
Abstract
Metastatic and localized mismatch repair-deficient (dMMR) tumors are exquisitely sensitive to immune checkpoint blockade (ICB). The ability of ICB to prevent dMMR malignant or pre-malignant neoplasia development in patients with Lynch syndrome (LS) is unknown. Of 172 cancer-affected patients with LS who had received ≥1 ICB cycles, 21 (12%) developed subsequent malignancies after ICB exposure, 91% (29/32) of which were dMMR, with median time to development of 21 months (interquartile range, 6–38). Twenty-four of 61 (39%) ICB-treated patients who subsequently underwent surveillance colonoscopy had premalignant polyps. Within matched pre-ICB and post-ICB follow-up periods, the overall rate of tumor development was unchanged; however, on subgroup analysis, a decreased incidence of post-ICB visceral tumors was observed. These data suggest that ICB treatment of LS-associated tumors does not eliminate risk of new neoplasia development, and LS-specific surveillance strategies should continue. These data have implications for immunopreventative strategies and provide insight into the immunobiology of dMMR tumors.
This is a preview of subscription content, access via your institution
Access options
Access Nature and 54 other Nature Portfolio journals
Get Nature+, our best-value online-access subscription
$29.99 / 30 days
cancel any time
Subscribe to this journal
Receive 12 print issues and online access
$209.00 per year
only $17.42 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout


Similar content being viewed by others


Data availability
All information regarding the study cohort and pre-ICB and post-ICB malignancies is available in the extended data and supplementary tables. Additional information can be provided by the corresponding author in accordance with institutional regulatory approval within 8 weeks of request. Genomic data derived from MSK-IMPACT are available in aggregated form via the cBioPortal for Cancer Genomics (http://cbioportal.org).
References
Win, A. K. et al. Colorectal and other cancer risks for carriers and noncarriers from families with a DNA mismatch repair gene mutation: a prospective cohort study. J. Clin. Oncol. 30, 958–964 (2012).
Latham, A. et al. Microsatellite instability is associated with the presence of Lynch syndrome pan-cancer. J. Clin. Oncol. 37, 286–295 (2019).
Le, D. T. et al. Mismatch repair deficiency predicts response of solid tumors to PD-1 blockade. Science 357, 409–413 (2017).
Cercek, A. et al. PD-1 blockade in mismatch repair–deficient, locally advanced rectal cancer. N. Engl. J. Med. 386, 2363–2376 (2022).
Chalabi, M. et al. Neoadjuvant immunotherapy leads to pathological responses in MMR-proficient and MMR-deficient early-stage colon cancers. Nat. Med. 26, 566–576 (2020).
Heudel, P. et al. Immune checkpoint inhibitor treatment of a first cancer is associated with a decreased incidence of second primary cancer. ESMO Open 6, 100044 (2021).
Zehir, A. et al. Mutational landscape of metastatic cancer revealed from prospective clinical sequencing of 10,000 patients. Nat. Med. 23, 703–173 (2017).
Yan et al. Structure of the mucosal and stool microbiome in Lynch syndrome. Cell Host Microbe 27, 585–600 (2020).
Del Carmen, G et al. Colorectal surveillance outcomes from an institutional longitudinal cohort of lynch syndrome carriers. Front. Oncol. 13, 1146825.
Middha, S. et al. Reliable pan-cancer microsatellite instability assessment by using targeted next-generation sequencing data. JCO Precis. Oncol. 2017, PO.17.00084 (2017).
Moller, P. et al. Incidence of and survival after subsequent cancers in carriers of pathogenic MMR variants with previous cancer: a report from the prospective Lynch syndrome database. Gut 66, 1657–1664 (2017).
Mandal, R. et al. Genetic diversity of tumors with mismatch repair deficiency influences anti-PD-1 immunotherapy response. Science 364, 485–491 (2019).
Amodio, V. et al. Genetic and pharmacological modulation of DNA mismatch repair heterogeneous tumors promotes immune surveillance. Cancer Cell 41, 196–209 (2022).
Westcott, P. M. K. et al. Mismatch repair deficiency is not sufficient to increase tumor immunogenicity. Nat Genet (2023). https://doi.org/10.1038/s41588-023-01499-4
Ahadova, A. et al. The ‘unnatural’ history of colorectal cancer in Lynch syndrome: lessons from colonoscopy surveillance. Int. J. Cancer 148, 800–811 (2021).
Kloor, M. et al. Prevalence of mismatch repair-deficient crypt foci in Lynch syndrome: a pathological study. Lancet Oncol. 13, 598–606 (2012).
Ahadova, A. et al. A ‘two-in-one hit’ model of shortcut carcinogenesis in MLH1 Lynch syndrome carriers. Gastroenterology 165, 267–270 (2023).
Chang, K. et al. Immune profiling of premalignant lesions in patients with Lynch syndrome. JAMA Oncol. 4, 1085–1092 (2018).
Yurgelun, M. B. et al. Microsatellite instability and DNA mismatch repair protein deficiency in Lynch syndrome colorectal polyps. Cancer Prev. Res. 5, 574–582 (2012).
Roudko, V. et al. Shared immunogenic poly-epitope frameshift mutations in microsatellite unstable tumors. Cell 183, 1634–1649 (2020).
Cheng, D. T. et al. Comprehensive detection of germline variants by MSK-IMPACT, a clinical diagnostic platform for solid tumor molecular oncology and concurrent cancer predisposition testing. BMC Med. Genomics 10, 33 (2017).
Cheng, D. T. et al. Memorial Sloan Kettering-Integrated Mutation Profiling of Actionable Cancer Targets (MSK-IMPACT): a hybridization capture-based next-generation sequencing clinical assay for solid tumor molecular oncology. J. Mol. Diagn. 17, 251–264 (2015).
Shia, J. The diversity of tumours with microsatellite instability: molecular mechanisms and impact upon microsatellite instability testing and mismatch repair protein immunohistochemistry. Histopathology 78, 485–497 (2021).
Ziegler, J. et al. MiMSI—a deep multiple instance learning framework improves microsatellite instability detection from tumor next-generation sequencing. Preprint at bioRxiv https://doi.org/10.1101/2020.09.16.299925 (2020).
Jurtz, V. et al. NetMHCpan-4.0: improved peptide–MHC class I interaction predictions integrating eluted ligand and peptide binding affinity data. J. Immunol. 199, 3360–3368 (2017).
Paul, S. et al. Benchmarking predictions of MHC class I restricted T cell epitopes in a comprehensively studied model system. PLoS Comput. Biol. 16, e1007757 (2020).
Shukla, S. A. et al. Comprehensive analysis of cancer-associated somatic mutations in class I HLA genes. Nat. Biotechnol. 33, 1152–1158 (2015).
Shen, R. & Seshan, V. E. FACETS: allele-specific copy number and clonal heterogeneity analysis tool for high-throughput DNA sequencing. Nucleic Acids Res. 44, e131 (2016).
McGranahan, N. et al. Allele-specific HLA loss and immune escape in lung cancer evolution. Cell 171, 1259–1271 (2017).
Harrold, E. et al. The frequency of second primary malignancies and colonic polyps in Lynch syndrome with MSI tumors following immune checkpoint blockade. J. Clin. Oncol. 40, 10505–10505 (2022).
Acknowledgements
This work was supported, in part, through the Marie-Josée and Henry R. Kravis Center for Molecular Oncology at Memorial Sloan Kettering Cancer Center (D.B.S., M.F.B. and Z.K.S.); the Precision, Interception and Prevention Program at Memorial Sloan Kettering Cancer Center (Z.K.S. and L.A.D.); the Robert and Kate Niehaus Center for Inherited Cancer Genomics at Memorial Sloan Kettering Cancer Center (Z.K.S. and K.O.); the Romeo Milio Lynch Syndrome Foundation (Z.K.S.); the Fieldstone Fund (Z.K.S.); Swim Across America (L.A.D.); National Institutes of Health, National Cancer Institute exploratory/developmental grant R21 CA252519 (L.A.D. and A.C.); National Institutes of Health 1K08CA279922 (M.B.F.); the Chris4Life Colorectal Cancer Alliance Early Investigator Award (M.B.F.); and the National Institutes of Health, National Cancer Institute Cancer Center Support Grants P30 CA008748 (all authors), P50 CA221745 (D.B.S. and J.E.R.) and P50 CA092629 (D.B.S. and D.R.). The authors would also like to acknowledge the contributions of D. Stephens who assisted with the use of SnpEff program version 5.1d (https://pcingola.github.io/SnpEff/) to predict translated amino acid sequences for each respective mutation derived from the MSK-IMPACT NGS panel. This work, in part, was an Oral Presentation at the American Society of Clinical Oncology Annual Meeting in 2022 (ref. 30).
Author information
Authors and Affiliations
Contributions
E.C.H. and Z.K.S. conceived of the presented idea. E.C.H. collated the data and annotated the clinicodemographic details. A.M., M.B. and F.K. assisted with data collection and collation. B.R. and M.B.F. advised on reinterpretation of genomic data and derivation of neoantigen sequences. H.W. assisted with analysis of MSK-IMPACT targeted NGS genomic data. C.B. assisted with derivation of HLA subtypes using the MSK-IMPACT targeted NGS panel. M.B.F. completed the analysis of pre-ICB and post-ICB tumors using R software. A.L.R. completed analysis of post-ICB tumors for HLA LOH. Both Z.K.S. and L.A.D. supervised the findings of this work. All authors discussed the results and contributed to the final manuscript.
Corresponding author
Ethics declarations
Competing interests
E.C.H. has received funding from the Conquer Cancer ASCO Foundation. She also served as a consultant to Pfizer Ireland on one occasion in 2021. She reports education grants from Merck and Amgen to attend GI ASCO in 2020. B.R. serves as a consultant for Neophore and has a patent: ‘Methods and composition for cancer immunotherapy’. F.K. has received funding from the Conquer Cancer ASCO Foundation. A.C. serves as a consultant for Bayer, GlaxoSmithKline, Janssen Biotech, Merck and Seagen and receives research funding from GlaxoSmithKline, Inspirna and Seagen. R.Y. serves as a consultant for Array BioPharma/Pfizer, Amgen, Mirati Therapeutics and Natera and receives research funding to her institution from Pfizer, Boehringer Ingelheim, Mirati Therapeutics and Daiichi Sankyo. D.R. is an uncompensated advisor/steering committee member and receives research support from Janssen, AstraZeneca, Bayer, Myovant, Genentech, Promontory and Bristol Myers Squibb/Celgene. N.H.S. serves as a consultant for ABL Bio, Amgen, AstraZeneca, Boehringer Ingelheim, GlaxoSmithKline, Immunocore, Novartis, Psioxus, Puretech, Revitope, Roche/Genentech and Numab and receives grant/contracts from AstraZeneca, Bristol Myers Squibb, Immunocore, Merck, Pfizer, Puretech, Regeneron Pharmaceuticals, Roche/Genentech and Agenus. E.M.O. receives research from Genentech/Roche, Bristol Myers Squibb/Celgene, BioNTech, AstraZeneca, Arcus, Elicio, Parker Institute and NIH/NCI and serves as a consultant for CytomX Therapeutics (Data and Safety Monitoring Board (DSMB)), Rafael Therapeutics (DSMB), Seagen, Boehringer Ingelheim, BioNTech, Ipsen, Merck, IDEAYA, Silenseed, Novartis, AstraZeneca, BioSapien, Astellas, Thetis, Autem, Novocure, Neogene, Bristol Myers Squibb, ZielBio, Merus, Tempus and Fibrogen. An immediate family member serves as a consultant for Agios, Genentech/Roche, Eisai and Servier. D.R. receives research funds from Merck, Novartis and Ipsen and is on the scientific advisory board for Chiasma, Novartis and Advanced Accelerator Applications. Y.Y.J. receives research funding from Bayer, Bristol Myers Squibb, Cycle for Survival, the US Department of Defense, Eli Lilly, Fred’s Team, Genentech/Roche, Merck, NCI and RGENIX and serves on the advisory boards/is a consultant for Amerisource Bergen, Arcus Biosciences, AstraZeneca, Basilea Pharmaceutica, Bayer, Bristol Myers Squibb, Daiichi Sankyo, Eli Lilly, Geneos Therapeutics, GlaxoSmithKline, Imedex, Imugene, Lynx Health, Merck, Merck Serono, Mersana Therapeutics, Michael J. Hennessy Associates, Paradigm Medical Communications, PeerView Institute, Pfizer, Research to Practice, RGENIX, Seagen, Silverback Therapeutics and Zymeworks and has stock options in RGENIX. Y.R.M.-G. reports travel, accommodation and expenses from AstraZeneca and Loxo Oncology/Eli Lilly. She acknowledges honoraria from Virology Education and Projects in Knowledge (for a CME program funded by an educational grant from Amgen). She also acknowledges associated research funding to the institution from Mirati Therapetuics, Loxo Oncology/Eli Lilly, Elucida Oncology, Taiho Oncology, Hengrui USA, Jiangsu Hengrui Pharmaceuticals, Luzsana Biotechnology, Endeavor Biomedicines and AbbVie. She is an employee of Memorial Sloan Kettering Cancer Center, which has an institutional interest in Elucida. She acknowledges royalties from Rutgers University Press and Wolters Kluwer. She acknowledges food and beverages from Endeavor Biomedicines. Y.R.M.-G. also acknowledges receipt of training through an institutional K30 grant from the NIH (CTSA UL1TR00457). She has received funding from a Kristina M. Day Young Investigator Award from Conquer Cancer and the ASCO Foundation, endowed by Dr. Charles M. Baum and Carol A. Baum. She is also funded by the Fiona and Stanley Druckenmiller Center for Lung Cancer Research, the Andrew Sabin Family Foundation, the Society for MSK and a Paul Calabresi Career Development Award for Clinical Oncology (NIH/NCI K12 CA184746). Y.L.L. reports research funding from AstraZeneca, GlaxoSmithKline and Repare Therapeutics outside this work. J.E.R. has received research support for clinical trials from Bayer, Seagen, Astellas, AstraZeneca and Roche/Genentech. He has served as an advisor or consultant to Bayer, Seagen, Astellas, AstraZeneca, Roche/Genentech, Bristol Myers Squibb, Merck, Pfizer, Boehringer Ingelheim, GlaxoSmithKline, Janssen, Mirati, EMD Serono, Gilead, Alligator Biosciences, Eli Lilly, Tyra Biosciences, Infinity, IMVax, Aadi, Century Therapeutics, Emergence Therapeutics and Hengrui. M.R.W. participates in Precisa online tumor board and is editor of Colorectal Section UpToDate. A.M.R. serves as a consultant for Regeneron, Evolve CME, Almiral, Mavig, Dynamed, Canfield Scientific, Evolus, Biofrontera, QuantiaMD, Lam Therapeutics and Cutera. He participated in an Advisory board for AllerganInc. He serves as an advisor to Skinfix and L’Oreal; he is a founder of DAR companies and is on the Board of Skinpass. A.M.R. received research/study funding from ASLMS: A Ward Memorial Research Grant, Skin Cancer Foundation, Regen, LeoPharma and Biofrontera and serves as Editorial Board: Lasers in Surgery and Medicine, CUTIS, Journal of the American Academy of Dermatology and Dermatologic Surgery. He is a Board Member: ASDS, and a Committee Member and/or Chair: AAD, ASDS and ASLM. A.M.R acknowledges travel support from Merz. K.O. is a founder (uncompenstated, shares not alloted) of AnaNeo Therapeutics. Patents, royalties, other intellectual property: ‘Diagnosis and treatment of ERCC3-mutant cancer’; inventors: Joseph Vijai, Sabine Topka and Kenneth Offit; US National Stage Patent Application No.: 16/493,214; filing date: 11 September 2019 (institution). M.F.B. serves as a consultant for Eli Lilly and AstraZeneca and receives research support from Boundless Bio. D.B.S. has served as a consultant for/received honorarium from Pfizer, Loxo Oncology/Eli Lilly, Vividion Therapeutics, Scorpion Therapeutics, FORE Therapeutics, Fog Pharma, Elsie Biotechnologies and BridgeBio. L.S. serves as consultant and is a member of the scientific advisory board for Genor Biopharma. J.S. serves as a consultant for Paige AI. L.A.D. is a member of the board of directors of Quest Diagnostics and Epitope. He is a compensated consultant to PetDx, Innovatus CP, Se’er, Delfi, Blackstone, Kinnate and Neophore. L.A.D. is an inventor on multiple licensed patents related to technology for circulating tumor DNA analyses and mismatch repair deficiency for diagnosis and therapy. Some of these licenses and relationships are associated with equity or royalty payments to the inventors. He holds equity in Quest Diagnostics, Epitope, PetDx, Se’er, Delfi, Kinnate and Neophore. He divested his equity in Personal Genome Diagnostics to LabCorp in February 2022 and divested his equity in Thrive Earlier Detection to Exact Biosciences in January 2021. His spouse holds equity in Amgen. The terms of all these arrangements are being managed by Memorial Sloan Kettering Cancer Center in accordance with their conflict of interest policy. Z.K.S.’s immediate family member serves as a consultant in ophthalmology for Adverum, Genentech, Neurogene, Novartis, Optos Plc, Outlook Therapeutics and Regeneron outside the submitted work. Z.K.S. serves as an associate editor for JCO Precision Oncology and as a section editor for UpToDate. E.C.H., M.B.F., B.R., L.A.D. and Z.K.S. filed a patent application (patent number 63/578,057) reflecting the findings of this manuscript.
Peer review
Peer review information
Nature Medicine thanks Eduardo Vilar, Takayuki Yoshino and the other, anonymous, reviewer(s) for their contribution to the peer review of this work. Primary Handling Editor: Saheli Sadanand, in collaboration with the Nature Medicine team.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Extended data
Extended Data Fig. 1 Study Cohort of patients with Lynch Syndrome from MSKCC.
Consort diagram of study cohort. Segregated by microsatellite status as designated by MSIsensor14. MSKCC: Memorial Sloan Kettering Cancer Center; MSI: Microsatellite unstable; MSS: Microsatellite stable.
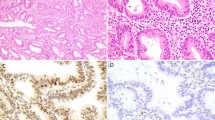
Extended Data Fig. 2 Histological evaluation of patient 7′s sequential tumors demonstrating distinct histological and immunohistochemical features.
(Patient example Fig. 1a, patient 7 Fig. 1b, Extended Data Tables 3/4). a, Tumor 3: Gastric adenocarcinoma. b, Tumor 4: Colorectal adenocarcinoma. c, Tumor 5: Prostate adenocarcinoma. d, Tumor 6: Small bowel adenocarcinoma. The relevant stain, hematoxylin and eosin, was run on each chosen study tissue block once. All antibodies and staining protocols are validated and optimized to current standards.
Extended Data Fig. 3 Paired analysis of pre- and post-immune checkpoint blockade (ICB) exposed tumors using MSK-IMPACT next-generation sequencing derived data22.
Nonsynonymous somatic mutations from the MSK IMPACT variant call format (VCF) output from each sequenced patient tumor were input into the SnpEff program v5.1d (https://pcingola.github.io/SnpEff/) to predict translated amino acid sequences for each respective mutation. The number of unique mutation associated neoantigens (MANA) was determined by taking the defined peptide sequence and evaluating all potential contiguous 9′mer variations using a sliding reading frame. a, Comparison of total missense mutations in pre- and post-ICB tumors. b, Comparison of mutation associated neoantigens between pre- and post-ICB tumors. All boxplots are composed of median (central line), 25th–75th percentile (box edges), and minimum and maximum values (whiskers). All analyses included 9 distinct pre and 9 distinct post tumors paired for 9 unique patients. p-values are derived from pairwise t-testing based on patient.
Extended Data Fig. 4 Sensitivity analyses of pre- and post-immune checkpoint blockade (ICB) exposed tumors using MSK-IMPACT next generation sequencing derived data22.
a, d, MSIsensor score, tumor mutational burden (TMB), frameshift mutation rates and number of mutation associated neoantigens (MANA) between pre- and post-ICB exposed tumors when grouped by gastrointestinal cancer only. e-h, MSIsensor score, tumor mutational burden (TMB), frameshift mutation rates and number of mutation associated neoantigens (MANA) between pre- and post-ICB exposed tumors when grouped by urothelial cancers only. All boxplots are composed of median (central line), 25th–75th percentile (box edges), and minimum and maximum values (whiskers). P-values are derived from student’s t-test (unpaired) between pre and post tumors agnostic of patient identity. Analysis a (MSIsensor score) includes 8 unique tumors (6 pre and 2 post) from 7 unique patients, and the other analyses, b-h, include 9 unique tumors (6 pre and 3 post) from 7 unique patients.
Extended Data Fig. 5 Immunohistochemical analysis of immune cell infiltration of pre-immune checkpoint blockade (ICB) and post-ICB tumors.
a, and b, Intra-patient comparison of paired pre- (a) and post-ICB tumors (b). CD8 tumor infiltrating lymphocytes (CD8 TILS) in the non-ICB exposed urothelial cancer and the post-ICB exposure cutaneous squamous cell carcinoma. HPF: High Power Field. c, Interpatient comparisons of CD8 TILS, programmed cell death 1 protein (PD1) positive TILS and programmed cell death ligand 1 (PDL1) combined positive score (CPS) in tumors arising prior to ICB exposure (N = 8), tumors arising whilst patients were on ICB (N = 5) and tumors arising post completion of ICB (N = 2). Mean and standard deviation (SEM) are represented and compared using ordinary one way ANOVA test corrected for multiple comparisons.*: P ≤ 0.05 and P > 0.01, ns: non significant. Stains with the relevant antibodies, CD8 antibody (clone C8/144B, Catalog # sc-53212, diluted 1:100, Dako), PD-1 (clone NAT105, Catalog # 760-4895, ready to use, Cell Marque), and PD-L1 (cloneE1L3N, Catalog # 13684 S, diluted 1:100, Cell Signaling) were run on each chosen study tissue block once. All antibodies and staining protocols are validated and optimized to current standards.
Extended Data Fig. 6 Incidence of subsequent primary malignancies (SPM) in the immune checkpoint blockade (ICB) treated and non-ICB (chemotherapy) treated patients with Lynch syndrome.
a, SPM incidence at 5-years matched follow-up in the ICB treated (pre- and post-ICB) and non-ICB treated cohort (pre- and post-chemotherapy). The number of matched patient pre/post ICB or pre/post chemotherapy is reported below the figure. The 5 year incidence of 2nd neoplasm for each clinical condition is reported above the box plot representing the mean and standard deviation (SEM). Pre and post 5 year incidence were compared using paired t test. ns: non significant, P > 0.05. b, SPM incidence in patients defined as high risk (HR). HR-patients were defined as patients presenting with multiple non concomitant cancers (> = 2) in a pre-ICB delay matched with post-ICB follow up. 3-year and 5-year incidence calculation was performed excluding the index cancer and concomitant cancers ( < 1 month between diagnoses of cancers). The number of matched patient pre/post ICB or pre/post chemotherapy for 3-year and 5-year incidence of 2nd neoplasm is reported below the figure. The 3-year and 5-year incidence of 2nd neoplasm for each clinical condition is reported above the box plot representing the mean and standard deviation (SEM). Pre and post 3-year or 5-year incidence were compared using paired t test. ns: non significant, P > 0.05. c, Swimmers plot demonstration cancer occurrence pre- and post-ICB exposure in the HR patient cohort over time in months for patients with match pre and post ICB follow up. The patient numbers for the ones developing post ICB neoplasms correspond to those reported in Fig. 1 (patients 15, 8, 7 and 4). Other high-risk patients (HR) are numerated from 1 to 12. Median ICB duration and follow up (FU) are reported for patients developing post ICB neoplasms and for the patients not developing post ICB neoplasm. The order of neoplasm occurring during the matched pre and post ICB follow up is reported. No statistical comparison was performed. d, Cumulative post-ICB cancer incidence in the ICB-exposed HR-patient cohort. High risk Patients with a matched follow up pre- and post-ICB of 36 months were selected and all non-index cancers occurring during the window of observation were accounted for. Cumulative incidence is reported as the cumulative sum of non-index cancers occurring during the period of observation. Number of patients and cumulative observation time in months are reported. Fisher’s exact test comparing the cumulative observation time without a neoplasm event to the number of months with an event was used for statistical analysis. ***: P < 0.001.
Supplementary information
Supplementary Table 1
Characteristics of tumors targeted (TT) by ICB and the SPM after ICB. ADT, androgen deprivation therapy; CR, complete response; DCIS, ductal carcinoma in situ; HCC, hepatocellular carcinoma; POD, progression of disease; PSA, prostate-specific antigen; SCC, squamous cell carcinoma of skin; SD, stable disease; SNV, single-nucleotide variant; TVA, tubulovillous adenoma. *Not present radiologically on baseline imaging.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Harrold, E.C., Foote, M.B., Rousseau, B. et al. Neoplasia risk in patients with Lynch syndrome treated with immune checkpoint blockade. Nat Med 29, 2458–2463 (2023). https://doi.org/10.1038/s41591-023-02544-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41591-023-02544-9
