
Abstract
Purpose
Genetic and genomic health information increasingly informs routine clinical care and treatment. This systematic review aimed to identify the barriers and facilitators to integrating genetics and genomics into nurses’ and physicians’ usual practice (mainstreaming).
Methods
A search of MEDLINE, EMBASE, CINAHL, and PsycINFO generated 7873 articles, of which 48 were included. Using narrative synthesis, barriers and facilitators were mapped to the Theoretical Domains Framework (TDF).
Results
Barriers were limitations to genetics knowledge and skill, low confidence initiating genetics discussions, lack of resources and guidelines, and concerns about discrimination and psychological harm. Facilitators were positive attitudes toward genetics, willingness to participate in discussions upon patient initiation, and intention to engage in genetics education.
Conclusion
Nurses and physicians are largely underprepared to integrate genetic and genomic health information into routine clinical care. Ethical, legal, and psychological concerns surrounding genetic information can lead to avoidance of genetics discussions. The knowledge–practice gap could limit patients’ and families’ access to vital genetic information. Building the capacity of the current and next generation of nurses and physicians to integrate genetics and genomics into usual clinical practice is essential if opportunities afforded by precision medicine are to be fully realized.
Similar content being viewed by others

INTRODUCTION
During the past two decades, the field of human genetics has undergone significant change. The sequencing of the human genome has fueled understanding of the relationship between genetic variation and human health.1 Demand is such that clinical nurses and physicians working in a variety of clinical disciplines are now required to integrate genetics into routine care. For example, ovarian cancer patients with a DNA-repair deficiency may be exquisitely responsive to poly-ADP ribose polymerase inhibitors2 and cardiologists may consider implantable cardioverter defibrillators for those at risk of sudden cardiac death.3 Reductions in the cost of genetic testing4 and greater public access to and awareness of genetic information5 mean more people seek genetic information than ever before. Collectively, these changes have prompted the acceleration of genetic information as a critical element of care for many patient populations.
Considering the changing landscape of genetic and genomic (herein referred to as “genetic” only) opportunities, care pathways for patients to access genetic information need to adapt. Traditionally, access involved referral of patients to tertiary centers for genetic counseling. However, the demands on genetics services are outweighing workforce capacity,6 with policy makers calling for alternative genetic models of care.7,8 One such model is mainstreaming, which involves nongenetics nurses and physicians identifying at-risk individuals and initiating genetics discussions9 by integrating genetics into practice. Examples include taking a family history, assessing the chance of a genetic condition, organizing genetic testing, or delivering a genetic test result to a patient. The benefits of identifying individuals with a genetic condition through mainstreaming are threefold: targeted treatments may be available, a genetic diagnosis may alert the treating specialist to other possible health problems the individual could face, and the individual’s relatives can be offered predictive testing (targeted testing for the genetic condition identified in their relative). Predictive testing guides the relative’s need for health screening or risk management.
Despite the benefits of genetic health information, translation of research to clinical practice is slow, highlighting the complex and interconnected barriers and facilitators within health-care pathways.10 Identifying the underlying barriers and facilitators to nurses and physicians integrating genetics into their practice will lay the groundwork for the development of an evidence-based intervention to encourage behavior change.11 The aim of this review was to identify the barriers and facilitators for nurses and physicians working in secondary and tertiary care to integrate genetics and genomics into their usual practice. The secondary aim was to explore the similarities and differences between the specialties and disciplines.
MATERIALS AND METHODS
This systematic review was registered with PROSPERO (CRD42019134752) and conducted in accordance with the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) statement.12 MEDLINE, Cochrane Database of Systematic Reviews, PROSPERO, and the Joanna Briggs Institute Systematic Reviews database were searched to ensure this systematic review would not duplicate existing work.
Search strategy
The search strategy was developed in consultation with an information services librarian. MEDLINE, EMBASE, CINAHL, and PsycINFO were searched on 30 August 2019 with no restrictions (MEDLINE search available in Supplementary file 2). Further articles were elicited by backwards searching reference lists of included articles and relevant literature reviews, forwards searching articles using the Web of Science database, and reviewing first author profiles of included articles on ResearchGate (www.researchgate.net).
Inclusion and exclusion criteria
Inclusion and exclusion criteria were developed using the PICOS framework.12 Articles were included if they were reported after the first initial human genome sequence was published in February 2001,1 published in English in a peer-reviewed journal, and reported empirical data on the barriers or facilitators nurses and/or physicians encountered when providing genetic information to adults cared for in a secondary or tertiary health-care setting. The Royal Australasian College of Physicians Advanced Training Programs were used as a specialty guide to include nurses and doctors who were most likely to work in secondary and tertiary care.13 Articles were excluded if they reported on direct-to-consumer genetic testing, pharmacogenetic testing, or reproductive carrier testing, or the nurse or physician worked in a primary care, pediatric, prenatal, research, or clinical genetics setting. Primary care nurses and doctors were excluded due to the breadth of articles in this area and the existence of previous systematic reviews evaluating genetic interventions in the primary care setting.14 See Supplementary file 3 for further details.
Screening and extraction
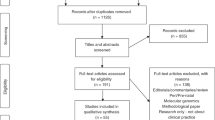
Following deduplication, one reviewer (S.W.) screened all articles against the inclusion and exclusion criteria by title and abstract and then by full text (see Fig. 1). A 20% sample was allocated to a second reviewer (C.J.) at both stages and interrater concordance was calculated using a prevalence-adjusted, bias-adjusted kappa statistic (≥0.7.)15 Disagreements were resolved through discussion. Up to three attempts were made to email authors of articles with missing or ambiguous information.

Following deduplication, 7873 unique articles were screened against eligibility criteria, resulting in 48 articles for inclusion.
Data items were predetermined using the Joanna Briggs data extraction instrument.16 Extraction was performed using QSR International’s NVivo Version 12 and exported to an Excel spreadsheet.
Risk of bias
Individual risk of bias assessments were conducted using the QualSyst tool.17 With the aim of including a range of clinical disciplines, articles with a high risk of bias were not excluded. To assess for outcome reporting bias, published study protocols were searched using the World Health Organization’s (WHO) International Clinical Trial’s registry platform. No study protocols were identified in the initial systematic search, therefore publication bias could not be assessed.
Data synthesis
Narrative synthesis was performed using the Theoretical Domains Framework (TDF) to map the barriers and facilitators to higher behavioral domains and components.18 The TDF is a validated, comprehensive framework describing factors affecting health professional behavior and can be adapted to diverse clinical contexts.10
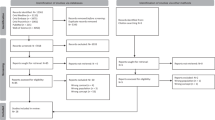
Extracted data items were grouped into themes. If the data item did not adequately correspond to an existing theme, a new theme was created. Each theme was mapped to a TDF domain and the frequency of each domain was calculated as a percentage of the total number of articles. The TDF domains sit within the Behaviour Change Wheel’s Capability–Opportunity–Motivation Behaviour System (COM-B19) and these components were used to organize and describe the results. This process is represented in Fig. 2. The differences between nurses and physicians and between clinical disciplines were described narratively.

Extracted data items were systematically grouped into themes. Themes were mapped to the correpsonding TDF Domain, and each TDF Domain is associated with a COM-B component. TDF Theoretical Domains Framework, COM-B Capability-Opportunity-Motivation system in the Behaviour Change Wheel.
RESULTS
Study characteristics
Nearly all of the 48 included articles were from high income countries (n = 45, 94%). Half of the articles originated from the United States (n = 25, 52%) and involved oncology nurses or physicians (n = 24, 48%). The majority of articles were surveys (n = 38, 79%), which largely used novel, unvalidated instruments (37/38, 97%). Three-quarters of the articles only included physicians (n = 35, 73%), were published after 2011 (n = 36, 75%), and were assessed as having a low risk of bias (0.67–1.0; n = 35, 73%). There were no significant differences in reported barriers and facilitators between quantitative, qualitative, and mixed-methods articles.
Factors influencing integration of genetics and genomics
Most articles (n = 40, 83%) reported both barriers and facilitators, while a small number only reported the facilitators (n = 5, 10%)20,21,22,23,24 or the barriers (n = 3, 6%).25,26,27 Themes were broadly associated with nurses’ and physicians’ capability (n = 44, 92%), opportunity (n = 39, 81%), and motivation (n = 38 articles, 79%) to integrate genetics into practice (Supplementary file 4).
Capability to integrate genetics into practice
Knowledge and skill
Twenty-seven articles (56%) explored nurses’ and physicians’ knowledge of genetics,9,26,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52 while 41 articles (85%) reported on their skills.9,21,22,23,24,25,27,28,29,30,31,32,33,34,35,37,38,39,40,41,42,43,44,45,46,47,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63 While nurses and physicians routinely engaged in discussions about genetics with their patients,22,24,29,31,38,42,47,49,52,53,54,55,56 most demonstrated limited understanding of general genetic concepts, and/or concepts relevant to their specialty.26,28,29,30,31,32,33,34,35,36,37. In some specialties, family history information was routinely obtained,21,29,30,32,33,38,39,47,49,52,53,54,55 although the extent of the family history was not always adequate.28,31,32,35,39,57 A smaller number of articles reported that physicians did assess genetic risk,23,30,34,49,50,52,60,61 however, confidence in family history and individual risk assessment was low.9,29,32,35,37,38,40,43,44,45,49,53,57,58,59 Four articles reported an inverse relationship between years of clinical practice and level of knowledge.29,32,33,38
Oncologists and neurologists were most likely to order genetic testing. There were no reports of nurses or physicians from other specialties ordering testing.25,26,39,49,53,59,60,64,65,66 Most nurses and physicians had low awareness of genetic tests relevant to their area of practice.28,30,38,39,40,41,42,43 They also had difficulty interpreting a genetic test result.28,31,45,46,47,49,51
Opportunity to integrate genetics into practice
Environmental context and resources
Thirty-nine articles (81%) explored the impact of environmental context and resources on nurses’ and physicians’ ability to integrate genetics into practice. Nurses and physicians infrequently referred patients to clinical genetics services,28,29,31,32,33,34,36,38,40,51,53,54,55,60 primarily because of the prohibitive cost of accessing genetic testing,34,39,44,45,46,60,61,62,63,64,65 lack of resources,32,34,37,38,44,53,61,62,65 absence of guidelines,26,27,28,45,55,56,61 and of lack of time to initiate a genetics discussion.36,37,44,53,58,59,65 Some nurses and physicians had concerns about the privacy of genetic information or the process of informed consent.9,37,43,44,52,64,66 However, if patients raised questions or concerns about genetics, nurses and physicians did engage in these discussions.9,24,34,36,42,43,45,49,55,60,62
A small number of articles reported nurses and physicians actively avoided or refused to discuss genetics with their patients, where they felt genetics was not relevant to clinical care and there may be potential negative consequences of genetic information.21,28,36,39,44 For example, some palliative care clinicians considered their clinical setting as inappropriate to initiate discussions about genetics and were disappointed when this had not been addressed previously.9,40 Nurses and physicians reported the value of close working relationships or collaboration with clinical genetics professionals.9,28,29,32,34,37,49,56,59,62,65
Motivation to integrate genetics into practice
Belief about consequences
In total, 26 articles (54%) explored nurses’ and physicians’ belief about consequences. Nurses and physicians are cognizant of the potential medical benefit that genetic information can provide for patients,20,34,44,45,49,55,58,59,63,65,66 but this was tempered by concerns about the risk of psychological harm, such as inducing feelings of guilt or hopelessness.9,25,36,37,43,44,46,49 The potential benefit to relatives was described, including clarifying family members’ risks and providing screening or family planning options.9,28,38,44,47,52,55 Some nurses and physicians worried about the emotional impact of genetic information on the family.9,25,36,40,46,49 There were additional concerns about insurance and employment discrimination based on a genetic test result.29,41,43,44,46,47,64
Goals and professional role
Goals of the nurse or physician were explored by 11 articles (23%), while 14 articles (29%) reported views on professional roles. Nurses and physicians had mixed feelings about whether genetic information contributed to their clinical goals for the patient or aligned with their views about their professional role. Genetic information was not always perceived as particularly useful in the clinical setting.36,39,45,58,59,61,62,65 Genetic information was described as irrelevant by nurses and physicians in certain clinical disciplines, such as ophthalmology,36 and by particular professionals, such as breast surgeons.58,59 Viewing genetics as irrelevant to clinical practice appeared to foster an active resistance to integrating genetics into practice.36,58,59 In contrast, other nurses and physicians were confident in their competence to provide genetic information9,21,38,39,41,47,49,52,53,58,59,62 and, in their view, genetic information provision was appropriate within their clinical role.9,20,24,29,31,46,47,49,58,59,64 However, nurses and physicians were uncomfortable about providing genetic health information to at-risk relatives of their patients.31,36,49,56,58,59
Intention and optimism
Intention of the nurse or physician was explored by 16 articles (33%), while 14 articles (29%) reported on optimism. Nurses and physicians expressed positive attitudes toward genetics,9,20,24,32,34,37,55,58,59,64,66 reported their beliefs about the future benefit of genetic information for patients and society as a whole,22,29,36,47,55,64 and regarded genetic health information as an inevitable major factor in clinical care in the future.20,37,42,58,59 Nurses and physicians expressed their intention to engage in continuing professional education, demonstrating the need for increased genetic literacy. Most nurses and physicians preferred clinically relevant education in the form of workshops, lectures, or online content.9,21,28,29,30,33,35,36,43,45,47,53,56,57,58,59 Descriptions of nurses’ intentions to pursue further genetics education were more prevalent than articles reporting physicians’ intentions.
DISCUSSION
This systematic review identified that, while there are a number of indicators that nurses and physicians are engaging with genetics and have positive attitudes, there are also significant barriers that prevent them from doing this on a routine basis.
Consistent with previous reports,67 this review identified that nurses and physicians under-refer patients who require, or may require, assessment of their genetic risk based on their diagnosis or family history. Although there are likely to be a number of additional precursors to low referral rates, many nurses and physicians lack adequate genetics knowledge. Nurses’ and physicians’ low confidence in engaging in discussions about genetics or performing genetics-related tasks (such as obtaining family history information, performing a risk assessment, or interpreting a genetic test result) suggests an awareness of their limited knowledge. While it has been suggested that few nursing and medical undergraduate degrees adequately prepare graduates to integrate genetic health information into their clinical practice,68,69 this review found that more recent nursing and physician graduates had better genetics knowledge scores than their more experienced colleagues.29,32,33,38 Although an inverse relationship between years of practice and knowledge has been reported previously,70 this finding suggests educators are recognizing the importance of graduates having adequate genetics knowledge and incorporating this into undergraduate programs. It was noted, however, that articles describing nurses’ skill sets were less prevalent than articles describing the abilities of physicians. For nurses and physicians who did not receive adequate genetics education in basic training or who trained a long time ago, accessing continuing professional development can be marred by financial and scheduling barriers.71
Collaborative relationships between the nurse or physician and clinical genetics professionals was highlighted in this review as a valuable resource, with the potential to improve access to genetics education and increase the number of appropriate referrals to clinical genetics services.72 Nonetheless, while some nurses and physicians do feel capable of raising and discussing relevant genetic health information with their patients, others appear to engage reactively to their patients’ requests for genetic information or may feel obligated to initiate discussions where there are medical management implications dependent on a genetic test result.73 Articles describing nurses’ views about the appropriateness of genetics within their role were more prevalent than articles describing physicians’ views. Although issues of knowledge, skill, training, and resources play a significant role, other important factors contribute to nurses’ and physicians’ capacity to integrate genetics information into their practice.
Concerns about the ethical, legal, and psychological aspects of genetic information appear to critically inform their motivation to integrate genetics into practice. Depending on the nurse’s or physician’s views, motivation to integrate genetics into practice may vary. Pleasingly, a substantial number reported the potential positive effect of genetic health information, such as personalizing and improving medical management or providing risk advice to relatives who can benefit from screening or risk-reducing interventions.2 However, only a small number of nurses and physicians feel genetic information can improve psychological wellbeing.9,37,46 Concerns about the potential for genetic information to inflict psychological harm on patients were frequently reported, despite genetic counseling demonstrating an ability to reduce anxiety and improve accuracy of perceived genetic risk.74
Ethical and legal considerations, such as insurance or employment discrimination resulting from inappropriate sharing of genetic information, were also raised. While these concerns have been reported elsewhere by research participants and the general public, sharing of genomic data is widely considered to be a necessary step to improve understanding of the genetic basis of disease and future medical care.75 In this genomics era, government bodies are moving to develop ethical and legal safeguards for individuals and families; however, these processes can lag behind scientific developments and require refinement even after implementation.76 Meanwhile, nurses and physicians who have significant ethical, legal, or psychological concerns about genetic information may actively avoid initiating conversations about genetics with their patients.36 Sidestepping the opportunity to explore a patient’s genetic concerns may mean a vital opportunity is missed, particularly in specialties like palliative care, which represent the final chance to collect valuable patient knowledge about family history or a DNA sample that could benefit their relatives.77
Implication for future research
The majority of articles included in this review utilized an unvalidated survey to capture the barriers and facilitators faced by nurses and physicians in integrating genetics in their practice. Development of a validated tool to assess genetics practice, attitudes, and knowledge could be considered in future research, to enable more accurate comparisons between different specialties and disciplines.
To ensure patients and families have appropriate access to genetic health information, nurses and physicians need to successfully integrate genetics into their practice.11 To achieve this aim, there is a need for further research to understand the context-specific barriers and facilitators (for example in palliative care, oncology, and neurology) and develop evidence-based, theory-informed interventions.
Limitations
Limitations of this review relate to both the individual articles and review methodology. As discussed above, almost all quantitative reports used novel, unvalidated measures. To represent a range of disciplines and specialties, articles with high risk of bias were included, although their findings were present in other articles. Given resource issues, only English-language articles were included. The review was strengthened by adhering to the PRISMA guidelines and the use of a theoretical framework to map and synthesize outcomes.10,12 Although the findings of this review are not necessarily novel, synthesizing the literature to date will assist the genomics implementation field in developing theory-informed, evidence-based interventions.
Conclusion
Building the capacity of nurses and physicians to integrate genetics and genomics into routine clinical care is essential if opportunities afforded by precision medicine are to be fully realized. Many nurses and physicians have limited knowledge and skills about genetics and genomics, do not feel confident addressing these issues with patients, and lack resources and guidelines to direct them. Apprehension about ethical, legal, and psychological impacts of genetic information influence willingness to engage in genetics discussions, unless requested by patients. This review identified potential behavioral targets to inform the development of theory-informed, evidence-based interventions to facilitate the integration of genetics into nurses’ and physicians’ usual care. Such interventions will need to be tailored to the specific clinical setting.11
References
Lander ES, Linton LM, Birren B, et al. Initial sequencing and analysis of the human genome. Nature. 2001;409:860–921.
Konstantinopoulos PA, Matulonis UA. PARP inhibitors in ovarian cancer: a trailblazing and transformative journey. Clin Cancer Res. 2018;24:4062–4065.
Maron BJ, Spirito P, Shen WK, et al. Implantable cardioverter-defibrillators and prevention of sudden cardiac death in hypertrophic cardiomyopathy. JAMA. 2007;298:405–412.
Wetterstrand K. DNA sequencing costs: data from the NHGRI Genome Sequencing Program 2019. http://www.genome.gov/sequencingcostsdata. Accessed 28 Mar 2019.
Lee J, Kim S, Kang E, et al. Influence of the Angelina Jolie announcement and insurance reimbursement on practice patterns for hereditary breast cancer. J Breast Cancer. 2017;20:203–207.
Hoskovec JM, Bennett RL, Carey ME, et al. Projecting the supply and demand for certified genetic counselors: a workforce study. J Genet Couns. 2018;27:16–20.
Burke W, Khoury MJ, Stewart A, Zimmern RL. The path from genome-based research to population health: development of an international public health genomics network. Genet Med. 2006;8:451.
Department of Health. National Health Genomics Policy Framework 2018–2021. Canberra, ACT: Commonwealth of Australia; 2017.
Dearing A, Taverner N. Mainstreaming genetics in palliative care: barriers and suggestions for clinical genetic services. J Community Genet. 2018;9:243–256.
Cane J, O’Connor D, Michie S. Validation of the theoretical domains framework for use in behaviour change and implementation research. Implement Sci. 2012;7:37.
Craig P, Dieppe P, Macintyre S, Michie S, Nazareth I, Petticrew MJB. Developing and evaluating complex interventions: the new Medical Research Council guidance. BMJ. 2008;337:1655.
Moher D, Liberati A, Tetzlaff J, Altman D, The PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6:e1000097.
Royal Australasian College of Physicians. Advanced training programs 2020. https://www.racp.edu.au/trainees/advanced-training/advanced-training-programs.
Paneque M, Turchetti D, Jackson L, Lunt P, Houwink E, Skirton H. A systematic review of interventions to provide genetics education for primary care. BMC Fam Pract. 2016;17:89.
Mak H, Yau K, Chan B. Prevalence-adjusted bias-adjusted k values as additional indicators to measure observer agreement. Radiology. 2004;232:302–303.
Lockwood C, PorritK. Munn Z, et al.Systematic reviews of qualitative evidence. In:Aromataris E, Munn Z, editors. Reviewers’ manual. Joanna Briggs Institute; 2017.
Kmet LM, Cook LS, Lee RC. Standard quality assessment criteria for evaluating primary research papers from a variety of fields. Edmonton: Alberta Heritage Foundation for Medical Research; 2004.
Popay J, Roberts H, Sowden A, et al. Guidance on the conduct of narrative synthesis in systematic reviews: a product from the ESRC methods programme. Lancaster, UK: Institute of Health Research; 2006.
Michie S, van Stralen MM, West R. The behaviour change wheel: a new method for characterising and designing behaviour change interventions. Implement Sci. 2011;6:42.
Burcher S, Meiser B, Mitchell G, et al. Oncology health professionals’ attitudes toward treatment-focused genetic testing for women newly diagnosed with breast cancer. Pers Med. 2013;10:431–440.
Beitsch PD, Whitworth PW. Can breast surgeons provide breast cancer genetic testing? An American Society of Breast Surgeons survey. Ann Surg Oncol. 2014;21:4104–4108.
Arthur KC, Doyle C, Chiò A, Traynor BJ. Use of genetic testing in amyotrophic lateral sclerosis by neurologists. JAMA Neurol. 2017;74:125–126.
Katz SJ, Bondarenko I, Ward KC, et al. Association of attending surgeon with variation in the receipt of genetic testing after diagnosis of breast cancer. JAMA Surg. 2018;153:909–916.
Cleophat JE, Pelletier S, Joly Y, et al. Addressing cancer family history at the end of life: how frequent, relevant, and feasible is it? A survey of palliative care providers. Palliat Med. 2019;33:856–858.
Lillie AK, Clifford C, Metcalfe A. Caring for families with a family history of cancer: why concerns about genetic predisposition are missing from the palliative agenda. Palliat Med. 2011;25:117–124.
Kelly PP. Colorectal cancer family history assessment. Clin J Oncol Nurs. 2011;15:E75–E82.
Monahan KJ, Clark SK, British Society of Gastroenterology Cancer Group. A national survey of hereditary colorectal cancer services in the UK. Frontline Gastroenterol. 2014;5:130–134.
Van Langen I. Genetic knowledge and counselling skills of Dutch cardiologists: sufficient for the genomics era? Eur Heart J. 2003;24:560–566.
Finn CT, Wilcox MA, Korf BR, et al. Psychiatric genetics: a survey of psychiatrists’ knowledge, opinions, and practice patterns. J Clin Psychiatry. 2005;66:821–830.
Quillin JM, Bodurtha JN, Siminoff LA, Smith TJ. Physicians’ current practices and opportunities for DNA banking of dying patients with cancer. J Oncol Practice. 2011;7:183–187.
Nippert I, Julian-Reynier C, Harris H, et al. Cancer risk communication, predictive testing and management in France, Germany, the Netherlands and the UK: general practitioners’ and breast surgeons’ current practice and preferred practice responsibilities. J Community Genet. 2014;5:69–79.
Tanabe N, Shikama A, Bando H, Satoh T, Shimizu C. A survey of the practice patterns of gynecologic oncologists dealing with hereditary cancer patients in Japan. Fam Cancer. 2014;13:489–498.
Prolla CM, da Silva PS, Netto CB, Goldim JR, Ashton-Prolla P. Knowledge about breast cancer and hereditary breast cancer among nurses in a public hospital. Rev Lat Am Enfermagem. 2015;23:90–97.
Jacher JE, Martin LJ, Chung WK, Loyd JE, Nichols WC. Pulmonary arterial hypertension: specialists’ knowledge, practices, and attitudes of genetic counseling and genetic testing in the USA. Pulm Circ. 2017;7:372–383.
Gonthier C, Pelletier S, Gagnon P, et al. Issues related to family history of cancer at the end of life: a palliative care providers’ survey. Fam Cancer. 2018;17:303–307.
Loss J, Muller D, Weigl J, et al. Views of ophthalmologists on the genetics of age-related macular degeneration: results of a qualitative study. PLoS ONE. 2018;13:e0209328.
Jenkins S, Arribas-Ayllon M. Genetic counselling for psychiatric disorders: accounts of psychiatric health professionals in the United Kingdom. J Genet Couns. 2016;25:1243–1255.
Hoop JG, Roberts LW, Hammond KA, Cox NJ. Psychiatrists’ attitudes, knowledge, and experience regarding genetics: a preliminary study. Genet Med. 2008;10:439–449.
Batra S, Valdimarsdottir H, McGovern M, Itzkowitz S, Brown K. Awareness of genetic testing for colorectal cancer predisposition among specialists in gastroenterology. Am J Gastroenterol. 2002;97:729–733.
Metcalfe A, Pumphrey R, Clifford C. Hospice nurses and genetics: implications for end-of-life care. J Clin Nurs. 2010;19:192–207.
Prochniak CF, Martin LJ, Miller EM, Knapke SC. Barriers to and motivations for physician referral of patients to cancer genetics clinics. J Genet Couns. 2012;21:305–325.
Klitzman R, Abbate K, Chung WK, et al. Psychiatrists’ views of the genetic bases of mental disorders and behavioral traits and their use of genetic tests. J Nerv Ment Dis. 2014;202:530–538.
Salm M, Abbate K, Appelbaum P, et al. Use of genetic tests among neurologists and psychiatrists: knowledge, attitudes, behaviors, and needs for training. J Genet Couns. 2014;23:156–163.
Cox SM, Starzomski RC. Genes and geneticization? The social construction of autosomal dominant polycystic kidney disease. New Genet Soc. 2004;23:137–166.
Bonter K, Desjardins C, Currier N, Pun J, Ashbury FD. Personalised medicine in Canada: a survey of adoption and practice in oncology, cardiology and family medicine. BMJ Open. 2011;1:e000110.
Graves KD, Christopher J, Harrison TM, Peshkin BN, Isaacs C, Sheppard VB. Providers’ perceptions and practices regarding BRCA1/2 genetic counseling and testing in African American women. J Genet Couns. 2011;20:674–689.
Zhou YZ, Wilde A, Meiser B, Mitchell PB, Barlow-Stewart K, Schofield PR. Attitudes of medical genetics practitioners and psychiatrists toward communicating with patients about genetic risk for psychiatric disorders. Psychiatr Genet. 2014;24:94–101.
Eccles BK, Copson E, Maishman T, Abraham JE, Eccles DM. Understanding of BRCA VUS genetic results by breast cancer specialists. BMC Cancer. 2015;15:936.
Gray SW, Park ER, Najita J, et al. Oncologists’ and cancer patients’ views on whole-exome sequencing and incidental findings: results from the CanSeq study. Genet Med. 2016;18:1011–1019.
Parikh AR, Keating NL, Liu PH, et al. Oncologists’ selection of genetic and molecular testing in the evolving landscape of stage II colorectal cancer. J Oncol Pract. 2016;12:e308–19. 259
Kurian AW, Li Y, Hamilton AS, et al. Gaps in incorporating germline genetic testing into treatment decision-making for early-stage breast cancer. J Clin Oncol. 2017;35:2232–2239.
Choi MC, Lim MC, Lee M, et al. Practice patterns of hereditary ovarian cancer management in Korea. Int J Gynecol Cancer. 2017;27:895–899.
Culver JO, Hull JL, Dunne DF, Burke W. Oncologists’ opinions on genetic testing for breast and ovarian cancer. Genet Med. 2001;3:120–125.
Agnese DM, Hampel H, Farrar WB. Utilization of genetic counseling services by surgical oncologists: education a must. Clin Genet. 2006;70:524–525.
Klepek H, Nagaraja H, Goutman SA, Quick A, Kolb SJ, Roggenbuck J. Lack of consensus in ALS genetic testing practices and divergent views between ALS clinicians and patients. Amyotroph Lateral Scler Frontotemporal Degener. 2019;20:216–221.
van Langen IM, Birnie E, Schuurman E, et al. Preferences of cardiologists and clinical geneticists for the future organization of genetic care in hypertrophic cardiomyopathy: a survey. Clin Genet. 2005;68:360–368.
Burke S, Barker C, Marshall D. Developing education tailored to clinical roles: genetics education for haemophilia nurses. Nurse Educ Today. 2012;32:52–56.
Hallowell N, Wright S, Stirling D, Gourley C, Young O, Porteous M. Moving into the mainstream: healthcare professionals’ views of implementing treatment focussed genetic testing in breast cancer care. Fam Cancer. 2019;18:293–301.
Wright S, Porteous M, Stirling D, Young O, Gourley C, Hallowell N. Negotiating jurisdictional boundaries in response to new genetic possibilities in breast cancer care: the creation of an ‘oncogenetic taskscape’. Soc Sci Med. 2019;225:26–33.
Claybrook J, Hunter C, Wetherill LF, Vance GH. Referral patterns of Indiana oncologists for colorectal cancer genetic services. J Cancer Educ. 2010;25:92–95.
Vajda A, McLaughlin RL, Heverin M, et al. Genetic testing in ALS: a survey of current practices. Neurology. 2017;88:991–999.
Ferraro L, Pollard JR, Helbig I. Attitudes toward epilepsy genetics testing among adult and pediatric epileptologists—results of a Q-PULSE survey. Epilepsy Curr. 2016;16:46–47.
Murciano-Goroff YR, McCarthy AM, Bristol MN, et al. Uptake of BRCA 1/2 and oncotype DX testing by medical and surgical oncologists. Breast Cancer Res Treat. 2018;171:173–180.
Hoop JG, Roberts LW, Green Hammond KA, Cox NJ. Psychiatrists’ attitudes regarding genetic testing and patient safeguards: a preliminary study. Genetic Test. 2008;12:245–252.
Paller CJ, Antonarakis ES, Beer TM, et al. Germline genetic testing in advanced prostate cancer, practices and barriers: survey results from the germline genetics working group of the Prostate Cancer Clinical Trials Consortium. Clin Genitourin Cancer. 2019;17:275–282. e1
Grant RW, Hivert M, Pandiscio JC, Florez JC, Nathan DM, Meigs JB. The clinical application of genetic testing in type 2 diabetes: a patient and physician survey. Diabetologia. 2009;52:2299–2305.
Cohen PA, Nichols CB, Schofield L, Van Der Werf S, Pachter N. Impact of clinical genetics attendance at a gynecologic oncology tumor board on referrals for genetic counseling and BRCA mutation testing. Int J Gynecol Cancer. 2016;26:892–897.
Aday AW, Macrae CA. Genomic medicine in cardiovascular fellowship training. Circulation. 2017;136:345–346.
Dodson CH, Lewallen LP. Nursing students’ perceived knowledge and attitude towards genetics. Nurse Educ Today. 2011;31:333–339.
Choudhry NK, Fletcher RH, Soumerai SB. Systematic review: the relationship between clinical experience and quality of health care. Ann Intern Med. 2005;142:260–273.
Lalonde M, Hall LM, Price S, Andrews G, Harris A, MacDonald-Rencz S. Support and access for nursing continuing education in Canadian work environments. Nurs Leadersh (Tor Ont). 2013;26:51–60.
Kentwell M, Dow E, Antill Y, et al. Mainstreaming cancer genetics: A model integrating germline BRCA testing into routine ovarian cancer clinics. Gynecol Oncol. 2017;145:130–136.
Turner NC, Tutt ANJ. Platinum chemotherapy for BRCA1-related breast cancer: Do we need more evidence? Breast Cancer Res. 2012;14:115.
Meiser B, Halliday JL. What is the impact of genetic counselling in women at increased risk of developing hereditary breast cancer? A meta-analytic review.Soc Sci Med. 2002;54:1463–1470.
Shabani M, Bezuidenhout L, Borry P. Attitudes of research participants and the general public towards genomic data sharing: a systematic literature review. Expert Rev Mol Diagn. 2014;14:1053–1065.
Hindmarsh R, Abu-Bakar A. Balancing benefits of human genetic research against civic concerns: Essentially Yours and beyond—the case of Australia. Pers Med. 2007;4:497–505.
Jacobs C, White S, Phillips J. Genetics in palliative care: too much to ask? Int J Palliat Nurs. 2019;25:212–214.
Acknowledgements
This project is funded by a Translational Cancer Research Network PhD Scholarship Top-up Award, supported by the Cancer Institute NSW. S.W. is the recipient of a PhD stipend scholarship from the Translational Cancer Research Network (http://www.tcrn.unsw.edu.au/).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosure
The authors declare no conflicts of interest.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
About this article

Cite this article
White, S., Jacobs, C. & Phillips, J. Mainstreaming genetics and genomics: a systematic review of the barriers and facilitators for nurses and physicians in secondary and tertiary care. Genet Med 22, 1149–1155 (2020). https://doi.org/10.1038/s41436-020-0785-6
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41436-020-0785-6
Keywords
This article is cited by
-
A survey of genetic and palliative care health professionals’ views of integrating genetics into palliative care
European Journal of Human Genetics (2024)
-
Secondary use of genomic data: patients’ decisions at point of testing and perspectives to inform international data sharing
European Journal of Human Genetics (2024)
-
The implementation of large-scale genomic screening or diagnostic programmes: A rapid evidence review
European Journal of Human Genetics (2023)
-
Approaching discussions about genetics with palliative patients and their families: a qualitative exploration with genetic health professionals
European Journal of Human Genetics (2023)
-
Investigating genomic medicine practice and perceptions amongst Australian non-genetics physicians to inform education and implementation
npj Genomic Medicine (2023)
