination accessibility (i.e., enhancing public transport to regional employment and activity centres), Distribution of employment (i.e., creating poly-centric cities with diverse employment opportunities that reduce commute distances, enable sustainable mobility, and increase the potential to work locally on at least some days of the week), Demand management (i.e., reducing the convenience and increasing the cost of driving and parking); and Disaster mitigation (i.e., restricting urban development in flood and fire prone areas; and using nature-based solutions that mitigate flood risk and protect natural habitats and biodiversity)) (Fig. 1). We also include four additional urban design Ds: Design (i.e., movement network design for a multi-modal transportation system that prioritises infrastructure and space for active transport31); Distance to transit (i.e., to facilitate public transport use); Desirability (i.e., urban greening that ensures sufficient access to public open space, while protecting biodiversity and habitats and increasing tree canopy that contributes to urban cooling); and Distributed (i.e., that ensures equity of access to all of the other Ds).
However, the success of compact urban developments that deliver the 15-minute city will be determined by the quality and resilience of its high-density housing stock. Given pressures on apartment dwellers during the pandemic, the next section focuses on lessons for optimising higher density housing.
High-quality higher-density housing
Consistent with our framework, higher residential Density is essential to the creation of 15-minute cities as they provide the population needed to increase Destination proximity and decreases the Distance to a frequent public transport service49. However, the success and health impacts of the compact 15-minute city – particularly in a pandemic – also depend on the Design and Desirability of its high-density housing, and the level of Digitisation that allows residents to easily work from home50. This was exacerbated during the COVID-19 pandemic, with lockdowns and physical and social distancing restrictions increasing the ‘dose’ of exposure to the home environment, and accentuating the negative impacts of poor quality housing.
Like other housing types, poor apartment design and quality can expose residents to temperature extremes, inadequate ventilation, too little (or too much) sunlight, poor acoustic and visual privacy, and insufficient and/or inflexible space, with consequences for health and wellbeing50,51. However some of these design problems are heightened for apartment dwellers who typically have less control over indoor environmental conditions, less private indoor and outdoor space, and less flexible layouts52,53. This placed additional stresses on apartment dwellers during COVID-19, as there was limited capacity to socially distance within households to reduce disease spread, repurpose the space for home-based schooling, work or exercise (despite Digitalisation enabling home schooling and/or work), or retrofit apartments to address design problems that limited light, ventilation, thermal comfort or contact with nature18,52,53,54,55. Indeed, the pandemic re-emphasised the need for apartment standards that promote health and wellbeing, and building approval processes that ensure these requirements are implemented as intended56.
The nature of apartment living also affects social distancing between households within the building or apartment complex. Individual apartments are accessed via shared circulation spaces – lifts/elevators, stairwells, and corridors – that increase the potential for transmission between households, via contact with surfaces (e.g., door handles, lift call buttons) or closer physical proximity52. Communal spaces, such as outdoor gardens, provide additional space and respite, assuming they include the design features that make these spaces attractive and encourage their use (e.g., trees, greenery, seating)57. However, during COVID-19 peaks, many shared spaces were closed to residents to minimise infection52, confining residents to their apartment or forcing them into the wider neighbourhood, when permitted. While the closure of communal areas had worthy intentions, it had the potential to further penalise apartment residents, particularly those in smaller apartments where lockdowns increased mental distress18. Building designs that minimise physical proximity between residents (e.g., wider corridors, inviting staircases)19,47, improve natural ventilation (e.g., openable windows in internal circulation corridors)56, and incentivise larger communal areas with greenery would help minimise the impacts of future pandemics on apartment residents.
These policy settings for apartments and buildings are also important to adapt to extreme heat events associated with climate change (Disaster mitigation) and are vital for lower-income populations to reduce energy use and decrease the costs of mechanical heating and cooling58. However, healthy apartment design policy requires the support of wider neighbourhood planning policies that deliver nature-based solutions and preserve green space. These increase the Desirability of local neighbourhoods and the potential for green views, promote urban cooling that reduces heat islands19,52, and limit exposure to traffic and noise pollution14, all of which are important risk factors for health outcomes downstream (Fig. 1).
Discussion
Transitioning to healthy and sustainable 15-minute cities is challenging. Yet cities and organisations around the world, including organisations such as C40, are committing to the concept46. As Nieuwenhuijsen43 points out, numerous urban models are already being implemented to improve established areas in cities through motorised traffic management and supporting active transportation in residential areas to reduce air and noise pollution and greenhouse gas emissions. This includes the Barcelona superblocks, London’s low-traffic neighbourhoods and Hamburg’s car-free city planning43. None of this is easy, but with courageous leadership, change is clearly possible. Creating resilient 15-minute cities for all will require a rethink of urban planning32, a commitment to delivering health-supportive high density housing, greater emphasis on the timely-delivery and financing of digital, and social infrastructure, and a compact city structure that ensures that all citizens have access to basic amenities required for daily living by active transport25. This necessitates a shift away from car-centric planning – whether electric, autonomous or not – and towards city planning that prioritises sustainable mobility: walking, cycling, public transport use and micro-mobility59.
Addressing complex city planning problems requires sector and academic silos to be broken down, and for ‘nexus’ or cross-sector integrated planning to be prioritised14,15,60. In nexus planning, each component is assessed without prioritising one over the other, to identify trade-offs and synergies to reduce the risk of negative externalities to another sector, duplication of efforts and resources25. Nexus planning requires good and integrated governance and shared budgets across government: hence, political will and leadership is vital to create an authorising environment that enables action and integrated planning across all urban system policies15.
Indeed, political will from all levels of government and the private sector is essential61. To achieve healthy, sustainable and resilient 15-minute cities for all requires investment in both green and social infrastructure. In the 21st century, neighbourhoods are rarely built without clean water and sanitation. Similarly, green and social infrastructure must be elevated to ‘essential infrastructure’;61,62 and regulations and standards must ensure that human, eco-system, and planetary health are primary considerations in building new, and retrofitting existing, neighbourhoods and housing. Indeed, achieving healthy and sustainable 15-minute cities for all will require new legislation, regulations, and standards; cross-sector integrated horizontal planning across government departments, and vertical planning between different levels of government and the private sector as well as participatory planning with the community (particularly in established areas); and new co-funding arrangements across all levels of government to fund land and physical, digital, and social infrastructure development. Finally, inter-disciplinary research co-designed with policymakers and practitioners will be vital to optimise the 15-minute city, to benchmark and monitor implementation and to avoid any unintended consequences.
References
Corburn, J. Reconnecting with our roots. American urban planning and public health in the twenty-first century. Urban Aff. Rev 42, 688–713 (2007).
Barton, H. City of wellbeing: A radical guide to planning (Abingdon, Oxon, 2017).
Banai, R. Pandemic and the planning of resilient cities and regions. Cities 106, 102929 (2020).
Corburn, J. Confronting the challenges in reconnecting urban planning and public health. Am J Public Health 94, 541–546 (2004).
Yang, H., Oldfield, P. & Easthope, H. Influences on apartment design: a history of the spatial layout of apartment buildings in sydney and implications for the future. Buildings 12, 628 (2022).
Wang, R., Yang, L. & Chen, H. Editorial: supporting wellbeing during and after COVID-19 in cities. Front. Sustain. Cities 3, https://doi.org/10.3389/frsc.2021.798063 (2021).
de León, E. A. et al. Beyond building back better: imagining a future for human and planetary health. Lancet Planet Health 5, e827–e839 (2021).
World Health Organization. Coronavirus disease (COVID-19) weekly epidemiological update and weekly operational update, https://www.who.int/publications/m/item/weekly-epidemiological-update-on-covid-19-7-september-2022 (2022).
Majewska, A., Denis, M., Jarecka-Bidzinska, E., Jaroszewicz, J. & Krupowicz, W. Pandemic resilient cities: possibilities of repairing Polish towns and cities during COVID-19 pandemic. Land Use Policy 113, https://doi.org/10.1016/j.landusepol.2021.105904 (2022).
AbouKorin, S. A. A., Han, H. & Mahran, M. G. N. Role of urban planning characteristics in forming pandemic resilient cities - case study of Covid-19 impacts on European cities within England, Germany and Italy. Cities 118, 103324 (2021).
Askarizad, R. & He, J. Post-pandemic urban design: the equilibrium between social distancing and social interactions within the built environment. Cities 124, 103618 (2022).
World Health Organization. One Health, https://www.who.int/news-room/questions-and-answers/item/one-health (2017).
UN-Habitat. City resilience profiling tool (United Nations Human Settlements Programme, 2018).
Giles-Corti, B. et al. What next? Expanding our view of city planning and global health, and implementing and monitoring evidence-informed policy. Lancet Global Health 10, e919–e926 (2022).
Lowe, M. et al. City planning policies to support health and sustainability: an international comparison of policy indicators for 25 cities. Lancet Global Health 10, e882–e894 (2022).
Pakoz, M. Z. & Isik, M. Rethinking urban density, vitality and healthy environment in the post-pandemic city: the case of Istanbul. Cities 124, 103598 (2022).
Zhang, X. et al. Compact cities and the Covid-19 pandemic: systematic review of the associations between transmission of Covid-19 or other respiratory viruses and population density or other features of neighbourhood design. Health Place 76, 102827 (2022).
Amerio, A. et al. COVID-19 lockdown: housing built environment’s effects on mental health. Int. J. of Env. Res. Public Health 17, 5973 (2020).
Frumkin, H. COVID-19, the built environment, and health. Environ. Health Perspect. 129, 75001 (2021).
Lambert, H. et al. COVID-19 as a global challenge: towards an inclusive and sustainable future. Lancet Planet. Health 4, e312–e314 (2020).
Do, D. P. & Frank, R. Unequal burdens: assessing the determinants of elevated COVID-19 case and death rates in New York City’s racial/ethnic minority neighbourhoods. J. Epidemiol. Commun. Health 75, 321–326 (2021).
Khavarian-Garmsir, A. R., Sharifi, A. & Moradpour, N. Are high-density districts more vulnerable to the COVID-19 pandemic? Sustain. Cities Soc. 70, 102911 (2021).
Jinjarak, Y., Ahmed, R., Nair-Desai, S., Xin, W. & Aizenman, J. Accounting for global COVID-19 diffusion patterns, January–April 2020. Eco. Disasters Clim. Change 4, 515–559 (2020).
Hamidi, S., Sabouri, S. & Ewing, R. Does density aggravate the COVID-19 pandemic? J. Am. Plann. Assoc. 86, 495–509 (2020).
Sharifi, A. & Khavarian-Garmsir, A. R. The COVID-19 pandemic: impacts on cities and major lessons for urban planning, design, and management. Sci. Total Environ. 749, 142391 (2020).
Bil, J. S., Bulawa, B. & Swierzawski, J. Mental health and the city in the post-COVID-19 era. Sustain. 13, 7533 (2021).
Rojas-Rueda, D. & Morales-Zamora, E. Built environment, transport, and COVID-19: a review. Current Env. Health Rep. 8, 138–145 (2021).
Giles-Corti, B. et al. Spatial and socioeconomic inequities in liveability in Australia’s 21 largest cities: Does city size matter? Health Place 8, 102899.t (2022).
Ali, N. & Islam, F. The effects of air pollution on COVID-19 infection and mortality-a review on recent evidence. Front. Public Health 8, 7 (2020).
Lelieveld, J. et al. Effects of fossil fuel and total anthropogenic emission removal on public health and climate. Proc. Nat. Acad. Sci. 116, 7192–7197 (2019).
Nikitas, A., Tsigdinos, S., Karolemeas, C., Kourmpa, E. & Bakogiannis, E. Cycling in the era of COVID-19: lessons learnt and best practice policy recommendations for a more bike-centric future. Sustain. 13, 4620 (2021).
Moreno, C., Allam, Z., Chabaud, D., Gall, C. & Pratlong, F. Introducing the “15-Minute City”: sustainability, resilience and place identity in future post-pandemic cities. Smart Cities 4, 93–111 (2021).
Lawler, O. K. et al. The COVID-19 pandemic is intricately linked to biodiversity loss and ecosystem health. Lancet Planet. Health 5, e840–e850 (2021).
Rayner, G. Conventional and ecological public health. Pub. Health 123, 587–591 (2009).
Naughtin, C. et al. Our Future World: Global megatrends impacting the way we live over coming decades (CSIRO, Brisbane, Queensland, 2022).
Keesing, F. et al. Impacts of biodiversity on the emergence and transmission of infectious diseases. Nature 468, 647–652 (2010).
Oke, C. et al. Cities should respond to the biodiversity extinction crisis. npj Urban Sustain. 1, 11 (2021).
IPCC. Climate Change 2022: Impacts, Adaptation, and Vulnerability. Contribution of Working Group II to the Sixth Assessment Report of the Intergovernmental Panel on Climate Change (IPCC, 2022).
Golechha, M. & Panigrahy, R. K. COVID-19 and heatwaves: a double whammy for Indian cities. Lancet Planet Health 4, e315–e316 (2020).
Leppold, C., Gibbs, L., Block, K., Reifels, L. & Quinn, P. Public health implications of multiple disaster exposures. Lancet Public Health 7, e274–e286 (2022).
Sharifi, A., Pathak, M., Joshi, C. & He, B.-J. A systematic review of the health co-benefits of urban climate change adaptation. Sustain. Cities Soc. 74, 103190 (2021).
Honey-Rosés, J. et al. The impact of COVID-19 on public space: an early review of the emerging questions – design, perceptions and inequities. Cities Health, 5 (Sup. 1) 1–17 (2020).
Nieuwenhuijsen, M. J., Hahad, O. & Munzel, T. The COVID-19 pandemic as a starting point to accelerate improvements in health in our cities through better urban and transport planning. Env. Sci. Pollut. Res. 29, 16783–16785 (2022).
Allam, Z., Nieuwenhuijsen, M., Chabaud, D. & Moreno, C. The 15-minute city offers a new framework for sustainability, liveability, and health. Lancet Planet. Health 6, e181–e183 (2022).
Pozoukidou, G. & Chatziyiannaki, Z. 15-minute city: decomposing the new urban planning Eutopia. Sustain. 13, 928 (2021).
C40 Cities & Arup. Green and thriving neighbourhoods: a pathway to net zero, featuring the ‘15-minute city’ (C40 Cities and Arup, 2021).
Megahed, N. A. & Ghoneim, E. M. Antivirus-built environment: Lessons learned from Covid-19 pandemic. Sustain. Cities Soc. 61, 102350 (2020).
Kakderi, C., Oikonomaki, E. & Papadaki, I. Smart and resilient urban futures for sustainability in the post COVID-19 era: a review of policy responses on urban mobility. Sustain. 13, 6486 (2021).
Giles-Corti, B. et al. City planning and population health: a global challenge. Lancet 388, 2912–2924 (2016).
World Health Organization. WHO Housing and health guidelines (World Health Organization, Geneva, Switzerland, 2018).
Foster, S., Hooper, P., Kleeman, A., Martino, E. & Giles-Corti, B. The high life: a policy audit of apartment design guidelines and their potential to promote residents’ health and wellbeing. Cities 96, 102420 (2020).
Peters, T. & Halleran, A. How our homes impact our health: using a COVID-19 informed approach to examine urban apartment housing. Archnet-Ijar Int. J. Archit. Res. 15, 10–27 (2021).
Horne, R., Willand, N., Dorignon, L. & Middha, B. The lived experience of COVID-19: housing and household resilience (Australian Housing and Urban Research Institute Limited, Melbourne, 2020).
Domínguez-Amarillo, S., Fernández-Agüera, J., Cesteros-García, S. & González-Lezcano, R. A. Bad air can also kill: residential indoor air quality and pollutant exposure risk during the COVID-19 crisis. Int. J. Env. Res. Public Health 17, 7183 (2020).
Bourion-Bedes, S. et al. The effects of living and learning conditions on the health-related quality of life of children and adolescents during the COVID-19 lockdown in the French Grand Est region. BMC Public Health 22, 517 (2022).
Foster, S., Hooper, P., Duckworth, A. & Bolleter, J. An evaluation of the policy and practice of designing and implementing healthy apartment design standards in three Australian cities. Build. Env. 207, 108493 (2022).
Kleeman, A., Giles-Corti, B., Gunn, L., Hooper, P. & Foster, S. Exploring the design, quality and use of communal areas in apartment developments. Cities Health 6, 480–494 (2022).
Howden-Chapman, P. et al. in International Encyclopedia of Housing and Home (ed Smith, S. J.) 344–354 (Elsevier, 2012).
Giles-Corti, B., Zapata-Diomedi, B., Jafari, A., Both, A. & Gunn, L. Could smart research ensure healthy people in disrupted cities? J. Transp Health 19, 100931 (2020).
Nhamo, L. & Ndlela, B. Nexus planning as a pathway towards sustainable environmental and human health post Covid-19. Env. Res. 192, 110376 (2021).
Mell, I. & Whitten, M. Access to nature in a post Covid-19 world: opportunities for green infrastructure financing, distribution and equitability in urban planning. Int. J. Env. Res. Public Health 18, https://doi.org/10.3390/ijerph18041527 (2021).
Klinenberg, E. Palaces for the people. How social infrastructure can help fight inequality, polorization, and the decline of civic life (Crown, 2018).
Acknowledgements
B.G.-C. is supported by an RMIT University Vice Chancellor’s Professorial Fellowship and grants from the National Health and Medical Research Council APP1192788 and GNT9100003. S.F. is supported by an ARC Future Fellowship (FT210100899). M.L. is supported by an RMIT University Vice-Chancellor’s Senior Research Fellowship; and has been awarded an AXA Research Fund Postdoctoral Fellowship.
Author information
Authors and Affiliations
Contributions
B.G.-C., S.F. and M.L. conceptualised the paper, and B.G.-C. led the team. B.L. searched the literature and assisted with analysis. B.G.-C., S.F. and M.L. drafted sections. All authors reviewed the literature, critically edited the paper and approved final submission.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Giles-Corti, B., Foster, S., Lynch, B. et al. What are the lessons from COVID-19 for creating healthy, sustainable, resilient future cities?. npj Urban Sustain 3, 29 (2023). https://doi.org/10.1038/s42949-023-00107-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s42949-023-00107-y
This article is cited by
-
The appeal of cities may not wane due to the COVID-19 pandemic and remote working
npj Urban Sustainability (2024)
-
Advancing Health Equity through 15-min Cities and Chrono-urbanism
Journal of Urban Health (2024)
-
Urban biodiversity and design in time of (post)pandemics: research perspectives from URBIO international network
Urban Ecosystems (2024)
-
Exploring the potential connection between place capital and health capital in the post COVID-19 city
npj Urban Sustainability (2023)
-
Covid, cities, and sustainability: a reflection on the legacy of a global pandemic
npj Urban Sustainability (2023)
