
Abstract
Background
This paper examines the visuospatial working memory (WM) performance of children and adults born very preterm (VPT) and/or very low birth weight (VLBW) relative to their full-term (FT)-born peers. Of interest was the nature and severity of observed impairments, as well associations with educational/occupational functioning at each age point.
Methods
Participants were drawn from two prospective cohort studies: (1) a regional cohort of 110 VPT (<32 weeks’ gestation and <1500 g) and 113 FT born children assessed at age 12 years; (2) a national cohort of 229 VLBW (<1500 g) and 100 FT born adults assessed at age 28 years. Visuospatial WM was assessed using a four-span/difficulty-level computerized task.
Results
Both children and adults born VPT/VLBW had poorer visuospatial WM than FT controls, with their performance less accurate, slower (correct trials), and less efficient with increasing task difficulty (Cohen’s d = 0.27–0.51; p < 0.05). Adults had better visuospatial WM than children, but between-group differences were highly similar across ages, before and after adjustment for confounding social background and individual factors. Poorer WM was associated with lower levels of educational and occupational/socioeconomic achievement.
Conclusions
Visuospatial WM difficulties persist into adulthood raising concerns for the longer-term cognitive and adaptive functioning of VPT survivors.
Impact
-
Both children and adults born very preterm have poorer visuospatial working memory than their term-born peers. They are less accurate, take longer to respond correctly and are less efficient, with test performance declining with increasing cognitive demand.
-
Similar differences in visuospatial working memory are observed between VPT/VLBW and full-term individuals during both childhood and adulthood, with these differences remaining even after covariate adjustment.
-
Individuals with poorer visuospatial working memory have lower levels of educational achievement and occupational/socioeconomic success.
-
Visuospatial working memory difficulties persist into adulthood and appear to continue to impact everyday functioning and life-course opportunities.
Similar content being viewed by others

Introduction
Executive function impairments represent a significant neurocognitive challenge for children born very preterm (VPT: <32 weeks’ gestation) and/or very low birth weight (VLBW: <1500 g). A recent meta-analysis of 44 studies showed that between the ages of 4 and 17 years, VPT-born children perform about a half standard deviation (SD) below their term-born peers on standardized measures of executive function.1 A similar mean between-group difference (0.4–0.5 SD) was also reported in a meta-analysis of 4.5–15-year-old lower-risk children born preterm (<37 weeks’ gestation) or low birth weight (<2500 g).2
Visuospatial working memory (WM), or the ability to temporarily store and actively manipulate spatial information in the absence of direct sensory input, is a core executive function skill that is adversely impacted by preterm birth.3,4,5 This skill emerges in early childhood and develops across childhood and adolescence. It plays a vital role in a range of everyday tasks from following visual instructions and remembering an object’s location, to more demanding cognitive tasks such as planning, problem-solving, and mental arithmetic. Thus, not surprisingly, childhood visuospatial WM problems predict educational underachievement over and above intelligence (IQ)6,7,8 and are likely to have long-term impacts on engagement in tertiary and secondary education, employment, and income.9,10
Existing research examining the visuospatial WM abilities of VPT survivors, and to a large extent the general population, has primarily consisted of cross-sectional analyses of preschool and school-age samples, with a smaller number of similarly designed studies extending into late adolescence.11,12,13 Only a very small handful of studies have examined the visuospatial WM abilities of adults born VPT, with these almost exclusively involving cross-sectional analyses of groups in their early 20s.14,15,16 Test measures across studies have also generally varied by age and/or consisted of subtests from an IQ measure or larger executive function battery. For example, Aanes et al. found that at age 19–20 years, adults born VLBW obtained lower scores than term-born controls on the visual subtest (spatial span) of the WM Index from the Wechsler Memory Test.14 Similarly, data from a Finnish cohort reported that 23-year-old adults born early (<34 weeks’ gestation) and late (>34 weeks) preterm had similar neurocognitive functioning to their term-born peers, with the exception of visuospatial WM efficiency on the Groton Maze Learning Test.15 However, after covariate adjustment, performance impairments disappeared for the late but not early preterm group.
Results from these single age, cross-sectional assessments generally suggest that problems may be ongoing, but with effect sizes varying depending on the sample studied and/or measure/s used. They also offer little information about the kinds of performance difficulties experienced by individuals born VPT (i.e., accuracy, speed, or both), or perhaps even more critically, how these might vary under different cognitive load conditions. Even more importantly, these studies provide limited insights into how visuospatial WM skills vary with age in both VPT and typically developing individuals due to measurement differences across age assessments.
Given the importance of visuospatial WM for successful adult academic and vocational functioning, multiage and longer-term outcome studies are urgently needed to address this issue. That is, whether neurocognitive problems observed during childhood, such as impairments in visuospatial WM, persist into adulthood, or whether some aspects of functioning such as the speed of response might improve while other aspects do not (e.g., accuracy). Alternatively, as the above single outcome studies using different assessments imply, do these skills reflect an enduring deficit that will require continued adaptation and compensation over the lifespan? If difficulties reduce with age, one would expect to see fewer differences in the visuospatial WM performance of older individuals born VPT relative to their same-age term-born peers. However, if the latter deficit hypothesis was true, one would expect to observe relatively similar between-group differences in older and younger cohorts, or possibly even a larger between-group difference with increasing life demands.
To address these important issues, the aims of this study were as follows:
-
1.
To describe the visuospatial WM performance of two cohorts of VPT and/or VLBW survivors, one assessed in childhood (age 12) and one in adulthood (age 28) compared to their same age, typically developing term-born peers. At both ages, the same WM task was administered under identical conditions to obtain three measures of task performance across four cognitive load or difficulty levels. These included accuracy (% trials correct), mean reaction time on successful (accurate) trials, and speed-accuracy trade-off or performance efficiency (ratio of reaction time to accuracy).
-
2.
To examine the extent to which the visuospatial WM performance of VPT and/or VLBW survivors relative to term controls differed depending on the developmental timing of assessment, with a particular focus on whether visuospatial impairments observed in the child cohort were also observed in the adult cohort.
-
3.
To examine linkages between visuospatial WM performance and concurrent educational (both cohorts) and occupational functioning (adult cohort only).
Methods
Sample
Data were drawn from two well-characterized prospective cohort studies undertaken in New Zealand to longitudinally assess the longer-term neurodevelopmental outcomes of infants born VPT and/or VLBW. Uniquely, both studies administered the same assessment of visuospatial WM using the same procedures, test conditions and personnel, but at very different stages of the lifespan: late childhood (mean age 12.1; range: 11.6–12.8 years) and early adulthood (mean age 28.5; range: 26–30 years).
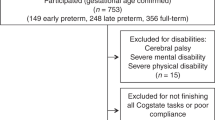
The younger sample consisted of a regional cohort of 110 VPT-born (<33 weeks’ gestation) infants recruited at birth (1998–2000, 92% recruitment) in Christchurch, New Zealand, and studied to mean corrected age 12 years alongside a comparison group of 113 term-born children matched for sex, birth date, and delivery hospital (38–41 weeks’ gestation, 62% recruitment at age 2 years). Of those who survived, 104 VPT (97% retention) and 109 term-born children (96% retention) were assessed at age 12 years. Within each group, there were no significant (p < 0.05) differences between those assessed and those not assessed at 12 years in terms of their neonatal and family social characteristics. Further details about this cohort are available in prior publications.4,17
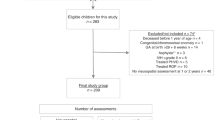
The older sample consisted of a national cohort of all VLBW (<1500 g) infants admitted to a New Zealand neonatal unit and who survived to discharge during 1986 (N = 338). Of those who survived, 229 were assessed at a mean age of 28.5 years with high retention (71%). This sample was studied alongside a comparison group of 100 healthy term-born individuals born in 1986 and recruited via peer nomination by a VLBW participant or through random sampling from the national electoral roll (n = 24), matching for sex, ethnicity, and regional distribution. Further details about this cohort are available in prior publications.18,19 Table 1 provides a descriptive profile of the clinical and family background characteristics of the two cohorts.
This research was completed in accordance with the Declaration of Helsinki. Study protocols were approved by the Upper South Regional Ethics Committee (URA/10/05/040—child cohort; URB/12/05/015—adult cohort). Informed, written consent was obtained from all adult participants and parents/guardians of all child participants.
Measures
Visuospatial WM
Children and adult’s visuospatial WM abilities were assessed using a novel computerized task adapted from the Sternberg spatial WM paradigm.20,21 It was developed using E-Prime (version 2.0) and administered on a keyboard computer setup in a dimly lit room. The task was presented as a detective game that required participants over multiple trials, to memorize, retain, and recall the spatial location of a set of visual objects or stimuli presented for a short retention interval. All stimuli were novel and presented as 1024 × 768-pixel images of familiar objects selected from the International Database of Affective Picture System. These were displayed at eye level on a 17.5-in. desktop screen (children) or 13.5-in. laptop screen (adults) approximately 60 cm parallel to the participant’s frontal plane, with a refresh rate of 59.402 Hz.
Before testing, all participants received comprehensive training using a training booklet covering all testing requirements. Feedback was provided until performance was 100% accurate. Then, a further 12 computer-based practice trials were administered with feedback before commencing testing. The overall task or trial set consisted of 48 test trials and an additional 12 neutral trials to ensure the alertness of the respondent over the session. Test trials varied in difficulty level from 1 to 4 depending on the number of visual objects the respondent was required to memorize and potentially recall. There were 12 trials per set size administered as four blocks, interspersed with rest breaks. Difficulty level and object congruence were randomized across trial blocks. At the beginning of each trial set, participants were reminded of task requirements and told to respond as quickly as possible without compromising accuracy.
The procedure for each test trial is illustrated in Fig. 1. As shown, each trial began with a fixation cross displayed at the center of the screen for a duration of 1000 ms to avoid or reduce potential visual aftereffects from the previous trial. After this time interval, the trial proper started with the presentation of a visual array of the novel but familiar stimuli or objects (crime scene). These were arranged in one of four quadrants on the screen or prime display, with the number of stimuli or objects varying from 1 to 4 depending on the difficulty level or set size. The participant was allowed to memorize these objects and their locations for 3000 ms, at which time another fixation cross appeared on the screen for 5000 ms. Following this delay, respondents were shown for 3000 ms, one of the objects from the original prime display positioned either in the same or different location. Respondents were asked to indicate, via a keypress, whether or not the previously seen object was still in the same spatial location as the prime display. That is, whether or not the crime scene had been tampered with and the object moved since the initial sighting. Unlike the practice session, no performance feedback was provided.

Schematic Illustration of the Stimulus Presentation for a Single Trial of the Sternberg-based visuospatial working memory task.
For each set size (1–4), task performance was assessed using three measures averaged across trials. These included the percentage of trials correct (accuracy), mean reaction time on successful (accurate) trials, and the speed-accuracy trade-off or performance efficiency (ratio of reaction time to accuracy) to compensate for incorrect and fast responses. These scores were computed as follows.
Data were processed in three stages after excluding missed responses (i.e., trials without a response for >3000 ms). First, the percentage of accurate responses was determined for each of the four set sizes or difficulty levels. Second, the mean reaction time of accurate responses for each set size was calculated. The reaction time of unsuccessful (inaccurate) responses was excluded as they were assumed to manifest through a distinct neurocognitive process. This approach ensured homogeneity of response measures and limited the potential risk of skewing the data due to a disproportionate rate of accurate to inaccurate responses. Furthermore, for each participant, trials with reaction times >3 SD of the mean reaction time across all valid trials were also excluded as potential erroneous responses. Third, the efficiency of visuospatial WM performance was determined by taking into consideration both the accuracy and speed of responses.
Concurrent educational achievement and occupational functioning
To examine the functional correlates of visuospatial WM abilities, measures of educational achievement and socioeconomic status (adulthood only) were identified for both cohorts. At age 12 years, educational achievement was assessed using the Broad Reading and Broad Math indices from the Woodcock Johnson-III Tests of Achievement (WJ-III; Woodcock, 2001 #198}. The WJ-III has good test–retest reliability (0.75–0.95) and correlates highly (r = 0.59–0.80) with other standardized educational measures. At age 28 years, educational achievement was recorded on a 5-point scale (0 = no formal qualifications; 1 = basic high school qualification; 2 = higher-level high school qualification; 3 = tertiary technical qualification below degree level; 5 = university degree or equivalent). Adult occupational status was assessed using the New Zealand Socioeconomic Index, with higher scores indicating higher socioeconomic status.22
Data analysis
Data analysis proceeded in four steps. First, differences between the two study cohorts were examined across a range of neonatal and social background factors to identify potential cohort effects arising from the different ages (and recruitment periods) of the two samples (see Tables 1 and 2). This was done using either the χ2 test of independence or t test for independent samples. Second, we compared at each age (12 and 28 years) the visuospatial WM performance of VPT/VLBW and term-born samples within a repeated-measures random-effects regression framework (see Table 3). Third, the joint associations between cohort age (child vs. adult), group (VPT/VLBW vs. term-born), and span difficulty (1–4 set size) and each of our visuospatial WM outcomes was modeled to summarize bivariate associations between participant age, preterm birth status, and increasing task span difficulty on our measures of visuospatial WM test performance. This model was then extended to include family background and individual variables that varied by cohort age and group (preterm birth) to assess the extent to which the effects of age, group, and task difficulty on visuospatial WM outcomes were independent of, or could be explained by, these confounding factors (see Table 4). These factors included family socioeconomic status, maternal age, maternal ethnicity, maternal education, sex, cerebral palsy, and vision problems. For this analysis, models were fitted to a combined data set, pooling the repeated-measures outcome data over cohorts and were of the general form: Yijk = β0k + β1k COHij + β2k GRPij + β3k (COHij × GRPij) + Σβjp Zijp + µi + εijk, where Yijk was the observed outcome (accuracy, reaction time, or efficiency) for the ith participant in the jth cohort at span difficulty level k (k = 1, …, 4); COHij was a dichotomous variable reflecting membership of the younger (age 12 years) cohort compared to the older cohort; GRPij was a dichotomous variable representing study group membership (VPT/VLBW vs. term-born); COHij × GRPij was the multiplicative interaction of cohort with study group; Zijp was the set of family background and individual characteristics for cohort j; µi was an individual specific random intercept and εijk a set of random disturbance terms.
To aid model interpretation, all predictors were scaled to have mean zero, and the models were parameterized to estimate intercepts (β0k); main effects of age cohort (β1k), study group (β2k), and cohort by study group interactions (β3k) that were specific to span difficulty level k (k = 1, …, 4). With the model parameterized in this way, the coefficients β0k can be interpreted as estimates of the covariate-adjusted mean test scores in the combined cohort sample at span difficulty level k (k = 1, …, 4); β1k as estimates of the adjusted mean differences in task performance between cohorts; and β2k as estimates of the adjusted mean differences in task performance between VPT/VLBW and term-born controls pooled over cohorts. The effects of the covariates (βjp) were permitted to vary between age cohorts.
Using the fitted model for each outcome, a series of Wald χ2 tests were then conducted to provide overall tests of main effects (age cohort, group, task span difficulty) and interactions. Separate Wald tests of the hypotheses that each set of parameters β1k, β2k, and β3k were jointly zero provided overall tests of the main effects of the age cohort, group status, and the interaction of cohort by group status, respectively. Similarly, separate Wald tests of the hypothesis that each set of parameters (β0k, β1k, β2k, and β3k) were equal at all span difficulty levels provided an overall test of the (a) main effect of span difficulty, (b) cohort by span difficulty interaction, (c) group status by span difficulty interaction, and the (d) three-way interaction of cohort by group status by span difficulty.
The final step in our analysis involved examining, for each group as well as the total sample, associations between respondents’ mean overall WM inverse efficiency score and their concurrent educational/socioeconomic functioning on age-appropriate measures. This was done using regression methods with tests for linear trend (see Table 5).
Results
Sample characteristics and differences between the child and adult cohorts
As shown in Table 1, across both age cohorts, similar differences were observed between VPT/VLBW and term-born comparison groups on measures of gestational age at birth, birth weight, sex, maternal age, and maternal educational underachievement. Rates of sepsis were also similar across the two VPT cohorts. However, despite these similar relative differences, there was some suggestion that individuals born VPT in 1998–2000 and assessed at age 12 years were subject to higher neonatal medical and social risk than those born in 1986 and assessed at age 28 years. Closer examination of the two VPT/VLBW cohorts tended to confirm this. As shown in Table 2, the younger VPT cohort was on average born earlier, weighed less, and had higher rates of chronic lung disease (supplementary oxygen at 36 weeks) than the older cohort. There was also some suggestion that the younger cohort was subject to higher rates of brain injury, but this very likely reflects, at least in part, better detection due to advances in routine cranial ultrasound. In contrast, the older cohort was less likely to have experienced the protective benefits of antenatal corticosteroids and had higher rates of growth restriction. Finally, across both cohorts, VPT/VLBW individuals had higher rates of cerebral palsy and lower IQ scores than term-born controls at ages 12 and 28 years (see Table 1). Notably, mean differences in IQ scores across the two age assessments were very similar (mean difference = 9 at age 12 years vs. mean difference = 10 at age 28 years).
Visuospatial WM performance of the younger and older cohorts
To describe the performance profile of children and adults on our visuospatial WM task, Table 3 compares the performance of VPT/VLBW individuals at ages 12 and 28 years relative to their same-age, typically developing, term-born peers. Between-group differences and variations in task performance were examined across the 4 span or difficulty levels ranging from 1 (easiest) to 4 (most difficult). These included: accuracy (% trials correct); reaction time or response speed on accurate trials (ms); and performance efficiency, i.e., ratio of reaction time to accuracy (ms). Visuospatial WM data were available for 98/104 VPT and 106/109 term-born children at age 12 years and 212/229 VLBW and 100/100 term-born adults at age 28 years. Reasons for data loss in the child cohort included blindness (1 VPT), failed practice trials (3 VPT of which 2 were severely delayed, 1 term), refusal (1 VPT, 1 term), and unknown (1 VPT, 1 term). For the adult cohort, these included blindness (n = 3), inadequate vision (n = 1), incomplete (n = 1), failed practice trials (n = 1), and not administered due to fatigue, time constraints, or unspecified reasons (n = 11).
As shown in Table 3, with respect to task accuracy at age 12 years, when the task or cognitive load was easiest (span level 1), both groups obtained a similar proportion of trials correct. However, as span level or task difficulty/cognitive load increased, both groups showed declines in accuracy, with this decline more marked for children in the VPT group. Alongside this decrement in accuracy with increasing task demand, VPT-born children also took significantly longer to respond accurately and were less efficient in their responses than term-born children, further suggesting that their performance was impacted to a larger degree by task difficulty.
A very similar pattern of results was evident in the older adult cohort at age 28 years across all three outcome measures and the four task span levels. Specifically, between-group differences were similar despite both VLBW and control adults generally performing better than their younger counterparts on the task, including being more accurate, quicker, and more efficient in their task performance. These results suggest a consistent performance profile decrement for VPT/VLBW individuals relative to term controls in both childhood and adulthood.
Effects of preterm birth and age on visuospatial WM performance after adjustment for the effects of confounding factors
To test the veracity of these observations, and to take account of potential cohort differences and confounding factors associated with preterm birth, the data reported in Table 3 were reanalyzed using mixed-effects regression methods to adjust observed differences for childhood family background (family socioeconomic status, maternal age, maternal education, and ethnicity) and individual-level (sex, cerebral palsy, and vision impairment) factors as described in the “Methods.”
Table 4 summarizes the key model parameters and tests of significance for each outcome. Examination of this table shows:
-
1.
For all outcomes, there was a statistically significant (p < 0.001) main effect of span difficulty level, indicating that overall test performance decreased with increasing span difficulty. In the combined sample adjusting for confounding: accuracy declined from a mean of 96.6% at difficulty level 1 to 86.8% at difficulty level 4; mean reaction time increased from 1077 to 1590 ms; and relative efficiency declined from a mean of 1131 to 1919 ms over the same interval.
-
2.
The cohort parameters can be interpreted as the mean difference in test performance in the child cohort compared to the adult cohort at each level of span difficulty. For all outcomes, there was a statistically significant (p < 0.001) overall main effect of cohort and a significant (p < 0.001) cohort by span difficulty interaction, reflecting the facts that (a) the WM performance of the child cohort was consistently lower than in the adult cohort and b) the differences in test performance varied with span difficulty. After adjustment, mean accuracy in the child cohort was 5.2% lower at span difficulty level 1, with this difference increasing to 10.2% at difficulty level 4. Conversely, the difference in mean reaction times was greatest at the easiest difficulty level (187 ms) and declined to a mean difference of 55 ms at level 4. The net effects of these two trends were reflected in the differences in mean efficiency, which were at their greatest at the intermediate difficulty levels 2 and 3. The adjusted between-cohort differences in test performance were negligibly different from the observed differences (data not shown), suggesting that the better performance of the adult cohort was not explained by prior family or individual context.
-
3.
The study group parameters can be interpreted as the mean difference in test performance among the VPT/VLBW compared to term-born controls in the combined sample (pooled over cohorts) at each level of span difficulty. For all outcomes, there was a statistically significant main effect of group status (p < 0.05), reflecting poorer overall test performance in the VPT/VLBW group. For two outcomes (accuracy, efficiency), there was also a significant (p < 0.05) study group by span difficulty interaction, reflecting the fact that for these outcomes the relative performance of VPT/VLBW declined with increasing span difficulty. After adjustment, the mean difference in accuracy was negligible at difficulty level 1 (0.4%), but increased to a decrement of 3% at difficulty level 4; and relative efficiency declined from a mean difference of 69 to 189 ms over the same span interval. In general, the adjusted differences in visuospatial WM performance in VPT/VLBW compared to controls were substantially smaller than the corresponding differences in performance between the younger and older cohorts.
-
4.
For all outcomes, there was no evidence of either a cohort by study group interaction or a three-way cohort by study group by span difficulty interaction. This suggests that the covariate-adjusted decrements in test performance among VPT/VLBW compared to controls were similar in both child and adult cohorts, and did not vary systematically with cohort and span difficulty levels.
A further supplementary analysis was done to estimate possible effect size differences between VPT/VLBW and the term-born comparison group for each cohort separately. Results showed that adjustment for family background and individual characteristics had a greater impact on explaining the observed differences in visuospatial WM performance in the child cohort than in the adult cohort. Prior to adjustment the effect size differences (Cohen’s d, see Table 3) in accuracy between VPT and term-born in the child cohort ranged from 0.11 to 0.39; after adjustment, these reduced to 0.03–0.28. By comparison, the corresponding effect sizes for accuracy between VLBW and term-born controls in the adult cohort ranged from 0.03 to 0.32 (unadjusted) reducing to 0.06–0.29 (adjusted). Similarly, effect size differences for efficiency in the child cohort reduced from 0.34 to 0.51 to a range of 0.12–0.34 after adjustment. By comparison, the effect size differences in the adult cohort remained stable: unadjusted 0.31–0.36 and adjusted 0.29–0.34. In general, the adjusted associations were in the modest to small effect size range for both cohorts.
Associations between visuospatial WM and concurrent functioning
Finally, Table 5 shows at each age assessment, associations between participants’ overall mean inverse efficiency scores on the WM task and their concurrent educational achievement, and in addition for the adult cohort, occupational/socioeconomic functioning. With the exception of occupational status in the adult full-term (FT)-born group (p = 0.20), results show clear linear associations between visuospatial WM performance and concurrent educational/occupational functioning, with those obtaining poorer WM scores having poorer educational and occupational outcomes.
Discussion
This study is novel in characterizing the visuospatial WM performance of two cohorts of prematurely born individuals at two important developmental time points, in late childhood and early adulthood. It also advances previous research by employing a common measure of visuospatial WM that could effectively be administered over approximately 16 years of development. Further, in contrast to earlier single outcome variable studies, our assessment based on the well-established Sternberg paradigm allowed us to cross-sectionally examine multiple indices of task performance (accuracy, response time, and efficiency) at two different stages of the life course due to the task inclusion of a range of difficulty levels. This is important but also highly relevant since in everyday life it is often not just a question of whether or not an individual can perform a task, but whether they can do so in an accurate, timely and efficient manner, especially under more challenging conditions such as when time or safety constraints exist.
Across both the younger and older cohorts, the same profile of visuospatial WM functioning was evident for individuals born VPT/VLBW. Their performance was characterized by lower levels of accuracy, longer reaction times for accurate responses, and poorer efficiency relative to their same-age term-born peers, suggesting pervasive and persistent WM impairments associated with being born VPT or VLBW. Moreover, it is noteworthy that when the task or cognitive load was easiest (span level 1), both preterm groups performed similarly to term-born controls. However, as task cognitive load increased, decrements in performance became more marked for VPT than term-born individuals. This is consistent with studies examining the attentional abilities of VPT survivors during childhood, which show that differences between VPT and term-born individuals increase at higher levels of cognitive demand.23 These findings suggest that VPT individuals may experience greater difficulty, tire more easily, and struggle to focus/attend to a task when executive function demand or cognitive load is high.
Examination of the effects of cohort age on visuospatial WM performance of VPT and term-born individuals showed that between-group differences were very similar in both the child and adult cohorts, despite observed age-related gains in visuospatial WM for both adult groups relative to comparable child groups. These results suggest that visuospatial WM impairments associated with VPT birth persist into adulthood and continue to pose challenges, rather than resolving with age and neurological maturation. This is consistent with results from the Stockholm Neonatal Project, which examined the development of visuospatial WM abilities from 5.5 to 18 years in a cohort of 115 VPT and 94 term-born individuals.24 At age 5.5 years, visuospatial WM was assessed using the total correct trials on the Knox Cubes task, and at age 18 years, the Corsi Blocks from the WAIS. Similar to our results, using a latent variable approach over this earlier developmental period they found clear between-group differences in visuospatial WM, with considerable across age/time stability in overall performance (r = 0.77). WM at age 5.5 years mediated WM outcome at age 18 years. Relatedly, longitudinal data from the Victorian Infant Collaborative Study has also shown that verbal WM impairments were largely stable from 7 to 18 years in a cohort of extremely preterm and/or extremely low birth weight individuals.25 More generally, these results also correspond with previous general cognitive data suggesting that VPT/VLBW-born individuals do not appear to fully compensate for or catch-up cognitively with their term-born peers.26,27 These findings, in combination with the current study, which extends well into adulthood, tend to suggest that visuospatial WM difficulties associated with preterm birth may best be viewed as a persistent and chronic impairment.
Furthermore, in support of the importance of visuospatial WM skills for everyday functioning, results showed that for both VPT/VLBW and FT-born children and adults, poorer WM abilities were associated with lower levels of educational achievement, and for VPT-born adults, poorer occupational/socioeconomic status. This is in agreement with general population studies highlighting the importance of WM for educational and occupational success and emphasizes the need to monitor and support the development of this executive function skill during early and middle childhood.
However, on a positive note, as shown by our effect sizes, these skill deficits are modest, suggesting that they may be highly amenable to improvement through appropriate intervention/prevention efforts as well as environmental/social supports when executive demands are high. They also suggest that ongoing mindfulness around the possible need for new or adapted strategies may be helpful as VPT-born individuals take on new roles and responsibilities in adulthood. This may vary depending on individual needs and personal circumstances, but is likely to be especially important in situations where safety is an issue or during high-risk adult activities such as driving and operating dangerous equipment. It also reinforces the importance of putting in place environmental strategies in the home and workplace to help optimize individual performance and safety when visuospatial WM demands of an activity are high.
While investigating the developmental mechanisms underlying poorer visuospatial WM outcomes following preterm birth was outside the scope of this study, our findings do suggest that neurosensory difficulties and childhood social risk exposure contributed in part to later observed difficulties. Although being born VPT/VLBW remained an independent, albeit modest, predictor of later visuospatial WM problems in both childhood and adulthood. They also potentially lend support to a neurological basis for the executive function difficulties associated with VPT birth. Structural magnetic resonance imaging findings from the current child and adult cohorts,19,23 as well as those of others,28 provide converging evidence of alterations in brain networks pertinent to executive function and in particular WM from early childhood to adulthood. In addition, longitudinal neuroimaging data increasingly suggest that despite gains in brain maturation indices over time, subsequent brain growth and development is unable to fully compensate for early neuroanatomical alterations associated with preterm birth.
This study had several methodological strengths, including (1) the regionally and nationally representative cohorts of VPT individuals, (2) our high recruitment and retention rates across both cohorts, (3) the inclusion of age- and sex-matched term-born comparison groups, (4) the same administrator and testing conditions across assessments, (5) the use of a single visuospatial WM assessment measure which permitted direct comparison of children and adult’s performance on a common set of identical parameters, (6) our novel neurocognitive task purposefully designed according to the well-established Sternberg paradigm, to collect cognitive load-sensitive data on the quality of visuospatial WM performance in high-risk and typically developing samples, and (7) covariate adjustment for family social background and individual factors that might account for observed between-group and age effects. The latter was important given the limitation of using two different age cohorts recruited from the same general population rather than conducting a longitudinal analysis of the same individual’s performance across a 16-year interval using the same measure. However, the latter longitudinal approach would not be without major challenges and potential limitations, including sample retention, staffing changes, and measurement/technological changes. Nonetheless, to understand as best we could possible cohort differences that might influence our study results, we examined the neonatal, social background, and neurodevelopmental profiles of each VPT cohort relative to a contemporary term-born control group. This analysis revealed greater immaturity and medical acuity consistent with international data,29,30 as well as greater family social risk in the younger 1998–2000 cohort than the older 1986 cohort. Given known links between these risk factors and poorer neurodevelopmental outcomes, this would be expected to have biased findings towards fewer between-group differences and smaller effect sizes in the adult cohort compared to the child cohort. However, this was not the case. In further support of the veracity of study findings, the mean IQ score differences between VPT and contemporary controls were almost identical in both age cohorts, further confirming our and others observations of persistent neurocognitive impacts of prematurity into adulthood.26,27 Nonetheless, further replication using prospective intraindividual longitudinal analytic approaches, with repeated measurements (>2) over time, will be important in confirming the present findings and further advancing our understanding of the development of visuospatial WM from childhood to adulthood in both high-risk and typically developing populations.
In conclusion, the current findings lend support to the notion that observed difficulties in visuospatial WM common among very preterm born survivors may reflect an enduring neurocognitive deficit rather than a maturational or developmental lag. Regardless of the underlying etiological mechanisms, this is concerning because of potential impacts on educational, social, and occupational functioning, as well as everyday life activities such as driving. Further longitudinal research is warranted to fully characterize the longer-term developmental trajectory of this important neurocognitive skill and to assess the effects of normal aging processes on the cognitive and neurological functioning of this already high-risk population. Also, of interest is whether verbal WM and other executive function difficulties that are commonly observed in children born VPT show a similar pattern of development over the transition from childhood to adulthood.
References
Brydges, C. R. et al. Cognitive outcomes in children and adolescents born very preterm: a meta-analysis. Dev. Med. Child Neurol. 60, 452–468 (2018).
van Houdt, C. A., Oosterlaan, J., van Wassenaer-Leemhuis, A. G., van Kaam, A. H. & Aarnoudse-Moens, C. S. Executive function deficits in children born preterm or at low birthweight: a meta-analysis. Dev. Med. Child Neurol. 9, 1015–1024 (2019).
Aarnoudse-Moens, C. S., Smidts, D. P., Oosterlaan, J., Duivenvoorden, H. J. & Weisglas-Kuperus, N. Executive function in very preterm children at early school age. J. Abnorm. Child Psychol. 37, 981–993 (2009).
Woodward, L. J., Edgin, J. O., Thompson, D. & Inder, T. E. Object working memory deficits predicted by early brain injury and development in the preterm infant. Brain 128, 2578–2587 (2005).
Fitzpatrick, A., Carter, J. & Quigley, M. A. Association of gestational age with verbal ability and spatial working memory at age 11. Pediatrics 138, e20160578 (2016).
Clark, C. A., Pritchard, V. E. & Woodward, L. J. Preschool executive functioning abilities predict early mathematics achievement. Dev. Psychol. 46, 1176–1191 (2010).
Simms, V. et al. Nature and origins of mathematics difficulties in very preterm children: a different etiology than developmental dyscalculia. Pediatr. Res. 77, 389–395 (2015).
Clark, C. A. & Woodward, L. J. Neonatal cerebral abnormalities and later verbal and visuospatial working memory abilities of children born very preterm. Dev. Neuropsychol. 35, 622–642 (2010).
Moffitt, T. E. et al. A gradient of childhood self-control predicts health, wealth, and public safety. Proc. Natl Acad. Sci. USA 108, 2693–2698 (2011).
Dodgeon, B., Patalay, P., Ploubidis, G. B. & Wiggins, R. D. Exploring the role of early-life circumstances, abilities and achievements on well-being at age 50 years: evidence from the 1958 British birth cohort study. BMJ Open 10, e031416 (2020).
Luu, T. M., Ment, L., Allan, W., Schneider, K. & Vohr, B. R. Executive and memory function in adolescents born very preterm. Pediatrics 127, e639–e646 (2011).
Lundequist, A., Bohm, B., Lagercrantz, H., Forssberg, H. & Smedler, A. C. Cognitive outcome varies in adolescents born preterm, depending on gestational age, intrauterine growth and neonatal complications. Acta Paediatr. 104, 292–299 (2015).
Schneider, L. A. et al. Cognitive abilities in preterm and term-born adolescents. J. Pediatr. 165, 170–177 (2014).
Aanes, S., Bjuland, K. J., Skranes, J. & Lohaugen, G. C. Memory function and hippocampal volumes in preterm born very-low-birth-weight (VLBW) young adults. Neuroimage 105, 76–83 (2015).
Suikkanen, J. et al. Reaction times, learning, and executive functioning in adults born preterm. Pediatr. Res. 89, 198–204 (2021).
Pyhälä, R. et al. Self-reported mental health problems among adults born preterm: a meta-analysis. Pediatrics 139, e20162690 (2017).
Woodward, L. J. et al. Very preterm children show impairments across multiple neurodevelopmental domains by age 4 years. Arch. Dis. Child Fetal Neonatal Ed. 94, F339–F344 (2009).
Darlow, B. A. et al. The New Zealand 1986 very low birth weight cohort as young adults: mapping the road ahead. BMC Pediatr. 15, 90 (2015).
Pascoe, M. J., Melzer, T. R., Horwood, L. J., Woodward, L. J. & Darlow, B. A. Altered grey matter volume, perfusion and white matter integrity in very low birthweight adults. Neuroimage Clin. 22, 101780 (2019).
Sternberg, S. High-speed scanning in human memory. Science 153, 652–654 (1966).
Sternberg, S. In defence of high-speed memory scanning. Q. J. Exp. Psychol. 69, 2020–2075 (2016).
Milne, B. J., Byun, U. & Lee, A. New Zealand Socio-Economic Index (Statistics New Zealand, 2006).
Lean, R. E., Melzer, T. R., Bora, S., Watts, R. & Woodward, L. J. Attention and regional gray matter development in very preterm children at age 12 years. J. Int Neuropsychol. Soc. 23, 539–550 (2017).
Stalnacke, J., Lundequist, A., Bohm, B., Forssberg, H. & Smedler, A. C. A longitudinal model of executive function development from birth through adolescence in children born very or extremely preterm. Child Neuropsychol. 25, 318–335 (2019).
Burnett, A. C. et al. Executive function in adolescents born <1000 g or <28 weeks: a prospective cohort study. Pediatrics 135, e826–e834 (2015).
Mangin, K. S., Horwood, L. J. & Woodward, L. J. Cognitive development trajectories of very preterm and typically developing children. Child Dev. 88, 282–298 (2017).
Darlow, B. A., Woodward, L. J., Levin, K. J., Melzer, T. & Horwood, L. J. Perinatal and childhood predictors of general cognitive outcome at 28 years in a very-low-birthweight national cohort. Dev. Med. Child Neurol. 62, 1423–1428 (2020).
Nosarti, C. & Froudist-Walsh, S. Alterations in development of hippocampal and cortical memory mechanisms following very preterm birth. Dev. Med. Child Neurol. 58(Suppl. 4), 35–45 (2016).
Cheong, J. L. Y. et al. Changing neurodevelopment at 8 years in children born extremely preterm since the 1990s. Pediatrics 139, e20164086 (2017).
Stoll, B. J. et al. Trends in care practices, morbidity, and mortality of extremely preterm neonates, 1993-2012. JAMA 314, 1039–1051 (2015).
Funding
This work was supported by grants from the Health Research Council of New Zealand (11-283; 12-129) and Cure Kids (CHRF 5040; CHRF 5041) to B.A.D., L.J.H., and L.J.W., and a Mater Foundation Principal Research Fellowship to S.B. The funding sources had no role in the writing of the manuscript or in the decision to submit it for publication. The authors have no financial relationships relevant to this work to disclose.
Author information
Authors and Affiliations
Contributions
Substantial contributions to conception and design: B.A.D., L.J.H., and L.J.W.; acquisition of data: L.J.H. and B.A.D.; analysis: L.J.H. and S.B.; interpretation of data: all authors). Drafting the article or revising it critically for important intellectual content: L.J.W. with L.J.H., B.A.D., and S.B. Final approval of the version to be published: all authors.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Woodward, L.J., Horwood, L.J., Darlow, B.A. et al. Visuospatial working memory of children and adults born very preterm and/or very low birth weight. Pediatr Res 91, 1436–1444 (2022). https://doi.org/10.1038/s41390-021-01869-w
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41390-021-01869-w
This article is cited by
-
Novel metrics to characterize temporal lobe of very preterm infants on term-equivalent brain MRI
Pediatric Research (2023)
-
Advocacy for research starting early in the life course
Pediatric Research (2022)
