
Abstract
Acute kidney injury (AKI) following hyperthermic intraperitoneal chemotherapy (HIPEC) is common. Identifying patients at risk could have implications for surgical and anesthetic management. We aimed to develop a predictive model that could predict AKI based on patients’ preoperative characteristics and intraperitoneal chemotherapy regimen. We retrospectively gathered data of adult patients undergoing HIPEC at our health system between November 2013 and April 2022. Next, we developed a model predicting postoperative AKI using multivariable logistic regression and calculated the performance of the model (area under the receiver operating characteristics curve [AUC]) via tenfold cross-validation. A total of 412 patients were included, of which 36 (8.7%) developed postoperative AKI. Based on our multivariable logistic regression model, multiple preoperative and intraoperative characteristics were associated with AKI. We included the total intraoperative cisplatin dose, body mass index, male sex, and preoperative hemoglobin level in the final model. The mean area under the receiver operating characteristics curve value was 0.82 (95% confidence interval 0.71–0.93). Our risk model predicted AKI with high accuracy in patients undergoing HIPEC in our institution. The external validity of our model should now be tested in independent and prospective patient cohorts.
Similar content being viewed by others

Introduction
Hyperthermic intraperitoneal chemotherapy (HIPEC) following cytoreductive therapy has become a common treatment for peritoneal metastases from mesothelioma, colorectal, gastric, appendiceal, ovarian, and primary peritoneal cancer1. Advantages include higher concentrations of heated chemotherapeutic agents with improved cytotoxicity and limited systemic side effects2.
Still, acute kidney injury (AKI) following HIPEC remains a known and common complication3,4,5,6,7, which is associated with increased length of stay and major postoperative morbidities8. While prior prediction models for AKI have focused on patients presenting for non-cardiac surgery9,10, patients undergoing HIPEC are exposed to more unique causes of AKI, including nephrotoxic chemotherapy agents3,4,5,6,7, excessive blood loss5,8, increased intraabdominal pressure during intraperitoneal perfusion5, and vasodilation related to induced hyperthermia intraoperatively11. Most recent literature focuses on intraoperative and postoperative interventions to reduce the risk of AKI following HIPEC12,13. But little is known about the ability to stratify the risk of postoperative AKI in this surgical patient population preoperatively.
Identifying patients at risk of AKI prior to HIPEC could have implications for the surgical and anesthetic plan. Modifiable risk factors can be optimized, nephrotoxic medication can be held prior to surgery, adjustments can be made to the type and dosing of intraperitoneal chemotherapeutic drugs, and alternative intraoperative hemodynamic monitoring techniques could be applied14. Thus, the objective of this study was to develop a predictive model for postoperative AKI using preoperative features such as demographics, chronic comorbidities, preoperative laboratory tests, home medications, and the chosen chemotherapy agent.
Methods
Our study was approved by the University of California San Diego Institutional Review Board (IRB number 804874) and was carried out in accordance with the principles of the Declaration of Helsinki15. All methods were performed in accordance with the relevant guidelines and regulations. This study followed the Transparent Reporting of a multivariable prediction model for Individual Prognosis Or Diagnosis (TRIPOD) recommendations16. The aim of this study was to develop a predictive model for postoperative AKI based on data from the institution’s electronic health record (EHR) via manual chart review. Investigators were identified and authenticated via username and password, granting access to the institutional EHR. Password-protected and de-identified patient information was used for data analysis.
All adult patients that underwent HIPEC at the health system between November 2013 and April 2022 were eligible for inclusion. Exclusion criteria were age < 18 years old, patients who were scheduled but did not undergo intraoperative HIPEC, and patients on dialysis prior to surgery. The primary outcome of the study was postoperative AKI and defined as the difference between postoperative and preoperative creatinine closest to surgery ≥ 0.3 mg/dl within 48 postoperative hours or a quotient of postoperative and preoperative creatinine closest to surgery ≥ 1.5 within 7 postoperative days (KDIGO stage 1 or higher)8,17.
Covariates in the model were those known preoperatively and included: (1) patient demographics, (2) chronic comorbidities, (3) laboratory tests, (4) and medications prior to surgery. Patient demographics included: age in years, body mass index (BMI) in kg/m2 as continuous variables, and legal sex, race, and ethnicity as categorical variables. Chronic comorbidities were chosen from previously reported findings based on relevant pre-existing International Classification of Diseases codes (ICD-10) (Supplementary Table 1). These included the categorical variables: cardiac disease, asthma, chronic obstructive pulmonary disease (COPD), other pulmonary disease, hypertension, diabetes mellitus, renal disease, and liver disease. Laboratory tests were treated as categorical variables in the univariate and included preoperative creatinine, blood urea nitrogen (BUN), potassium, bicarbonate, total bilirubin, hemoglobin, platelet count, and glomerular filtration rate (GFR). Chronic kidney disease was defined as a preoperative estimated GFR < 60 ml/min/1.73 m218. Anemia was defined as a hemoglobin level below 12 mg/dl for females and 13 mg/dl for males9,19. Categorical covariates on medications taken prior to surgery included renin inhibitors, nonsteroidal anti-inflammatory drugs (NSAIDs), nephrotoxic antiviral drugs, antibiotics, antifungals, chemotherapeutic agents, and antiepileptic drugs (Supplementary Table 2). AKI associated with intraperitoneal chemotherapy is dose-dependent3, and the intraoperative dosing of chemotherapeutic agents is standardized or otherwise determined preoperatively20. Therefore, we also considered the intraperitoneal dose of cisplatin, carboplatin, doxorubicin, gemcitabine, and mitomycin as continuous variables in our model.
R Statistical Programming Language (v4.4.2) was used for all statistical analyses. Initially, we compared statistical differences in each covariate in the two cohorts—patients who did not develop postoperative AKI versus patients that did develop postoperative AKI—using chi-squared test or Fisher’s exact test for categorical and Wilcoxon Rank Sum test or t-test for continuous variables, respectively. A P < 0.05 was considered statistically significant. To develop a predictive model, we utilized multivariable logistic regression with feature selection. The features selected for the final model were preoperatively known variables that had an association with the primary outcome on univariate logistic regression with P < 0.2 based on recommendations for prediction modeling21. After plotting the receiver operating characteristics curve (package pROC_1.18.5), model performance was measured by the area under the receiver operating characteristics curve (AUC). To calculate the AUC, we performed tenfold cross-validation, in which the entire dataset was split into 10 folds. Of those folds, nine served as the training set and one as the test set. The model was trained on the training set, and the AUC of that model was calculated on the test set. This was repeated until each fold served as the test set. The average AUC was then reported. Furthermore, to account for class imbalance, we applied Synthetic Minority Oversampling Technique (SMOTE) on the nine training folds (package smotefamily_1.3.1) when training the model for each iteration22. A dataset is considered imbalanced if there are large differences in the rate of negative versus positive outcomes. SMOTE takes samples of the feature space of the minority class (in this case, patients with postoperative AKI) and five of its nearest neighbors. Using this data, SMOTE then synthesizes new cases that combine features of the target case with features of its nearest neighbors by multiplying the difference between the examples by a number between 0 and 1. With the newly generated synthetic data for the minority class, the balance between the negative and positive classes becomes more balanced. Improving the balance between negative and positive classes may improve predictive performance of the models. Of note, SMOTE was only applied to training data and not test data.
We estimated the sample size needed for logistic regression using the equation N = 100 + EPV*i23, where the rule of event per variable (EPV) is 50 and i is the number of independent variables in the final model. The final model had four features; thus, the calculated sample size was 300.
Ethics approval and consent to participate
The Institutional Review Board was approved (IRB number 804874), and the requirement for informed consent was waived.
Results
During the study period, there were 556 patients who were scheduled to undergo HIPEC at our institution. After exclusion of ineligible participants, the final study population consisted of 412 patients, of which 36 (8.7%) developed postoperative AKI. Between the two cohorts (no postoperative AKI versus AKI), there were statistically significant differences between the following covariates: White, Black, preoperative total bilirubin and creatinine levels, cisplatin, doxorubicin, and mitomycin dose, crystalloids, packed red blood cell (PRBC) transfusions, and estimated blood loss (Table 1).
Male sex, BMI, White, Black, preoperative hemoglobin and total bilirubin levels, coronary artery disease, diabetes mellitus, lung disease other than COPD or asthma, NSAIDs taken prior to surgery, estimated blood loss, crystalloids, colloids, PRBC and platelet transfusions, the total intraoperative dose of phenylephrine and ephedrine as well as the total intraoperative dose of mitomycin, cisplatin, and doxorubicin had an association with the primary outcome in the univariate regression modeling AKI (Table 2).
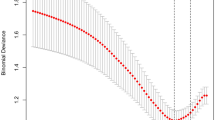
For our final model, multivariable logistic regression was utilized with the features BMI (OR 1.073, 95% CI 1.006–1.144, P = 0.031), preoperative hemoglobin level (OR 0.738, 95% CI 0.589–0.925, P = 0.008), male sex (2.033, 95% CI 0.905–4.567, P = 0.086), and intraperitoneal cisplatin (OR 1.023, 95% CI 1.015–1.031, P < 0.001) (Table 3). In Fig. 1, a plot illustrates the mean AUC (0.82, 95% confidence interval 0.71–0.93) from cross-validation.

Plot illustrating mean (95% confidence intervals) area under the receiver operating characteristics curve from cross-validation.
Based on the logistic regression model for predicting postoperative AKI in patients undergoing HIPEC surgery, the probability of the outcome may be calculated with the following equation:
Thus, the probability of postoperative AKI can be estimated and compared to other patients with different combinations of risk factors. For example, if a male patient had a BMI of 30 kg/m2, preoperative hemoglobin of 16 g/dl, and did not receive cisplatin, the probability of AKI would be:
The same patient, but with a preoperative hemoglobin of 8, would have the following probability:
Discussion
In our study, 8.7% of patients undergoing HIPEC developed postoperative AKI. Our primary outcome was associated with multiple preoperatively known variables and intraoperatively administered chemotherapeutic agents. The final predictive model for AKI included BMI, hemoglobin, male sex, and total dose of intraperitoneal cisplatin in our final model, which accurately predicted postoperative AKI (AUC of 0.82).
Obesity is a known independent risk factor of perioperative renal dysfunction, likely explained by proinflammatory, hemodynamic, and pharmacokinetic factors unique to obese patients24,25. Not surprisingly, low hemoglobin levels preoperatively are independent predictors of postoperative AKI in cardiac and non-cardiac surgery9,26. Male sex is associated with postoperative AKI and forms part of multiple validated risk scores9,27. Cisplatin is a known nephrotoxic drug and strongly associated with perioperative AKI following intraperitoneal administration3,4,5,6,7.
Prior univariate and multivariate regression analyses of patients undergoing HIPEC have found associations between postoperative AKI and a multitude of variables such as age, obesity, preoperative creatinine and urea levels, intraperitoneal cisplatin, excessive blood loss, low perioperative diuresis, and the extent of peritoneal cancer3,4,5,6,8. Our retrospective study analyzed one of the most extensive data sets focusing on this surgical patient population. Prior retrospective analyses have focused on identifying different risk factors for postoperative AKI. This study developed a predictive model for postoperative renal injury following HIPEC and could, thus, be utilized to identify patients at risk and optimize these patients preoperatively.
In our study, 8.7% developed postoperative AKI, which is less common than previously reported. The incidence in other studies varies between 11.1 and 47.5% and is likely related to different guidelines on defining postoperative AKI and varying use of cisplatin3,4,5,6,7,26. As expected, our study found a dose-dependent association between cisplatin and AKI. Furthermore, the intraperitoneal dose of doxorubicin was also associated with AKI, previously only described for systemic administration28,29. However, doxorubicin was only administered in conjunction with cisplatin. We, therefore, did not include doxorubicin in our final model to avoid confounding.
Postoperative AKI is associated with increased length of stay and health care costs, chronic kidney disease, dialysis-dependence, and death27. Risk indices for perioperative AKI in non-cardiac surgery have been developed in the past, identifying similar predictors such as male sex and anemia, amongst others9,30. However, HIPEC exposes patients to unique risk factors, such as cisplatin3,4,5,6,7, and increased intraabdominal pressure possibly exacerbated by obesity5. Our model could predict postoperative AKI with high discriminatory ability based on only four predictors.
Identifying patients at risk of AKI prior to HIPEC could have implications to the surgical and anesthetic plan. The volume status of patients with risk factors such as male sex and high BMI can be optimized prior to surgery. When possible, nephrotoxic medication should be replaced by equally effective alternative drugs14,17. In patients at high risk for AKI, adjustments can be made to the type or dosing of intraperitoneal chemotherapeutic agent. Preexisting anemia can be corrected before proceeding with surgery26, preoperative weight loss in obese patients can be encouraged31, and nephroprotective measures such as invasive intraoperative hemodynamic monitoring could be applied to patients at risk32. In the immediate postoperative period, renin inhibitors and contrast should be avoided, and glucose levels should be well controlled17.
Our study has several limitations. First, retrospective data analyses, in general, are confounded by missed data or unaccounted confounding variables. We excluded patients with the most critical data missing, such as type and dosing of intraperitoneal chemotherapy, and imputed missing laboratory values by utilizing the cohort’s median. While data imputation can affect a model’s external validity, it was only implemented for missing preoperative bicarbonate and bilirubin levels, neither included in the final model. Second, we were constrained to the covariates, which were selected and collected from our institutional EHR. Diagnoses of comorbidities were binary and did not include stages of severity. Still, our data set was extensive including patient’s baseline laboratory data, which are often utilized to stage end-organ injury such as creatinine and total bilirubin for renal and liver dysfunction17,33. We intentionally limited the covariates in our model to preoperatively known data points allowing clinicians to adjust anesthetic and surgical plans. However, we decided to include the type and dosing of intraperitoneal chemotherapeutic agent as it is often chosen prior to surgery and a known contributor to nephrotoxicity6. Lastly, there was no separate external validation set for the study and hence, the reported accuracy of the model has limited generalizability. We, therefore, further need to conduct external validation using data outside of our institutional dataset. The discriminatory ability of our model might be lower in other patient populations from different geographic locations and socioeconomic backgrounds.
To conclude, our model was able to predict AKI within the first seven days postoperatively in patients undergoing HIPEC in our institution and provides the surgical and anesthesia team with a potentially helpful preoperative tool. Future trials must confirm the external validity of our model.
Data availability
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Auer, R. C. et al. Indications for hyperthermic intraperitoneal chemotherapy with cytoreductive surgery: A systematic review. Eur. J. Cancer 127, 76–95 (2020).
Wong, L. C. K. et al. High intra-abdominal pressure during hyperthermic intraperitoneal chemotherapy (HIPEC) following cytoreductive surgery (CRS) for peritoneal surface malignancies. Int. J. Hyperthermia 39(1), 1195–1201 (2022).
Liesenfeld, L. F. et al. HIPEC-induced acute kidney injury: A retrospective clinical study and preclinical model. Ann. Surg. Oncol. 29(1), 139–151 (2022).
Angeles, M. A. et al. Predictive risk factors of acute kidney injury after cytoreductive surgery and cisplatin-based hyperthermic intra-peritoneal chemotherapy for ovarian peritoneal carcinomatosis. Int. J. Gynecol. Cancer 29(2), 382–391 (2019).
Cata, J. P. et al. Identification of risk factors associated with postoperative acute kidney injury after cytoreductive surgery with hyperthermic intraperitoneal chemotherapy: A retrospective study. Int. J. Hyperthermia 34(5), 538–544 (2018).
Chen, K. L., Shamavonian, R., Karpes, J. B., Alzahrani, N. A. & Morris, D. L. Acute kidney injury following hyperthermic intraperitoneal chemotherapy with cisplatin. Anticancer Res. 41(3), 1641–1646 (2021).
Ye, J. et al. Nephrotoxicity and long-term survival investigations for patients with peritoneal carcinomatosis using hyperthermic intraperitoneal chemotherapy with cisplatin: A retrospective cohort study. Surg. Oncol. 27(3), 456–461 (2018).
Naffouje, S. A., Tulla, K. A., Chorley, R., Armstrong, N. & Salti, G. I. Acute kidney injury increases the rate of major morbidities in cytoreductive surgery and HIPEC. Ann. Med. Surg. (Lond.) 35, 163–168 (2018).
Park, S. et al. Simple postoperative AKI risk (SPARK) classification before noncardiac surgery: A prediction index development study with external validation. J. Am. Soc. Nephrol. 30(1), 170–181 (2019).
Lei, V. J. et al. Risk stratification for postoperative acute kidney injury in major noncardiac surgery using preoperative and intraoperative data. JAMA Netw. Open 2(12), e1916921 (2019).
Cooksley, T. J. & Haji-Michael, P. Post-operative critical care management of patients undergoing cytoreductive surgery and heated intraperitoneal chemotherapy (HIPEC). World J. Surg. Oncol. 9, 169 (2011).
Laplace, N. et al. Sodium thiosulfate protects from renal impairement following hyperthermic intraperitoneal chemotherapy (HIPEC) with Cisplatin. Int. J. Hyperthermia 37(1), 897–902 (2020).
Liu, G. et al. Treatment of hypermyoglobinemia after CRS + HIPEC for patients with peritoneal carcinomatosis: A retrospective comparative study. Medicine (Baltimore) 96(45), e8573 (2017).
Romagnoli, S., Ricci, Z. & Ronco, C. Perioperative acute kidney injury: Prevention, early recognition, and supportive measures. Nephron 140(2), 105–110 (2018).
World Medical A. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 310(20), 2191–2194 (2013).
Collins, G. S., Reitsma, J. B., Altman, D. G. & Moons, K. G. Transparent Reporting of a multivariable prediction model for Individual Prognosis Or Diagnosis (TRIPOD): The TRIPOD statement. Br. J. Surg. 102(3), 148–158 (2015).
Khwaja, A. KDIGO clinical practice guidelines for acute kidney injury. Nephron. Clin. Pract. 120(4), c179-184 (2012).
National Kidney, F. K/DOQI clinical practice guidelines for chronic kidney disease: Evaluation, classification, and stratification. Am. J. Kidney Dis. 39(2 Suppl 1), S1-266 (2002).
Cappellini, M. D. & Motta, I. Anemia in clinical practice-definition and classification: Does hemoglobin change with aging?. Semin. Hematol. 52(4), 261–269 (2015).
Kuijpers, A. M. et al. Implementation of a standardized HIPEC protocol improves outcome for peritoneal malignancy. World J. Surg. 39(2), 453–460 (2015).
Steyerberg, E. W. & Van Calster, B. Redefining significance and reproducibility for medical research: A plea for higher P-value thresholds for diagnostic and prognostic models. Eur. J. Clin. Investig. 50(5), e13229 (2020).
Chawla, N. B. K., Hall, L. & Kegelmeyer, W. SMOTE: Synthetic minority over-sampling technique. J. Artif Intell. Res. 16, 321–357 (2002).
Bujang, M. A., Sa’at, N., Sidik, T. & Joo, L. C. Sample size guidelines for logistic regression from observational studies with large population: Emphasis on the accuracy between statistics and parameters based on real life clinical data. Malays. J. Med. Sci. 25(4), 122–130 (2018).
Suneja, M. & Kumar, A. B. Obesity and perioperative acute kidney injury: a focused review. J. Crit. Care 29(4), 694 e691-696 (2014).
Kheterpal, S. et al. Predictors of postoperative acute renal failure after noncardiac surgery in patients with previously normal renal function. Anesthesiology 107(6), 892–902 (2007).
Gumbert, S. D. et al. Perioperative acute kidney injury. Anesthesiology 132(1), 180–204 (2020).
Prowle, J. R. et al. Postoperative acute kidney injury in adult non-cardiac surgery: Joint consensus report of the acute disease quality initiative and perioperative quality initiative. Nat. Rev. Nephrol. 17(9), 605–618 (2021).
Mohamed, N., Goldstein, J., Schiff, J. & John, R. Collapsing glomerulopathy following anthracycline therapy. Am. J Kidney Dis 61(5), 778–781 (2013).
Carron, P. L., Padilla, M. & Maurizi Balzan, J. Nephrotic syndrome and acute renal failure during pegylated liposomal doxorubicin treatment. Hemodial. Int. 18(4), 846–847 (2014).
Kheterpal, S. et al. Development and validation of an acute kidney injury risk index for patients undergoing general surgery: Results from a national data set. Anesthesiology 110(3), 505–515 (2009).
Sun, Y. et al. Association of preoperative body weight and weight loss with risk of death after bariatric surgery. JAMA Netw. Open 3(5), e204803 (2020).
Salmasi, V. et al. Relationship between intraoperative hypotension, defined by either reduction from baseline or absolute thresholds, and acute kidney and myocardial injury after noncardiac surgery: A retrospective cohort analysis. Anesthesiology 126(1), 47–65 (2017).
Nayak, S. L., Kumar, M., Bihari, C. & Rastogi, A. Bile cast nephropathy in patients with acute kidney injury due to hepatorenal syndrome: A postmortem kidney biopsy study. J. Clin. Transl. Hepatol. 5(2), 92–100 (2017).
Author information
Authors and Affiliations
Contributions
M.K. helped collect the data, interpreted the results, drafted the manuscript, and read and approved the final manuscript. S.M. helped collect the data and read and approved the final manuscript. J.V. read and approved the final manuscript. J.B. read and approved the final manuscript. A.L. read and approved the final manuscript. R.G. helped collect the data, interpreted the results, and drafted the manuscript, and read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Krause, M., Mehdipour, S., Veerapong, J. et al. Development of a predictive model for risk stratification of acute kidney injury in patients undergoing cytoreductive surgery with hyperthermic intraperitoneal chemotherapy. Sci Rep 14, 6630 (2024). https://doi.org/10.1038/s41598-024-54979-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-54979-w
Keywords
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
