
Abstract
The unbound “free” bilirubin concentration (Bf), not the total bilirubin concentration, is the critical determinant of cellular uptake and toxicity of bilirubin. We compared Bf measured by a modified peroxidase method with published data obtained with ultrafiltration and examined conditions that affect the affinity (KF) of human (HSA) and bovine (BSA) serum albumin for bilirubin. The peroxidase and ultrafiltration methods yielded similar KF values that decreased with increasing HSA concentration and the presence of 50 mM chloride. When related to ionic strength, inhibition of BSA-bilirubin binding by chloride, bromide, and sulfate were similar, whereas phosphate buffer had a smaller effect. KF was lower at 37°C than at 25°C for HSA but not for BSA. KF for BSA was similar at pH 7.4 and 8.0. BSA and FCS had similar binding properties. The close agreement of Bf and KF values determined by the peroxidase method with published results obtained by ultrafiltration validates both methods and supports the use of the peroxidase method as a practical technique for measuring Bf under steady state conditions in minimally diluted serum or culture medium.
Similar content being viewed by others
Main
The unbound (“free”) concentration of unconjugated bilirubin (Bf) in plasma, although less than 0.1% of total bilirubin concentration, is the principal determinant of tissue uptake and toxicity of bilirubin, and plays a critical role in the pathogenesis of bilirubin encephalopathy in jaundiced newborns (1,2) and in patients with Crigler Najjar disease (3). Notwithstanding its biologic significance, Bf has rarely been measured in either clinical evaluation of jaundiced newborns or in vitro studies of bilirubin effects and toxicity. This avoidance is due in part to the perceived complexity of Bf assays and scepticism regarding their clinical value or accuracy (4–6).
Bilirubin-albumin binding has been studied using a variety of techniques, including fluorescent quenching, bilirubin fluorescence, circular dichroism, Sephadex gel filtration, optical rotary dispersion, dialysis, ultrafiltration, spectrophotometry, and enzymatic oxidation of bilirubin (peroxidase method). Reported association constants for HSA range from 6.7 × 106 M−1 to >108 M−1 (7–10). The binding constant of HSA has been estimated to be 2–13 times greater than that of BSA (11–13). Considerable variation in serum binding of bilirubin has been reported in newborn infants (2). These differences may be due to direct binding competitors (e.g. sulfonamides), allosteric effects, electrolyte environment, or simply the assay technique, e.g. serum sample dilution (14).
The dependency of bilirubin binding affinity on HSA concentration as well as chloride concentration was demonstrated by Weisiger et al. (15) using a complicated procedure in which binding affinity of 14C-bilirubin was calculated after the sequential removal of labeled impurities by serial ultrafiltration. A more practical technique for measuring Bf in clinical or laboratory settings was developed by Jacobsen and Wennberg (16) based on the observation that albumin-binding protects bilirubin from oxidation by HRP. Ahlfors (14,17) has modified the peroxidase method, emphasizing the need to measure Bf with two or more HRP concentrations and under the same conditions and albumin concentrations existing in plasma or incubation medium.
In this investigation, we replicated and extended the experimental conditions used in ultrafiltration studies (15) and examined the effects of albumin and electrolyte concentrations on bilirubin binding to HSA and BSA, using the modified peroxidase method (17). We then evaluated various experimental conditions that must be controlled when measuring Bf in tissue culture medium.
MATERIALS AND METHODS
Materials.
PBS, DMEMHG, penicillin, and streptomycin were purchased from Euroclone, Milan, Italy. FCS, obtained from Invitrogen (Carlsbad, CA), contained 24 g/L albumin. Chloroform, HPLC grade was obtained from Carlo Erba, Milan, Italy. Bilirubin, DMSO (HPLC grade), HRP (EC.1.11.1.7/P 8125, Type I), hydrogen peroxide (H2O2, 30% wt/vol), fatty acid–free HSA, and fatty acid–free BSA fraction V, were purchased from Sigma Chemical Co.-Aldrich, Milan, Italy.
Preparation of solution and reagents.
Bilirubin was purified using the method of McDonagh and Assisi (18), divided into 50 μg aliquots, and stored at −20°C until used. Aliquots were dissolved in either 200 μL 0.01 N NaOH, followed by dilution with 2.64 mL H2O (final concentration 30 μM) or 17 μL DMSO, yielding 5 mM (3 μg/mL).
Immediately after preparation, the bilirubin stock solution was added to PBS or DMEMHG containing 30 or 60 μM HSA or BSA, or 10% FCS (33 μM BSA). Final DMSO concentrations never exceeded 0.5% (vol/vol). When NaOH stock was added, the pH was adjusted to 7.4 with 0.01 N HCl. Total bilirubin concentrations (B) in albumin solutions were confirmed by the absorbance (A) at 468 nm (BSA) or 460 nm (HSA) assuming ɛ1 cm = 49,000 A/mol for BSA and 48,000 A/mol for HSA (16).
HRP stock solution (1 mg/mL) was prepared by dissolving 2 mg HRP (EC.1.11.1.7/P 8125, Type I) in 2 mL PBS, pH 7.4, and stored at −20°C (19).
1.0% Hydrogen peroxide was prepared freshly each day by diluting 1 mL 30% H2O2 with 29 mL PBS.
Peroxidase method—basic principles and calculations.
Unbound bilirubin is oxidized to mostly colorless compounds by peroxide (H2O2) in the presence of HRP with first-order kinetics; albumin-bound bilirubin is not oxidized. The rate constant for oxidation of bilirubin by HRP (kp) is determined by measuring the decrease in A440 following addition of HRP and H2O2 to dilute solutions of bilirubin (1–3 μM):
eq. (1)

Vo, the initial oxidation velocity determined using a recording spectrophotometer, can be expressed either as the initial decrease in total bilirubin concentration (B) or simply ΔA440/min (i.e. Ao − At)/t:
eq. (1a)

Alternatively, kp may be calculated from an integrated form of eq. (1), which accounts for nonlinear oxidation as B decreases:
eq. (2)

The steady state Bf in bilirubin-albumin solutions is determined by measuring the decrease in A460 (HSA) or A468 (BSA) over 30–60 s in the presence of HRP and H2O2 and calculated from the rate constant (kp), the concentration of HRP, and the initial change in bilirubin concentration (or ΔA) over time.
eq. (3)

where ɛ* is the molar absorbance coefficient of bilirubin-albumin (BSA or HSA), or with the integrated form:
eq. (4)

The instantaneous decrease in A460 (HSA) or A468 (BSA) reflects the equilibrium Bf, but thereafter the rate of oxidation represents the steady state concentration of Bf reflecting bilirubin-albumin association/dissociation and enzyme oxidation (14,17). To determine the equilibrium Bf, the assay is performed with at least two concentrations of enzyme. As the bilirubin/albumin molar ratio (B/A) increases, albumin-bilirubin dissociation becomes rate limiting, and a significant underestimation of Bf will occur if several concentrations of HRP are not used. Because 1/[steady-state Bf] is proportional to 1/([Bf] + [HRP]), the equilibrium Bf is determined from the inverse of the y intercept of a plot of 1/[steady-state Bf] versus[HRP] (17).
The binding constant was calculated assuming a single albumin binding site because measurements were performed at low B/A ratios (0.2–0.3), where binding to other sites should be minimal (15). Because of these assumptions, we adopted the term KF (formation constant), as used by Weisiger et al. (15), rather than the customary association constant, Ka, to describe binding. Thus:
eq. (5)

HRP standardization (kp).
Stock solutions of bilirubin in NaOH or DMSO were protected from light and used within 1 h. Appropriate volumes were added to 2.8 mL of medium without albumin, to reach final bilirubin concentrations of 1, 2, and 3 μM, and the concentration of bilirubin determined spectrophotometrically (Beckman DU 640 spectrophotometer) assuming ɛ1 cm = 47,500 per mol at 440 nm (16). Then 10 μL of 1.0% H2O2 and 10 μL of diluted HRP (1.65 × 10−2 μg/mL) were added and the cuvette inverted twice without shaking the supersaturated solution. ΔA440 nm was recorded for 30–60 s and kp calculated as described above. Using the same (albumin-free) medium used for Bf determination, 5 replicates were run at each of 2–3 HRP concentrations, and the 10–15 measurements averaged to determine kp.
Measurement of Bf.
Bf was measured using undiluted samples to avoid alteration in KF. Following measurement of A0 at the appropriate wavelength, 5 μL of 1.0% H2O2 and 5–20 μL HRP (final concentration 0.6–2.5 μg/mL) were added to 3 mL bilirubin-albumin solution. The cuvette was inverted twice and ΔA measured for 30 s. The HRP concentration was adjusted to produce a ΔA of 10–20% over 1 min. Triplicate determinations were performed at each of 2 to 3 peroxidase concentrations (0.6, 1.2, and/or 2.5 μg/mL) and the steady state Bf was calculated as described above. The equilibrium Bf was then calculated from formula 5.
Comparison of peroxidase and ultrafiltration methods using HSA.
Bf was measured using media of the same composition as those used in ultrafiltration studies (15) (250 mM sucrose + 50 mM KCl or 350 mM sucrose without chloride, HEPES 20 mM, pH 7.4, and variable HSA concentration). The B/A ratio was maintained at 0.2. Our studies were performed at 37°C rather than 25°C.
Bilirubin binding in solutions containing HSA, BSA, or FCS.
In vitro studies of bilirubin toxicity often use bilirubin bound to HSA or BSA, or media containing FCS. The binding of bilirubin to HSA, BSA, and FCS was examined using albumin concentrations of 30 μM, and varying B, in PBS and DMEMHG, pH 7.4, at 37°C in the dark.
Bilirubin stability in solutions without or with albumin.
We evaluated the effect of bilirubin solvent (0.01 N NaOH or DMSO) on aqueous stability and kp determination in DMEMHG and PBS, pH 7.4, 37°C. Final bilirubin concentrations of 1, 2, and 3 μM were confirmed by measuring absorbance at 440 nm, and stability was determined by monitoring ΔA440· Kp was measured as noted above. The stability of bilirubin-BSA solutions (B/A ratio = 0.3) was evaluated by monitoring A468 over 24 h.
Other factors affecting Kp and bilirubin binding to BSA.
Unless otherwise noted, the remaining studies were performed in DMEMHG medium, pH 7.4, at 37°C using 30 μM BSA.
The effects of inorganic anions on binding were studied at a B/A ratio of 0.2. Sodium salts of Cl−, Br−, or SO4− were added to 250 mM sucrose, containing 20 mM HEPES; HEPES was omitted from studies of phosphate.
The effects of impurities in commercial bilirubin on kp and Bf determinations were determined by comparison with purified bilirubin. The effect of light (1000 lux) on Bf was evaluated using 60 μM BSA and 12 μM bilirubin in DMEMHG. The solution flask was placed 10 cm below a POLILUX 4000 58WT8 fluorescent lamp in a biologic safety cabin (Model-VBH72 MP/99; Steril, Milan, Italy). After 15, 30, and 60 min light exposure at 25°C, Bf was measured at 37°C.
The effects of temperature were studied at 25°C and 37°C. Kp was determined at bilirubin concentrations of 1.8 and 3.5 μM. Bf was measured using 60 μM BSA or HSA and B/A ratios of 0.23 and 0.17, respectively.
The effects of pH on kp and on binding by HSA and BSA were evaluated at pH 7.4 and 8.0. The pH was adjusted by addition of 0.01N HCl or NaOH. Effects on Bf were assessed at a B/A ratio of 0.3.
The effect of commonly used tissue culture additives (streptomycin, penicillin, glutamine) on binding were studied in DMEMHG using BSA, B/A 0.2 at 37°C.
Statistical analysis.
Results are expressed as mean ± SD of three to five assays per condition. Statistical analysis was performed using ANOVA combined with Student's two-tailed t test. Differences among the conditions were considered significant at p< 0.05.
RESULTS
Comparison of the peroxidase and ultrafiltration methods with HSA (Fig. 1).

Effect of HSA concentration on the binding affinity (KF) of bilirubin, 37°C, in the absence (A) or presence (B) of 50 mM KCl. Data are compared with reported KF values determined in identical media by ultrafiltration (15). The bilirubin/albumin molar ratio was maintained at 0.2. Peroxidase method (•), ultracentrifugation method (^).
HEPES buffer, used for ultrafiltration, inhibited HRP activity, resulting in a kp an order of magnitude lower than in PBS. This required a higher concentration of HRP for measuring Bf in the presence of albumin, but the calculated Bf in a control serum (60 μM BSA, 12 μM B) was the same with either HEPES or PBS buffer (18.9 ± 1.7 nM versus 19.2 ± 0.3 nM, respectively).
Data obtained with the peroxidase method confirmed the findings of Weisiger et al. (15). The affinity of HSA for bilirubin decreased with increasing albumin concentration and with the addition of chloride (Fig. 1). In the absence of chloride, at HSA concentrations of 60 μM or above, the peroxidase and ultrafiltration methods yielded nearly identical results. At lower HSA concentrations, especially in the presence of chloride, the peroxidase method yielded a somewhat higher KF than had ultrafiltration, but the patterns were similar.
Comparison of KF for HSA and BSA using the peroxidase method.
The effects of albumin and electrolyte concentrations on bilirubin binding to BSA had unique features (Table 1). In the absence of chloride, KF-HSA was about two times higher than KF-BSA at each albumin concentration (1.6× at 150 μM to 2.7× at 10 μM). However, in the presence of 50 mM Cl−, the ratio KF-HSA/KF-BSA increased from 3× at 150 μM to about 10× at 10 μM albumin. With BSA, the dilution effect was mitigated by 50 mM Cl−. In the presence of chloride anion, KF-HSA increased 7× when albumin was diluted from 150 μM to 10 μM, whereas KF-BSA increased less than 2× and remained nearly constant with BSA concentrations of 60 μM or higher. However, the effect of chloride on BSA binding was substantial. With HSA, chloride decreased KF about 40% at all HSA concentrations, whereas KF-BSA decreased 3-fold with 150 μM BSA and more than 6-fold with albumin concentrations of 30 μM or lower.
Bf measurements in culture media containing BSA, HSA, or 10% FCS.
In vitro studies of bilirubin toxicity often use bilirubin bound to HSA or BSA, and many cell cultures require media containing FCS. We, therefore, compared the binding of bilirubin to HSA, BSA, and FCS in DMEMHG.
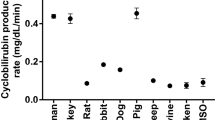
Addition of H2O2 alone to DMEMHG with 10% bilirubin-FCS revealed intrinsic oxidase activity that followed saturation kinetics, with a Vmax of 0.07 ΔA468/min at about 20 μM bilirubin (data not shown). This background oxidation rate, which was not diminished by pretreating the medium with a heme-adsorbing resin, was subtracted from the oxidation rate obtained with added HRP to obtain the corrected oxidation rate:
eq. (6)

Background oxidation was not observed when either HSA or BSA was added to DMEMHG in the absence of FCS.
Incubation of bilirubin/BSA in DMEMHG in the dark at 37°C resulted in a 13% decay of bilirubin (ΔA468) in 24 h but only 7% over 6 h. By contrast, there was no decrease in A468 when bilirubin/BSA was dissolved in PBS.
Titrations of bilirubin using a constant albumin concentration of 30 μM in DMEMHG (Fig. 2) revealed a greater binding affinity with HSA than with either BSA or FCS. Bf was similar with BSA and FCS up to a B/A ratio of 0.5 but rose steeply at higher B/A ratios with FCS. Addition of glutamine (2 mM), streptomycin (100 mg/L), and 1% (vol/vol) penicillin (100,000 U/L) to culture medium (B/A 0.2) did not alter Bf (37 ± 5 nM versus 39 ± 7 nM in controls).

Effect of albumin species on the concentration of unbound bilirubin (Bf) at various bilirubin/albumin (B/A) molar ratios, comparing FCS (□), BSA (▪), and HSA (♦), each 30 μM. Medium was DMEMHG. Bf was measured at 37°C, pH = 7.4, using HRP concentrations of 0.6, 1.2, and 2.5 μg/mL.
Effect of inorganic anions on binding affinity of BSA for bilirubin.
The addition of 118 mM NaCl increased Bf from 10 to 179 nM and, as shown in Figure 3A, decreased KF from 28.7 to 1.3 μM−1. Bromide behaved similarly (data not shown). Divalent sulfate anion decreased KF more than chloride, with inhibition of bilirubin binding by 97% or more at sulfate concentrations of 50 mM or higher. In contrast, phosphate (50 mM, pH 7.4) produced only a 30% reduction in KF.

Effect of sodium salts of different anions on binding of bilirubin to BSA. The experiments were performed at 37°C in 250 mM sucrose, 20 mM HEPES, pH 7.4, containing 30 μM BSA at a constant bilirubin/albumin molar ratio of 0.2. Data represent the mean ± SD of three experiments. For 50 and 100 mM phosphate vs no phosphate, p< 0.02 and p< 0.002, respectively. For each concentration of chloride or sulfate vs no anion, p< 0.001. Phosphate (▪), chloride (•), sulfate (♦).
For each anion, log KF was negatively correlated with the square root of ionic strength (Fig. 3B). Chloride, bromide (not shown), and sulfate produced similar decreases in binding with increasing ionic strength; the effect of phosphate was much less at all ionic strengths.
Effect of bilirubin solvent and medium on bilirubin stability and Kp determination.
DMSO is frequently used as a bilirubin solvent for in vitro toxicity studies, while NaOH is usually used for peroxidase standardization. Bilirubin dissolved in DMSO precipitated when added to DMEMHG, so DMSO could not be used to determine kp in this medium. In PBS, spontaneous absorbance decay was greater for bilirubin dissolved in NaOH (ΔA/min = 0.0028) than in DMSO (ΔA/min = 0.0014).
Kp values in PBS were not significantly different for bilirubin dissolved with NaOH (463 ± 53 mL · μg−1 · min−1) or DMSO (491 ± 30 mL · μg−1 · min−1) and were unaffected by bilirubin concentration (1, 2, or 3 μM). Kp did not differ significantly between DMEMHG (445 ± 41 mL · μg−1 · min−1) and PBS (463 ± 53 mL · μg−1 · min−1) when bilirubin was dissolved in NaOH.
Effect of bilirubin purity and light exposure on binding to BSA in DMEMHG.
Purified and commercial bilirubin yielded similar kp values (439 ± 24 versus 450 ± 44 mL · μg−1 · min−1, respectively) and Bf values (21.1 ± 1.8 versus 21.2 ± 0.9 nM, respectively). After 15, 30, and 60 min exposure of bilirubin-BSA to intense light, Bf remained unchanged (25.0 ± 1.1 nM at time 0 versus 25.4 ± 0.6 nM after 1 h) despite a 14% drop in total bilirubin.
Effect of temperature on Kp and Bf.
In DMEMHG, the kp at 25°C, 282 ± 34 mL·μg−1·min−1, was much lower than at 37°C, 445 ± 41 mL·μg−1·min−1. In the small sample size studied (n = 5), we did not observe a temperature effect on binding to BSA (Bf measured at 25°C was 41.3 ± 4.8 nM versus 34.5 ± 5.6 nM at 37°C, p = 0.07). Bilirubin binding to HSA decreased slightly at the higher temperature (Bf = 22.8 ± 1.6 nM at 25°C versus 31.3 ± 6.1 nM at 37°C, p = 0.03), consistent with observations of Jacobsen (20).
Effect of pH on Kp and Bf in DMEMHG.
Tissue culture is frequently buffered by a CO2–bicarbonate system, resulting in an increased pH when removed from the CO2 atmosphere. The kp of 463 ± 31 at pH 7.4 fell to 402 ± 29 mL · μg−1 · min−1 at 8.0 (p< 0.03). Nonetheless, Bf values for bilirubin-BSA did not differ between pH 7.4 and 8.0 (51 ± 9.0 and 48 ± 8.0 nM, respectively). Similar results have been reported using HSA (21,22).
DISCUSSION
Our data confirm the effects of albumin and chloride concentration on bilirubin binding to HSA (15). There was good agreement with the ultrafiltration data (15), especially at HSA concentrations of 60 μM or higher in the absence of chloride. At low HSA concentrations, the peroxidase method yielded somewhat higher KF values than observed with ultrafiltration (15). This difference may be due in part to an albumin gradient created by ultracentrifugation, engendering higher HSA concentrations at the interface of the retentate with the filter. This would increase filtered bilirubin, yielding a higher apparent Bf and lower KF.
The range of KF values for HSA observed under various conditions in our study (6.9 × 106 M−1 to 1.1 × 108 M−1, Table 1) reflects the range of association constants reported in the literature using a variety of experimental techniques. Interestingly, the higher published values (KF> 108 M−1) were performed with very dilute albumin solutions (7,10), whereas the lower KF of 6.7 × 106 M−1, reported by Lamola et al. (8), used 440 μM HSA. The effect of albumin concentration on binding was far greater with HSA than with BSA (Table 1).
Our studies extend to BSA the previously reported inhibitory effect of 50 mM chloride anion on HSA binding (15) and also measured the effect of higher (physiologic) chloride concentrations. Chloride, bromide, and sulfate have the same effect on binding when analyzed as a function of ionic strength. Dehydration has been implicated in potentiating kernicterus, but variations in anion concentration within the range observed clinically should have little impact on bilirubin binding (Fig. 3A). The effect of phosphate is much smaller though still related to ionic strength, confirming the findings of Jacobsen (20). In contrast, Weisiger et al. (15) found that gluconate anion had no effect on bilirubin binding. Although the inhibition of organic anion binding by chloride roughly parallels the extent of binding by chloride (23,24), chloride binds to many more sites on albumin than does bilirubin (24). Thus, the relative roles of ionic strength, allosteric effects, and specific binding competition with anions remain uncertain.
A potential error in measuring Bf with the peroxidase method is that the HRP activity (kp) must be standardized with supersaturated bilirubin solutions. Aggregation of bilirubin might impair its oxidation, yielding a falsely low kp and overestimate of Bf. However, we found no differences in kp values measured at bilirubin concentrations of 1, 2, and 3 μM, suggesting that aggregation did not affect oxidation rates during the brief duration of the assay.
Water-soluble photoisomers, which form rapidly when bilirubin is exposed to light, cannot be distinguished from native ZZ-bilirubin IXα by either light absorbance or diazo reaction, but are thought to bind less tightly to albumin (25). Although photoisomer concentration was not determined, we found no effect on Bf of short-term, intense exposure of bilirubin-BSA to light. This result is explicable only if the photoproducts are bound to the bilirubin site on BSA, contribute to absorbance at 440 nm, and/or are substrates oxidized by HRP. Itoh et al. (26) previously demonstrated that the initial rate of the peroxidase reaction with HSA is not accelerated by either (ZE)-photobilirubin or (EZ)-cyclobilirubin when present at clinically relevant concentrations.
Most reported in vitro studies examining bilirubin effects or toxicity use HSA or BSA as a bilirubin stabilizer or donor, but rarely measure Bf and often use initial bilirubin concentrations that greatly exceed physiologic or pathologic significance (27). Even fewer studies measured the more meaningful equilibrium concentration of bilirubin during or after incubation (22,28). Ostrow et al. (27) recently calculated the Bf from molar bilirubin/albumin ratios (B/A) reported in several studies by applying ultrafiltration-determined binding constants for HSA in similar media (15). This study confirms, however, that calculated Bf's are unreliable since binding affinity varies with albumin species, albumin concentration, and the buffer medium used.
Tissue culture media typically contain 10% FCS, providing a BSA concentration of about 33 μM. Thus, bilirubin can be added directly to the medium rather than replacing medium with albumin solution. However, when using FCS, we found it important to correct for background oxidase activity. We also confirmed that commonly used culture medium additives, glutamine, streptomycin, and penicillin, do not alter binding.
In conclusion, our goal was to validate a practical method for measuring Bf and to adapt the method for studies using tissue culture media. The peroxidase method yielded KF values concordant with ultrafiltration data (15) obtained with nearly identical experimental conditions, and consistent with published values for KF. Compared with HSA, BSA has a lower binding affinity, greater sensitivity to chloride and less sensitivity to temperature. Our findings emphasize the need to measure HRP activity (kp) and Bf under the same conditions and in the same media used experimentally. We recommend that Bf be measured under steady state or equilibrium conditions in all studies in which albumin is used as a reservoir for bilirubin. This would facilitate interpretation of dose-response relationships and improve comparisons of in vitro studies conducted in different laboratories.
Abbreviations
- B:
-
total unconjugated bilirubin concentration
- B/A:
-
molar ratio of bilirubin to albumin
- DMEMHG:
-
Dulbecco's modified Eagle's medium—high glucose
- HRP:
-
horseradish peroxidase
- HSA:
-
human serum albumin
- KF:
-
calculated equilibrium binding constant of bilirubin to albumin
- kp:
-
first-order rate constant for the oxidation of bilirubin by HRP
References
Ahlfors CE, Wennberg RP 2004 Bilirubin-albumin binding and neonatal jaundice. Semin Perinatol 28: 334–339
Wennberg RP, Ahlfors CE, Bhutani VK, Johnson LH, Shapiro SM 2006 Toward understanding kernicterus: a challenge to improve the management of jaundiced newborns. Pediatrics 117: 474–485
Ihara H, Hashizume N, Shimizu N, Aoki T 1999 Threshold concentration of unbound bilirubin to induce neurological deficits in a patient with type I Crigler-Najjar syndrome. Ann Clin Biochem 36: 347–352
Levine RL 1979 Bilirubin: worked out years ago?. Pediatrics 64: 380–385
Robinson PJ, Rapoport SI 1987 Binding effect of albumin on uptake of bilirubin by brain. Pediatrics 79: 553–558
McDonagh AF, Maisels MJ 2006 Bilirubin unbound: deja vu all over again?. Pediatrics 117: 523–525
Levine RL 1977 Fluorescence-quenching studies of the binding of bilirubin to albumin. Clin Chem 23: 2292–2301
Lamola AA, Eisinger J, Blumberg WE, Patel SC, Flores J 1979 Flurorometric study of the partition of bilirubin among blood components: basis for rapid microassays of bilirubin and bilirubin binding capacity in whole blood. Anal Biochem 100: 25–42
Sato H, Honoré B, Brodersen R 1988 Multiple binding of bilirubin to human albumin and cobinding with laurate. Arch Biochem Biophys 260: 811–821
Brodersen R 1979 Binding of bilirubin to albumin; implications for prevention of bilirubin encephalopathy in the newborn. CRC Crit Rev Clin Lab Sci 11: 305–399
Faerch T, Jacobsen J 1975 Determination of association and dissociation rate constants for bilirubin-bovine serum albumin. Arch Biochem Biophys 168: 351–357
Blauer G, Lavie E, Silfen J 1977 Relative affinities of bilirubin for serum albumins from different species. Biochim Biophys Acta 492: 64–69
Reed RG 1977 Kinetics of bilirubin binding to bovine serum albumin and the effects of palmitate. J Biol Chem 252: 7483–7487
Ahlfors CE 1981 Effect of serum dilution on apparent unbound bilirubin concentration as measured by the peroxidase method. Clin Chem 27: 692–696
Weisiger RA, Ostrow JD, Koehler RK, Webster CC, Mukerjee P, Pascolo L, Tiribelli C 2001 Affinity of human serum albumin for bilirubin varies with albumin concentration and buffer composition: results of a novel ultrafiltration method. J Biol Chem 276: 29953–29960
Jacobsen J, Wennberg RP 1974 Determination of unbound bilirubin in the serum of newborns. Clin Chem 20: 783–789
Ahlfors CE 2000 Measurement of plasma unbound unconjugated bilirubin. Anal Biochem 279: 130–135
McDonagh AF, Assisi F 1972 The ready isomerization of bilirubin-IXα in aqueous solution. Biochem J 129: 797–800
Delincee H, Radola BJ 1975 Fractionation of horseradish peroxidase by preparative isoelectric focusing, gel chromatography and ion-exchange chromatography. Eur J Biochem 52: 321–330
Jacobsen J 1977 Studies of the affinity of human serum albumin for binding of bilirubin at different temperatures and ionic strength. Int J Pept Protein Res 9: 235–239
Jacobsen J, Brodersen R 1976 The effect of pH on albumin-bilirubin binding affinity. Birth Defects Orig Artic Ser 12: 175–178
Wennberg RP 1988 The importance of free bilirubin acid salt in bilirubin uptake by erythrocytes and mitochondria. Pediatr Res 23: 443–447
Klotz IM 1950 The nature of some ion-protein complexes. Cold Spring Harb Symp Quant Biol 14: 97–112
Scatchard G, Scheinberg IH, Armstrong SH Jr 1950 Physical chemistry of protein solutions. IV. The combination of human serum albumin with chloride ion. J Am Chem Soc 72: 535–540
Lamola AA, Flores J, Blumberg WE 1983 Binding of photobilirubin to human serum albumin. Estimate of the affinity constant. Eur J Biochem 132: 165–169
Itoh S, Yamakawa T, Onishi S, Isobe K, Manabe M, Sasaki K 1986 The effect of bilirubin photoisomers on unbound-bilirubin concentrations estimated by the peroxidase method. Biochem J 239: 417–421
Ostrow JD, Pascolo L, Tiribelli C 2003 Reassessment of the unbound concentrations of unconjugated bilirubin in relation to neurotoxicity in vitro. Pediatr Res 54: 98–104
Nelson T, Jacobsen J, Wennberg RP 1974 Effect of pH on the interaction of bilirubin with albumin and tissue culture cells. Pediatr Res 8: 963–967
Author information
Authors and Affiliations
Corresponding author
Additional information
Partially supported by grants from Telethon, Italy (GGP05062), and from Fondazione Cassa Risparmio, Trieste, Italy (FCRT 03-01). LR and SC were supported by fellowships from Ministero Affari Esteri, Rome, Italy. RPW was supported by a Senior Fellowship from AREA Science Park, Trieste, Italy.
Rights and permissions
About this article
Cite this article
Roca, L., Calligaris, S., Wennberg, R. et al. Factors Affecting the Binding of Bilirubin to Serum Albumins: Validation and Application of the Peroxidase Method. Pediatr Res 60, 724–728 (2006). https://doi.org/10.1203/01.pdr.0000245992.89965.94
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1203/01.pdr.0000245992.89965.94
This article is cited by
-
Molecular mechanisms of bilirubin induced G1 cell cycle arrest and apoptosis in human breast cancer cell lines: involvement of the intrinsic pathway
Molecular Biology Reports (2022)
-
Bilirubin disrupts calcium homeostasis in neonatal hippocampal neurons: a new pathway of neurotoxicity
Archives of Toxicology (2020)
-
Fabrication of Organic Hec Nanocomposites Modified with Lysine as a Potential Adsorbent for Bilirubin Removal
Applied Biochemistry and Biotechnology (2019)
-
Neuro-inflammatory effects of photodegradative products of bilirubin
Scientific Reports (2018)
-
Evaluation of region selective bilirubin-induced brain damage as a basis for a pharmacological treatment
Scientific Reports (2017)
