
Abstract
We assessed S-268019-b, a recombinant spike protein vaccine with a squalene-based adjuvant, for superiority in its immunogenicity over ChAdOx1 nCoV-19 vaccine among adults in Japan. In this multicenter, randomized, observer-blinded, phase 3 study, severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2)–naïve participants (aged ≥ 18 years, without prior infection or vaccination against SARS-CoV-2) were randomized (1:1) to receive either S-268019-b or ChAdOx1 nCoV-19 as two intramuscular injections given 28 days apart. Participants who provided consent for a booster administration received S-268019-b at Day 211. The primary endpoint was SARS-CoV-2 neutralizing antibody (NAb) titer on Day 57; the key secondary endpoint was the seroconversion rate for SARS-CoV-2 NAb titer on Day 57. Other endpoints included anti–SARS-CoV-2 S-protein immunoglobulin (Ig)G antibody titer and safety. The demographic and baseline characteristics were generally comparable between S-268019-b (n = 611) and ChAdOx1 nCoV-19 (n = 610) groups. S-268019-b showed superior immunogenicity over ChAdOx1 nCoV-19, based on their geometric mean titers (GMTs) and GMT ratios of SARS-CoV-2 NAb on Day 57 by cytopathic effect assay (GMT [95% confidence interval {CI}] 19.92 [18.68, 21.23] versus 3.63 [3.41, 3.87]; GMT ratio [95% CI] 5.48 [5.01, 6.00], respectively; two-sided p-values < 0.0001). Additionally, NAb measured using a cell viability assay also showed similar results (GMT [95% CI] 183.25 [168.04, 199.84] versus 24.79 [22.77, 27.00]; GMT ratio [95% CI] 7.39 [6.55, 8.35] for S-268019-b versus ChAdOx1 nCoV-19, respectively; p < 0.0001). The GMT of anti–SARS-CoV-2 S-protein IgG antibody was 370.05 for S-268019-b versus 77.92 for ChAdOx1 nCoV-19 on Day 57 (GMT ratio [95% CI] 4.75 [4.34, 5.20]). Notably, immune responses were durable through the end of the study. S-268019-b elicited T-helper 1 skewed T-cell response, comparable to that of ChAdOx1 nCoV-19. After the first dose, the incidence of solicited systemic treatment-related adverse events (TRAEs) was higher in the ChAdOx1 nCoV-19 group, but after the second dose, the incidence was higher in the S-268019-b group. Headache, fatigue, and myalgia were the most commonly reported solicited systemic TRAEs, while pain at the injection site was the most frequently reported solicited local TRAE following both doses in both groups. No serious treatment-related adverse serious TRAEs events were reported in the two groups. S-268019-b was more immunogenic than ChAdOx1 nCoV-19 vaccine and was well tolerated (jRCT2051210151).
Similar content being viewed by others


Introduction
Coronavirus disease 2019 (COVID-19), caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), has caused over 765 million confirmed cases and 7.7 million reported deaths worldwide as of December 12, 20231. Since the emergence of COVID-19 in 2020, many vaccines have been developed and a few approved for emergency use by the World Health Organization after they met rigorous, scientific standards for safety, short-term effectiveness, and the manufacturing quality mandated for such expedited authorization. Multiple vaccines with diverse platforms have been developed against SARS-CoV-2 infection in the past 3 years: 50 vaccines are approved in one or more nations and 183 new vaccine candidates are in the clinical development pipeline globally as of March 20232. Although a majority of the world’s population is vaccinated, the risk of waning immunity following natural infection or immunization and the risk of new emerging variants of concern3,4 make booster administration of vaccines increasingly relevant to protect the vulnerable populations.
Seven vaccines have been approved to date in Japan: (1) BNT162b2 and (2) mRNA-1273, both mRNA vaccines; (3) ChAdOx1 nCoV-19, a viral vector vaccine containing a modified, replication-deficient chimpanzee adenovirus ChAdOx1; (4) NVX-CoV2373, a recombinant nanoparticle vaccine; (5) Ad26.COV2.S, a recombinant, replication-incompetent human adenovirus type 26 vector, (6) DS-5670, an Omicron XBB.1.5-adapted monovalent mRNA vaccine, and (7) KD-414, an inactivated and self-amplifying mRNA vaccine. These vaccines have been highly effective compared with placebo in their pivotal clinical studies5,6,7,8,9. Conducting placebo-controlled disease endpoint efficacy trials for new vaccine candidates is challenging, as only a few individuals globally are still unvaccinated and uninfected. As neutralizing antibodies are considered a surrogate marker of the conferred protection against SARS-CoV-2 infection10,11,12, appropriately designed active comparator-controlled, immuno-bridging studies utilizing neutralizing antibody titers as a suitable primary endpoint to predict vaccine effectiveness are an acceptable alternative approach for authorizing new vaccines13,14.
Shionogi & Co., Ltd., has been developing the S-268019-b vaccine, comprising a full-length recombinant SARS-CoV-2 S-protein, modifying putative furin cleavage site at the middle of the protein and two proline substitutions in the C-terminal region to secure stability, produced using the baculovirus expression system in rhabdovirus-free insect cells, with a squalene-based adjuvant (A-910823) in an oil-in-water emulsion formulation15. We have previously reported that the S-268019-b vaccine elicited robust immunogenic response 4 weeks after the second dose of the vaccine in healthy Japanese adult participants in an interim analysis of the double-blinded phase 1/2 trial16. Moreover, S-268019-b was well tolerated and immunogenic in a large participant pool comprising SARS-CoV-2–naïve adults and elderly participants, and adult participants with a history of either prior infection or vaccination against SARS-CoV-2 for 4 weeks following the second injection in an open-label study in Japan16.
Based on the encouraging interim results from the phase 1/2 study followed by the phase 2/3 study, this phase 3 study reported here was planned. Given the availability of multiple approved vaccines in Japan by the end of 2021, we decided to use the ChAdOx1 nCoV-19 vaccine as the control. We aimed to evaluate whether the immunogenicity of S-268019-b (10 μg antigen strength used based on the phase 1/2 study results16) is superior to that of ChAdOx1 nCoV-19 after two intramuscular injections in SARS-CoV-2–naïve participants. Herein, we report the results from an analysis of the phase 3 study, with safety and immunogenicity data collected until 4 weeks following the second dose of S-268019-b and ChAdOx1 nCoV-19 vaccines and immunogenicity data collected until the end of the study (393 days) following initial vaccination.
Methods
Study design and participants
This multicenter, randomized, observer-blind, active-controlled study included participants aged ≥ 18 years without a history of a laboratory-confirmed diagnosis of SARS-CoV-2 infection or COVID-19, or previous vaccination against SARS-CoV-2 in Japan from January 17, 2022, to January 30, 2022 (jRCT2051210151, the first registration date: January 13, 2022). Detailed inclusion and exclusion criteria are described in Supplementary Fig. 1.
Randomization and masking
Over 1000 eligible participants were randomized 1:1 and allocated to either the S-268019-b group or the active control group on Day 1 by using a Web response interactive system. The assignment was stratified by age groups (18–39 years, 40–64 years, and ≥ 65 years). This was an observer-blinded study; the participants, investigators, and site staff not involved in preparation and vaccination were blinded to the study intervention. Since S-268019-b and the active control vaccine were distinguishable by appearance, a pharmacist preparing study interventions and a vaccine administrator were unblinded and were not allowed to communicate with the participants, investigators, and other site staff about participants’ treatment assignment. While assignment of participants to the intervention groups was unblinded at the time of the primary immunogenicity analysis and the database lock, participants remained blinded until the end of the study. The Web response interactive system will be programmed with blind-breaking instructions. In case of an emergency or participant safety concerns, the investigator had the sole responsibility for determining if unblinding of a participant’s intervention assignment or stoppage was warranted.
Study intervention
The study comprised a screening period (Day − 28 to Day 1 pre-dose), an evaluation period (Day 1 post-dose to Day 57), and a follow-up period (Day 58 to Day 393; Supplementary Fig. 2). Participants were administered the S-268019-b (10 μg antigen with 0.25 mL A-910823 adjuvant in 0.5 mL oil-in-water emulsion) or ChAdOx1 nCoV-19 suspension injection, both given intramuscularly at a 4-week interval (first dose: Day 1, second dose: Day 29). Participants visited the study site on Days 1, 29, 43, 57, 97, 211, and 393 for administration of intervention or further assessments. Participants who had given additional consent to cellular immunity and Th1/Th2 balance analyses also visited the study site on Day 15 for the scheduled visit. Additionally, participants who provided consent for a booster dose were administered S-268019-b on Day 211 regardless of the vaccine received on Days 1 and 28.
Outcomes
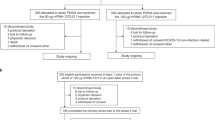
The primary endpoint was SARS-CoV-2 neutralizing antibody titer 28 days following the second vaccination (i.e., Day 57 of the study) (Fig. 1).

Participant disposition. Safety analysis population included randomized participants who received at least one dose of study intervention. Immunogenicity subset population included participants selected from all randomized participants who were included in the mITT population and had at least 1 valid immunogenicity result after the first dose of vaccination. mITT, modified intent-to-treat. One participant who received ChAdOx1 nCoV-19 was excluded due to double enrolment; therefore, the safety analysis population for ChAdOx1 nCoV-19 included 610 participants.
The key secondary endpoint was seroconversion rate for SARS-CoV-2 neutralizing antibody titer at 28 days after the second dose. Seroconversion rate was defined as the percentage of participants with a ≥ fourfold increase in the post-vaccination antibody titer from baseline. If the post-vaccination antibody titer was below the lower level of quantification (LLoQ), participants were considered seroconversion negative. Other secondary endpoints included safety (number of specific adverse events [AEs], serious AEs [SAEs], etc.), efficacy (COVID-19 incidence, asymptomatic COVID-19 incidence, etc.), and immunogenicity parameters (anti–SARS-CoV-2 S-protein IgG antibody titer, neutralizing antibody titer, etc.). Safety was assessed by monitoring solicited local and systemic AEs, unsolicited AEs, treatment-related AEs (TRAEs), SAEs, medically attended adverse events (MAAEs), and AEs of special interest (AESIs). Solicited local and systemic AEs were recorded for 7 days following each vaccination using an e-diary. Unsolicited non-serious AEs were collected from the date of signing of the informed consent form to Day 57. SAEs, MAAE, and AESIs were collected until Day 393.
Exploratory endpoints included neutralizing antibody titer against variants of interest and variants of concern, and cellular immunity assessed using cytokine-producing cell count by interferon-gamma (IFN-γ) ELISPOT assay and Th1/Th2 balance by intracellular cytokine staining assay. The methodology for quantification of the anti-spike protein IgG titer, neutralizing antibody titer, IFN-γ ELISPOT assay, and intracellular cytokine staining by flow cytometry (ICS-FCM) has been previously described16. Neutralizing antibody levels for the SARS-CoV-2 variants were assessed using the ancestral strain (D614E) as described in the phase 2/3 booster publication17. Notably, the values below LLoQ were replaced by values of 0.5 × LLoQ. Additional methods are described in Supplementary Appendix.
Ethics approval and statement
The study was approved by Review Board of Human Rights and Ethics for Clinical Studies Institutional Review Board in Clinical Research Hospital Tokyo, Shinei Diabetes Clinic, Yamazaki Otorhinolaryngology and Vertigo Clinic, Public Health Insurance Association Clinic, Shinagawa Strings Clinic, Tokyo Asbo Clinic, Motomachi Takatsuka Naika Clinic, Dojinkinenkai Meiwa Hospital, Shimamura Memorial Hospital, Koseikai Yotsubashi Clinic, and Tenjin Sogo Clinic, by Takahashi Pediatric Clinic Institutional Review Board in Irie Medical Clinic, Aijinkai Takatsuki General Hospital, and Nihonbashi Sakura Clinic, by Tokyo-Eki Center-building Clinic Institutional Review Board in Tokyo-Eki Center-Building Clinic and Fukuwa Clinic, by Institutional Review Board, P1 Clinic, Keiko-kai Medical Corporation in Higashi Shinjuku Clinic, by Yoyogi Mental Clinic Institutional Review Board in Samoncho Clinic, by Medical Corporation Cattleyakai Dr.Mano Medical Clinic Institutional Review Board in Sapporo Odori Endoscopy Clinic, and by Sekino Hospital Institutional Review Board in Sekino Hospital (Supplementary Table 1). The study was conducted in accordance with the protocol, the Declaration of Helsinki and Council for International Organizations of Medical Sciences (CIOMS) International Ethical Guidelines, the International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use (ICH) Good Clinical Practice Guidelines, and other applicable laws and regulations. All participants provided written informed consent.
Statistical analyses
Sample size determination indicated that a total of 882 participants from the immunogenicity subset whose SARS-CoV-2 neutralizing antibody titers were observed at 28 days after the second dose were required to demonstrate the superiority with at least 90% power at a two-sided significance level of 0.05, assuming the standard deviation (SD) of the natural log-transformed titers of SARS-CoV-2 neutralizing antibody titers to be 1.2 and the true geometric mean titer ratio (GMTR) between S-268019-b and the ChAdOx1 nCoV-19 vaccine to be 1.3. Considering early termination, the target number of participants who had immunogenicity assessment and had no SARS-CoV-2 seropositivity at baseline was 1,000.
The following analysis sets were included (1) full analysis set (FAS) containing all randomized participants who received at least one dose of the study intervention; (2) modified intent-to-treat (mITT) population comprising participants in the FAS but excluding participants who had evidence of past or present SARS-CoV-2 infection at baseline; (3) immunogenicity subset containing participants selected from all randomized participants who were included in the mITT population and had at least one valid immunogenicity result after the first vaccine dose; and (4) safety analysis set comprising randomized participants who received at least one dose of the study intervention.
The immunogenicity subset population was used for the following hypothesis testing:
Null hypothesis: \({\mu }_{\text{A}}\)=\({\mu }_{\text{c}}\)
Alternative hypothesis: \({\mu }_{\text{A}}\ne {\mu }_{\text{c}}\)where \({\mu }_{\text{A}}\) and \({\mu }_{\text{C}}\) are the geometric means of SARS-CoV-2 neutralizing antibody titers at 28 days following the second vaccination for S-268019-b recipients and that for ChAdOx1 nCoV-19 recipients, respectively. If the lower limit of the 95% confidence interval (CI) for the GMTR (S-268019-b to the ChAdOx1 nCoV-19 vaccine) was greater than 1, superiority of S-268019-b was confirmed.
For the primary endpoint analysis, superiority assessment was planned assuming a low proportion of neutralizing antibody titer below the LLoQ. Otherwise, post hoc analysis by Wilcoxon rank-sum test, which is a non-parametric statistical hypothesis test, was planned to compare the two groups. No statistical analysis was planned for neutralizing antibody responses against virus variants.
Results
Overall, 1,243 participants were enrolled, of which 1,225 were randomized to receive S-268019-b (n = 613) or ChAdOx1 nCoV-19 (n = 612; Fig. 1). Of the 18 participants who were excluded from the study after enrollment, the most common reason was that participants no longer met the inclusion criteria (n = 12). Among the randomized participants, 2 and 40 participants in the S-268019-b group and 1 and 37 in the ChAdOx1 nCoV-19 group discontinued the study before and after the first dose, respectively. Consequently, 571 and 574 participants received second doses of S-268019-b and ChAdOx1 nCoV-19 vaccines, respectively. Although immunogenicity subset population included 563 and 581 participants in the S-268019-b and ChAdOx1 nCoV-19 groups, only 497 and 514 participants were eligible for immunogenicity analysis at Day 57 as measurements obtained after a postbaseline dose of approved vaccine, a postbaseline positive anti-N-protein antibody or SARS-CoV-2 RT-PCR test result, or a postbaseline onset of COVID-19 were not included in the analysis.
Baseline demographic characteristics of the participants in the S-268019-b and ChAdOx1 nCoV-19 groups were similar and are described in Table 1. Less than a quarter of the participants in both S-268019-b and ChAdOx1 nCoV-19 groups had a history of smoking (23.4% and 23.0%, respectively), while hypertension was the most common risk factor in both groups (6.9% and 9.3%, respectively).
The two-dose regimen of intramuscular injection of S-268019-b was more immunogenic than that of ChAdOx1 nCoV-19, based on the SARS-CoV-2 neutralizing antibody titer measured by cytopathic effect assay 28 days after the second dose of the respective vaccine (geometric mean titer [GMT] 19.92 vs. 3.63; GMTR [95% CI] 5.48 [5.01, 6.00]; two-sided p-value for superiority < 0.0001; Fig. 2a). Robust immunogenicity of S-268019-b was evident across all age groups (Fig. 2c). Notably, the difference in the initial immune responses seen at Day 57 between both vaccines were maintained following administration of a booster dose on Day 211 (Supplementary Fig. 3). Indeed, GMTs on Days 239, 302, and 393 were substantially higher than those seen on Day 211 (considered baseline for the booster dose). Additionally, GMTs for the neutralizing antibody titers continued to be substantially higher in the S-268019-b vs. the ChAdOx1 nCoV-19 group. The seroconversion rate in participants receiving S-268019-b for SARS-CoV-2 neutralizing antibody using the cytopathic effect assay 28 days after the second dose of the vaccine was noninferior to the response in the ChAdOx1 nCoV-19 group (seroconversion rate [95% CI] 91.1% [88.3%, 93.5%] vs. 8.2% [6.0%, 10.9%]; one-sided p-value for non-inferiority < 0.0001; Supplementary Fig. 4). Since approximately 60% of the neutralizing antibody titers in the ChAdOx1 nCoV-19 group were below the LLoQ (Supplementary Fig. 5a), to confirm the robustness of the result, an additional neutralizing antibody measurement by a cell viability assay, which is more sensitive than the cytopathic effect assay, was conducted. The cell viability assay also showed similar results (GMT [95% CI] 183.25 [168.04, 199.84] vs. 24.79 [22.77, 27.00]; GMT ratio [95% CI] 7.39 [6.55, 8.35], p < 0.0001; Fig. 2b). Moreover, the neutralizing antibody titers were statistically significantly different between groups when assessed using the Wilcoxon rank-sum test, a post hoc analysis for both methods (both p < 0.0001). GMT in the S-268019-b group was comparable to that observed in a set of convalescent serum samples from symptomatic outpatients who had recovered from COVID-19 (GMT in the convalescent serum samples was 145.9 [n = 30]). The seroconversion rate following S-268019-b for SARS-CoV-2 neutralizing antibody measured by cell viability assay 28 days after the second dose of the vaccine was higher than that in the ChAdOx1 nCoV-19 group (seroconversion rate [95% CI] 98.8% [97.4%, 99.6%] vs. 66.6% [61.7%, 70.0%]; data not shown). Approximately 20% of the neutralizing antibody titers in the ChAdOx1 nCoV-19 group were below LLoQ (Supplementary Fig. 5b). The GMT of anti–SARS-CoV-2 S-protein IgG antibody titer was higher in the S-268019-b group than the ChAdOx1 nCoV-19 group 28 days after the second dose (GMT 370.05 vs. 77.92; GMTR [95% CI], 4.75 [4.34, 5.20]; Supplementary Fig. 6). Similar to the trend seen for neutralizing antibody titer, anti–SARS-CoV-2 S-protein IgG responses were durable. GMTs for anti–SARS-CoV-2 S-protein IgG titers were substantially higher through Day 393 for both groups when compared to the baseline. Moreover, anti–SARS-CoV-2 S-protein IgG responses in the S-268019-b group continued to be substantially higher than those in the ChAdOx1 nCoV-19 group after Day 57 through Day 393 (Supplementary Fig. 7). The seroconversion rate (95% CI) after S-268019-b for anti–SARS-CoV-2 S-protein IgG antibody 28 days after the second dose was comparable with that in the ChAdOx1 nCoV-19 group (99.8% [98.9%, 100.0%] vs. 98.2% [96.7% vs. 99.2%]; data not shown).

GMTs for SARS-CoV-2 neutralizing antibody: immunogenicity subset using two different methods: (a) cytopathic effect assay; (b) cell viability assay; and (c) GMTs for SARS-CoV-2 neutralizing antibody measured using the cytopathic effect assay in the S-268019-b group: immunogenicity subset in subgroups by age. CI, confidence interval; GMT, geometric mean titer; GMTR, geometric mean titer ratio; LLoQ, lower limit of quantification; SARS-CoV-2, severe acute respiratory syndrome coronavirus 2. Wilcoxon rank-sum test was applied as a post hoc analysis for both methods because there was a certain level of proportion of neutralizing antibody titer below the LLoQ in the ChAdOx1 nCoV-19 group in the results of both methods.
S-268019-b was well-tolerated without any new safety concerns; no treatment-related TRAEs were noted (Supplementary Table 1). Only one participant in each group reported AEs leading to discontinuation of study interventions; no deaths were reported till the data cut-off. Solicited AEs were mild to moderate in severity in most participants. The incidence of solicited systemic TRAEs within 7 days after both vaccinations in the safety analysis set are presented in Fig. 3a, b, whereas the corresponding solicited local TRAEs are presented in Fig. 3c, d. The incidence of solicited systemic TRAEs was higher after the first dose than the second dose in the ChAdOx1 nCoV-19 group, but higher after the second dose than the first dose in the S-268019-b group (Figs. 3a, b). Regardless, headache, fatigue, and myalgia were the most commonly reported solicited systemic TRAEs, while pain at the injection site was the most frequently reported solicited local TRAE. Overall, 1.3% and 7.9% of participants in the S-268019-b and ChAdOx1 nCoV-19 groups, respectively, experienced grade 3 solicited systemic TRAEs, and 0.3% of participants in both groups experienced grade 3 solicited local TRAEs. While 0.2% of participants in both groups experienced grade 4 solicited systemic TRAES, no grade 4 solicited local TRAEs were noted. There were no grade 5 systemic or local TRAEs within 7 days after both vaccinations in both S-268019-b and ChAdOx1 nCoV-19 groups.

(a) Incidence of solicited systemic TRAEs by severity within 7 days after the first dose of the vaccine in the safety analysis set; (b) Incidence of solicited systemic TRAEs by severity within 7 days after the second dose of the vaccine in the safety analysis set; (c) Incidence of solicited local TRAEs by severity within 7 days after the first dose of the vaccine in the safety analysis set; (d) Incidence of solicited local TRAEs by severity within 7 days after the second dose of the vaccine in the safety analysis set. TRAE, treatment-related adverse event.
Both S-268019-b and ChAdOx1 nCoV-19 elicited Th1-skewed responses evident in percentage of CD4 cells positive for IFN-γ and interleukin-2 (IL-2) in flow cytometry with intracellular cytokine staining (Supplementary Fig. 8a). The magnitude of effect at Day 43 was similar or greater with S-268019-b than with ChAdOx1 nCoV-19. Both vaccines had comparable IFN-γ spot forming units when assessed in the ELISPOT assay (Supplementary Fig. 8b).
S-268019-b elicited about eightfold and 19-fold higher neutralizing antibodies against wildtype (D614G) and Delta pseudovirus variants, respectively, compared with ChAdOx1 nCoV-19 (Fig. 4a). However, compared with wildtype, there was a 15-fold and 21-fold reduction in GMT of the neutralizing antibodies elicited by S-268019-b against Omicron BA.1 and BA.2 variants, while GMTs in ChAdOx1 nCoV-19 were mostly below the detection limits. A similar trend was observed when tested with authentic SARS-CoV-2 variants (Fig. 4b).

Neutralizing antibodies against the virus variants in the serum samples collected from vaccinated individuals at Day 57. Neutralizing antibody titers against (a) spike protein-bearing pseudoviruses and (b) live virus variants are shown. Selected samples from the immunogenicity subset (n = 24/group) were assessed for neutralizing antibody titer testing, and the sampling ensured no significant differences in age and neutralizing antibody titer against live wildtype virus on Day 57 compared with the entire cohort. The solid and open circles represent individual values for the S-268019-b and ChAdOx1 nCoV-19 groups, respectively. Titer values reported as below the LLoQ were replaced with 0.5 × LLoQ. Each bar represents the GMT with error bars indicating 95% CI. Samples were selected from the immunogenicity subset (n = 24/group) assessed on Day 57, and sampling ensured no significant differences in age and neutralizing antibody titer against live wildtype virus on Day 57 compared with the entire cohort. The 95% CIs were constructed using Student’s t distribution for log-transformed titers. CI, confidence interval; GMT, geometric mean titer; LLoQ, lower limit of quantification; NT50, serum titers at which 50% neutralization was achieved.
Discussion
In this randomized, controlled, phase 3 clinical trial, a superior neutralizing antibody response was shown 28 days after the second dose of the S-268019-b vaccine compared with the response to the ChAdOx1 nCoV-19 vaccine. A similar trend for higher magnitude of responses for neutralizing antibody and anti–SARS-CoV-2 S-protein IgG antibody titers in the S-268019-b group was observed in the follow-up period through Day 393.
S-268019-b showed good safety and immunogenicity in a preclinical study in cynomolgus monkeys15 and in a randomized, placebo-controlled, phase 1/2 study, a large open-label phase 2/3 study, and a randomized phase 2/3 study as a booster in Japanese participants16,17. In a preclinical study, immunization with 10 µg of S-910823 with A-910823 demonstrated protective efficacy against SARS-CoV-2 challenge according to genomic and subgenomic viral RNA transcript levels in nasopharyngeal, throat, and rectal swab specimens15. Furthermore, pathological analysis revealed no detectable vaccine-dependent enhancement of disease in the lungs of challenged vaccinated monkeys15. Additionally, based on the favorable results from the placebo-controlled phase 1/2 study and open-label phase 2/3 studies, S-268019-b is being evaluated in large phase 3 trials. The immunogenicity and safety results of S-268019-b from this large phase 3 trial are in alignment with previously published findings.
Some studies showed that neutralizing antibody titers correlate with vaccine efficacy in clinical trials of COVID-19 vaccines10,11,12. In our study, superior immunogenicity of S-268019-b when compared with a licensed active control vaccine with proven efficacy and effectiveness indicates the possibility that S-268019-b will provide good protection against symptomatic COVID-19 and SARS-CoV-2 infection. Clinical endpoints pertaining to the prevention of COVID-19 could not be analyzed in the current study as a result of limited statistical power, but another currently ongoing phase 3 study of S-268019-b will provide direct evidence on the potential of the vaccine to prevent COVID-19 (ClinicalTrials.gov number, NCT05212948). S-268019-b elicited robust and consistent immunogenicity in this study. The cytopathic assay in the present study showed lower levels of neutralizing antibodies in the ChAdOx1 nCoV-19 group compared with the published findings18,19,20. This likely reflects the differences in the cytopathic effect assays used across studies, and the one used in our study appears to have a lower sensitivity for detecting antibody at the lower end of the dynamic range, especially those elicited by ChAdOx1 nCoV-19. Such variability from using different assays was observed in the phase 1 trials of ChAdOx1 nCoV-1921. Indeed, most neutralizing antibody titer readings in the ChAdOx1 nCoV-19 group were below the LLoQ. However, seroconversion rates for the anti–SARS-CoV-2 S-protein IgG antibody 28 days after the second dose of S-268019-b vs ChAdOx1 nCoV-19 were 99.8% versus 98.2%, respectively. Moreover, a more sensitive cell viability assay confirmed our findings and showed a similar trend in favor of S-268019-b over ChAdOx1 nCoV-19 in neutralizing antibody responses. For primary endpoint comparison with this cell viability assay, approximately 60% of the neutralizing antibody titers for ChAdOx1 nCoV-19 were below the LLoQ. However, comparison of GMTs between S-268019-b and ChAdOx1 nCoV-19 groups using Wilcoxon rank-sum test, which is a non-parametric statistical hypothesis test, showed the robustness of the S-268019-b immunogenic response in both methods. The GMT of neutralizing antibody titer against wildtype (D614G) pseudovirus after two doses of ChAdOx1 nCoV-19 was 96 (Fig. 4a) and it was equivalent to 40 IU/mL as WHO international standard units22. Since GMTs of the neutralizing antibody titer against wildtype (D614G) pseudovirus in previous studies were 56.8 IU/mL23 and 39.0 IU/mL (median of inhibitory dilution (50%), 254 converted into WHO international standard unit)12, those were in the similar range observed in this study.
In the follow-up phase, the booster administration with S-268019-b elicited a durable neutralizing antibody response in both groups through the end of the study. Considering that the neutralizing antibodies tend to wane in 6–8 months following administration of the second dose for multiple vaccine types in previously published studies, booster application within that time frame could ensure maintenance of protective immunity24,25. Indeed, the fact that the neutralizing antibody titer following the booster dose was higher than that after the second dose suggests that immune system was adequately primed with two initial doses to mount the response in both treatment groups. Moreover, anti–SARS-CoV-2 S-protein IgG antibody titers were maintained through Day 393, further establishing the durability of the response. Notably, the magnitude of the neutralizing antibody and anti–SARS-CoV-2 S-protein IgG antibody responses as measured in GMTs was substantially higher in S-268019-b group versus that in ChAdOx1 nCoV-19, further corroborating the findings from the interim analysis 28 days after the second dose. It must be noted that results under controlled conditions in clinical trials may not always apply directly to the clinical settings.
Neutralizing antibody titers against the Omicron variant after two doses were lower for both S-268019-b and ChAdOx1 nCoV-19 compared with the wildtype with a pseudovirus assay, which aligns with previous reports on other vaccines, including ChAdOx1 nCoV-1926,27. Of note, studies have shown that a third dose of a COVID-19 vaccine increased vaccine effectiveness against the Omicron variant28. A third dose of BNT162b2 boosted neutralizing antibody titer against Omicron to a level just a couple of times lower than the neutralizing antibody titer against the wildtype, while neutralizing antibody titer against Omicron after just two doses was more than 10 times lower than that against the wildtype29. Moreover, in our earlier study, neutralizing antibody titers against the Omicron variants BA.1 and BA.2 elicited by a booster dose of S-268019-b in subjects who had received two doses of BNT162b2 as primary vaccination were similar to those seen with BNT162b2, which was reported to be effective against Omicron17. The booster dose of S-268019-b also elicited neutralizing antibody response against the more recent Omicron variants BA.4 and BA.5 in Japanese subjects who had received two doses of either mRNA-1273 or BNT162b230.
Reactogenicity was mild to moderate in most participants and comparable between the two groups. No vaccine-related SAEs or AESIs were noted in the study. Headache, fatigue, and myalgia were the most common solicited systemic AEs, while pain at the injection site was the most frequently reported solicited local AE, all in agreement with previous published reports on S-268019-b and ChAdOx1 nCoV-1916,17,18,19. Solicited AEs were more frequent in the ChAdOx1 nCoV-19 group after the first dose, and in the S-268019-b group after the second dose, showing the same trend as reported previously with both vaccines16,31.
The S-268019-b formulation utilized a squalene-based adjuvant, which has been used in other vaccine formulations. A previous study has reported that an influenza vaccine containing a similar adjuvant, deployed in the 2009 pandemic, was associated with an increased risk of narcolepsy in a certain population32; however, the association has not been detected in other epidemiological studies. No neurological AESIs, including narcolepsy, were noted in the current study. As shown in preclinical studies, S-268019-b induced strong antibody responses, likely enhanced by the use of the adjuvant. In this study, S-268019-b, the adjuvanted vaccine, induced cytokine responses similar to ChAdOx1 nCoV-19, which produces competent levels of T-cell responses33. S-268019-b predominantly induced Th1 cell cytokines, while Th2 responses were minimal, aligning with the findings of a previous study17. Th1-skewed responses are considered important in avoiding the potential for risk related to vaccine-associated enhanced disease.
Our study has many strengths. A large phase 3 randomized clinical trial has high internal validity. Higher immunogenicity and tolerability of S-268019-b were demonstrated relative to an established active control, which is already approved for use globally. Favorable immunogenicity results at 28 days after the second dose were consistent across all age-groups assessed in the study, implying robustness of the results. Moreover, immunogenicity for both groups was maintained through the duration of the study, while the magnitude of the response was consistently and substantially higher in the S-268019-b group, establishing the durability and credibility of the initial response. The study also has its limitations, however. We presented information on safety from only the interim analysis (28 days following the second dose) as the most solicited adverse AEs occur within 7–10 days of vaccine administration and resolve within a few days34. We acknowledge that this may have precluded the possibility of capturing any long-term safety signals. However, participants were followed up, up to 1 year for additional immunogenicity endpoints, which provided valuable information on the durability of responses across vaccine platforms. The limited statistical power did not allow meaningful assessment of any clinical endpoints. Consequently, the study relied on surrogate data (immunogenicity in terms of neutralizing antibodies) rather than definite clinical endpoints (e.g., SARS-CoV-2 infection or time to first SARS-CoV-2 infection). Although the measurement of neutralizing antibodies may have been limited by the relatively low sensitivity in measuring the neutralizing antibody titer in the ChAdOx1 nCoV-19 group in one method, the more sensitive method also corroborated the same findings from the first method. Inclusion of a low number of non-Japanese study participants and a low number of elderly participants and those with risk factors for COVID-19 who need vaccination reduce generalizability of the current study. An ongoing study with S-268019-b specifically in the elderly is expected to address this gap. Regardless, our study adds value as a large comparative phase 3 study report of a recombinant protein vaccine showing superior neutralizing antibody induction than that observed with a globally COVID-19 vaccine in Japanese participants. The immune responses were durable and sustained through the duration of the study following booster administration. Importantly, the strong immunogenicity of the vaccine was not produced at the expense of tolerability. Future plans will include updating of the spike protein of S-268019-b in accordance with the recommendations of healthcare authorities in response to evolving SARS-CoV-2 variants, consistent with the examples of recombinant influenza vaccines.
Conclusion
The results of this phase 3 study show superior neutralizing antibody responses 28 days after the second dose of and an acceptable safety profile for the S-268019-b vaccine with a modified recombinant spike protein of SARS-CoV-2 antigen, formulated with a squalene-based adjuvant, compared with the ChAdOx1 nCoV-19 vaccine.
Data availability
The datasets analyzed in this study are available on reasonable request of researchers through the clinical study data request platform (https://vivli.org/) after the researchers and SHIONOGI Group enter into a contract (which will have certain requirements with respect to personal data privacy, confidentiality, and compliance with the law). For further details, please refer to the websites of Shionogi & Co, Ltd (https://www.shionogi.com/shionogi/global/en/company/policies/shionogi-group-clinical-trial-data-transparency-policy.html).
References
World Health Organization. WHO coronavirus (COVID-19) dashboard. Available from: https://covid19.who.int. Accessed 12 December 2023.
World Health Organization. COVID-19 vaccine tracker and landscape. Available from https://www.who.int/publications/m/item/draft-landscape-of-covid-19-candidate-vaccines. Accessed 12 December 2023.
Choe, P. G. et al. Waning antibody responses in asymptomatic and symptomatic SARS-CoV-2 infection. Emerg. Infect. Dis. 27(1), 327–329 (2021).
Pavot, V. et al. Protein-based SARS-CoV-2 spike vaccine booster increases cross-neutralization against SARS-CoV-2 variants of concern in non-human primates. Nat. Commun. 13(1), 1699. https://doi.org/10.1038/s41467-022-29219-2 (2022).
Polack, F. P. et al. Safety and efficacy of the BNT162b2 mRNA Covid-19 vaccine. N. Engl. J. Med. 383(27), 2603–2615. https://doi.org/10.1056/NEJMoa2034577 (2020).
Baden, L. R. et al. Efficacy and safety of the mRNA-1273 SARS-CoV-2 vaccine. N. Engl. J. Med. 384(5), 403–416. https://doi.org/10.1056/NEJMoa2035389 (2021).
Voysey, M. et al. Safety and efficacy of the ChAdOx1 nCoV-19 vaccine (AZD1222) against SARS-CoV-2: An interim analysis of four randomised controlled trials in Brazil, South Africa, and the UK. Lancet 397(10269), 99–111. https://doi.org/10.1016/S0140-6736(20)32661-1 (2021).
Heath, P. T. et al. Safety and efficacy of NVX-CoV2373 Covid-19 vaccine. N. Engl. J. Med. 385(13), 1172–1183. https://doi.org/10.1056/NEJMoa2107659 (2021).
Sadoff, J. et al. Safety and efficacy of single-dose Ad26.COV2.S vaccine against Covid-19. N. Engl. J. Med. 384(23), 2187–2201. https://doi.org/10.1056/NEJMoa2101544 (2021).
Khoury, D. S. et al. Neutralizing antibody levels are highly predictive of immune protection from symptomatic SARS-CoV-2 infection. Nat. Med. 27(7), 1205–1211. https://doi.org/10.1038/s41591-021-01377-8 (2021).
Krammer, F. A correlate of protection for SARS-CoV-2 vaccines is urgently needed. Nat. Med. 27(7), 1147–1148. https://doi.org/10.1038/s41591-021-01432-4 (2021).
Feng, S. et al. Correlates of protection against symptomatic and asymptomatic SARS-CoV-2 infection. Nat. Med. 27(11), 2032–2040. https://doi.org/10.1038/s41591-021-01540-1 (2021).
Lazarus, R. et al. Immunogenicity and safety of an inactivated whole-virus COVID-19 vaccine (VLA2001) compared with the adenoviral vector vaccine ChAdOx1-S in adults in the UK (COV-COMPARE): interim analysis of a randomised, controlled, phase 3, immunobridging trial. Lancet Infect. Dis. 22(12), 1716–1727. https://doi.org/10.1016/S1473-3099(22)00502-3 (2022).
World Health Organization. Statement for healthcare professionals: How COVID-19 vaccines are regulated for safety and effectiveness (Revised March 2022). Joint Statement from the International Coalition of Medicines Regulatory Authorities and World Health Organization Available from https://www.who.int/news/item/17-05-2022-statement-for-healthcare-professionals-how-covid-19-vaccines-are-regulated-for-safety-and-effectiveness. Accessed 12 December 2023.
Hashimoto, M. et al. Immunogenicity and protective efficacy of SARS-CoV-2 recombinant S-protein vaccine S-268019-b in cynomolgus monkeys. Vaccine 40(31), 4231–4241. https://doi.org/10.1016/j.vaccine.2022.05.081 (2022).
Iwata, S. et al. Phase 1/2 clinical trial of COVID-19 vaccine in Japanese participants: A report of interim findings. Vaccine 40(27), 3721–3726. https://doi.org/10.1016/j.vaccine.2022.04.054 (2022).
Shinkai, M. et al. Immunogenicity and safety of booster dose of S-268019-b or BNT162b2 in Japanese participants: An interim report of phase 2/3, randomized, observer-blinded, noninferiority study. Vaccine 40(32), 4328–4333. https://doi.org/10.1016/j.vaccine.2022.06.032 (2022).
Ramasamy, M. N. et al. Safety and immunogenicity of ChAdOx1 nCoV-19 vaccine administered in a prime-boost regimen in young and old adults (COV002): A single-blind, randomised, controlled, phase 2/3 trial. Lancet 396(10267), 1979–1993. https://doi.org/10.1016/S0140-6736(20)32466-1 (2021).
Falsey, A. R. et al. Phase 3 safety and efficacy of AZD1222 (ChAdOx1 nCoV-19) Covid-19 vaccine. N. Engl. J. Med. 385(25), 2348–2360. https://doi.org/10.1056/NEJMoa2105290 (2021).
Asano, M. et al. Immunogenicity and safety of AZD1222 (ChAdOx1 nCoV-19) against SARS-CoV-2 in Japan: A double-blind, randomized controlled phase 1/2 trial. Int. J. Infect. Dis. 114, 165–174. https://doi.org/10.1016/j.ijid.2021.10.030 (2022).
Folegatti, P. M. et al. Safety and immunogenicity of the ChAdOx1 nCoV-19 vaccine against SARS-CoV-2: A preliminary report of a phase 1/2, single-blind, randomised controlled trial. Lancet 396(10249), 467–478 (2020). doi: https://doi.org/10.1016/S0140-6736(20)31604-4. Erratum in: Lancet 396(10249), 466 (2020). Erratum in: Lancet 396(10266), 1884 (2020).
World Health Organization. Establishment of the WHO International Standard and Reference Panel for anti-SARS-CoV-2 antibody. Available from: https://cdn.who.int/media/docs/default-source/biologicals/ecbs/bs-2020-2403-sars-cov-2-ab-ik-17-nov-2020_4ef4fdae-e1ce-4ba7-b21a-d725c68b152b.pdf. Accessed 10 May 2023.
Kulkarni, P. S. et al. A phase 2/3, participant-blind, observer-blind, randomised, controlled study to assess the safety and immunogenicity of SII-ChAdOx1 nCoV-19 (COVID-19 vaccine) in adults in India. EClinicalMedicine. 42, 101218. https://doi.org/10.1016/j.eclinm.2021.101218 (2021).
Gobeil, P. et al. Durability and cross-reactivity of immune responses induced by a plant-based virus-like particle vaccine for COVID-19. Nat. Commun. 13, 6905. https://doi.org/10.1038/s41467-022-34728-1 (2022).
Korosec, C. S. et al. Long-term durability of immune responses to the BNT162b2 and mRNA-1273 vaccines based on dosage, age and sex. Sci. Rep. 12, 21232. https://doi.org/10.1038/s41598-022-25134-0 (2022).
Muik, A. et al. Neutralization of SARS-CoV-2 Omicron by BNT162b2 mRNA vaccine-elicited human sera. Science 375(6581), 678–680. https://doi.org/10.1126/science.abn7591 (2022).
Madhi, S. A. et al. Efficacy of the ChAdOx1 nCoV-19 Covid-19 vaccine against the B.1.351 variant. N. Engl. J. Med. 384(20), 1885–1898. https://doi.org/10.1056/NEJMoa2102214 (2021).
UK Health Security Agency. SARS-CoV-2 variants of concern and variants under investigation in England. 2021. Technical briefing 31. https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1040076/Technical_Briefing_31.pdf. Date: Dec 10, 2021. Accessed 12 December 2023.
Yu, J. et al. Neutralization of the SARS-CoV-2 Omicron BA.1 and BA.2 variants. N. Engl. J. Med. 386(16), 1579–1580. https://doi.org/10.1056/NEJMc2201849 (2022).
Sonoyama, T. et al. Safety and immunogenicity of a booster dose of S-268019-b: Interim findings of a Phase 3, open-label clinical study in Japan. Vaccine X. 15, 100390. https://doi.org/10.1016/j.jvacx.2023.100390 (2023).
Vaxzevria™ Package Insert, 5th edition. April 2022. https://www.ema.europa.eu/en/documents/product-information/vaxzevria-previously-covid-19-vaccine-astrazeneca-epar-product-information_en.pdf. Accessed 12 December 2023.
Montplaisir, J. et al. Risk of narcolepsy associated with inactivated adjuvanted (AS03) A/H1N1 (2009) pandemic influenza vaccine in Quebec. PLoS One 9(9), 108489. https://doi.org/10.1371/journal.pone.0108489 (2014).
Ewer, K. J. et al. T cell and antibody responses induced by a single dose of ChAdOx1 nCoV-19 (AZD1222) vaccine in a phase 1/2 clinical trial. Nat. Med. 27(2), 270–278. https://doi.org/10.1038/s41591-020-01194-5 (2021).
Dhamanti, I. et al. Adverse reactions of COVID-19 vaccines: A scoping review of observational studies. Int. J. Gen. Med. 20(16), 609–618. https://doi.org/10.2147/IJGM.S400458 (2023).
Acknowledgements
We thank AstraZeneca for providing the ChAdOx1 nCoV-19 vaccine. We also thank Ken J Ishii and Norio Ohmagari for their contribution to development of this manuscript, Naomi M Seki and Ken Yoshihara for conducting neutralizing antibody titer testing against the variant viruses, and Satoshi Kojima for the management of this publication. We also thank Vidula Bhole and Ivan D’Souza of MedPro Clinical Research for providing medical writing support for this manuscript. This work was funded by Shionogi & Co., Ltd., and Ministry of Health, Labour and Welfare (MHLW) under its supplementary budget for emergency maintenance associated with the vaccine production system. Preparation of clinical trial materials of S-268019-b was supported by Japan Agency for Medical Research and Development (AMED) under Grant Number JP21nf0101626. Medical writing support by MedPro Clinical Research was funded by Shionogi & Co., Ltd. Shionogi & Co., Ltd., was involved in study design; in the collection, analysis, and interpretation of data; in the writing of the report; and in the decision to submit the paper for publication.
Author information
Authors and Affiliations
Contributions
SI, YT, SO, RYS, KI, TH, MA and TS contributed to conceptualization. YT, SO, RYS and KI contributed to data curation and validation. YT, RYS and TH contributed to formal analysis. All authors contributed to methodology and data interpretation. KI and MA contributed to funding acquisition and project administration. SI and TS contributed to investigation. MA contributed to supervision. All authors contributed to revision and editing the draft manuscript. All authors read and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
SI received payment or honoraria for lectures, presentations, speakers’ bureaus, manuscript writing, and educational events from Astellas Pharma Inc., Gilead Sciences, Inc., Japan Vaccine Co., Ltd., Meiji Seika Pharma Co., Ltd., Pfizer Japan Inc., and Taisho Toyama Pharmaceutical Co. Ltd., in addition to consulting fees from Shionogi & Co., Ltd. for advisory board participation. AJP is chair of the UK Department of Health and Social Care’s (DHSC) Joint Committee on Vaccination and Immunisation (JCVI) but does not take part in the JCVI COVID-19 committee. AJP’s employer, Oxford University has entered into a partnership with AstraZeneca for the development of a COVID-19 vaccine. AJP has received consulting fees for providing advice to Shionogi & Co., Ltd., on the development of the COVID-19 vaccine. AJP has received grants from Bill and Melinda Gates Foundation, Wellcome Trust, UK Research and Innovation Medical Research Council, and National Institute of Health and Care Research. YT, SO, RYS, KI, TH, MA, and TS are employees of Shionogi & Co., Ltd. TH and TS own stocks in Shionogi & Co., Ltd. YT owns stocks in Ono Pharmaceutical Co., Ltd. and Shionogi & Co., Ltd.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Iwata, S., Pollard, A.J., Tada, Y. et al. A phase 3 randomized controlled trial of a COVID-19 recombinant vaccine S-268019-b versus ChAdOx1 nCoV-19 in Japanese adults. Sci Rep 14, 9830 (2024). https://doi.org/10.1038/s41598-024-57308-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-57308-3
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}