
Abstract
Vitiligo is clinically characterized by the appearance of non-symptomatic depigmented macules, but the disorder is highly correlated with a wide range of psychiatric disorders and psychological problems. The aim of our study was to investigate serum brain-derived neurotrophic factor (BDNF) and corticotropin releasing hormone (CRH) levels in vitiligo patients and healthy controls in relation to the observed symptoms of depression and anxiety disorders. This study comprised 96 vitiligo patients and 96 healthy controls who filled out the Patient Health Questionnaire-9 (PHQ-9) and Generalized Anxiety Disorder-7 (GAD-7) scales. Serum levels of BDNF and CRH were measured using enzyme-linked immunosorbent assay (ELISA) technique. There was a significant increase of depression and anxiety scores in vitiligo patients as compared with healthy controls (P < 0.05). The serum levels of BDNF were significantly lower in vitiligo patients than in healthy individuals (Z = 4.002; P < 0.001), while the serum levels of CRH were markedly higher in cases than those in controls (Z = 3.764; P < 0.001). The significant positive correlations between serum CRH levels and GAD-7, PHQ-9 scores were observed. However, the aforementioned psychometric scales did not correlate significantly with serum BDNF level. Vitiligo is associated with the depression and is closely linked with lower BDNF levels.
Similar content being viewed by others


Vitiligo is a common autoimmune disease which affects pigment producing melanocytes, resulting in the appearance of visible whitish patches on skin and mucosal membranes1. The prevalence of vitiligo varies from 0.5% to 2% worldwide2. The origin of vitiligo is unknown though the pathogenesis is associated with the intrinsic abnormalities of melanocytes, oxidative stress, and sympathetic neurogenic imbalances3. Vitiligo is clinically characterized by the appearance of non-symptomatic depigmented macules, but the disorder is highly correlated with a wide range of psychiatric disorders and psychological problems4. Because of emotional and social burden associated with vitiligo, numerous studies investigating relationship between psychiatric disturbances and manifestation, course, and severity of the disease have been conducted. Individuals with vitiligo suffer from depressive disorders, stigmatization, emotional and behavioral impairment, sleep disturbance, and decreased quality of life5,6,7,8. In addition, a meta-analysis reported that patients with vitiligo have the same risk of anxiety as compared to subjects suffering from eczema, psoriasis, and acne9. Certainly, the pathogenetic relationship between vitiligo and mental impairments needs to be considered in detail. A better understanding of mechanisms of neuroendocrine and inflammatory disturbances in vitiligo might be achieved by investigation of some crucial signaling substances.
Corticotropin releasing hormone (CRH) is the important hypothalamic factor which regulates the pituitary secretion of adrenocorticotropic hormone (ACTH). As the crucial part of the hypothalamo-pituitary-adrenal (HPA) axis, CRH is the driver of the stress response. The role of CRH is well described in pathogenesis of some autoimmune diseases, neurological and mental abnormalities10. Some studies suggest that CRH is increased in depression and anxiety disorders. For example, Cao S et al. (2020) found that the serum levels of CRH was significantly higher in women with postpartum depression (PPD) than in the non-PPD group. The authors offered that the serum levels of CRH and serotonin may serve as a potential early marker for identifying women at high risk for PPD11. To date, there are practically no studies devoted to determine the serum levels of CRH in vitiligo patients. Some authors described the cutaneous expression of CRH and its’ receptor, which is detected by performing a skin biopsy. The authors found a significant increase in the expression of CRH and corticotropin releasing hormone receptor 1 (CRH-R1) in both damaged and intact skin of vitiligo patients that were exposed to stress12. Besides, the in vitro studies and clinical evidence of direct and indirect pro-inflammatory action of CRH were reported for vitiligo. A recent research found that CRH may also contribute greatly to skin homeostasis. The CRH activates regional mast cells and its receptor (CRH-R1) is expressed on melanocytes. In its turn, the damage of melanocytes causes the hypopigmentation process13. In addition, the cutaneous CRH increases the production and extrication of pro-opiomelanocortin (POMC), which is involved in melanogenesis14.
Brain-derived neurotrophic factor (BDNF) is another important agent which may act as potential regulator of neuropsychiatric processes. It plays vital role in different stages of neurons’ life cycle, such as growth, survival, differentiation, and repair15. BDNF has been established already as the possible biomarker for the onset and progression of major depressive disorder (MDD), bipolar disorder, schizophrenia, Alzheimer disease, Parkinson’s disease, and epilepsy16. The above-mentioned spectrum of neuropsychiatric abnormalities was conceivably associated with the decreased BDNF levels. In addition to that, some chronic somatic conditions are also linked with the reduced level of BDNF. For instance, Tschorn et al. (2020) reported the lower BDNF levels in patients with chronic heart failure17. Similarly, the serum levels of BDNF were investigated in chronic skin disorders. Such, Sjahrir et al. (2019) showed that a low level of serum BDNF may increase severity of both depression and psoriasis vulgaris18. Besides, recent research reported the decreased level of BDNF in patients with vitiligo19. Thus, the aim of our study was to investigate serum BDNF and CRH levels in vitiligo patients and healthy controls in relation to the observed symptoms of depression and anxiety disorders.
Methods
Subjects and study proceedings
This study was carried out during a 6-month period from October 2020 to March 2021. The participants were adult patients who were referred to Dermatology department of General Hospital #2 of Semey City, Kazakhstan. The study was approved by the local Ethics Committee of Semey Medical University (Protocol #2, from 18 October 2019), and the research was conducted in compliance with principles of the Declaration of Helsinki and the Guideline for Good Clinical Practice. All participants provided written informed consent. Totally, 192 individuals aged 16–79 years were selected for the study based on inclusion/exclusion criteria. The participants were divided into two groups: 96 patients with a confirmed diagnosis of vitiligo and 96 healthy controls. Exclusion criteria for patients or healthy individuals included: subjects who were younger than 16 years of age, who were currently treated for a psychiatric disorder, who had another dermatologic disease or severe concomitant pathology (liver dysfunction, alcoholism, drug addiction, cancer), and who did not want to participate in the study.
Enrollment and assessment criteria
All patients were subjected to complete history taking regarding their age, sex, ethnicity, educational level, duration and activity of the disease, history of vitiligo in parents or grandparents, previous treatment, general and dermatological examination in daylight and using a Wood lamp to determine Fitzpatrick's skin photo type. The type of vitiligo and the percentage of affected body area were determined by the Vitiligo Extent Score (VES) associated with mucosal lesions, leukotrichia, Koebner's phenomenon and halo-nevi20.
Laboratory tests
Five milliliters of venous blood samples were withdrawn from each participant on an empty stomach in the morning (before 10.00 AM) using serum separator tubes and left for 30 min at room temperature to allow clotting and then centrifuged for 15 min at 3000 rpm. All serum samples were collected and then stored for less than 6 months at −20 °C. A double-antibody sandwich enzyme-linked immunosorbent assay (ELISA) technique was used to determine BDNF serum levels with the help of a commercial kit (Serial #: 9F1F9F01E4, Cloud-Clone Corp., USA). Measurement of CRH was also performed by ELISA kit (Serial #: 09A102086A, Cloud-Clone Corp., USA) according to the same technique. All manufacturer instructions were strictly followed.
Evaluation of depression and anxiety
Depression was evaluated on the basis of the Patient Health Questionnaire-9 (PHQ-9), which is an internationally recognized screening tool. The PHQ-9 consists of nine questions that are based on the DSM-IV criteria for a MDD. The questionnaire explores the symptoms experienced by patients during the two immediately preceding weeks. The scores for each PHQ-9 item range from 0 (not at all), to 3 (nearly every day). Total scores of 5, 10, 15, and 20 indicate the presence of mild, moderate, moderately severe and severe disorder, respectively. MDD should be considered in patients who endorse ≥ 5 of the 9 symptoms as present “more than half the days” (the 9th item counts if endorsed “several days”) and one of the first two symptoms (depressed mood or loss of interest) is endorsed21. Likewise, the anxiety was evaluated with the help of the Generalized Anxiety Disorder-7 (GAD-7) scale, which is also a well-recognized international screening tool. The GAD-7 scores range from 0 to 27, with 5, 10 and 15 representing mild, moderate and severe levels of anxiety symptoms22. Previously, both tools were successfully utilized in the Kazakhstani population23.
Statistical analysis
Qualitative data presented as absolute numbers and their percentages. The test of difference in groups of nominal data was Chi square test. All numerical variables were tested by the Kolmogorov–Smirnov test for normality of distribution. Since the observed data did not follow the normal distribution, the quantitative data were expressed as median and 25th-75th percentiles. For difference testing in groups of quantitative variables, we used a Mann Whitney U-test. To find any possible correlation between the variables, we used the Spearmen's correlation test. Receiver operating curve and logistic regression procedure were used to analyze a predictive significance of laboratory markers (BDNF and CRH). The associations between vitiligo and BDNF/CRH levels were assessed in relation to a patient gender and anxiety/depression scores. The critical value of statistical significance was at a probability of α less than 5%. All statistical procedures were performed in SPSS 20.
Results
Table 1 contains the data related to the demographic and clinical characteristics of the vitiligo patients and healthy controls. In this study, 96 patients with vitiligo (59.4% females, 97.9% Kazakhs) and 96 healthy participants (55.2% females, 89.6% Kazakhs) were compared. There was no difference between the groups in terms of age, gender, ethnicity, and education level (all P > 0.05). Nearly half of the participants were married, and more than the half of them had both parents. The study cohort was mostly represented by the second and the third Fitzpatrick skin types (48.4% and 31.8%, respectively).
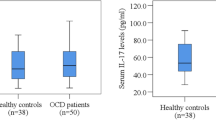
The patients with vitiligo demonstrated significantly higher anxiety and depression scores (all P < 0.05). The serum level of BDNF was significantly lower in vitiligo patients as compared with the healthy controls (2.60 (1.88–3.01) vs. 3.23 (2.52–4.33); P < 0.001). Median serum CRH level was 6.39 (2.46–8.31) in vitiligo patients and 3.24 (2.18–3.85) in healthy subjects (P < 0.001) (Table 2).
Female vitiligo patients had significant higher GAD-7 scores as compared with male patients: 3.0 (2.0–6.0) vs.5.0 (3.0–7.0) (P = 0.032) (Table 3).
Anxiety level correlated positively with PHQ-9 score (r = 0.296; P = 0.003). We detected statistically significant positive weak correlations between serum CRH level and GAD-7 scores (r = 0.214; P = 0.036) (Table 4).
The area under curve (AUC) for serum BDNF showed no prognostic value of vitiligo (AUC = 0.333) (Fig. 1). Only serum CRH level had poor prognostic value for forecasting of vitiligo event, which was statistically significant (AUC = 0.657) with cut-off point 0.222 at sensitivity equal to 0.938 and specificity equal to 0.990 (Fig. 2).

Receiver operating curve graph to evaluate the diagnostic performance of serum BDNF for forecasting of vitiligo event.

Receiver operating curve graph to evaluate the diagnostic performance of serum CRH for forecasting of vitiligo event.
Discussion
In the current study, the serum levels of BDNF and CRH with respect to depression and anxiety scores in vitiligo patients and control subjects were compared. The present data demonstrate the significant increase of depression and anxiety in vitiligo patients as compared with healthy controls. The serum levels of BDNF were significantly lower in vitiligo patients than in healthy individuals, while the serum levels of CRH were markedly higher in cases than those in controls. Moreover, we detected significant positive correlations between serum CRH level and GAD-7 score. However, the aforementioned psychometric scales did not correlate significantly with serum BDNF level.
Previous studies revealed the relationship between vitiligo and psychiatric morbidities. Recent meta-analyses reported that vitiligo patients were averagely 5 times more prone to depression as compared with controls5,6. Our results agree with these data displaying the higher scores of PHQ-9 scale in patients with vitiligo than in healthy participants. Numerous studies have detected a significant increase of anxiety symptoms among vitiligo patients9. In this study, there were significantly lower BDNF levels in vitiligo patients than in controls. In line with these findings, several studies reported the decreased levels of serum BDNF in patients with acne vulgaris and psoriasis in comparison with healthy individuals24,25,26. These results agree with Yanik et al. (2014) who found significant differences in serum BDNF levels between vitiligo and healthy control groups. The authors also attempted to find any correlations between mean serum BDNF level and Beck Depression Inventory and Beck Anxiety Inventory self-reported scales19. Our results were consistent with these findings since we also failed to detect associations between serum BDNF levels and PHQ-9 and GAD-7 scores.
However, in our study serum CRH level was significantly higher in vitiligo patients as compared with controls. In addition, serum CRH levels positively correlated with depression and anxiety. Shaker et al. demonstrated significantly higher mean expressions of CRH, and corticotropin releasing hormone receptor 1 (CRHR-1) detected by real-time polymerase chain reaction (PCR) in the depigmented lesions than in control skin. Moreover, significantly higher expressions of CRH and CRH-R1 were correlated with a stress scale12. In the current study, there was a positive correlation between serum CRH level and GAD-7. In line with our findings, Tagen et al. reported higher serum levels of CRH in psoriasis patients in contrast with controls. Still, the authors did not find significant correlation between CRH-R1 expression or serum CRH levels, psoriasis area and severity index (PASI) score27.
The etiopathogenesis of vitiligo is complex. There are numerous presumed theories of the disease development including oxidative stress hypothesis, genetic predisposition, autoimmune abnormalities, CD8 + T-cells toxicity, biochemical theory, decreased melanocytes regeneration, and neural hypothesis28,29,30. The last theory might play a significant role in interpretation of our main findings. Such, according to neurohumoral theory, the increased levels of certain neuromediators and neuropeptides that are released by neural endings, may launch inflammatory and destructive processes in the skin. This assumption might explain the mechanisms of pathogenesis of segmental vitiligo and its distribution patterns31. Numerous studies examined the potential role of BDNF in the development of neuropsychiatric disorders.
Molecular mechanisms of neuronal adaptive plasticity in the brain include interactions between BDNF and tropomysin-related kinase B (TrkB) that, in turn, involves downstream signaling through phosphatidyl inositol-3 kinase (PI3K)-Akt (serine threonine kinase or protein kinase B), Ras/microtubule-associated protein kinase (MAPK), and the phospholipase Cg (PLCg)-Ca2+ pathways. According to both in-vitro and clinical studies, the aforementioned pathways, for their part, display the decreased levels of BDNF in situations of stress and depression32. Thus, neurotrophins act as inflammatory cytokines, giving signals of activation and survival to effector cells in allergic reactions, and chronic inflammatory skin disorders. Numerous studies reported the crucial role of BDNF in some specific neurobiological processes which may lead to depressive disorders, anxiety-like behavior, and other stress-related mental disorders33,34,35.
Being the part of the proopiomelanocortin system, CRH coordinates pigmentation and immune response in the skin. Stress triggers the release of hormones, especially CRH, from the paraventricular nuclei of the hypothalamus. CRH stimulates the release of ACTH from the anterior pituitary gland. ACTH, in turn, regulates the secretion of glucocorticoids by the adrenal cortex. Cortisol has a suppressive effect on the hypothalamus and the anterior pituitary gland and stimulates the production of epinephrine and norepinephrine by the adrenal glands. In small concentrations, cortisol, adrenaline, and norepinephrine can enhance the immune response in the skin, while in large concentrations they are capable to suppress it14,36.
Our paper has some limitations and strengths. Firstly, a cross-sectional design was applied and thus, it was impossible to determine a cause-and-effect relationship between the study variables. Secondly, the self-report measurements for depression and anxiety were used, whereas the gold standard for a psychiatric diagnosis is a structured/semi-structured clinical interview. Thirdly, despite the fact that PHQ-9 and GAD-7 are often used in surveys studying the prevalence of mental disorders, the above-mentioned questionnaires are not intended for people with skin diseases. Thus, it would be desirable to develop and approve a more specific scale for assessing mental health in patients with vitiligo. And finally, we utilized the ELISA kit that detected serum BDNF levels without the identification of precursor and mature forms of this neuropeptide. Nevertheless, our study has several advantages. To the best of our knowledge, this is the first investigation of serum CRH levels in vitiligo patients since other authors performed the CRH measurements in skin only. Also, the current study makes a significant contribution to the limited evidence of relationship between BDNF, vitiligo, and mental comorbidities.
Data availability
The data and material are available from the corresponding author on request.
Abbreviations
- BDNF:
-
Brain-derived neurotrophic factor
- CRH:
-
Corticotropin releasing hormone
- PHQ-9:
-
Patient Health Questionnaire-9
- GAD-7:
-
Generalized Anxiety Disorder-7
- ELISA:
-
Enzyme-linked immunosorbent assay
- ACTH:
-
Adrenocorticotropic hormone
- HPA:
-
Hypothalamo-pituitary-adrenal
- PPD:
-
Postpartum depression
- VES:
-
Vitiligo Extent Score
- HRP:
-
Horseradish Peroxidase
- TMB:
-
3,3′,5,5′-Tetramethylbenzidine
- OD:
-
Optical density
- HS:
-
Higher School
- HE:
-
Higher Education
- AUR:
-
Area under curve
- CRHR-1:
-
Corticotropin releasing hormone receptor 1
- MDD:
-
Major depressive disorder
- PCR:
-
Polymerase chain reaction
- PASI:
-
Psoriasis area and severity index
- TrkB:
-
Tropomysin-related kinase B
- PI3K:
-
Phosphatidyl inositol-3 kinase
- MAPK:
-
Microtubule-associated protein kinase
- PLCg:
-
Phospholipase Cg
References
Ezzedine, K., Eleftheriadou, V., Whitton, M. & van Geel, N. Vitiligo. Lancet 386(9988), 74–84. https://doi.org/10.1016/S0140-6736(14)60763-7 (2015).
Bergqvist, C. & Ezzedine, K. Vitiligo: A review. Dermatology 236(6), 571–592. https://doi.org/10.1159/000506103 (2020).
Abdel-Malek, Z. A. et al. The enigma and challenges of vitiligo pathophysiology and treatment. Pigment Cell Melanoma Res. 33(6), 778–787. https://doi.org/10.1111/pcmr.12878 (2020).
Simons, R. E., Zevy, D. L. & Jafferany, M. Psychodermatology of vitiligo: Psychological impact and consequences. Dermatol. Ther. 33(3), e13418. https://doi.org/10.1111/dth.13418 (2020).
Lai, Y. C., Yew, Y. W., Kennedy, C. & Schwartz, R. A. Vitiligo and depression: A systematic review and meta-analysis of observational studies. Br. J. Dermatol. 177(3), 708–718. https://doi.org/10.1111/bjd.15199 (2017).
Wang, G., Qiu, D., Yang, H. & Liu, W. The prevalence and odds of depression in patients with vitiligo: A meta-analysis. J Eur Acad Dermatol Venereol. 32(8), 1343–1351. https://doi.org/10.1111/jdv.14739 (2018).
Ezzedine, K. et al. Psychosocial effects of Vitiligo: A systematic literature review. J Am Acad Dermatol. https://doi.org/10.1007/s40257-021-00631-6 (2021).
Morales-Sánchez, M. A., Vargas-Salinas, M., Peralta-Pedrero, M. L., Olguín-García, M. G. & Jurado-Santa Cruz, F. Impact of Vitiligo on quality of life. Actas Dermosifiliogr. 108(7), 637–642. https://doi.org/10.1016/j.ad.2017.03.007 (2017).
Kussainova, A. et al. Vitiligo and anxiety: A systematic review and meta-analysis. PLoS ONE 15(11), e0241445. https://doi.org/10.1371/journal.pone.0241445 (2020).
Nieman, L. K. & Loriaux, D. L. Corticotropin-releasing hormone: clinical applications. Annu Rev Med. 40, 331–339. https://doi.org/10.1146/annurev.me.40.020189.001555 (1989).
Cao, S. & Wei, L. Predictive value of serum CRH/5-HT ratio for postpartum depression. Int. J. Gynaecol. Obstet. 151(3), 438–442. https://doi.org/10.1002/ijgo.13351 (2020).
Shaker, O. G., Eltahlawi, S. M., Tawfic, S. O., Eltawdy, A. M. & Bedair, N. I. Corticotropin-releasing hormone (CRH) and CRH receptor 1 gene expression in vitiligo. Clin. Exp. Dermatol. 41(7), 734–740. https://doi.org/10.1111/ced.1290 (2016).
Lotti, T., Zanardelli, M. & D’Erme, A. M. Vitiligo: what’s new in the psycho-neuro-endocrine-immune connection and related treatments. Wien Med. Wochenschr. 164(13–14), 278–285. https://doi.org/10.1007/s10354-014-0288-7 (2014).
Slominski, A., Wortsman, J., Luger, T., Paus, R. & Solomon, S. Corticotropin releasing hormone and proopiomelanocortin involvement in the cutaneous response to stress. Physiol. Rev. 80(3), 979–1020. https://doi.org/10.1152/physrev.2000.80.3.979 (2000).
Lin, C. C. & Huang, T. L. Brain-derived neurotrophic factor and mental disorders. Biomed. J. 43(2), 134–142. https://doi.org/10.1016/j.bj.2020.01.001 (2020).
Lima Giacobbo, B. et al. Brain-derived neurotrophic factor in brain disorders: Focus on neuroinflammation. Mol. Neurobiol. 56(5), 3295–3312. https://doi.org/10.1007/s12035-018-1283-6 (2019).
Tschorn, M. et al. Brain-derived neurotrophic factor, depressive symptoms, and somatic comorbidity in patients with coronary heart disease. Acta Neuropsychiatrica https://doi.org/10.1017/neu.2020.31 (2020).
Sjahrir, M., Roesyanto-Mahadi, I. D. & Effendy, E. Correlation between serum brain-derived neurotrophic factor level and depression severity in psoriasis vulgaris patients. Open Access Maced. J. Med. Sci. 7(4), 583–586. https://doi.org/10.3889/oamjms.2019.142 (2019).
Yanik, M. E. et al. Reduced serum brain-derived neurotrophic factor in patients with first onset vitiligo. Neuropsychiatr. Dis. Treat. 12(10), 2361–2367. https://doi.org/10.2147/NDT.S74826 (2014).
van Geel, N. et al. Development and validation of the vitiligo extent score (VES): An international collaborative initiative. J. Invest. Dermatol. 136(5), 978–984. https://doi.org/10.1016/j.jid.2015.12.040 (2016).
Kroenke, K., Spitzer, R. L., Williams, J. B. & Löwe, B. The patient health questionnaire somatic, anxiety, and depressive symptom scales: A systematic review. Gen. Hosp. Psychiatry 32(4), 345–359. https://doi.org/10.1016/j.genhosppsych.2010.03.006 (2010).
Spitzer, R. L., Kroenke, K., Williams, J. B. & Löwe, B. A brief measure for assessing generalized anxiety disorder: The GAD-7. Arch Intern Med. 166(10), 1092–1097. https://doi.org/10.1001/archinte.166.10.1092 (2006).
Semenova, Y. et al. Mental distress in the rural Kazakhstani population exposed and non-exposed to radiation from the Semipalatinsk Nuclear Test Site. J. Environ. Radioact. 203, 39–47. https://doi.org/10.1016/j.jenvrad.2019.02.013 (2019).
He, H. Y. et al. Association of brain-derived neurotrophic factor levels and depressive symptoms in young adults with acne vulgaris. BMC Psychiatry 19(1), 193. https://doi.org/10.1186/s12888-019-2182-8 (2019).
Mikhael, N. W., Hamed, A. M., Mansour, A. I. & Abdelrahman, E. S. Serum levels of brain-derived neurotrophic factor in patients with acne vulgaris. J. Cosmet. Dermatol. 18(6), 1998–2003. https://doi.org/10.1111/jocd.12940 (2019).
Brunoni, A. R. et al. Decreased brain-derived neurotrophic factor plasma levels in psoriasis patients. Braz. J. Med. Biol. Res. 48(8), 711–714. https://doi.org/10.1590/1414-431X20154574 (2015).
Tagen, M. et al. Skin corticotropin-releasing hormone receptor expression in psoriasis. J. Invest. Dermatol. 127(7), 1789–1791. https://doi.org/10.1038/sj.jid.5700757 (2007).
Speeckaert, R. & van Geel, N. Vitiligo: An update on pathophysiology and treatment options. Am. J. Clin. Dermatol. 18(6), 733–744. https://doi.org/10.1007/s40257-017-0298-5 (2017).
Rodrigues, M., Ezzedine, K., Hamzavi, I., Pandya, A. G. & Harris, J. E. Vitiligo Working Group: New discoveries in the pathogenesis and classification of vitiligo. J. Am. Acad. Dermatol. 77(1), 1–13. https://doi.org/10.1016/j.jaad.2016.10.048 (2017).
Frisoli, M. L., Essien, K. & Harris, J. E. Vitiligo: Mechanisms of pathogenesis and treatment. Annu. Rev. Immunol. 26(38), 621–648. https://doi.org/10.1146/annurev-immunol-100919-023531 (2020).
van Geel, N. & Speeckaert, R. Segmental Vitiligo. Dermatol. Clin. 35(2), 145–150. https://doi.org/10.1016/j.det.2016.11.005 (2017).
Duman, R. S. & Voleti, B. Signaling pathways underlying the pathophysiology and treatment of depression: Novel mechanisms for rapid-acting agents. Trends Neurosci. 35(1), 47–56. https://doi.org/10.1016/j.tins.2011.11.004 (2012).
Miao, Z., Wang, Y. & Sun, Z. The relationships between stress, mental disorders, and epigenetic regulation of BDNF. Int. J. Mol. Sci. 21(4), 1375. https://doi.org/10.3390/ijms21041375 (2020).
Peng, S., Li, W., Lv, L., Zhang, Z. & Zhan, X. BDNF as a biomarker in diagnosis and evaluation of treatment for schizophrenia and depression. Discov. Med. 26(143), 127–136 (2018).
Notaras, M. & van den Buuse, M. Neurobiology of BDNF in fear memory, sensitivity to stress, and stress-related disorders. Mol. Psychiatry. 25(10), 2251–2274. https://doi.org/10.1038/s41380-019-0639-2 (2020).
Slominski, A. et al. Cutaneous expression of corticotropin-releasing hormone (CRH), urocortin, and CRH receptors. FASEB J. 15(10), 1678–1693. https://doi.org/10.1096/fj.00-0850rev (2001).
Acknowledgements
The authors would like to thank all patients who agreed to participate in this study.
Funding
This research was carried out as the part of PhD project.
Author information
Authors and Affiliations
Contributions
Conceptualization: Y.S., A.A., E.D., S.A., Methodology: Y.S., A.K., L.K. Validation: A.K., L.K. Formal analysis: N.G., L.K. Resources: A.A., M.M., R.T., S.A., Z.Kh., L.P. A.Ka. Data curation: A.A., E.D., R.T., Z.Kh., A.Ka., M.M., L.P. Writing—original draft preparation: Y.S., A.K., L.K., N.G. Writing—review and editing: A.K., L.K., Y.S., A.A., M.M., R.T., Z.Kh., A.Ka., L.P., D.E., S.A., N.G. Visualization: A.K., L.K., N.G., M.M., E.D. Supervision: Y.S., A.A., R.T., S.A., Z.Kh., L.P., A.Ka. Project administration: A.K., Y.S., A.A., E.D., S.A. Software: N.G., L.K.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Kussainova, A., Kassym, L., Akhmetova, A. et al. Associations between serum levels of brain-derived neurotrophic factor, corticotropin releasing hormone and mental distress in vitiligo patients. Sci Rep 12, 7260 (2022). https://doi.org/10.1038/s41598-022-11028-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-022-11028-8
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
