
Abstract
There are no reports on hip kinetics including contact forces and muscle activities during the golf swing after total hip arthroplasty (THA). The aim of this study was to identify the characteristics of three-dimensional dynamics during the golf swing. Ten unilateral primary THA patients participated in motion capture test of their driver golf swing. The driver swing produced approximately 20–30° of rotation in both lead and trail replaced hips. The mean hip contact forces (HCFs) of lead and trail replaced hips were 5.1 and 6.6 × body weight, respectively. Left and right THAs showed similar HCFs of lead and trail hips. More than 60% of the Percent maximum voluntary isometric contraction was found in bilateral iliopsoas muscles in all unilateral THA. Three factors [female sex, lower modified Harris Hip Score, and higher HCF of surgical side] were associated with the golf-related replacement hip pain. Golf is an admissible sport after THA because driver swings do not contribute excessive rotation or contact forces to hip prostheses. HCF could be reduced through swing adjustments, which may allow patients with golf-related replacement hip pain to develop a comfortable golf game free from pain.
Similar content being viewed by others

Introduction
Total hip arthroplasty (THA) is one of the most successful orthopedic procedures1. Golf is a globally popular sport with participants from a broad range of ages with a significant portion having a hip replacement (1–9.5%)2,3,4, making it the most common sport followed by walking, swimming, gymnastics, and cycling5,6. While golf is not considered to be a high-impact sport and the majority of attending surgeons recommend a return to golf after THA, no previous study has addressed the kinetic data of golfers performing a drive after THA7.
D’Lima et al. showed that a golf swing produces an in vivo contact force of 4.5 × body weight (BW) on the lead knee and 3.2 × BW on the trailing knee in total knee arthroplasty (TKA) patients, similar to the peak load during jogging8. The percentage of TKA patients that felt mild pain during and after playing golf were 16% and 35%, respectively. The pain was greater in the lead knee because of the higher force applied to the lead knee while hitting the ball9. Mallon et al. recorded that 11% and 41% of THA patients have mild pain during and after playing, respectively10. A recent study reports that 98% of patients return to golf after THA, with an improvement in pain visual analog scale (VAS) from 6.4 to 2.5 while playing11.
Using image-matching techniques, Hara et al. have demonstrated that the golf swing does not produce excessive hip rotation or cup-head translation after THA. However, there are no reports on hip kinetics including contact force in the golf swing after THA12.
The present study aimed to address: (1) three-dimensional (3D) motion including hip range of motion (RoM), (2) HCF and hip muscle activation, and (3) the influencing factors for replaced hip pain related golf actions. Query ID="Q4" Text="Please note we have moved the section “Ethics approval and consent to participate, Informed consent” to the end of the methods, as per house style".
Methods
Patients
All patients (n = 1197) underwent primary cementless THA in our institution between January 2008 and December 2018. Among them, 766 satisfied each of the following inclusion criteria: (1) alive at the time of the survey and (2) evaluation by a surgeon within the past two years. A review of medical records revealed that 17 patients (2.2%) were recreational golfers. Of the 17 golfers, the following were excluded: three patients with bilateral THAs, one patient hospitalized with a medical condition, one with back pain that made swinging difficult, and one declined participation; the remaining 10 patients signed an institutional review board-approved (IRB Number: 2019–323) informed consent. All THAs were performed using a posterolateral approach, with a uniform protocol for postoperative rehabilitation13.
Radiographic data
Leg length difference (LLD) and global femoral offset (GFO) before and after THA were assessed using anteroposterior radiographs of the pelvis as described previously14,15.
Patient reported outcome measurements
VAS pain scores in which a respondent selects a whole number (0–10) while playing and after playing golf, and the Modified Harris Hip Score (mHHS) were assessed during the dynamic capturing of the golf swing16,17.
Data capture
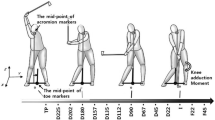
A 10-camera VICON motion capture system with a sampling frequency of 200 Hz (VICON, Oxford Metrics Group, UK) and two force plates with a sampling frequency of 1000 Hz (AMTI, Waterton, MA, USA) were used (Fig. 1). Each patient was provided with form-fitting shorts and a shirt during testing; patients were barefoot during testing to control for footwear-associated changes in the ground reaction forces (GRF)18. Reflective markers were placed on the full body in accordance with the Plug-in Gait configuration19, with additional markers on the lateral foot and anterior thigh and shank; in addition, a total of six markers were placed—three on the club head and three on the shaft of the driver club, respectively; the club head markers were used to identify the phases of the golf swing20. Each patient was asked to perform a drive swing without a ball using the 285 g driver club (Head, HONMA Twin Marks MG410; Shaft, HONMA ARMRQ 851). After a minimum of three practice trials, patients repeated the motions until three trials suitable for data analysis were obtained.

Patient's (recreational right-handed golfer) driver golf swing. (A) Actual driver swing scene, (B) Motion capture system (VICON), (C) Musculoskeletal modeling system (AnyBody).
Data processing
The golf swing is divided into four events (setup, top, impact, and finish; Fig. 1). Maximum club head speed was calculated from the club head markers around impact. The marker trajectories and the GRF data were low pass filtered using a Butterworth filter with a cutoff frequency of 20 Hz and 12 Hz, respectively. The hip joint angle was calculated using the Plug-in Gait model with Cardin rotational sequence of flexion–extension, adduction-abduction, and internal–external rotation (Fig. 1).
The musculoskeletal model used in this study is a standard model (v.2.3.4, AMMR, MoCapModel) available in the AnyBody Modeling System (v.7.3.4, AnyBody Technology, Denmark). The hip joint was modeled as a spherical joint with three rotational degrees of freedom. The knee, ankle, and subtalar joints were simulated as hinge joints. A detailed musculoskeletal model based on the cadaveric data set by Carbone et al21. was scaled to each patient's body size, based on marker data collected in the setup position. For fat scaling, the body mass index (BMI) was taken into account according to the equation proposed by Frankenfield et al22.
Marker trajectories and the GRF data for each trial were used as inputs for inverse kinematic analysis based on third-order polynomial muscle mobilization calculate HCF and muscle force23,24,25,26 (Fig. 1). HCF was evaluated using a value criteria to normalized by BW ratio. Percent maximum voluntary isometric contraction (%MVIC) is defined as muscle force divided by maximal muscle strength for a particular muscle at a particular instant in time27. The muscles around the hip joint [iliopsoas, gluteus maximus, gluteus medius, gluteus minimus, rectus femoris, biceps femoris long head, medial hamstring (semimembranosus and semitendinosus), adductor magnus, and adductor longus] with greater than 40% of %MVIC during the golf swing were extracted28,29.
Statistical analysis
Continuous variables were expressed as mean ± standard deviation (range or 95%CI). Statistical analysis was performed using JMP software v.14.0 (SAS Institute, Cary, NC). The Wilcoxon rank-sum test was used to compare demographic data [age, height (Ht), BW, BMI, follow-up duration, LLD, GFO, mHHS, average score, handicap, and VAS pain score] and kinematics and kinetics data [maximum club head speed, hip range of motion (RoM), and HCFs and %MVIC of muscles around hip joint] between left THA and right THA patients, along with the same factors between painful and painless patients during and after playing golf. The chi-square test was used to compare sex and diagnosis. Statistical significance was set as P < 0.05. Power analyses in the HCF difference between left THA and right THA and between with and without hip pain showed that the combined sample size of the two groups were 8 (4 and 4 patients) and 10 (2 and 8 patients) which provided 80% statistical power to detect the 1.6 difference in HCF between the two groups for a ratio one-to-one and one-to-four, respectively. This assumes that the probability value is < 0.05 and the standard deviation is 0.730.
Ethics approval and consent to participate
This study was approved by the Clinical Research Ethics Review Committee, Department of Medical Sciences, Kyushu University (IRB Number: 2019-323). All patients gave informed consent for the use of their demographic data, clinical score data, dynamic data, and images in motion in the study. The study was carried out in accordance with the principles of the Helsinki declaration. All authors agree to participate and consent to the manuscript.
Informed consent
Informed consent obtained from all study participants for publishing identifying information/image for this study.
Results
Patient demographics
Demographic characteristics (sex, preoperative diagnosis, age, height, weight, postoperative follow-up duration, GFO, LLD, mHHS, average score, and handicap) were similar between L-THA and R-THA patients (P > 0.05; Table 1). There were two patients (1 left THA and 1 right THA) with mild pain in the surgical hip during and after playing golf; VAS pain score in and after golf were also similar between L-THA and R-THA patients (P > 0.05; Table 1).
Kinematics and kinetics data
The mean maximum club head speed and the mean left and right hip RoMs of 3D were no significant difference between left THA and right THA (Table 2 and Fig. 2).

Hip range of motion. Blue solid line, Left THA; Orange solid line, Right THA; First black dotted line, Top; Second black dotted line, Impact.
There was no significant difference in HCF of lead and trail hips between left THA and right THA, with a tendency for a larger HCF of trail hips in unilateral THA (6.6 N/BW vs 5.1 N/BW, P = 0.06; Table 2 and Fig. 3). The %MVIC of the iliopsoas muscles in the left THA and right THA patients were more than 80% both on the surgical and contralateral sides (Table 2 and Fig. 4). The biceps femoris long head and medial hamstring of the surgical side in left and right THA patients were less and more than 40%, respectively (Table 2 and Fig. 4). The %MVIC of these hip muscles showed no significant difference between left THA and right THA (Table 2).

Hip contact force (HCF). Blue solid line, Left THA; Orange solid line, Right THA; First black dotted line, Top; Second black dotted line, Impact.

Percentage maximum voluntary isometric contraction (%MVIC). Blue line, Left THA; Orange line, Right THA; First black dotted line, Top; Second black dotted line, Impact.
Difference of demographics, kinetics, and kinetics data between patients with and without golf-related replaced hip pain
Patients without replaced hip pain had a significantly higher proportion of males, higher mHHS, and lower HCF of the surgical side compared to patients with pain [seven male and one female vs. zero male and two female, 97.0 ± 1.6 vs. 92.3 ± 1.6 and 5.6 ± 1.8 × BW vs. 8.1 ± 0.1 × BW; P = 0.02, 0.03, and 0.04, respectively]. The other demographics, kinetics, and kinetics data showed no significant difference (P > 0.05; Table 3).
Discussion
This in vivo study for the first time examined kinematics and kinetics of the hip joint during driver golf swings of patients who had undergone unilateral THA. This study evaluated different parameters including HCF and muscle activation of muscles that exhibited more than 40% of the %MVIC in recreational golfers after unilateral THA, in order to examine the differences in hip loading and muscle activation between left and right THA and between with and without golf-related pain. During the driver swing at a mean maximum head speed of 31 m/s, the mean replaced hip rotations were approximately 20–30° and mean HCFs were 5 and 6.6 × BW at the lead and trail replaced hips, respectively. More than 60% of the %MVIC was found in both iliopsoas muscles, regardless of the surgical side. Being female, lower mHHS, and higher HCF of surgical side were associated with golf-induced pain of the replaced hip.
The 31 m/s of mean maximum head speed in unilateral THA patients was equivalent to that of a similar aged healthy cohort: mean 28.3–38.9 m/s31,32,33. An approximate mean of 20–30° of hip rotation during the driver swing in patients who underwent THA is also equivalent to that of the golf swing analyzed by the motion capture methods in normal hips: mean 20–60°34,35. As in a previous study12, the driver swing had comparable lead and trail hip rotations regardless of the surgical side, and no excessive deviation of rotational balance. Hip rotation during the golf swing of similar aged THA patients analyzed by the image-matching method was approximately 50°12, which is greater than the 20–30° in the present study. The results may have been influenced by differences in the club used (grip only vs. driver club) and analysis method (image matching vs. motion capture)36,37. The motion capture system was reported to underestimate hip rotation by approximately 20° in motion involving large hip rotation compared to shape matching technique37. However, hip rotation during the golf swing was not an excessive RoM of the Int-Ext rotation, after accounting for this underestimation. RoMs of the Flex-Ext and Add-Abd during the driver swing in this study were similar to those of the golf swing in healthy participants34,35. In other words, club head speed and 3D hip RoMs were comparable to those of healthy participants, suggesting that THA had a positive effect on golf performance, including distance and handicap; this is supported by previous reports that most patients are able to play golf after THA, and mostly with an improvement in performance1,10,11,38.
Advances in computational techniques using musculoskeletal modeling systems have shown the comparability of estimating hip contact force (HCF) data to in vivo HCF23,24. The use of a musculoskeletal modeling system has the advantage that data can be safely collected from a larger number of cases rather than using implants with built-in devices to measure loading data in THA. The mean HCFs of the lead and trail replaced hips during the golf swing (5.5 and 6.7 × BW, respectively) were comparable, with a tendency of larger HCF of trail hips in both left THA and right THA, which was somewhat lower than the HCF while jogging at 6–8 km/h: 5.4–8.5 × BW30,39. Although jogging has been classified as a high-impact sport, it has been reported to have no adverse effect on mid-term survival outcome in THA5,40. The number of golf swing motions is much less than the number of steps taken while jogging and the repetition of loading cycles is significantly smaller. In addition, no negative effects on mid-term survival rate of implants have been previously observed in golfers11,41. Thus, it is suggested that the golf swing is an acceptable motion in patients with unilateral THA, although it produces a high HCF for both lead and trail replaced hips, comparable to that of jogging. There have been no previous reports of HCF in normal participants and THA patients during a golf swing, the proximo-distal component of HCF showed a similar pattern and magnitude as the resultant HCF, consistent with the reported HCF of daily activities in THA patients23,24.
The musculoskeletal modeling system can estimate the activation of each muscle around the hip joint which is in agreement with the measured activation25,26. It has been reported that more than 60% of MVIC intensity should be used for effective muscle strengthening and that the range should be at least 40–60% to stimulate muscle strength adaptation28,29. The driver swing may be useful as an iliopsoas strengthening exercise, because the %MVIC of the bilateral iliopsoas muscles is greater than 60%. Marta et al. demonstrated that the driver swing activated hip extensors in the order of strength of the biceps femoris long head, gluteus maximus, and semimembranosus in the lead leg (51–83%) and gluteus maximus, biceps femoris long head, and semimembranosus in the trail leg (67–100%), indicating a higher muscle activity of the trail leg42, which was consistent with the present study, where more than 40% of %MVIC was found in the hip extensors (the biceps femoris long head and medial hamstring) of the trail leg, except in the bilateral iliopsoas muscles. However, overall, %MVIC values were higher in the Marta et al. report5 than in the present study, which may have been influenced by differences in the participants (mean 36-year-old healthy volunteers vs. mean 68-year-old THA patients), handicap (< 5 vs. 8–45), and analysis methods (electromyogram vs. musculoskeletal modeling method). The biceps femoris long head and medial hamstring on the right side had approximately 40% of MVIC. Therefore, opposite-direction driver swings may be required to provide a level of muscle activation that balances the bilateral biceps femoris long head and medial hamstring muscular adaptations.
A significantly higher proportion of males were found in the patients without golf-related replaced hip pain compared to patients with pain, consistent with previous reports on the association between sex and persistent pain after THA43,44. A significantly higher proportion of males were found in the patients without golf-related replaced hip pain compared to patients with pain, consistent with previous reports on the association between sex and persistent pain after THA9. Of golf swings, the minimalist golf swing and partial golf swing are designed to reduce the loading that hips experience throughout the swing43,45,46. The minimalist golf swing, which requires torso rotation to be completed in a more upright position during the set-up, results in less hip extension and abduction moments while maintaining golf performance47. The partial golf swing, which is adjusted to approximately 80% of full swing distance, requires limiting the natural weight shift of the swing to reduce lateral motion, resulting in a significant reduction in the peak horizontal ground reaction force of both legs46,47. This reduction in joint loading resulting from swing adjustments may provide relief from hip pain during and after playing golf.
There are several limitations to the present study. First was the limitation of the small number of study patients. Although power analysis is done, number could be insufficient for groups with and without hip pain. A larger number of patients might have revealed further kinematic and kinetic differences. In addition, we recruited recreational golfers from unilateral primary THA patients; therefore, findings in this study cannot be generalized to amateur or professional golfers. Furthermore, we only analyzed swings using a driver for our data collection. Therefore, we cannot make inferences as to kinematics and kinetics produced using other clubs. Finally, the patients performed their golf swing while barefoot and without a golf ball, which could have altered swing mechanics.
Conclusion
The driver swing of unilateral THA patients did not contribute excessive hip contact forces to the right and left hip prosthesis, with a maximum club head speed and hip RoMs comparable to those of healthy participants. The driver swing activated more than 60% of %MVIC at bilateral iliopsoas muscles and could be useful as a strength exercise for those muscles. The replaced hip pain related to golf activity was associated with male female, a lower mHHS, and higher HCF of the surgical side; in particular HCF could be reduced through swing adjustments, which may allow for the development of a comfortable golf game free from pain.
Data availability
The datasets used and/or analyzed during the current study available from the corresponding author on reasonable request.
References
Arbuthnot, J. E., McNicholas, M. J., Dashti, H. & Hadden, W. A. Total Hip Arthroplasty and the Golfer. A study of participation and performance before and after surgery for osteoarthritis. J. Arthroplast. 22, 549–552 (2007).
Learmonth, I. D., Young, C. & Rorabeck, C. The operation of the century: Total hip replacement. Lancet 370, 1508–1519 (2007).
Ollivier, M., Frey, S., Parratte, S., Flecher, X. & Argenson, J. N. Pre-operative function, motivation and duration of symptoms predict sporting participation after total hip replacement. Bone Joint J. 96B, 1041–1046 (2014).
Schmidutz, F. et al. Sports activity after short-stem hip arthroplasty. Am. J. Sports Med. 40, 425–432 (2012).
Harada, S. et al. Wear analysis of the first-generation cross-linked polyethylene at minimum 10 years follow-up after THA: No significant effect of sports participation. J. Artif. Organs 25, 140–147 (2022).
Komiyama, K. et al. In vivo kinematic analysis of replaced hip during stationary cycling and computer simulation of optimal cup positioning against prosthetic impingement. Clin. Biomech. 68, 175–181 (2019).
Papaliodis, D. N., Photopoulos, C. D., Mehran, N., Banffy, M. B. & Tibone, J. E. Return to golfing activity after joint arthroplasty. Am. J. Sports Med. 45, 243–249 (2017).
D’Lima, D. D., Patil, S., Steklov, N. & Colwell, C. W. ’Lab’-in-a-Knee: In vivo knee forces, kinematics, and contact analysis. Clin. Orthop. Relat. Res. 469, 2953–2970 (2011).
Mallon, W. J. & Callaghan, J. J. Total knee arthroplasty in active golfers. J. Arthroplast. 8, 299–305 (1993).
Mallon, W. J. & Callaghan, J. J. Total hip arthroplasty in active golfers. J. Arthroplast. 7, 339–346 (1992).
Pioger, C. et al. Return to competitive level of play and performance in regular golfers after total hip arthroplasty: Analysis of 599 patients at minimum 2-year follow-up. J. Arthroplast. 36, 2858-2863.e2 (2021).
Hara, D. et al. Dynamic hip kinematics during the golf swing after total hip arthroplasty. Am. J. Sports Med. 44, 1801–1809 (2016).
Nakashima, Y. et al. Combined anteversion technique reduced the dislocation in cementless total hip arthroplasty. Int. Orthop. 38, 27–32 (2014).
Keršič, M., Dolinar, D., Antolič, V. & Mavčič, B. The impact of leg length discrepancy on clinical outcome of total hip arthroplasty: Comparison of four measurement methods. J. Arthroplast. 29, 137–141 (2014).
Kabata, T. et al. Safety range for acute limb lengthening in primary total hip arthroplasty. Int. Orthop. 43, 2047–2056 (2019).
Byrd, J. W. T. & Jones, K. S. Hip arthroscopy in the presence of dysplasia. Arthrosc. J. Arthrosc. Relat. Surg. 19, 1055–1060 (2003).
Rodriguez, C. S. Pain measurement in the elderly: A review. Pain Manag. Nurs. 2, 38–46 (2001).
Mcnair, P. J. & Marshall, R. N. Kinematic and kinetic parameters associated with running in different shoes. Br. J. Sports Med. 28, 256–261 (1994).
Vicon Documentation. Available online: https://docs.vicon.com/display/Nexus212/Full+body+modeling+with+Plug-in+Gait (accessed on 12 April 2023)
Coleman, S. & Anderson, D. An examination of the planar nature of golf club motion in the swings of experienced players. J. Sports Sci. 25, 739–748 (2007).
Carbone, V. et al. TLEM 2.0—a comprehensive musculoskeletal geometry dataset for subject-specific modeling of lower extremity. J. Biomech. 48, 734–741 (2015).
Frankenfield, D. C., Rowe, W. A., Cooney, R. N., Smith, J. S. & Becker, D. Limits of body mass index to detect obesity and predict body composition. Nutrition 17, 26–30 (2001).
Lunn, D. E. et al. Current preclinical testing of new hip arthroplasty technologies does not reflect real-world loadings: Capturing patient-specific and activity-related variation in hip contact forces. J. Arthroplast. 35, 877–885 (2020).
De Pieri, E. et al. Refining muscle geometry and wrapping in the TLEM 2 model for improved hip contact force prediction. PLoS ONE 13, e0204109 (2018).
Alexander, N. & Schwameder, H. Comparison of estimated and measured muscle activity during inclined walking. J. Appl. Biomech. 32, 150–159 (2016).
Wibawa, A. D. et al. Musculoskeletal modeling of human lower limb during normal walking, one-legged forward hopping and side jumping: Comparison of measured EMG and predicted muscle activity patterns. J. Biomech. 49, 3660–3666 (2016).
de Zee, M. et al. Validation of a musculo-skeletal model of the mandible and its application to mandibular distraction osteogenesis. J. Biomech. 40, 1192–1201 (2007).
Andersen, L. L. et al. Neuromuscular activation in conventional therapeutic exercises and heavy resistance exercises: Implications for rehabilitation. Phys. Ther. 86, 683–697 (2006).
Kraemer, W. J. et al. Progression models in resistance training for healthy adults. Med. Sci. Sports Exerc. 34, 364–380 (2002).
Giarmatzis, G., Jonkers, I., Wesseling, M., van Rossom, S. & Verschueren, S. Loading of hip measured by hip contact forces at different speeds of walking and running. J. Bone Miner. Res. 30, 1431–1440 (2015).
Hegedus, E. J., Hardesty, K. W., Sunderland, K. L., Hegedus, R. J. & Smoliga, J. M. A randomized trial of traditional and golf-specific resistance training in amateur female golfers: Benefits beyond golf performance. Phys. Ther. Sport 22, 41–53 (2016).
Thompson, C. J., Cobb, K. M. & Blackwell, J. Functional training improves club head speed and functional fitness in older golfers. J. Strength Cond. Res. 21, 131–137 (2007).
Thompson, C. J. & Osness, W. H. Effects of an 8-week multimodal exercise program on strength, flexibility, and golf performance in 55- to 79-year-old men. J. Aging Phys. Act. 12, 144–156 (2004).
Gulgin, H., Armstrong, C. & Gribble, P. Weight-bearing hip rotation range of motion in female golfers. N. Am. J. Sports Phys. Ther. 5, 55–62 (2010).
Kim, S. B., You, J. H., Kwon, O. Y. & Yi, C. H. Lumbopelvic kinematic characteristics of golfers with limited hip rotation. Am. J. Sports Med. 43, 113–120 (2015).
Egret, C. I., Vincent, O., Weber, J. & Dujardin, F. H. Analysis of 3D kinematics concerning three different clubs in golf swing. Int. J. Sports Med. 24, 465–470 (2003).
Fiorentino, N. M. et al. Soft tissue artifact causes significant errors in the calculation of joint angles and range of motion at the hip. Gait Posture 55, 184–190 (2017).
Ollivier, M., Frey, S., Parratte, S., Flecher, X. & Argenson, J. N. Does impact sport activity influence total hip arthroplasty durability?. Clin. Orthop. Relat. Res. 470, 3060–3066 (2012).
Bergmann, G., Graichen, F. & Rohlmann, A. Hip joint loading during walking and running, measured in two patients. J. Biomech. 26, 969–990 (1993).
Abe, H. et al. Jogging after total hip arthroplasty. Am. J. Sports Med. 42, 131–137 (2014).
Oljaca, A., Vidakovic, I., Leithner, A. & Bergovec, M. Current knowledge in orthopaedic surgery on recommending sport activities after total hip and knee replacement. Acta Orthop. Belg 84, 415–422 (2018).
Bechler, J. R., Jobe, F. W., Pink, M., Perry, J. & Ruwe, P. A. Electromyographic analysis of the hip and knee during the golf swing. Clin. J. Sport Med. 5, 162–166 (1995).
Hofstede, S. N., Gademan, M. G. J., Vliet Vlieland, T. P. M., Nelissen, R. G. H. H. & Marang-Van De Mheen, P. J. Preoperative predictors for outcomes after total hip replacement in patients with osteoarthritis: A systematic review. BMC Musculoskelet Disord. 17, 1–11 (2016).
Rojanasopondist, P. et al. What preoperative factors are associated with not achieving a minimum clinically important difference after tha? Findings from an international multicenter study. Clin. Orthop. Relat. Res. 477, 1301–1312 (2019).
McNitt-Gray, J. L., Munaretto, J., Zaferiou, A., Requejo, P. S. & Flashner, H. Regulation of reaction forces during the golf swing. Sports Biomech. 12, 121–131 (2013).
Todd, S. D., Wiles, J. D., Coleman, D. A. & Brown, M. B. Partial swing golf shots: Scaled from full swing or independent technique?. Sports Biomech. 19, 353–365 (2020).
Kanwar, K. D., Cannon, J., Nichols, D. L., Salem, G. J. & Mann, M. D. Injury risk-factor differences between two golf swing styles: A biomechanical analysis of the lumbar spine, hip and knee. Sports Biomech. 00, 1–22 (2021).
Acknowledgements
This work was performed at the Department of Orthopaedic Surgery, Graduate School of Medical Sciences, Kyushu University. The authors would like to express their heartfelt thanks Yuki Nasu (Physical Therapist Staff of Department of Rehabilitation, Kyushu University) for their assistance and contribution to the development and achievement of this research.
Funding
This work was supported by a Grant-in-Aid for Scientific Research awarded by the Japan Society for the Promotion of Science [Grant Number JP19K09652 and JP21K21256], the Ogata Memorial Foundation, Inc. (No. 135), Shimadzu Science Foundation, Grant of The Clinical Research Promotion Foundation 2021 and Foundation for the Promotion of Clinical Medicine.
Author information
Authors and Affiliations
Contributions
Conception and design of study: T.H., S.H.; acquisition of data: T.H., S.H., D.H., K.O., T.F., N.K., S.K., R.Y., M.F., S.I., G.M., Y.N.; analysis and/or interpretation of data: T.H., S.H.; Drafting the manuscript: T.H.; revising the manuscript critically for important intellectual content: S.H., Y.N.; Approval of the version of the manuscript to be published: T.H., S.H., D.H., K.O., T.F., N.K., S.K., R.Y., M.F., S.I., G.M., Y.N.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Harada, T., Hamai, S., Hara, D. et al. Reverse dynamics analysis of contact force and muscle activities during the golf swing after total hip arthroplasty. Sci Rep 13, 8688 (2023). https://doi.org/10.1038/s41598-023-35484-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-023-35484-y
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
