
Abstract
Oxygen is one of the most critical components of life. Nature has taken billions of years to develop optimal atmospheric oxygen concentrations for human life, evolving from very low, peaking at 30% before reaching 20.95%. There is now increased understanding of the potential toxicity of both too much and too little oxygen, especially for preterm and asphyxiated infants and of the potential and lifelong impact of oxygen exposure, even for a few minutes after birth. In this review, we discuss the contribution of knowledge gleaned from basic science studies and their implication in the care and outcomes of the human infant within the first few minutes of life and afterwards. We emphasize current knowledge gaps and research that is needed to answer a problem that has taken Nature a considerably longer time to resolve.
Similar content being viewed by others
Introduction
Today, one-fifth (20.95%) of the Earth’s atmosphere consists of oxygen, but this has not always been so. During the Great Oxygenation Event (GOE) approximately 2.3 billion years ago, a rapid increase from low atmospheric oxygen occurred, resulting in oxygen levels that at some stage were probably as high as 30% (Fig. 1). This phenomenon most likely explained the great size of organisms from that era where fossils of insects with wingspans as large as 2 m have been found.1,2

The great oxygenation event and endosymbiosis. The presence of low oxygen levels and greenhouse gases such as methane (CH4) increased planetary heat. Photosynthesis led to increasing oxygen levels following the “great oxygenation event” 2.3 billion years ago. Increased oxygen led to removal of methane, reduction of greenhouse gases and planetary cooling. Irradiation and oxidative stress both lead to free radical formation. Primitive cells engulfed aerobic bacteria and cyanobacteria leading to the formation of the “modern” eukaryotic cell with mitochondria and chloroplasts by a mechanism called endosymbiosis (see text for details)
Life, however, evolved within an oxygen-poor atmosphere before the GOE. Oxygen was primarily produced by photosynthesis as a waste product by prokaryotic (and later, eukaryotic) organisms 3.5 billion years ago and by oceanic cyanobacteria a billion years after this.3,4,5 Primitive bacteria then merged with eukaryotes and became organelles (chloroplasts and mitochondria, respectively), which provided cells with energy. These organelles eventually lost their ability to live independently outside cells, in a process called endosymbiosis. Photosynthesis by cyanobacteria soon led to the eventual accumulation of atmospheric oxygen, which oxidized methane, a strong greenhouse gas, to carbon dioxide and water which then reduced the greenhouse effect with subsequent planetary cooling.6,7,8
Higher atmospheric oxygen levels not only cooled the planet but also provided biological diversification.9 Achieving the perfect balance between protection and lethality is a delicate process. It has taken Nature billions of years to reach the present (and probably) optimal atmospheric oxygen levels for human life, and, therefore, it is perhaps understandable that neonatology and modern medicine have not had the time to catch up with this need, especially in the case of preterm and asphyxiated newborn infants, who are physiologically unstable and who only a few decades ago were at extremely high chance of death.
In 1954, Gerschman et al.10 described what had been known by Nature for billions of years: that injury from irradiation and oxygen is both mediated via the same mechanisms (free radicals) and that protection is conferred also by identical means. This led to a better understanding of how humans, especially newborn infants, are injured by oxygen. In the 1980s, a new dimension in the understanding of the ill effects of oxygen was established, where it was shown that oxidative stress was caused not only by hyperoxia but also by factors related to oxidative defense, including inflammation.11,12,13
This contributed to a renewed interest in oxygen management of newborn infants. Valuable observational studies regarding associations between adverse clinical sequel and oxygenation, particularly in premature infants, were published around the turn of the century.14,15,16 It also rapidly became clear that randomized controlled trials (RCTs) were needed to find the right balance between too much and too little oxygen.17,18,19 In the 1990s, the first delivery room studies showed that term or near-term infants could be given respiratory support with air as well as oxygen.20,21 This practice was found to be associated with a 30% decrease in the risk of early death22 and led to major changes in recommendations for oxygen delivery at birth.23,24,25 Similar studies were then conducted in premature infants with pulmonary immaturity26,27,28,29,30,31,32,33,34,35,36 with parallel examination of the impact of hyperoxia and oxidative stress in non-human subjects.37,38,39,40
Currently, we know that evidence is still lacking regarding the optimum amount of oxygenation required for newborn infants, especially those who are premature or asphyxiated, who may need supplemental oxygen but at the same time are poorly equipped to deal with oxidative stress. We recognize that sufficiently large, well-designed RCTs are required to answer the question of best oxygen strategies in newborn infants. There is a need to incorporate individualized medicine into the equation, to recognize that oxygen exposure could create long-lasting and even inter-generational epigenetic changes. There has been a frantic exchange of information between experimental and preclinical studies with human application and today we know more about how genes and pathways are affected by hypoxia as well as hyperoxia. These studies now lead to one major question: can basic science studies contribute to improving our practice of providing best oxygenation for newborn infants and can we ever reach a satisfactory understanding of this very important process?
Oxygen toxicity
Oxygen was discovered independently by Carl Wilhelm Scheele in 1772 and by Joseph Priestley in 1774. The name oxygene (acid former) was coined by Antoine Lavoisier in 1777, but it seemed clear that the Polish alchemist, Michael Sendivogius, had already described the element as arial nitrate from as early as 1604.1 Priestly quickly realized the toxicity of oxygen. Di-oxygen has four unpaired electrons in its outer shell that spin in opposite directions giving O2 its paramagnetic and reactive properties, slowing the establishment of covalent bonds.
Oxygen’s role in energy metabolism is to be an electron acceptor in the respiratory chain. By accepting four electrons, oxygen is reduced to water, but a small part of the oxygen requires not one but four steps for this process to be complete. Each intermediate step occurs within the mitochondria and generates reactive oxygen species (ROS), including superoxide radical (O2−), hydrogen peroxide (H2O2), and the hydroxyl radical (OH). Superoxide and hydroxyl radicals are free radicals and therefore highly toxic and have the capacity to destroy cell membranes by lipid peroxidation, structural and enzymatic proteins, and DNA oxidation. Free radicals may interfere with protein folding and unfolding leading to abnormal function or structure.41 In the presence of transition metals (copper, iron, zinc, manganese, selenium), the reactivity of oxygen to capture electrons from other molecules gets enormously enhanced. The Haber–Weiss reaction for instance generates hydroxyl radicals from hydrogen peroxide and superoxide. The reaction is slow but is catalyzed by iron.41
Hydrogen peroxide is, however, not a free radical and acts as a signaling molecule essential for cell cross-talk (e.g., regulating blood flow within the ductus arteriosus and the pulmonary circulation).42,43,44
There are several reasons that newborn infants, especially those born preterm, are at risk of oxidative stress. First, relative oxidative stress is generally high within the first weeks of birth after transitioning from the low oxygen environment of the uterus to air. Sick newborns may need supplemental oxygen if there is respiratory insufficiency. The addition of asphyxia as well as free iron increases the risk of oxidative stress as described above.45,46 Most importantly, preterm infants do not have sufficient antioxidant defense, either de novo or passively acquired from the mother, until the third trimester, which increases susceptibility to oxidative stress.47,48 Current lung protective strategies, such as antenatal steroids, only have minor influence on the maturation of the antioxidant defense system.49
Oxygen sensing
The carotid bodies. Precise co-ordination of oxygen supply with demand is essential to meet the needs of metabolism. In the 1920s, the carotid bodies, located at the bifurcation of the common carotid artery, were identified as the organs responsible for the sensing of arterial blood oxygen levels.50 Hypoxemia induces stimulation of breathing due to a chemosensory reflex arising from the carotid body. This process is fast (<1 s) and is assumed to involve change to existing proteins rather than de novo synthesis. Hypoxic sensing appears to utilize two gaseous messengers: carbon monoxide (CO) and hydrogen sulfide (H2S). CO is generated by heme oxygenase 2, which is constitutively expressed in a number of tissues as the brain and the carotid body and suppresses carotid body sensory activity.50,51 H2S varies inversely with the oxygenation status of the carotid body such that hypoxia causes a rise in intracellular H2S.52 H2S may have several actions but also inhibits Ca2+-activated K+ channel conductance within the glomus cells of the carotid body, consequently inhibiting excitatory neurotransmitter release and preventing stimulation of afferent nerve endings (which would increase activity of the carotid sinus nerve).53
Hypoxia-inducible factor. Many different molecular mechanisms are utilized to maintain oxygen homeostasis. One of the most important ones is hypoxia-inducible factor (HIF), the master regulator of oxygen homeostasis at the transcriptional level (Fig. 2). Today it is known that more than 2500 target genes are activated by HIF.54,55,56 Within any given cell, HIF activates promoters in the region of hypoxia-responsive elements (HREs) and increases the expression of hundreds of messenger RNAs and decreases the expression of a similar number. These molecular mechanisms lead to either an increase in oxygen delivery or a decrease in oxygen consumption. Under normoxic conditions, HIF-1α is rapidly degraded by hydroxylation of a family of prolyl-4-hydroxylase (PHD) enzymes. The hydroxylated prolines are then recognized by the Von Hippel-Lindau/E3 ubiquitin ligase complex, which targets HIF-1α for proteasomal degradation. This system is sensitive to oxygen. Following as little as 5 min of reoxygenation, most stabilized HIF-1α is degraded. During oxygen deprivation, mitochondria increase their production of ROS. Serving as signaling molecules these ROS then inhibit hydroxylation of HIF-1α, preventing proteasomal degradation.55,56,57

The role of hypoxia-inducible factor (HIF) in normal lung development—alveologenesis and angiogenesis. During fetal period, relative low levels of oxygen promote lung development. Following preterm delivery, “normoxia” or hyperoxia can lead to degradation of HIF, poor alveolarization and vascular pruning. ROS: reactive oxygen species, HRE: hypoxia-responsive element, PHD: prolyl-4-hydroxylase enzyme, VEGF: vascular endothelial growth factor, BPD: bronchopulmonary dysplasia. Please see text for details
HIF regulates erythropoiesis by activating transcription of erythropoietin.58 Other examples of HIF-induced action are regulation of angiogenesis via HIF-dependent production of angiogenic cytokines and growth factors such as vascular endothelial growth factor as well as regulation of angiopoietins, placental growth factor, and platelet-derived growth factor B. These responses are slow, occurring over days to weeks. In contrast, responses designed to reduce oxygen consumption are rapid: occurring over hours to days, mediated through the switch from oxidative to glycolytic metabolism. HIF-1 controls expression of multiple genes that mediate this metabolic switch via several mechanisms. One is gene activation of the LDHA gene encoding lactate dehydrogenase, which converts pyruvate to lactate. HIF-1 also mediates an increased efficiency of electron transfer, and processes that trigger mitochondrial autophagy in this way reducing cellular oxidation of both glucose and fatty acids.59
A fundamental physiological response to hypoxia is cell cycle arrest, which necessitates HIF-1α.60 Cyclin-dependent kinase 2 (CDK2), active in the cell cycle from late G1 through S phase and G2 binds to HIF-1α and triggers lysosomal degradation. CDK1, active from late G2 through M phase, binds to HIF-1α and protects it from lysosomal degradation, thus controlling HIF-1α’s (with HIF-1β) role to mediate adaptive responses to hypoxia. HIF-1 therefore increases erythropoiesis, enhances breathing, glucose uptake, promotes angiogenesis, reduces mitochondrial oxygen consumption, and induces cell cycle arrest (Fig. 2).
Newborn experimental oxygen studies
A number of newborn animal models have been employed to study effects of oxygenation of different organs.
Inflammation and DNA damage. Reoxygenation with hyperoxia (60 or 100% O2) not only induces inflammation in the lungs but also in the brain and probably in other organs as well.61,62 Even a brief (minutes) hyperoxic exposure immediately after birth has been epidemiologically linked to conditions associated with inflammation and DNA damage, such as childhood malignancies.63,64 It is therefore of interest that hyperoxic resuscitation in both newborn piglets and mice increases the level of 8-oxoguanine in tissues and urine, indicating oxidation of guanine into this mutagenic base lesion,65,66 which in turn suggests that oxygen may be a mutagen. Furthermore, it has been demonstrated that base repair mechanisms are affected by hyperoxic reoxygenation, and if protective DNA glycosylases are knocked out, DNA injury increases. The DNA glycosylase Neil 3 is important for removal of oxidative base lesions on single-stranded DNA, cellular-dependent cellular responses to hypoxia–ischemia in the perinatal mouse brain, and maintenance of microglia number. Profound neuropathology was found in Neil 3-knockout mice characterized by a reduced number of microglia and loss of proliferating neuronal progenitors in the striatum after hypoxia–ischemia. In vitro expansion of Neil 3-deficient neural stem/progenitor cells revealed an inability to augment neurogenesis and a reduced capacity to repair for oxidative base lesions in single-stranded DNA.67
Metabolomics. Metabolomic studies suggest that resuscitation with air from a metabolic viewpoint is more optimal than resuscitation with either 18% or 100% oxygen. Hypoxia leads to elevation of Krebs' cycle intermediates, such as α-ketoglutarate, succinate, and fumarate.68 However, these intermediates decrease more slowly after resuscitation with 100% oxygen, suggesting that hyperoxia leads to mitochondrial dysfunction. Different FiO2 may also impact of metabolic recovery. In a piglet model of asphyxia, Fanos et al.69 showed with nuclear magnetic resonance spectroscopy that resuscitation with 18% oxygen led to carbohydrate exhaustion, while using supraphysiologic (40% or 100%) oxygen led to the generation of free radicals and activation of scavenging systems. This suggested that 21% oxygen could lead to best physiologic recovery after hypoxemia.
Furthermore, succinate, considered a highly relevant marker of mitochondrial dysfunction due to its ability to regulate electron flow across the electron respiratory chain,70,71 creates the so-called reverse electron transport from Complex-II to Complex-I, which generates a many-fold increased production of ROS compared to the conventional forward electron transport from Complex-I to Complex-II.70 Therapeutic hypothermia in asphyxiated babies after reoxygenation, for example, favors normalization of energy metabolites such as pyruvate and Krebs’ cycle components, particularly succinate. Several studies and a recent review have now outlined the molecular and metabolomics changes associated with asphyxia and resuscitation with various concentrations of oxygen.72,73,74,75
Gene regulation and epigenetic changes. Gene regulation in different organs of newborn animal models after brief hyperoxia at resuscitation and after long-term oxygen exposure has been studied.76 Several hundred genes were changed within the lungs of newborn mice reoxygenated with 60% or 100% oxygen (hyperoxia) when compared to air.77 HIF-1-responsive genes and pathways related to cell cycling and nucleotide excision repair are up-regulated with involvement of the mammalian target of rapamycin signaling pathway, including genes related to growth (VegfC, Pgf) and signal transduction. This pathway plays a crucial role in the regulation of cell proliferation, survival, and energy metabolism in response to stress. An indication of DNA-damage response includes the up-regulation of nucleotide excision repair mechanisms after hyperoxic (60% O2) reoxygenation. Conversely, DNA polymerase is down-regulated by hyperoxia, leading to reduction of DNA replication78 and hyperoxic reoxygenation induces a stronger brain inflammatory gene response than reoxygenation with air.79
Chen et al.80 studied epigenetic changes in the lungs of newborn rats breathing either air or 85% O2 from day 1 to 14. On day 14, rats exposed to hyperoxia had significantly lower body and lung weights than rats breathing air. Hyperoxia also induced alveolar arrest. In total, four DNA methylated genes associated with hyperoxia-induced inhibition of alveolarization were found, including a growth factor receptor-bound protein involved in signal transduction and cell communication and a β1-integrin that links cytoskeleton to the extracellular environment, acting as adhesion receptors, signaling receptors, and mechanoreceptors to regulate cell growth, migration, and differentiation. β1-Integrin is also required for lung branching morphogenesis and alveolarization. At 4 weeks of age, the lungs of mice exposed to hyperoxia for 14 days were changed, suggesting an overall DNA-hypermethylation effect of hyperoxia.81 The hypermethylated genes, including Tgfbr1, Crebbp, and Creb1, play central roles in the tumor growth factor-β (TGF-β) signaling pathway and cell cycle regulation. They also had a statistically significant enrichment of five pathways, particularly of the TGF-β signaling pathway, that is involved in the inhibition of branching morphogenesis in embryonic lung development.82
Whether these findings are clinically pertinent are uncertain. In preterm infants, apnea leads to the major clinical problem of intermittent hypoxia (IH), when carotid body chemo-reflexes and catecholamine secretion from adrenal medullary chromaffin cells are important for maintenance of cardio-respiratory homeostasis. The effects of neonatal IH may persist into adulthood by triggering epigenetic mechanisms involving DNA hypermethylation, which in turn contribute to long-lasting increase in ROS levels. Adults born preterm exhibit a higher incidence of sleep-disordered breathing and hypertension that is associated with elevated oxidative stress, decreased expression of genes encoding antioxidant enzymes, and increased expression of pro-oxidant enzymes. DNA hypermethylation of a single CpG nucleoside has the capacity to alter expression of manganese superoxide dismutase 2 (mitochondrial SOD) and DNA-hypomethylating agents such as decitabine prevents oxidative stress, enhances hypoxic sensitivity, and reduces autonomic dysfunction. The use of DNA-hypomethylating agents might offer a novel therapeutic intervention to decrease long-term cardio-respiratory morbidity caused by neonatal IH.83,84
Overall, these studies indicate that long-term hyperoxic exposure leads to DNA methylation of genes that are related to lung growth and development including lung morphogenesis, branching, and alveolarization that are typical features of bronchopulmonary dysplasia. Epigenetic silencing may therefore potentially contribute to pathogenesis and lifelong consequence of bronchopulmonary dysplasia and other aspects of hyperoxia. Fig. 3 summarizes some of the relevant mechanisms and pathways for newborn hyperoxic exposure.

Summary of some pathways and mechanisms relevant for newborn hyperoxic exposure. Adapted from Bhandari.122 Please see text for details
Human data
In the delivery room: term infants. Pure oxygen has been integral to the delivery room support of newborn infants for 200 years,85 but in 1998 the World Health Organization (WHO) recommended that air (FiO2 0.21) could be used instead of pure oxygen (FiO2 1.0) for basic newborn resuscitation.86 In 2010, the International Liaison Committee on Resuscitation (ILCOR) followed up with a similar recommendation for term or near-term infants based on clinical data acquired over the previous decade, suggesting that pure oxygen resuscitation could lead to unfavorable outcomes, including increased time to first breath and mortality, when compared to the use of air.24,25 These recommendations were supported by human and animal data showing that even a brief exposure of pure oxygen in the delivery room could trigger long-term inflammation and oxidative stress that could last for weeks.40,87,88,89,90
This, however, does not mean that supplemental oxygen should never be used. The first studies conducted in the 1990s used pure oxygen to supplement air in infants that did not respond to resuscitative efforts within 90 s of life.20,21 Oxygen levels were not titrated as per today’s practice24,25 because “normative” data from spontaneously breathing term infants were not obtained until the next decade. Such data showed that preductal peripheral capillary oxygen saturation (SpO2) increased only gradually over 10 min of life91,92 and that using 100% oxygen for respiratory support led to a more rapid increase in SpO2 than was observed during normal transition of the healthy infant.30,93 Despite this, the optimum evolution of SpO2 following a pathological birth such as birth asphyxia or preterm delivery is unknown and could be very different to that of normal, full-term and healthy infants.
There are few data regarding optimal oxygenation immediately after completion of active resuscitation for pathological conditions such as hypoxic encephalopathy. Klinger et al.94 showed that the combination of hyperoxia and hypocapnia in the first hours after birth is especially detrimental for long-term outcome. In an observational study, Kapadia et al.95 observed a fourfold increased risk of moderate to severe hypoxic–ischemic encephalopathy within infants having a very high admission partial pressure of oxygen (PaO2) (>231 mmHg, 30.8 kPa) compared to those with PaO2 within physiological norms (<114 mmHg, 15.2 kPa) PaO2.
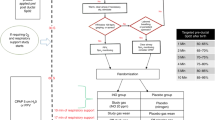
In the delivery room: preterm infants. The case for preterm infants is more ambiguous (Fig. 4). Currently, data from 11 published studies26,27,28,29,30,31,32,33,34,35,36 for babies <32 weeks gestation who were resuscitated with either initial FiO2≤0.3 or ≥0.6 and titrated to varying SpO2 targets in the first 10 min of life suggest that there is little benefit/risk to using different levels of initial FiO2. However, it must be recognized that these studies were planned and mostly completed prior to the availability of evidence for normal physiological SpO2 changes seen in healthy full-term infants.91,92 Indeed, none were designed to examine the impact of SpO2 targeting on infant outcomes and none were powered sufficiently to examine either short-term or long-term outcomes including death and bronchopulmonary dysplasia (BPD).

Possible mechanisms explaining the need for higher FiO2 in preterm infants in the delivery room. Ineffective gas exchange, vascular insensitivity to oxygen, and poor antioxidant defense may play a role in increasing the risk of respiratory failure
Nevertheless, a recent meta-analysis of these studies96 showed no difference in major outcomes, including death and morbidities such as BPD, regardless of initial FiO2, even though it was noted that none of these studies examined the most commonly used initial FiO2: 0.4–0.5. A recent Cochrane review of 10 of these studies97 continued to emphasize the uncertainty of this practice, finding that only one study showed an increased mortality rate in infants <28 weeks gestation resuscitated with lower (0.21) vs. higher (1.0) initial FiO2,31 but other factors may play a part in infant outcome, including SpO2. Oei et al.98 showed that regardless of initial FiO2, infants that did not reach SpO2 80% by 5 min of age were at significantly increased risk of bradycardia, intraventricular hemorrhage (IVH), and death. Whether these infants were unable to reach target SpO2 due to inherent clinical instability or whether they were given less oxygen than required is uncertain.
Most clinicians will now use lower amounts of oxygen (FiO2 ≤ 0.4) to initiate preterm infant resuscitation99 despite lack of evidence for both short-term and long-term outcomes. The lack of evidence is reflected in the astoundingly wide variations in clinical practice guidelines for oxygen use around the world, where SpO2 recommendations can vary by as much as 25%.100 Certainly, due to the widespread implementation of low oxygenation resuscitation within the last decade, sufficiently powered studies to determine the impact of both starting FiO2 and recommended FiO2 targets of preterm infants are needed.
The case of biological uncertainty in preterm infants. There is underlying pathophysiological evidence that hyperoxic resuscitation may cause as much biochemical derangement in preterm infants as hypoxia but whether this leads to clinical morbidity and mortality is unclear. For example, Vento et al.27 found that using higher FiO2 (0.9) to initiate preterm infant (≤28 weeks’ gestation) resuscitation significantly increased urinary 8-oxo-dihydroguanosine, isoprostanes, and isofurans, suggesting oxidative damage to cell components, when compared to resuscitation with FiO2 0.3, but whether this leads to clinically relevant outcomes is again unclear.27 Consideration must also be given to the potential long-term, including epigenetic, consequences of preterm oxygen exposure. As mentioned, hyperoxia is associated with significant changes to genes related to the cell cycle, antioxidant defense enzymes, DNA repair, and inflammation. Of note, DNA methylation was significantly increased when the oxygen load in the delivery room reached values above 500 mL O2/kg body weight,101 a possible explanation for the long-lasting effects of oxygen supplementation in the fetal to neonatal transition. Further analytical determinations are needed to assess long-lasting permanence of the effects of oxygen upon the methylome of preterm infants.
Should oxygen delivery be individualized? Preterm and term infants for different reasons require respiratory stabilization at birth.102 Currently, systematic reviews suggest that term and near-term infants (≥32 weeks GA) may benefit from initial resuscitation with 0.21 rather than 1.0 initial FiO2, but that lower FiO2 (≤0.3) should be used for infants <28 weeks gestation.102 Initial FiO2 appears to have minimal impact on mortality or short-term morbidity for infants between 28 and 31 weeks gestations.103,104,105 Data for infants <28 weeks gestation remain unclear, but there is indication from current evidence that regardless of initial FiO2, the amount of oxygen given to the infants should be manipulated to reach a target SpO2 of 80–85% and a heart rate of 100 bpm within 5 min to decrease the risk of serious IVH and death.98 It must also be remembered that data for “normal” physiological development of postnatal SpO2 in this group are lacking and that clinicians must be cognizant of the need to adjust FiO2 in response to the infant’s individual need.
The association between oxygen at birth and longer-term outcomes in preterm infants. There is emerging evidence that the amount of oxygen received at birth may have profound implications for the long-term outcomes of the high-risk newborn. In the initial studies,106 using air or pure oxygen to initiate delivery room resuscitation of asphyxiated term or near-term infants made no difference to the neurodevelopmental outcomes of survivors. However, the majority of these infants were recruited from low-income countries from more than 20 years ago, when resuscitation practices were very different. The infants were given either air or pure oxygen that was not titrated to SpO2 changes, and whether oxygen titration would have affected neurodevelopment in asphyxiated full-term newborn survivors is unclear.
There is slightly more information on preterm infants. A population review of preterm (<29 weeks) Canadian children found no difference in death or neurodevelopmental impairment after Canadian resuscitation guidelines were changed from FiO2 1.0 (n = 581) to FiO2 0.21 (n = 445)/intermediate FiO2 (0.22–0.99, n = 483). The use of pure oxygen, however, was associated with an increased risk of severe neurodevelopmental injury when compared to air (adjusted odds ratio (OR) 1.57, 95% confidence interval (CI): 1.05–2.35).103 Boronat et al.104 reported on the outcomes of 206 children enrolled in three multicenter RCTs examining infants <32 weeks gestation after resuscitation with either initial FiO2 0.3 or 0.6 and found no difference in the risk of major disability or death. In a meta-analysis involving 542 infants, a 5-min SpO2<80% was associated with IVH (OR 2.04, 95% CI 1.01–4.11, p < 0.05). Bradycardia (heart rate <100 bpm) at 5 min increased risk of death (OR 4.57, 95% CI 1.62–13.98, p < 0.05), while no differences were seen with initial FiO2.98
Secondary analyses
Follow-up to the Torpido study, the largest RCT to examine low (0.21) vs. high (1.0) initial FiO2 for preterm (<32 weeks gestation) infant resuscitation found no difference in the risk of death and/or major disability at 2 years.105 However, in exploratory, secondary analyses, infants who did not attain a minimum 5 min SpO2 of 80% were significantly more likely to be disabled/deceased than those with SpO2≥80% (OR 1.33). Cognitive subscales on the Bayley III test were also higher, especially in infants ≥28 weeks gestation who had SpO2≥80% (mean (SD) 100.8 (12.5) vs. 95.2 (12.4)). It must be acknowledged again that SpO2 targeting was not part of the study protocol and again, as noted previously, whether infants failed to achieve SpO2 80% by 5 min (a target that was only introduced in 2010) whether they were too sick or were not given enough oxygen is unclear.
Immature infants beyond the delivery room
Clinical guidelines for optimal oxygenation of preterm infants beyond the delivery room were based on weak evidence, such as observational studies. Such data suggest that low SpO2 or PaO2 may protect premature infants against the development of severe retinopathy of prematurity (ROP), without increase in mortality.107 However, these data were quickly challenged and the need for RCTs to obtain evidence-based data became clear.
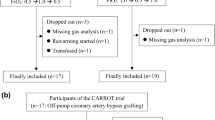
The five NeOProM (Neonatal Oxygen Prospective Meta-analysis) studies were the first RCTs to determine the effects of lower vs. higher SpO2 targets in newborn infants <28 weeks before the age of 24 h.108 In total, 4911 infants were enrolled: 2456 to low (85–89%) and 2455 to high (91–95%) SpO2 targets.108,109,110,111 Although no difference was found in the primary outcome (defined as combined death and/or major disability, i.e., neurodevelopmental impairment), infants nursed in lower SpO2 had a significantly increased risk (relative risk (RR) 1.18) of death. Survivors were at decreased risk of BPD (defined as O2 requirement at 36 weeks corrected gestation (RR 0.81)), but there was no difference in the risk of other outcomes, such as PDA, IVH or blindness, which was, in any case, a rare event112,113,114,115,116 (see Fig. 5).

The combined outcome of death and/or physiological BPD at 36 weeks was not uniformly reported in all of these studies. Only one study, the SUPPORT trial,109 provided data on this combined outcome (85–89% target group—319/654–49% and 91–95% target group—331/662 (50%) with an adjusted relative risk of 0.99 (95% CI: 0.9–1.1), but whether this outcome was based on physiological need or prescription of oxygen cannot be determined (i.e., need vs. use). Recommendations for oxygen therapy are summarized in Table 1
Conclusion
Experimental and clinical studies have promoted changes in clinical practice regarding newborn oxygenation. The understanding of the significance of oxidative stress in the 1980s led to a renewed interest for clinical studies a decade later. The demonstration that pure oxygen might be harmful in newborn resuscitation triggered a series of new studies leading to the dramatic change of clinical practice the last years. This new understanding confirms the importance of ventilation rather than oxygen as the basis of new resuscitation programs in developing and low resourced countries, such as Helping Babies Breathe.117
The quest to determine best oxygen therapy for sick patients seems to have even reached the echelons of adult medicine. The results from a meta-analysis of 16,037 patients with critical illnesses of comparable severity (e.g., stroke, trauma, myocardial infarction, cardiac arrest, etc.) from 25 RCTs showed that treatment with liberal oxygen therapies significantly increased the risk of death in hospital, at 30 days and at longest follow-up, when compared to treatment with conservative oxygen therapies.118
The enormous accumulation of knowledge and massive amounts of change in the recent years for the field of newborn oxygenation needs to be harnessed. Experimental data as well as large RCTs have contributed greatly to this knowledge, but there is increasing awareness that more data are needed. The amount of oxygen given to newborn infants has been substantially reduced over the last two decades, but whether this is best for survival and long-term outcomes is unclear, especially for preterm infants, who may need some amount of oxygen to decrease pulmonary arterial pressure119 and to stimulate the respiratory center to open their glottis and to initiate breathing or to remove the hypoxic inhibition of breathing.120
Until we solve this problem, the oxygen dilemma remains.121 The balance between death and morbidity for newborn infants is delicate. Higher oxygen levels may increase survival, but survivors may be left with serious morbidities such as ROP and BPD. Conversely, lower oxygen levels may lead to an increased risk of death, but survivors could be at lower risk of problems caused by oxygen toxicity. Much more information is needed to allow clinicians to choose between the lesser of two evils as whatever happens in the newborn period will impact on the infants for the whole of their lives.
References
Lane, N. Oxygen. The Molecule that Made the World (Oxford University Press, New York, 2002).
Luo, G. et al. Rapid oxygenation of Earth’s atmosphere 2.33 billion years ago. Sci. Adv. 2, e1600134 (2016).
Case, A. J. On the origin of superoxide dismutase: an evolutionary perspective of superoxide-mediated redox signaling. Antioxidants. (Basel) 6, pii: E82 (2017).
Jheeta, S. The landscape of the emergence of life. Life (Basel) 7, pii: E27 (2017).
Cantine, M. D. & Fournier, G. P. Environmental adaptation from the origin of life to the last universal common ancestor. Orig. Life Evol. Biosph. 48, 35–54 (2018).
Martin, W. F. & Sousa, F. L. Early microbial evolution: the age of anaerobes. Cold Spring Harb. Perspect. Biol. 8, a018127 (2015).
Margulis, L. & Chapman, M. J. Endosymbioses: cyclical and permanent evolution. Trends Microbiol. 6, 342–345 (1998).
Izon, G. et al. Biological regulation of atmospheric chemistry en route to planetary oxygenation. Proc. Natl. Acad. Sci. USA 114, E2571–E2579 (2017).
Schirrmeister, B. E., de Vos, J. M., Antonelli, A. & Bagheri, H. C. Evolution of multicellularity coincided with increased diversification of cyanobacteria and the Great Oxidation Event. Proc. Natl. Acad. Sci. USA 110, 1791–1796 (2013).
Gerschman, R., Gilbert, D. L., Nye, S. W., Dwyer, P. & Fenn, W. O. Oxygen poisoning and x-irradiation: a mechanism in common. Science 119, 623–626 (1954).
Frank, L. & Groseclose, E. E. Preparation for birth into an O2-rich environment: the antioxidant enzymes in the developing rabbit lung. Pediatr. Res. 18, 240–244 (1984).
Saugstad, O. D. Hypoxanthine as an indicator of hypoxia: its role in health and disease through free radical production. Pediatr. Res. 23, 143–150 (1988).
Sullivan, J. L. Iron, plasma antioxidants, and the ‘oxygen radical disease of prematurity’. Am. J. Dis. Child 142, 1341–1344 (1988).
Tin, W., Milligan, D. W., Pennefather, P. & Hey, E. Pulse oximetry, severe retinopathy, and outcome at one year in babies of less than 28 weeks gestation. Arch. Dis. Child. Fetal Neonatal Ed. 84, F106–F110 (2001).
Chow, L. C., Wright, K. W. & Sola, A., CSMC Oxygen Administration Study Group. Can changes in clinical practice decrease the incidence of severe retinopathy of prematurity in very low birth weight infants? Pediatrics 111, 339–345 (2003).
Anderson, C. G., Benitz, W. E. & Madan, A. Retinopathy of prematurity and pulse oximetry: a national survey of recent practices. J. Perinatol. 24, 164–168 (2004).
Silverman, W. A. A cautionary tale about supplemental oxygen: the albatross of neonatal medicine. Pediatrics 113, 394–396 (2004).
Supplemental Therapeutic Oxygen for Prethreshold Retinopathy Of Prematurity (STOP-ROP), a randomized, controlled trial. I: primary outcomes. Pediatrics 105, 295–310 (2000).
Askie, L. M., Henderson-Smart, D. J., Irwig, L. & Simpson, J. M. Oxygen-saturation targets and outcomes in extremely preterm infants. N. Engl. J. Med. 349, 959–967 (2003).
Ramji, S. et al. Resuscitation of asphyxic newborn infants with room air or 100% oxygen. Pediatr. Res. 34, 809–812 (1993).
Saugstad, O. D., Rootwelt, T. & Aalen, O. Resuscitation of asphyxiated newborn infants with room air or oxygen: an international controlled trial: the Resair 2 Study. Pediatrics 102, e1 (1998).
Saugstad, O. D., Ramji, S., Soll, R. F. & Vento, M. Resuscitation of newborn infants with 21% or 100% oxygen: an updated systematic review and meta-analysis. Neonatology 94, 176–182 (2008).
International Liaison Committee on Resuscitation. The International Liaison Committee on Resuscitation (ILCOR) consensus on science with treatment recommendations for pediatric and neonatal patients: pediatric basic and advanced life support. Pediatrics 117, e955–e977 (2006).
Wyllie, J. et al. Part 11: Neonatal resuscitation: 2010 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science with Treatment Recommendations. Resuscitation 81(Suppl 1), e260–e287 (2010).
Perlman, J. M. et al. Part 7: Neonatal Resuscitation: 2015 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations (Reprint). Pediatrics 132(Suppl. 1), S204–S241 (2015).
Wang, C. L. et al. Resuscitation of preterm neonates by using room air or 100% oxygen. Pediatrics 121, 1083–1089 (2008).
Vento, M. et al. Preterm resuscitation with low oxygen causes less oxidative stress, inflammation, and chronic lung disease. Pediatrics 124, e439–e449 (2009).
Rabi, Y., Singhal, N. & Nettel-Aguirre, A. Room-air versus oxygen administration for resuscitation of preterm infants: the ROAR study. Pediatrics 128, e374–e381 (2011).
Kapadia, V. S. et al. Resuscitation of preterm neonates with limited versus high oxygen strategy. Pediatrics 132, e1488–e1496 (2013).
Escrig, R. et al. Achievement of targeted saturation values in extremely low gestational age neonates resuscitated with low or high oxygen concentrations: a prospective, randomized trial. Pediatrics 121, 875–881 (2008).
Oei, J. et al. Targeted oxygen in the resuscitation of preterm infants, a randomized clinical trial. Pediatrics 139, e20161452 (2017). pii.
Rook, D. et al. Resuscitation of preterm infants with different inspired oxygen fractions. J. Pediatr. 164, 1322–6.e3 (2014).
Lundstrøm, K. E., Pryds, O. & Greisen, G. Oxygen at birth and prolonged cerebral vasoconstriction in preterm infants. Arch. Dis. Child. 73, F81–F86 (1995).
Ezaki, S. et al. Resuscitation of preterm infants with reduced oxygen results in less oxidative stress than resuscitation with 100% oxygen. J. Clin. Biochem. Nutr. 44, 111–118 (2009).
Harling, A. E. et al. Does the use of 50% oxygen at birth in preterm infants reduce lung injury? Arch. Dis. Child. Fetal Neonatal Ed. 90, F401–F405 (2005).
Kumar, V. H. et al. Oxygen resuscitation and oxidative stress biomarkers in premature infants. Res. Rep. Neonatol. 4, 91–99 (2014).
Rootwelt, T., Løberg, E. M., Moen, A., Oyasaeter, S. & Saugstad, O. D. Hypoxemia and reoxygenation with 21% or 100% oxygen in newborn pigs: changes in blood pressure, base deficit, and hypoxanthine and brain morphology. Pediatr. Res. 32, 107–113 (1992).
Poulsen, J. P., Oyasaeter, S. & Saugstad, O. D. Hypoxanthine, xanthine, and uric acid in newborn pigs during hypoxemia followed by resuscitation with room air or 100% oxygen. Crit. Care Med. 21, 1058–1065 (1993).
Patel, A. et al. Exposure to supplemental oxygen downregulates antioxidant enzymes and increases pulmonary arterial contractility in premature lambs. Neonatology 96, 182–192 (2009).
Lakshminrusimha, S. et al. Pulmonary arterial contractility in neonatal lambs increases with 100% oxygen resuscitation. Pediatr. Res. 59, 137–141 (2006).
Halliwell, B. & Gutteridge, J. M. Oxygen toxicity, oxygen radicals, transition metals and disease. Biochem. J. 219, 1–14 (1984).
Sanderud, J., Norstein, J. & Saugstad, O. D. Reactive oxygen metabolites produce pulmonary vasoconstriction in young pigs. Pediatr. Res. 29, 543–547 (1991).
Clyman, R. I., Saugstad, O. D. & Mauray, F. Reactive oxygen metabolites relax the lamb ductus. Circ. Res. 64, 1–8 (1989).
Wedgwood, S. et al. Hydrogen peroxide regulates extracellular superoxide dismutase activity and expression in neonatal pulmonary hypertension. Antioxid. Redox Signal. 15, 1497–1506 (2010).
Buonocore, G., Zani, S., Perrone, S., Caciotti, B. & Bracci, R. Intraerythrocyte nonprotein-bound iron and plasma malondialdehyde in the hypoxic newborn. Free Radic. Biol. Med. 25, 766–770 (1998).
Ciccoli, L. et al. Iron release in erythrocytes and plasma non-protein-bound iron in hypoxic and non hypoxic newborns. Free Radic. Res. 37, 51–58 (2003).
Viña, J. et al. l-Cysteine and glutathione metabolism are impaired in premature infants due to cystathionase deficiency. Am. J. Clin. Nutr. 61, 1067–1069 (1995).
Frank, L. & Sosenko, I. R. Prenatal development of lung antioxidant enzymes in four species. J. Pediatr. 110, 106–110 (1987).
Vento, M. et al. Antenatal steroids and antioxidant enzyme activity in preterm infants: influence of gender and timing. Antioxid. Redox Signal. 11, 2945–2955 (2009).
Prabhakar, N. R. & Peng, Y. J. Oxygen sensing by the carotid body: past and present. Adv. Exp. Med. Biol. 977, 3–8 (2017).
Prabhakar, N. R., Dinerman, J. L., Agani, F. H. & Snyder, S. H. Carbon monoxide: a role in carotid body chemoreception. Proc. Natl. Acad. Sci. USA 92, 1994–1997 (1995).
Prieto-Lloret, J. & Aaronson, P. I. Hydrogen sulfide as an O2 sensor: a critical analysis. Adv. Exp. Med. Biol. 967, 261–276 (2017).
Caravagna, C. & Seaborn, T. Oxygen sensing in early life. Lung 194, 715–722 (2016).
Prabhakar, N. R. & Semenza, G. L. Regulation of carotid body oxygen sensing by hypoxia-inducible factors. Pflug. Arch. 468, 71–75 (2016).
Semenza, G. L. & Prabhakar, N. R. The role of hypoxia-inducible factors in carotid body (patho) physiology. J. Physiol. https://doi.org/10.1113/JP275696 (2018).
Maltepe, E. & Saugstad, O. D. Oxygen in health and disease: regulation of oxygen homeostasis—clinical implications. Pediatr. Res. 65, 261–268 (2009).
Huang, L. E., Gu, J., Schau, M. & Bunn, H. F. Regulation of hypoxia-inducible factor 1alpha is mediated by an O2-dependent degradation domain via the ubiquitin-proteasome pathway. Proc. Natl. Acad. Sci. USA 95, 7987–7992 (1998).
Rankin, E. B. et al. Hypoxia-inducible factor-2 (HIF-2) regulates hepatic erythropoietin in vivo. J. Clin. Invest. 117, 1068–1077 (2007).
Bellot, G. et al. Hypoxia-induced autophagy is mediated through hypoxia-inducible factor induction of BNIP3 and BNIP3L via their BH3 domains. Mol. Cell. Biol. 29, 2570–2581 (2009).
Goda, N. et al. Hypoxia-inducible factor 1alpha is essential for cell cycle arrest during hypoxia. Mol. Cell. Biol. 23, 359–369 (2003).
Koch, J. D., Miles, D. K., Gilley, J. A., Yang, C. P. & Kernie, S. G. Brief exposure to hyperoxia depletes the glial progenitor pool and impairs functional recovery after hypoxic–ischemic brain injury. J. Cereb. Blood Flow Metab. 28, 1294–1306 (2008).
Munkeby, B. H. et al. Resuscitation of hypoxic piglets with 100% O2 increases pulmonary metalloproteinases and IL-8. Pediatr. Res. 58, 542–548 (2005).
Naumburg, E., Bellocco, R., Cnattingius, S., Jonzon, A. & Ekbom, A. Supplementary oxygen and risk of childhood lymphatic leukaemia. Acta Paediatr. 91, 1328–1333 (2002).
Spector, L.G., Klebanoff, M.A., Feusner, J. H., Georgieff, M. K. & Ross, J. A. Childhood cancer following neonatal oxygen supplementation. J. Pediatr. 147, 27–31 (2005).
Sejersted, Y., Aasland, A. L., Bjørås, M., Eide, L. & Saugstad, O. D. Accumulation of 8-oxoguanine in liver DNA during hyperoxic resuscitation of newborn mice. Pediatr. Res. 66, 533–538 (2009).
Solberg, R., Andresen, J. H., Escrig, R., Vento, M. & Saugstad, O. D. Resuscitation of hypoxic newborn piglets with oxygen induces a dose-dependent increase in markers of oxidation. Pediatr. Res. 62, 559–563 (2007).
Sejersted, Y. et al. Endonuclease VIII-like 3 (Neil3) DNA glycosylase promotes neurogenesis induced by hypoxia–ischemia. Proc. Natl. Acad. Sci. USA 108, 18802–18807 (2011).
Solberg, R. et al. Metabolomic analyses of plasma reveals new insights into asphyxia and resuscitation in pigs. PLoS ONE 5, e9606 (2010).
Fanos, V. et al. Metabolomics network characterization of resuscitation after normocapnic hypoxia in a newborn piglet model supports the hypothesis that room air is better. Biomed. Res. Int. 2014, 731620 (2014).
Sahni, P. V. et al. Krebs cycle metabolites and preferential succinate oxidation following neonatal hypoxic–ischemic brain injury in mice. Pediatr. Res. 83, 491–497 (2018).
Sánchez-Illana, Á. et al. Evolution of energy related metabolites in plasma from newborns with hypoxic–ischemic encephalopathy during hypothermia treatment. Sci. Rep. 7, 17039 (2017).
Saugstad, O. D., Sejersted, Y., Solberg, R., Wollen, E. J. & Bjørås, M. Oxygenation of the newborn: a molecular approach. Neonatology 101, 315–325 (2012).
Solberg, R. et al. Changes of the plasma metabolome of newly born piglets subjected to postnatal hypoxia and resuscitation with air. Pediatr. Res. 80, 284–292 (2016).
Solberg, R. et al. Resuscitation of hypoxic newborn piglets with supplementary oxygen induces dose-dependent increase in matrix metalloproteinase-activity and down-regulates vital genes. Pediatr. Res. 67, 250–256 (2010).
Kuligowski, J. et al. Plasma metabolite score correlates with hypoxia time in a newly born piglet model for asphyxia. Redox Biol. 12, 1–7 (2017).
Tyree, M. M., Dalgard, C. & O’Neill, J. T. Impact of room air resuscitation on early growth response gene-1 in a neonatal piglet model of cerebral hypoxic ischemia. Pediatr. Res. 59, 423–427 (2006).
Wollen, E. J. et al. Transcriptome profiling of the newborn mouse lung after hypoxia and reoxygenation: hyperoxic reoxygenation affects mTOR signaling pathway, DNA repair, and JNK-pathway regulation. Pediatr. Res. 74, 536–544 (2013).
Rognlien, A. G., Wollen, E. J., Atneosen-Åsegg, M. & Saugstad, O. D. Temporal patterns of gene expression profiles in the neonatal mouse lung after hypoxia–reoxygenation. Neonatology 111, 45–54 (2017).
Rognlien, A. G., Wollen, E. J., Atneosen-Åsegg, M. & Saugstad, O. D. Increased expression of inflammatory genes in the neonatal mouse brain after hyperoxic reoxygenation. Pediatr. Res. 77, 326–333 (2015).
Chen, C. M., Liu, Y. C., Chen, Y. J. & Chou, H. C. Genome-wide analysis of DNA methylation in hyperoxia-exposed newborn rat lung. Lung 195, 661–669 (2017).
Bik-Multanowski, M. et al. Hyperoxia induces epigenetic changes in newborn mice lungs. Free Radic. Biol. Med. 121, 51–56 (2018).
Ahlfeld, S. K., Wang, J., Gao, Y., Snider, P. & Conway, S. J. Initial suppression of transforming growth factor-β signaling and loss of TGFBI causes early alveolar structural defects resulting in bronchopulmonary dysplasia. Am. J. Pathol. 186, 777–793 (2016).
Nanduri, J. & Prabhakar, N. R. Developmental programming of O(2) sensing by neonatal intermittent hypoxia via epigenetic mechanisms. Respir. Physiol. Neurobiol. 185, 105–109 (2013).
Nanduri, J. et al. Epigenetic regulation of hypoxic sensing disrupts cardio-respiratory homeostasis. Proc. Natl. Acad. Sci. USA 109, 2515–2520 (2012).
Obladen, M. History of neonatal resuscitation. Part 2: oxygen and other drugs. Neonatology 95, 91–96 (2009).
Safe Motherhood—Basic Newborn Resuscitation: A Practical Guide—Maternal and Newborn Health/Safe Motherhood Unit; Division of Reproductive Health (technical support) (World Health Organization, Geneva, 1998).
Vento, M., Sastre, J., Asensi, M. A. & Viña, J. Room-air resuscitation causes less damage to heart and kidney than 100% oxygen. Am. J. Respir. Crit. Care. Med. 172, 1393–1398 (2005).
Vento, M. et al. Resuscitation with room air instead of 100% oxygen prevents oxidative stress in moderately asphyxiated term neonates. Pediatrics 107, 642–647 (2001).
Kumar, V. H. et al. Exposure to supplemental oxygen and its effects on oxidative stress and antioxidant enzyme activity in term newborn lambs. Pediatr. Res. 67, 66–71 (2010).
Vento, M. et al. Oxidative stress in asphyxiated term infants resuscitated with 100% oxygen. J. Pediatr. 142, 240–246 (2003).
Mariani, G. et al. Pre-ductal and post-ductal O2 saturation in healthy term neonates after birth. J. Pediatr. 150, 418–421 (2007).
Dawson, J. A. et al. Defining the reference range for oxygen saturation for infants after birth. Pediatrics 125, e1340–e1347 (2010).
White, L. N. et al. Achievement of saturation targets in preterm infants <32 weeks’ gestational age in the delivery room. Arch. Dis. Child. Fetal Neonatal Ed. 102, F423–F427 (2017).
Klinger, G., Beyene, J., Shah, P. & Perlman, M. Do hyperoxaemia and hypocapnia add to the risk of brain injury after intrapartum asphyxia? Arch. Dis. Child. Fetal Neonatal Ed. 90, F49–F52 (2005).
Kapadia, V. S. et al. Perinatal asphyxia with hyperoxemia within the first hour of life is associated with moderate to severe hypoxic–ischemic encephalopathy. J. Pediatr. 163, 949–954 (2013).
Oei, J. L. et al. Higher or lower oxygen for delivery room resuscitation of preterm infants below 28 completed weeks gestation: a meta-analysis. Arch. Dis. Child. Fetal Neonatal Ed. 102, F24–F30 (2017).
Lui, K. et al. Lower versus higher oxygen concentrations titrated to target oxygen saturations during resuscitation of preterm infants at birth. Cochrane Database Syst. Rev. 5, CD010239 (2018).
Oei, J. L. et al. Outcomes of oxygen saturation targeting during delivery room stabilisation of preterm infants. Arch. Dis. Child Fetal Neonatal Ed. pii: fetalneonatal-2016-312366 (2017).
Oei, J. L. et al. Clinicians in 25 countries prefer to use lower levels of oxygen to resuscitate preterm infants at birth. Acta Paediatr. 105, 1061–1066 (2016).
Wilson, A. et al. A review of international clinical practice guidelines for the use of oxygen in the delivery room resuscitation of preterm infants. Acta Paediatr. 107, 20–27 (2018).
Lorente-Pozo S. et al. Oxygen load influences DNA methylation in preterm infants upon delivery room stabilization. J. Pediatr. (2018) pii: S0022-3476(18)30902-8. https://doi.org/10.1016/j.jpeds.2018.07.009.
Oei, J. L., Saugstad, O. D. & Vento, M. Oxygen and preterm infant resuscitation: what else do we need to know? Curr. Opin. Pediatr. 30, 192–198 (2018).
Soraisham, A. S. et al. Neurodevelopmental outcomes of preterm infants resuscitated with different oxygen concentration at birth. J. Perinatol. 37, 1141–1147 (2017).
Boronat, N. et al. Survival and neurodevelopmental outcomes of preterms resuscitated with different oxygen fractions. Pediatrics 138, pii: e20161405 (2016).
Thamrin, V. et al. Preterm infant outcomes after randomization to initial resuscitation with FiO2 0.21 or 1.0. J. Pediatr. 201, 55–61 (2018).
Saugstad, O. D., Vento, M., Ramji, S., Howard, D. & Soll, R. F. Neurodevelopmental outcome of infants resuscitated with air or 100% oxygen: a systematic review and meta-analysis. Neonatology 102, 98–103 (2012).
Wright, K. W. et al. A physiologic reduced oxygen protocol decreases the incidence of threshold retinopathy of prematurity. Trans. Am. Ophthalmol. Soc. 104, 78–84 (2006).
Askie, L. M. et al. NeOProM: Neonatal Oxygenation Prospective Meta-analysis collaboration study protocol. BMC Pediatr. 11, 6 (2011).
Carlo, W. A. et al. Target ranges of oxygen saturation in extremely preterm infants. N. Eng. J. Med. 362, 1959–1969 (2010).
Schmidt, B. et al. Effects of targeting higher vs lower arterial oxygen saturations on death or disability in extremely preterm infants: a randomized clinical trial. JAMA 309, 2111–2120 (2013).
BOOST II United Kingdom Collaborative Group, BOOST II Australia Collaborative Group, BOOST II New Zealand Collaborative Group, Stenson, B. J. et al. Oxygen saturation and outcomes in preterm infants. N. Engl. J. Med 368, 2094–2104 (2013).
Saugstad, O. D. & Aune, D. Optimal oxygenation of extremely low birth weight infants: a meta-analysis and systematic review of the oxygen saturation target studies. Neonatology 105, 55–63 (2014).
Manja, V., Lakshminrusimha, S. & Cook, D. J. Oxygen saturation target range for extremely preterm infants: a systematic review and meta-analysis. JAMA Pediatr. 169, 332–340 (2015); erratum 169, 507 (2015).
Manja, V., Saugstad, O. D. & Lakshminrusimha, S. Oxygen saturation targets in preterm infants and outcomes at 18–24 months: a systematic review. Pediatrics 139, e20161609 (2017).
Askie, L. M. et al. Effects of targeting lower versus higher arterial oxygen saturations on death or disability in preterm infants. Cochrane Database Syst. Rev. 4, CD011190 (2017).
Askie, L. M. et al. Association between oxygen saturation targeting and death or disability in extremely preterm infants in the neonatal oxygenation prosepctive meta-analysis collaboration. JAMA 319, 2190–2201 (2018).
Singhal, N. et al. Helping babies breathe: global neonatal resuscitation program development and formative educational evaluation. Resuscitation 83, 90–96 (2012).
Chu, D. K. et al. Mortality and morbidity in acutely ill adults treated with liberal versus conservative oxygen therapy (IOTA): a systematic review and meta-analysis. Lancet 391, 1693–1705 (2018).
Chandrasekharan, P. et al. Effect of various inspired oxygen concentrations on pulmonary and systemic hemodynamics and oxygenation during resuscitation in a transitioning preterm model. Pediatr. Res. in (2018) https://doi.org/10.1038/s41390-018-0085-x.
Crawshaw, J. R. et al. Laryngeal closure impedes non-invasive ventilation at birth. Arch. Dis. Child. Fetal Neonatal Ed. 103, F112–F119 (2018).
Saugstad, O. D. Oxygenation of the immature infant: a commentary and recommendations for oxygen saturation targets and alarm limits. Neonatology 114, 69–75 (2018).
Bhandari, V. Hyperoxia-derived lung damage in preterm infants. Semin. Fetal Neonatal Med. 15, 223–229 (2010).
Sweet, D. G. et al. European Consensus Guidelines on the Management of Respiratory Distress Syndrome—2016 update. Neonatology 111, 107–125 (2017).
Cummings, J. J. & Polin, R. A., Committee on Fetus and Newborn. Oxygen targeting in extremely low birth weight infants. Pediatrics 138, pii: e20161576 (2016).
Acknowledgements
This work was supported by Health South East Trust, Norway 2013120. Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD), Bethesda MD, USA 7R01HD072929-07—Health Research Institute Carlos III; Spanish Ministry of Education and Science FIS Grant PI17/0131.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Saugstad, O.D., Oei, JL., Lakshminrusimha, S. et al. Oxygen therapy of the newborn from molecular understanding to clinical practice. Pediatr Res 85, 20–29 (2019). https://doi.org/10.1038/s41390-018-0176-8
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41390-018-0176-8
This article is cited by
-
Neonatal resuscitation with continuous chest compressions and high frequency percussive ventilation in preterm lambs
Pediatric Research (2024)
-
Neonatal Resuscitation in Delivery Room: Current Trends and Guidelines in 2022
Current Anesthesiology Reports (2023)
-
Splanchnic oxygen saturation during reoxygenation with 21% or 100% O2 in newborn piglets
Pediatric Research (2022)
-
TRAIL protects the immature lung from hyperoxic injury
Cell Death & Disease (2022)
-
Semi-mechanistic Modeling of Hypoxanthine, Xanthine, and Uric Acid Metabolism in Asphyxiated Neonates
Clinical Pharmacokinetics (2022)
