
Abstract
Introduction
Multiple systematic reviews have investigated the relation between socioeconomic position (SEP) and body mass index (BMI) throughout the life course. However, BMI does not capture quantity and distribution of fat and muscle, which are better indicators of obesity than BMI, and have been independently linked to adverse health outcomes. Less is known about the relation between SEP and body composition, and the literature has not been reviewed. We therefore systematically reviewed the literature on the association between life course SEP and body composition in adulthood.
Methods
A protocol was registered on PROSPERO (CRD42019119937), and the review followed PRISMA guidelines. An electronic search of three databases (MEDLINE, Embase Classic + Embase and SPORTDiscus) was conducted. Original studies in the English language were included that examine the association between any recognised measure of SEP at any age and body composition (fat mass, fat-free mass, ratio and distribution) in adulthood, measured using a direct technique, i.e., not an anthropometric measure. A narrative synthesis was conducted.
Results
A total of 47 papers were included in the final review, none were from low-income countries (LICs). Greater advantage in childhood and adulthood was associated with lower fat levels in high-income countries (HICs). Associations in the opposite direction were found exclusively in middle-income countries (MICs). No studies in MICs reported associations for childhood SEP. For measures of lean mass, the majority of papers reported no association, or greater advantage in adulthood associated with higher lean mass, with little variation between HICs and MICs. Associations in HICs are more often observed in women than men.
Conclusion
The results indicate that fat measures follow similar patterns to those seen for BMI, and that women in HICs are more likely to experience inequalities in both fat and lean measures. Further research in LICs and MICs is needed.
Similar content being viewed by others

Introduction
Socioeconomic position (SEP) across the life course has been repeatedly linked with obesity in high-income countries (HICs) and has been the subject of multiple systematic reviews [1,2,3,4,5,6]. These reviews demonstrate predominantly that, among adults in HICs, advantaged SEP in both childhood and adulthood is associated with lower levels of obesity defined by anthropometric measures such as body mass index (BMI), with stronger associations in women [1,2,3, 5, 6]. In studies from middle-income countries (MICs), systematic reviews have generally found associations in the same direction among women, but less consistent associations among men. In those from low-income countries (LICs) associations have been found in the opposite direction such that more advantaged SEP is associated with higher rates of obesity [7].
SEP is an umbrella term for multiple measures of social and economic circumstances that influence an individual’s position in society [8]. Different measures of SEP capture different aspects of these circumstances and may relate to health outcomes in different ways, thus providing information about the underlying pathways. Education is a proxy for health literacy; occupational social class represents working conditions and social standing; income is a direct measure of material resources; and area-level SEP captures elements of the broader environment. However, in LICs and MICs a composite measure of material living standards may better capture circumstances than education, occupation or income.
Although the literature linking SEP and BMI has been extensively reviewed, the evidence linking SEP and body composition has not. BMI is a measure of weight for height that does not distinguish fat mass (FM) from fat-free mass (FFM). Measures of body composition provide estimates of the proportion of FM to FFM, including in some cases lean mass (LM)—a measure of FFM most often captured through dual x-ray absorptiometry (DXA), which excludes bone mass—and can inform about the location of FM [9].
A lower proportion of FM and higher proportion of FFM has been shown to be associated with a reduced risk of cardiovascular disease and total mortality [10, 11]. Distribution of FM is also associated with cardiovascular and metabolic disease, with higher central adiposity and higher android-to-gynoid FM ratio shown to increase risk [12,13,14,15]. In addition, FFM plays a role in development of insulin sensitivity, with skeletal muscle being a key sight of glucose uptake [16]. Having higher levels of FFM therefore has the potential to reduce and delay the onset of metabolic disorders [17, 18]. LM is also important for maintaining musculoskeletal health in older age, with sarcopenia characterised by loss of skeletal muscle and muscle strength. Lower levels of LM also increases risk of osteoporosis as LM is positively associated with bone mineral density [19]. If inequalities in FM are similar or stronger than the inequalities in BMI, while greater advantage is associated with higher LM, then the impact of inequalities in adiposity on health may be underestimated if based on BMI alone.
We aimed to perform a systematic review of the literature to assess the association between SEP and measures of body composition in the general population. In addition, we aimed to assess differences in socioeconomic inequalities in body composition by birth cohort, sex and by SEP measure. In this paper we focus on associations between (a) SEP measured in childhood and adult body composition and (b) SEP in adulthood and adult body composition.
Methods
The protocol for this review was registered with the PROSPERO database (CRD42019119937) and has been carried out using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) checklist (Supplementary File 1). Full details of the methods can be found in the published protocol [20].
Eligibility
Peer-reviewed papers in the English language reporting an association between any recognised indicator of SEP (e.g., income, education, overcrowding, area-level deprivation) and a direct measure of body composition (i.e., measured using bioelectrical impedance analysis (BIA) or DXA) were included. Observational studies including samples from the general population were included where body composition was measured at the same, or later, time point to SEP. Body composition was defined as any measurement related to total FM and FFM, location of FM and FFM or any proportion or ratio of measures of FM and FFM. Studies based on anthropometric measurements such as BMI or abdominal circumference were excluded.
Search strategy
An electronic search of three databases (MEDLINE and Embase Classic + Embase using OvidSP as the interface, SPORTDiscus using EBSCO as the interface) was conducted by CBS to identify appropriate studies published from the earliest entry available for each database (MEDLINE: 1879; Embase Classic + Embase: 1947; SPORTDiscus: 1892) up until the 30th January 2019. The search terms used are shown in Table 1. The search was broad and included body composition in childhood as well as in adulthood. The results of the search were de-duplicated and stored in the reference manager, Endnote. This database was exported to Rayyan QCRI [21] to conduct screening. Titles and abstracts were screened for eligibility and full texts of the eligible papers were subsequently screened by CBS, AG, and JMB. Reasons for exclusion of studies were recorded at the full-text screening stage. The reference list of eligible full texts was screened to identify additional papers.
Extraction and quality assessment
Relevant data that examined the association between at least one measure of SEP and a measure of body composition were double extracted by CBS, AG, JMB, MA and EW using a data extraction form. Data extracted included citation details (author, title, paper, publication year, publication type), study details (cohort or sample description, study design, country, participant numbers), participant details (birth year or age or participants, sex of participants), exposure and outcome details (type of SEP and body composition variables presented, age variables recorded, how the variables were ascertained and measured) and statistical methods and information on adjustment for potential confounders and mediators. All available statistics relating to the association under study were extracted, along with statements of direction in text where statistics were not presented.
Assessment of study quality was carried out, using an amended version of the Newcastle-Ottawa Quality Assessment scale [22]. Quality assessment was used to inform on the variability of quality across the papers and potential bias arising, and not to guide the inclusion of results into the review. The original quality assessment form was amended during the review to account for the large number of cross-sectional studies and the variability in statistical reporting (questions 3bi, 3bii and 4—Supplementary File 2). Google Form was used to aid extraction and WebPlotDigitizer (https://automeris.io/WebPlotDigitizer/) was used to extract data that were only presented in graphs. Two reviewers (CBS and either AG, JMB, MA or EW) worked independently to complete every stage of the screening, extraction and quality assessment process. Disagreements were resolved through discussion.
Synthesis
Due to the considerable variability in analytic methods and presentation of results, a meta-analysis was not possible, and nor was it possible to use a funnel plot to assess publication bias. A narrative synthesis was conducted, guided by the Economic and Social Research Council Methods Programme guidelines [23]. Synthesis has been conducted according to the groupings of: (a) childhood SEP and adult body composition and (b) adult SEP and adult body composition.
The majority of papers presented multiple associations. Therefore, similar to methods adopted by McLaren [3] and Ball and Crawford [24], the individual associations between each different SEP and body composition variable, rather than individual papers, were considered as the units of analysis.
Associations were classified into positive associations (those reporting greater socioeconomic advantage associated with higher body composition measure), inverse association (those reporting greater socioeconomic advantages associated with lower body composition measures), non-linear (e.g curvilinear or heterogenous) association and no association. Associations were assigned to groups according to the effect estimates and 95% confidence intervals. Where this information was missing, trends identified in descriptive data, P values or statements of direction were used.
Where associations were provided for multiple subgroups, primary results selected for summary were those in men and women included together. As analysis by sex was pre-specified in the protocol, where papers only reported in males and females separately, both associations were included in the primary summary of results.
Heterogeneity was explored by body composition measure (FM, FFM, ratio and distribution), birth cohort, sex and SEP measure. On extraction it became clear that country income level should also be considered as sources of heterogeneity. Studies were categorised into HICs, upper middle- and lower middle-income countries, according to the World Bank classification in 2019 [25]. Those papers from ‘upper middle’ and ‘lower middle’ income countries will all be referred to as ‘middle-income countries’ (MIC).
Results
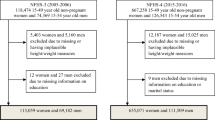
Figure 1 shows the study selection process, as outlined in the PRISMA flowchart. Searching the databases for potential papers returned 7145 papers, with 5725 once duplicates were removed. Title and abstract screening resulted in 513 papers, with 91 papers remaining following full-text screening. Searching the reference lists for additional papers returned 3, bring the total included papers to 94. Of those, 47 investigated either adult or childhood SEP and adult body composition and are reported on here [26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72]. Descriptive results and quality assessment for the included papers are shown in Table 2. The majority (n = 27) of papers were rated as medium quality, 14 were rated as low quality, and 6 papers were rated as high quality.

Numbers given for reasons for exclusion during full-text screening stage equal more than the total excluded at this stage (n = 422), because reasons for exclusion are not mutually exclusive.
Characteristics of included studies
There were 40 distinct study samples across the 47 papers, published between 1995 and 2018. The Study of Women’s Health Across the Nation (SWAN) was used in four papers. There were four other samples used in two papers each: Health 2000 Survey; Malmo ̈ Diet and Cancer study; The Korea National Health and Nutrition Examination Survey (KHANES); and the New England Family Study was used in addition to the Longitudinal Effects of Ageing on Perinatal (LEAP) project, which is a sub-set of the New England Family Study. The majority of papers were from Europe (n = 18, 38%) or North America (n = 14, 30%). There were 13 studies conducted in samples from the US and four each in Finland and the UK. Eleven papers were in MICs. No studies from LICs were identified. Sample sizes ranged from 86 to 162,691, with the interquartile ranges between 309 and 3285. One paper did not report sample size.
There was substantial variability in body composition measures used, especially for fat-free measures, but also terminology used to describe them. The different measures identified, and the definitions adopted in this review are shown in Supplementary Table 1. For the purposes of the review, fat-free measure is a general term that will refer to all measures of body composition that are not FM measures. Lean body mass (LBM) is a fat-free measure equivalent to FFM plus essential fats found in the nervous system, cell membranes and bone marrow [73]. This is different to the measure of LM, which is equivalent to FFM minus bone mass, and more closely captures what is colloquially thought of as ‘muscle’ [74]. LBM and FFM are most often measured through BIA, as it is not able to separate bone mass and lean tissue, whilst LM is most often measured through DXA as it uses a three-compartment model that splits the body into fat, lean and bone mass [74]. Appendicular skeletal muscle (ASM) is included as a total body fat-free measure, as muscle mass in the limbs represents 75% of total skeletal muscle mass (SMM) [74, 75]. The majority of papers used DXA to measure body composition (n = 22), with BIA the next most common method (n = 20). The remaining studies used underwater densitometry (n = 1), CT scans (n = 4), deuterium oxide dilution solution (total body water) (n = 1) and abdominal ultrasonography (n = 1). Two papers used more than one method.
Fat measures were considerably more frequently reported (in 30 papers) than fat-free measures (in 20 papers), with percentage fat mass (FM%) the most frequently analysed (reported in 21 papers). LM was the most frequently used fat-free measure (in 8 papers).
The most frequently reported SEP variable was education (in 32 papers). ‘Composite SEP’, which we define as any index combining two or more individual-level SEP indicators, was used the same number of times as income (10 papers). Occupational social class was used in 7 papers, and area-level SEP, which we define as any measure that captures the deprivation of an area, in 5 papers.
The majority of papers were conducted in adults over 45 or in samples with a mean age over 45 (n = 29). There were 13 studies where participants were either aged over 60 or had a mean age of 60+. Few cohort studies provided birth year (n = 5), or information from which this could be calculated, preventing assessment of secular differences in body composition by birth cohort as specified in the protocol.
Childhood socioeconomic position and adult body composition
There were seven papers investigating the associations between childhood SEP and adult body composition. We were unable to assess heterogeneity due to the small number of papers, all of which were conducted in HICs. Results are summarised in Table 3.
Total body fat measures
Five papers reported on SEP in childhood and measures of fat in adulthood, testing eight different associations. In four papers, testing seven associations, greater socioeconomic advantage in childhood was associated with lower FM index (FMI) or FM% in adulthood [33, 52, 54, 72]. One study reported that the association was somewhat explained by own SEP in adulthood [33], with the others not assessing this. The fifth paper found father’s education not to be directly related to a standardised FM% score (z-FM%) at age 32, but reported an indirect relation through own education and current physical activity levels [61].
Total body fat-free measures
Three papers reported on SEP in childhood and fat-free measures in adulthood, testing five associations. Two papers found evidence of positive associations, with greater socioeconomic advantage in childhood being related to higher LM [61] and higher ASM index (ASMI) [33] in adulthood. One of these presented only sex-stratified analyses and found the association with ASMI to be stronger in males before adjusting for FMI, whilst stronger in females after the adjustment for FMI [33]. The final paper reported no association with LM [72].
Ratio and distribution measures
Three associations across three papers investigated central fat. One found an inverse association in females only [26], one a curvilinear relation, where those in the medium third of android fat had the most advantaged SEP in childhood [56]. The final paper found no association [61].
Two papers reported on android-to-gynoid ratio, presenting four associations. Both papers found greater socioeconomic advantage in childhood to be associated with lower android-to-gynoid ratio. In one paper this was only the case in females [26], whilst in the other, the association was stronger in females than males [33]. The latter paper found that the association remained with adjustment for SEP in adulthood [33].
Adult socioeconomic predictors of adult body composition
There were 46 papers reporting on the association between SEP in adulthood and body composition in adulthood. Sixteen reported only in females, one only in males and the rest in both males and females.
Total body fat measures
Table 4 provides a summary of the patterns reported for each fat measure. There were 75 associations tested across 30 papers. Nearly half of associations between SEP and fat measures reported were inverse (44%). Similar numbers reported non-linear (17%), made up of heterogeneous and curvilinear associations, as reported positive (11%) patterning, and almost a third of papers reported no association (28%). There were clear differences between findings in HICs and MICs. In HICs (n = 54), associations were predominantly inverse (59%) with no positive associations observed. In MICs (n = 21), most studies found positive associations (38%) or no association (43%), with only 5% reporting inverse associations.
FM% was used 44 times across 21 papers, FMI was used 19 times across 10 papers and FM 12 times across 10 papers. Each fat measure showed predominantly inverse associations, and this was driven by inverse associations in HICS. In HICs, inverse associations were reported more frequently for FM (78%) compared to FM% (58%) and FMI (50%). Non-linear associations (including both heterogeneous and curvilinear) were more frequently reported for FMI (43%) than for other measures. In MICs, FM% and FMI predominantly showed positive associations (38% and 40%, respectively) and no association (38% and 60%, respectively). FM was used only three times in MICs with all patterns of association being different.
For education, the most commonly studied SEP measure, 12 of 29 associations showed an inverse association with a measure of fat (41%), again driven by findings in HICS. In MICs, education showed predominantly no association (six out of nine associations). Inverse associations were predominantly observed for occupational social class (six out of ten), but the measure was used almost exclusively in HICs. For area-level SEP, which was used only in HICs, predominantly inverse associations (six out of eight) were reported. In contrast, four out of nine associations with composite SEP showed positive associations. All of those reporting positive associations were conducted in MICs. Four of the remaining five studies that showed either inverse or no association were conducted in HICs. Non-linear associations were most frequently reported in studies investigating income in both HICs and MICs (in two out of three associations in both).
In studies that presented sex-stratified or sex-specific analysis (66 associations across 22 papers), inverse associations were reported over twice as frequently in females (77%) compared to males (33%) in HICs. There was a higher proportion of non-linear associations in males (29%) compared to females (14%) (Supplementary Fig. 1). In studies from MICs, no association was more commonly reported in women (57%) compared with men (44%). Positive associations were more commonly reported in men (55%) than women (21%).
Total body fat-free measures
Table 5 provides a summary of the patterns identified for each of the different fat-free measures. There were 44 associations tested across 19 papers. The majority found no association between SEP and fat-free measures (55%), whilst 32% found evidence of positive associations, 7% found inverse and 7% found non-linear associations. More associations were tested in HICs (30 association across 14 papers) compared to MICs (14 associations across 5 papers), and patterns of association were similar in both settings.
LM was used 10 times across 8 papers while FFM, ASM and ASMI were used 9–11 times each across 3–6 papers. Percentage LM (LM %), LM index (LMI) and FFM index (FFMI) were used in one paper each. FFM showed a greater frequency of positive associations (50%) while for all other measures no association was most commonly observed. ASMI reported a higher number of positive associations (36%) compared to LM and ASM. LM and ASM found positive associations in 10–30% of associations. Inverse and non-linear patterns were reported in approximately 0–20% of the associations for LM, FFM, ASM and ASMI.
For measures that include bone (FFM and LBM) (n = 11), there was a higher proportion of positive associations reported (45%) compared to measures that did not include bone, i.e., LM (n = 33, 27%). There was little difference in the distribution of associations between those that used index or percentage measures compared to those that used raw measures. Two papers made additional adjustments [33, 66], for either FM or body size that resulted in associations reversing in direction to become positive, or increasing in strength.
For all measures of SEP, no associations were most frequently observed. Positive associations were more frequently reported for education (35% of 23 associations) and income (29% of 7) compared with social class (17% of 6). Income showed a higher percentage of non-linear associations (29%) and a lower number of no associations (43%) compared to all other SEP measures. Composite measures of SEP were used twice and area-level SEP once.
Among studies that presented sex-specific or sex-stratified analysis (46 associations across 16 papers), there was greater variability in the patterns of associations observed among women in HICs compared with men in both HICs and MICs and women in MICs (Supplementary Fig. 2). There were a higher percentage of positive (40%) and inverse (16%) relationships, and a lower percentage reporting no association (40%). Among men and women in MICs and men in HICs, there was more consistent evidence of no association across the studies (70–73%).
Ratio and distribution measures
Thirteen papers reported on the association between SEP and ratio or distribution measures (Supplementary Table 2). Only two were from MICs preventing comparison of differences by the income level of the country.
There were 14 associations across ten papers that investigated the association between SEP and a measure of central fat. Four papers used the same all-female sample (SWAN) [40, 44, 55, 58], and one additional paper also tested the association in women only [50]. The majority of associations (9 out of 14, 64%) reported that greater socioeconomic advantage was associated with lower central adiposity. For education, five out of the seven associations found evidence that lower education level was associated with greater central fat, whilst two out of the three papers using income found some evidence of higher central fat among those with lower income.
Two papers used a distribution measure other than central fat. One found women who engaged in more labour-intensive occupations had lower leg FM [50]. The other found no association between education and the distribution of either upper or lower SMM [32].
Six associations across three papers reported on ratios, one conducted in an all-female population. One paper, which tested the association using education, occupational social class and income, found that greater socioeconomic advantage was related to a lower android-to-gynoid ratio [33]. Men showed a stronger association for education compared to other SEP measures, and also a stronger association than that observed in women when measured by education, whilst a heterogeneous association was observed for occupational social class [33]. Another paper found that those with higher education level were more likely to have a normal compared to high ratio of fat to LM, whilst employment was related to the ratio in a non-linear fashion [62]. In the third study no association was found between income and the ratios of central fat types in females [44].
Discussion
This systematic review finds evidence of socioeconomic inequalities in body composition, although the direction and strength of these inequalities varies by measure of SEP, measure of body composition, sex and economic development of the country of study. The review generally finds evidence of associations between more advantaged SEP in both childhood and adulthood and lower levels of total body FM, particularly in HICs, irrespective of which SEP or FM measure is used. Such associations were more frequently observed among females than males. In MICs, the majority of studies showed positive or no association for fat measures. For fat-free measures, findings were more mixed, with the majority of papers reporting no association or greater socioeconomic advantage being associated with greater FFM. There is some evidence of similar positive associations between childhood SEP and adult fat-free measures in HICs, although the small number of studies means caution is required in interpretation of these findings. No studies reported associations for childhood SEP and adult body composition in MICs, and no studies conducted in LICs were identified.
Our findings for adult SEP and fat measures are consistent with previous systematic reviews, showing predominantly inverse associations for anthropometric measures of adiposity such as BMI and waist circumference in HICs, especially among women [2, 3]. Also similar to reviews based on BMI and other anthropometric measures [2, 3, 7], we find positive associations to only be observed in MICs. We also found SEP to be inversely related to measures of central fat, whilst evidence for other measures of fat distribution is too sparse to draw conclusions [3].
Our findings in relation to childhood SEP and adult body fat measures are also similar to those for BMI that find mostly inverse associations [4, 6]. However, the small number of studies means that conclusions regarding differences between males and females are not possible. No studies reported on the association in MICs, and it was therefore not possible to compare findings between MICs and HICs. To the best of our knowledge, no systematic reviews have previously considered social inequalities in measures of FFM. One review did find more consistent evidence than our review that advantaged SEP in childhood is related to better physical capability in adulthood [76], with such measures of physical capability (i.e., grip strength) being correlated with muscle mass and strength [77, 78]. Few studies tested if associations with childhood SEP were independent of adult SEP, which has implications for the lasting role of early development in nutrition and physical activity patterns [79, 80]. Consideration of both child and adult SEP would also allow investigation of latency, trajectory or accumulation effects of SEP across the life course and help to identify the best time to intervene to prevent inequalities in body composition.
A range of measures of FM and FFM were used across the studies, and the majority of papers used a raw measure of mass, rather than measures indexed to height. However, indexed measures of FM and FFM are considered to be more appropriate as they can be interpreted independently of the other, and account for the contribution of height to mass [81, 82]. We found stronger evidence of inverse association for fat when using the raw measure, rather than indexed measures, indicating less evidence of inequalities in fat when appropriately accounting for height.
For fat-free measures, there was also variation in what composition of FFM was captured. Measures attained through BIA do not separate lean from bone mass, while use of DXA does allow separation of bone. Studies that used measures that included bone mass showed a higher proportion of positive associations compared to those that did not, indicating that bone may be contributing to observed inequalities in FFM. In addition, there were inconsistencies in the adjustment of LM for FM. Previous research has shown that adaptive increases in LM occur with increases in FM, highlighting a need to consider adjustment for FM [83,84,85]. In this review, adjusting FFM measures for FM or body size resulted in the direction of association reversing, becoming positive [33] or existing positive associations increasing in strength [66].
Differences observed in associations according to SEP measures could largely be explained by differences between HICs and MICs. Both occupational social class and area-level measures of SEP were predominantly used in HICs and also reported the highest proportion of inverse relations with total FM. Composite measures of SEP were more frequently used in MICs and reported a higher proportion of positive associations with total FM. Income was the only measure used in HICs that showed a low number of inverse associations and a high number of non-linear associations for FM measures. Income is considered a direct measure of material resources and is most prone to short-term change [8], which may explain the greater observed heterogeneity. Education is a more stable measure of SEP that captures early life conditions whilst also a determinant of later life SEP and reflects knowledge assets and health literacy as well as health behaviours [8]. Similarly, occupational social class is a good overall measure of SEP as it captures aspects of an individual’s education, income, social standing in addition to their occupation [8]. It is possible that area-level SEP may also be a particularly strong predictor of inverse associations in HICs due to the close link with obesogenic elements in the environment [86, 87].
Differences in findings between HICs and MICs, particularly for FM, may be, at least in part, explained by the nutrition transition. Consumption of energy-dense food that is high in fats and sugars is related to higher adiposity, whilst protein and micronutrients are required for lean tissue development. As countries develop, food becomes more abundant and accessible and, in particular, more frequently characterised by high-energy-dense and calorific foods [88]. In MICs, those with greater socioeconomic advantage have greater food security and access to the high-energy-dense foods, and more calorific diets [89]. In HICs, high-energy-dense and calorific foods tend to be cheaper and consumed more frequently among individuals of less-advantaged SEP [90, 91].
Physical activity is an important determinant of LM development and maintenance, as well as being important for maintenance of healthy adiposity levels. Levels of physical activity between MICs and HICs may be affected by different timings in the onset of the obesogenic environment and nutrition transition [88], which is in part characterised by a shift from more labour-intensive lifestyles to more sedentary lifestyles [92]. Although those in less-advantaged socioeconomic circumstances are more likely to work manual jobs, and therefore have higher occupational physical activity, those in positions of socioeconomic advantage in HICs tend to participate in more leisure time physical activity compared to those in less-advantaged positions [93, 94]. In particular, there is evidence of greater vigorous activity from leisure time activities among those in more advantaged positions in HICs [94]. This, combined with differences in nutrition, may explain the existence of inverse associations for fat measures and positive associations for lean measures in HICs, where those with low fat are also leaner. The existence of predominantly positive associations between SEP and fat measures and to a lesser extent in lean measures in MICs may reflect that those in less-advantaged SEPs with low fat may be malnourished, and therefore also have less muscle.
Differences in association by sex observed for both lean and fat measures, with women in HICs most likely to experience inequalities in lean and fat measures compared to other groups, may be explained by increases in gross national product shifting the burden of obesity to those of a less-advantaged position within society, affecting women first [95]. This may be a result of the greater pressures of weight-related ideals faced by women, which are easier to maintain in a position of advantage [96].
Based on previous evidence using anthropometric measures, it is possible that there are differences in inequality according to ethnicity. Among HICs, minority ethnic groups tend to have higher prevalence of obesity compared to the majority [97] and are more likely to be living in disadvantaged circumstances [98]. In the US, whilst a positive association among income and obesity is observed among African American and Caribbean Black men, an inverse association is observed for women [99]. In the UK, there is evidence that increased acculturation results in convergence in obesity among minority ethnic groups, all except for Black Caribbean groups [100]. Few studies in the review considered analyses stratified by ethnicity and further research is needed to understand the complexity of ethnic differences in body composition inequalities in both HICs and MICs, which are likely to be complex, influenced by cultural factors, migration status and structural racism.
Strengths and limitations
This review was registered with PROSPERO and has been carried out according to the published protocol [20]. Bias in the process was minimised by two independently working reviewers conducting each stage of the review, including selection of studies and extraction of data.
The review has an inclusion and exclusion criteria capturing a broad range of evidence, thereby reducing selection bias. However, this resulted in large heterogeneity among the included papers in both exposures, outcomes and statistical reporting with multiple associations often being tested in a single paper. This variation in statistical analyses prevented a meta-analysis from being conducted. Our narrative review followed previous similar reviews in using the association, rather than the paper, as the unit of analysis. However, this meant that in some cases one paper contributed multiple associations to the overall percentages. The same data sets were also used in multiple papers.
We assigned associations to the four categories of association using the effect estimates and confidence intervals, which convey more about the direction and strength of effect, and the accuracy of these estimates [101, 102]. This is to overcome the limitations where there has been a heavy reliance on P values to convey statistical results [102, 103]. However, many papers included did rely on P values in the reporting of their results and thus there may have been selective reporting of significant findings.
There is inconsistency in the literature relating to the terminology used to describe FFM [104], with a small number of papers using incorrect terminology based on the description of their body composition measure. Despite best efforts to ensure comparability by applying standard definitions of fat-free measures across the review, some papers did not provide enough clarity on the measures used to do this confidently, i.e., such as clearly stating if bone is included or excluded in estimates of FFM. This highlights the need for consistent definitions to be applied and used across the body composition literature, and for authors to provide clarity on the measures used, specifically ensuring use of the correct term if bone is included (FFM or LBM) or excluded (LM) and using appropriate and consistent terminology throughout when measures have been indexed or converted to percentages. We were unable to assess the differences in association by birth year due to lack of information. We were also not able to assess differences between childhood SEP and adulthood body composition by age and sex and income level of country due to the small number of papers reporting such associations.
Implications and conclusion
The results of this review indicate that inequalities in BMI are likely to capture inequalities in FM in adults, but not inequalities in FFM for which we find weak evidence of associations. Compared to total body FM, few studies looked at measures of FFM that exclude bone and that are indexed to height. There is a need for research to adopt better and more consistent measures of FFM that account for the contribution of height and bone, in order to better understand inequalities in LM. This may be particularly important for research in older age, as muscle mass becomes increasingly important for functional outcomes.
Few studies investigated the association between childhood SEP and adulthood body composition, and none were in MICs. Childhood SEP has previously been shown to be a strong predictor of BMI in adulthood, and further research is needed to understand how disadvantage may accumulate over the life course and influence body composition in adulthood. No data were available from LICs across the whole review, an area that warrants further research. Only a small number of studies provided birth years of participants, preventing investigation of secular differences in inequalities in body composition in the context of persisting inequalities in BMI. The majority of studies were conducted in those aged 40 and above, with fewer studies looking at young to mid-adult life, preventing full assessment of difference in body composition across the adult life course. Follow-up of cohorts across adulthood are needed to identify if there are either secular changes in body composition or age-related changes in body composition, or the existence of both simultaneously and how this might influence social inequalities.
The differences in associations between SEP and FM between HICs and MICs indicate emerging and, in some cases, reversing inequalities in body composition as countries go through the nutrition transition and with the onset of the obesogenic environment. These findings suggest that action is required in MICs to mitigate the negative effects of this transition. Mitigating action is likely needed in LICs also, which are expected to be further behind in the nutrition transition than MICs, and so information in LICs is needed. In particular, efforts should continue to focus on reducing the abundance of cheap energy-dense food in poorer communities and ensure access to healthy and nutritious food across SEP groups, as a way to combat inequalities in FM. Attention should also be paid to promotion of physical activity to ensure healthy levels of FFM across all SEP groups, and especially into older age where muscle mass may be more important for metabolic and functional outcomes.
References
Newton S, Braithwaite D, Akinyemiju TF. Socio-economic status over the life course and obesity: systematic review and meta-analysis. PLoS One. 2017;12:5.
Sobal J, Stunkard AJ. Socioeconomic status and obesity: a review of the literature. Psychol Bull. 1989;105:260–75.
McLaren L. Socioeconomic status and obesity. Epidemiol Rev. 2007;29:29–48.
Parsons TJ, Power C, Logan S, Summerbell CD. Childhood predictors of adult obesity: a systematic review. Int J Obes. 1999;23:S1–107.
Gonzalez D, Nazmi A, Victora CG. Childhood poverty and abdominal obesity in adulthood: a systematic review. Cad Saude Publica. 2009;25:S427–40.
Senese LC, Almeida ND, Fath AK, Smith BT, Loucks EB. Associations between childhood socioeconomic position and adulthood obesity. Epidemiol Rev. 2009;31:21–51.
Dinsa GD, Goryakin Y, Fumagalli E, Suhrcke M. Obesity and socioeconomic status in developing countries: a systematic review. Obes Rev. 2012;13:1067–79.
Galobardes B, Shaw M, Lawlor DA, Lynch JW, Davey, Smith G. Indicators of socioeconomic position (part 1). J Epidemiol Community Health. 2006;60:7–12.
Wells JC, Fewtrell MS. Measuring body composition. Arch Dis Child. 2006;91:612–7.
Srikanthan P, Horwich TB, Tseng CH. Relation of muscle mass and fat mass to cardiovascular disease mortality. Am J Cardiol. 2016;117:1355–60.
Medina-Inojosa JR, Somers VK, Thomas RJ, Jean N, Jenkins SM, Gomez-Ibarra MA, et al. Association between adiposity and lean mass with long-term cardiovascular events in patients with coronary artery disease: no paradox. J Am Heart Assoc. 2018;7:10.
Kang SM, Yoon JW, Ahn HY, Kim SY, Lee KH, Shin H, et al. Android fat depot is more closely associated with metabolic syndrome than abdominal visceral fat in elderly people. PLoS One. 2011;6:11.
Samsell L, Regier M, Walton C, Cottrell L. Importance of android/gynoid fat ratio in predicting metabolic and cardiovascular disease risk in normal weight as well as overweight and obese children. J Obes. 2014;2014:846578.
Vasan SK, Osmond C, Canoy D, Christodoulides C, Neville MJ, Di Gravio C, et al. Comparison of regional fat measurements by dual-energy X-ray absorptiometry and conventional anthropometry and their association with markers of diabetes and cardiovascular disease risk. Int J Obes. 2018;42:850–7.
Coutinho T, Goel K, Corrêa de Sá D, Kragelund C, Kanaya AM, Zeller M, et al. Central obesity and survival in subjects with coronary artery disease: a systematic review of the literature and collaborative analysis with individual subject data. J Am Coll Cardiol. 2011;57:1877–86.
Stanford KI, Goodyear LJ. Exercise and type 2 diabetes: molecular mechanisms regulating glucose uptake in skeletal muscle. Adv Physiol Educ. 2014;38:308–14.
Takamura T, Kita Y, Nakagen M, Sakurai M, Isobe Y, Takeshita Y, et al. Weight-adjusted lean body mass and calf circumference are protective against obesity-associated insulin resistance and metabolic abnormalities. Heliyon. 2017;3:e00347.
Yeung CHC, Yeung SLA, Fong SSM, Schooling CM. Lean mass, grip strength and risk of type 2 diabetes: a bi-directional Mendelian randomisation study. Diabetologia. 2019;62:789–99.
Ho-Pham LT, Nguyen UDT, Nguyen TV, Association. Between lean mass, fat mass, and bone mineral density: a meta-analysis. J Clin Endocrinol Metab. 2014;99:30–8.
Bridger Staatz C, Kelly Y, Lacey R, Hardy R. Socioeconomic position and body composition across the life course: a systematic review protocol. Syst Rev. 2019;8:263.
Ouzzani M, Hammady H, Fedorowicz Z, Elmagarmid A. Rayyan—a web and mobile app for systematic reviews. Syst Rev. 2016;5:210.
Wells GSB, O’connell D, Peterson J, Welch V, Losos M, Tugwell P. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. 2000.
Popay J, Roberts H, Sowden A, Petticrew M, Arai L, Rodgers M, et al. Guidance on the conduct of narrative synthesis in systematic reviews. Lancaster: Lancaster University; 2006.
Ball K, Crawford D. Socioeconomic status and weight change in adults: a review. Soc Sci Med. 2005;60:1987–2010.
The World Bank. World Bank Country and Lending Groups: The World Bank. 2019. https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groups. Accessed date 13 Nov. 2019.
Agha G, Buka S, Eaton C, Houseman EA, Kelsey K, Loucks E. Prenatal socioeconomic index in relation to adulthood fat mass and fat distribution. Am J Epidemiol. 2013;11:S10. Abstract 037-S.
Al-Qaoud TM, Nitsch D, Wells J, Witte DR, Brunner EJ. Socioeconomic status and reduced kidney function in the Whitehall II Study: role of obesity and metabolic syndrome. Am J Kidney Dis. 2011;58:389–97.
Amador C, Xia C, Nagy R, Campbell A, Porteous D, Smith BH, et al. Regional variation in health is predominantly driven by lifestyle rather than genetics. Nat Commun. 2017;8:801.
Amani R. Comparison between bioelectrical impedance analysis and body mass index methods in determination of obesity prevalence in Ahvazi women. Eur J Clin Nutr. 2007;61:478–82.
Azarbal F, Stefanick ML, Assimes TL, Manson JE, Bea JW, Li W, et al. Lean body mass and risk of incident atrial fibrillation in post-menopausal women. Eur Heart J. 2016;37:1606–13.
Bae YJ. Association between nutrient intake and osteosarcopenic obesity: Korea national health and nutrition examination survey 2008-2010. Osteoporos Int. 2018;29:S421–31. Abstract P825.
Bai HJ, Sun JQ, Chen M, Xu DF, Xie H, Yu ZW, et al. Age-related decline in skeletal muscle mass and function among elderly men and women in Shanghai, China: a cross sectional study. Asia Pac J Clin Nutr. 2016;25:326–32.
Bann D, Cooper R, Wills AK, Adams J, Kuh D, NSHD scientific and data collection t. Socioeconomic position across life and body composition in early old age: findings from a British birth cohort study. J Epidemiol Community Health. 2014;68:516–23.
Barrera G, Cases T, Bunout D, de la Maza MP, Leiva L, Rodriguez JM, et al. Associations between socioeconomic status, aging and functionality among older women. Geriatric Nursing. 2017;38:347–51.
Beydoun MA, Fanelli Kuczmarski MT, Mason MA, Ling SM, Evans MK, Zonderman AB. Role of depressive symptoms in explaining socioeconomic status disparities in dietary quality and central adiposity among US adults: a structural equation modeling approach. Am J Clin Nutr. 2009;90:1084–95.
Bhupathiraju SN, Dawson-Hughes B, Lichtenstein AH, Hannan MT, Tucker KL. Centrally located body fat is associated with lower bone mineral density in older Puerto Ricans. Am J Epidemiol. 2011;11:S116–1070.
Brennan SL, Henry MJ, Nicholson GC, Kotowicz MA, Pasco JA. Socioeconomic status and risk factors for obesity and metabolic disorders in a population-based sample of adult females. Prev Med. 2009;49:165–71.
Buemann B, Tremblay A, Bouchard C. Social-class interacts with the association between macronutrient intake and subcutaneous fat. Int J Obes. 1995;19:770–5.
De Marchi RJ, Hugo FN, Hilgert JB, Padilha DM. Association between number of teeth, edentulism and use of dentures with percentage body fat in south Brazilian community-dwelling older people. Gerodontology. 2010;29:e69–76.
Dugan SA, Everson-Rose SA, Karavolos K, Avery EF, Wesley DE, Powell LH. Physical activity and reduced intra-abdominal fat in midlife African-American and white women. Obesity. 2010;18:1260–5. (19307381)
Dupuy C, Lauwers-Cances V, van Kan GA, Gillette S, Schott AM, Beauchet O, et al. Dietary vitamin D intake and muscle mass in older women. Results from a cross-sectional analysis of the EPIDOS study. J Nutr Health Aging. 2013;17:119–24.
Fedewa MV, Das BM, Forehand RL, Evans EM. Area-level socioeconomic status, adiposity, physical activity, and inflammation in young adults, 2013. Prev Chronic Dis. 2014;11:E130
Guo W, Key TJ, Reeves GK. Adiposity and breast cancer risk in postmenopausal women: results from the UK Biobank prospective cohort. Int J Cancer. 2018;143:1037–46.
Kazlauskaite R, Karavolos K, Janssen I, Carlson K, Shipp KJ, Dugan SA, et al. The association between self-reported energy intake and intra-abdominal adipose tissue in perimenopausal women. J Obes. 2012;2012:567320.
Keighley ED, McGarvey ST, Turituri P, Viali S. Farming and adiposity in Samoan adults. Am J Hum Biol. 2006;18:112–22.
Keino S, Plasqui G, Van Den Borne B. Measuring adiposity among women in Narok county, Kenya: comparison between body mass index, waist-hip ratio, waist circumference, fat mass index and percentage fat mass. Ann Nutr Metab. 2017;71:1044. Abstract 144/319.
Kim J, Lee Y, Kye S, Chung YS, Kim KM. Association between healthy diet and exercise and greater muscle mass in older adults. J Am Geriatr Soc. 2015;63:886–92.
Krueger D, Vallarta-Ast N, Love G, Engelke J, Ryff C, Binkley N. Factors affecting vitamin D status: evaluation of a midus cohort. J Clin Densitom. 2010;13:125. Abstract 050.
Kruger HS, Havemann-Nel L, Ravyse C, Moss SJ, Tieland M. Physical activity energy expenditure and sarcopenia in black South African urban women. J Phys Act Health. 2016;13:296–302.
Kulkarni B, Shatrugna V, Nagalla B, Rani KU. Regional body composition of Indian women from a low-income group and its association with anthropometric indices and reproductive events. Ann Nutr Metab. 2010;56:182–9.
Lahmann PH, Lissner L, Gullberg B, Berglund G. Differences in body fat and central adiposity between Swedes and European immigrants: the Malmo Diet and Cancer Study. Obes Res. 2000;8:620–31.
Lahmann PH, Lissner L, Gullberg B, Berglund G. Sociodemographic factors associated with long-term weight gain, current body fatness and central adiposity in Swedish women. Int J Obes Relat Metab Disord. 2000;24:685–94.
Lantz H, Bratteby LE, Fors H, Sandhagen B, Sjöström L, Samuelson G. Body composition in a cohort of Swedish adolescents aged 15, 17 and 20.5 years. Acta Paediatr. 2008;97:1691–7.
Lewin A, Pannier B, Meline J, Karusisi N, Thomas F, Chaix B. Residential neighborhood, geographic work environment, and work economic sector: associations with body fat measured by bioelectrical impedance in the RECORD Study. Ann Epidemiol. 2014;24:180–6.
Lewis TT, Everson-Rose SA, Karavolos K, Janssen I, Wesley D, Powell LH. Hostility is associated with visceral, but not subcutaneous, fat in middle-aged african American and white women. Psychosom Med. 2009;71:733–40.
Loucks EB, Britton WB, Howe CJ, Gutman R, Gilman SE, Brewer J, et al. Associations of dispositional mindfulness with obesity and central adiposity: the New England Family Study. Int J Behav Med. 2015;23:224–33.
Lourenco AEP, Santos RV, Orellana JDY, Coimbra CEA. Nutrition transition in Amazonia: obesity and socioeconomic change in the Surui Indians from Brazil. Am J Hum Biol. 2008;20:564–71.
McClure CKA, Schwarz EB, Conroy MB, Tepper PG, Janssen I, et al. Breastfeeding and subsequent maternal visceral adiposity. Obesity. 2011;19:2205–13. (19307381)
Mongraw-Chaffin M, Allison MA, Burke GL, Criqui MH, Matsushita K, Ouyang P, et al. CT-derived body fat distribution and incident cardiovascular disease: the multi-ethnic study of atherosclerosis. J Clin Endocrinol Metab. 2017;102:4173–83.
Ozener B, Duyar I, Atamturk D. Body composition of young laborers: the results of a bioelectrical impedance analysis. Coll Antropol. 2007;31:949–54.
Pirilä S, Saarinen-Pihkala UM, Viljakainen H, Turanlahti M, Kajosaari M, Mäkitie O, et al. Breastfeeding and determinants of adult body composition: a prospective study from birth to young adulthood. Horm Res Paediatr. 2012;77:281–90.
Powell M, Lara J, Mocciaro G, Prado CM, Battezzati A, Leone A, et al. Association between ratio indexes of body composition phenotypes and metabolic risk in Italian adults. Clin Obes. 2016;6:365–75.
Rangel Peniche DB, Aleman Mateo H, Barreiro M, Ruiz Valenzuela RE, Ramirez-Torres M, Urquidez-Romero R. Differences in body composition in older people from two regions of mexico: implications for diagnoses of sarcopenia and sarcopenic obesity. Biomed Res Int. 2018;2018:7538625.
Rebato E, Rosique J, Vinagre A, Salces I, San Martin L, Susanne C. Nutritional status by socioeconomic level in an urban sample from Bilbao (Basque Country). Am J Hum Biol. 2001;13:668–78.
Sallinen J, Stenholm S, Rantanen T, Helioaara M, Sainio P, Koskinen S. Effect of age on the association between body fat percentage and maximal walking speed. J Nutr Health Aging. 2011;15:427–32.
Seppänen-Nuijten E, Lahti-Koski M, Männistö S, Knekt P, Rissanen H, Aromaa A, et al. Fat free mass and obesity in relation to educational level. BMC Public Health. 2009;9:448.
Sotillo C, López-Jurado M, Aranda P, López-Frías M, Sánchez C, Llopis J. Body composition in an adult population in southern Spain: influence of lifestyle factors. Int J Vitam Nutr Res. 2007;77:406–14.
Suder A. Body fatness and its social and lifestyle determinants in young working males from Cracow, Poland. J Biosoc Sci. 2009;41:139–54.
Velasquez-Melendez G, Silveira EA, Allencastro-Souza P, Kac G. Relationship between sitting-height-to-stature ratio and adiposity in Brazilian women. Am J Hum Biol. 2005;17:646–53.
Visser M, Harris TB, Langlois J, Hannan MT, Roubenoff R, Felson DT, et al. Body fat and skeletal muscle mass in relation to physical disability in very old men and women of the Framingham Heart Study. J Gerontol A Biol Sci Med Sci. 1998;53:M214–21.
Wu CH, Lu FH, Chang CS, Chang TC, Wang RH, Chang CJ. Relationship among habitual tea consumption, percent body fat, and body fat distribution. Obes Res. 2002;11:1088–95.
Yliharsila H, Kajantie E, Osmond C, Forsen T, Barker DJP, Eriksson JG. Birth size, adult body composition and muscle strength in later life. Int J Obes. 2007;31:1392–9.
Janmahasatian S, Duffull SB, Ash S, Ward LC, Byrne NM, Green B. Quantification of lean bodyweight. Clin Pharmacokinet. 2005;44:1051–65.
Buckinx F, Landi F, Cesari M, Fielding RA, Visser M, Engelke K, et al. Pitfalls in the measurement of muscle mass: a need for a reference standard. J Cachexia Sarcopenia Muscle. 2018;9:269–78.
Hansen RD, Raja C, Aslani A, Smith RC, Allen BJ. Determination of skeletal muscle and fat-free mass by nuclear and dual-energy x-ray absorptiometry methods in men and women aged 51-84 y (1-3). Am J Clin Nutr. 1999;70:228–33.
Birnie K, Cooper R, Martin RM, Kuh D, Sayer AA, Alvarado BE, et al. Childhood socioeconomic position and objectively measured physical capability levels in adulthood: a systematic review and meta-analysis. PLoS One. 2011;6:e15564.
Wind AE, Takken T, Helders PJ, Engelbert RH. Is grip strength a predictor for total muscle strength in healthy children, adolescents, and young adults? Eur J Pediatr. 2010;169:281–7.
Bouchard DR, Heroux M, Janssen I. Association between muscle mass, leg strength, and fat mass with physical function in older adults: influence of age and sex. J Aging Health. 2011;23:313–28.
Cruz F, Ramos E, Lopes C, Araujo J. Tracking of food and nutrient intake from adolescence into early adulthood. Nutrition. 2018;55-56:84–90.
Elhakeem A, Cooper R, Bann D, Hardy R. Childhood socioeconomic position and adult leisure-time physical activity: a systematic review. Int J Behav Nutr Phys Act. 2015;12:92.
Liu P, Ma F, Lou H, Liu Y. The utility of fat mass index vs. body mass index and percentage of body fat in the screening of metabolic syndrome. BMC Public Health. 2013;13:629.
VanItallie TB, Yang MU, Heymsfield SB, Funk RC, Boileau RA. Height-normalized indices of the body’s fat-free mass and fat mass: potentially useful indicators of nutritional status. Am J Clin Nutr. 1990;52:953–9.
Chaston TB, Dixon JB, O’Brien PE. Changes in fat-free mass during significant weight loss: a systematic review. Int J Obes (Lond). 2007;31:743–50.
Forbes GB. Some adventures in body composition, with special reference to nutrition. Acta Diabetol. 2003;40:S238–S41.
Cooper R, Hardy R, Bann D, Aihie Sayer A, Ward KA, Adams JE, et al. Body mass index from age 15 years onwards and muscle mass, strength, and quality in early old age: findings from the MRC National Survey of Health and Development. J Gerontol a-Biol. 2014;69:1253–9.
Navalpotro L, Regidor E, Ortega P, Martinez D, Villanueva R, Astasio P. Area-based socioeconomic environment, obesity risk behaviours, area facilities and childhood overweight and obesity: socioeconomic environment and childhood overweight. Prev Med. 2012;55:102–7.
Tyrrell J, Wood AR, Ames RM, Yaghootkar H, Beaumont RN, Jones SE, et al. Gene-obesogenic environment interactions in the UK Biobank study. Int J Epidemiol. 2017;46:559–75.
Popkin BM. Nutrition transition and the global diabetes epidemic. Curr Diab Rep. 2015;15:64.
Mayen AL, Marques-Vidal P, Paccaud F, Bovet P, Stringhini S. Socioeconomic determinants of dietary patterns in low- and middle-income countries: a systematic review. Am J Clin Nutr. 2014;100:1520–31.
Darmon N, Drewnowski A. Does social class predict diet quality? Am J Clin Nutr. 2008;87:1107–17.
Darmon N, Drewnowski A. Contribution of food prices and diet cost to socioeconomic disparities in diet quality and health: a systematic review and analysis. Nutr Rev. 2015;73:643–60.
Hallal PC, Andersen LB, Bull FC, Guthold R, Haskell W, Ekelund U, et al. Global physical activity levels: surveillance progress, pitfalls, and prospects. Lancet. 2012;380:247–57.
Gidlow C, Johnston L, Crone D, Ellisa N, James D. A systematic review of the relationship between socio-economic position and physical activity. Health Educ J. 2006;65:338–67.
Beenackers MA, Kamphuis CB, Giskes K, Brug J, Kunst AE, Burdorf A, et al. Socioeconomic inequalities in occupational, leisure-time, and transport related physical activity among European adults: a systematic review. Int J Behav Nutr Phys Act. 2012;9:116.
Monteiro CA, Moura EC, Conde WL, Popkin BM. Socioeconomic status and obesity in adult populations of developing countries: a review. Bull World Health Organ. 2004;82:940–6.
Pudrovska T, Reither EN, Logan ES, Sherman-Wilkins KJ. Gender and reinforcing associations between socioeconomic disadvantage and body mass over the life course. J Health Soc Behav. 2014;55:283–301.
Hill SE, Bell C, Bowie JV, Kelley E, Furr-Holden D, LaVeist TA, et al. Differences in obesity among men of diverse racial and ethnic background. Am J Mens Health. 2017;11:984–9.
El-Sayed AM, Scarborough P, Galea S. Ethnic inequalities in obesity among children and adults in the UK: a systematic review of the literature. Obes Rev. 2011;12:e516–34.
Barrington DS, James SA, Williams DR. Socioeconomic correlates of obesity in African-American and Caribbean-black men and women. J Racial Ethn Health Disparities. 2021;8:422–32.
Smith NR, Kelly YJ, Nazroo JY. The effects of acculturation on obesity rates in ethnic minorities in England: evidence from the Health Survey for England. Eur J Public Health. 2012;22:508–13.
Wasserstein RL, Schirm AL, Lazar NA. Moving to a world beyond “p < 0.05”. Am Stat. 2019;73:1–19.
Halsey LG. The reign of the p-value is over: what alternative analyses could we employ to fill the power vacuum? Biol Lett. 2019;15:5.
Sterne JA, Davey Smith G. Sifting the evidence-what’s wrong with significance tests? BMJ. 2001;322:226–31.
Scafoglieri A, Clarys JP. Dual energy X-ray absorptiometry: gold standard for muscle mass? J Cachexia Sarcopenia Muscle. 2018;9:786–7.
Acknowledgements
CBS is supported by a PhD studentship from the UK Medical research Council (MR/N013867/1). RH is Director of the CLOSER consortium, which is supported by the Economic and Social Research Council (ESRC) (award reference: ES/K000357/1). YK and RL are supported by the ESRC (ES/R008930/1, ES/P010229/1). AG, MA and EW are supported by PhD studentships from the ESRC (ES/P000347/1). JMB was supported by the Canadian Institutes of Health Research (FDSA) and the Canadian Centennial Scholarship Fund.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Bridger Staatz, C., Kelly, Y., Lacey, R.E. et al. Life course socioeconomic position and body composition in adulthood: a systematic review and narrative synthesis. Int J Obes 45, 2300–2315 (2021). https://doi.org/10.1038/s41366-021-00898-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41366-021-00898-z
This article is cited by
-
Socioeconomic inequalities in early adulthood disrupt the immune transcriptomic landscape via upstream regulators
Scientific Reports (2024)
-
AI-generated CT body composition biomarkers associated with increased mortality risk in socioeconomically disadvantaged individuals
Abdominal Radiology (2024)
-
Life-course social disparities in body mass index trajectories across adulthood: cohort study evidence from China health and nutrition survey
BMC Public Health (2023)
-
Socio-economic accounting of inequalities in excess weight: a population-based analysis
BMC Public Health (2023)
-
The psychological legacy of past obesity and early mortality: evidence from two longitudinal studies
BMC Medicine (2023)
