
Abstract
Purpose
To investigate the effects of tropicamide on chromatic and achromatic contrast sensitivities over the physiological range of spatial frequencies.
Methods
A total of 26 healthy volunteers, with a mean age of 32 years, were examined with and without one drop of 1% tropicamide being administered 30 min previously. On each occasion, acuity and pupil diameter were recorded, and chromatic and achromatic contrast sensitivities were examined using the Sussex Grating Machine.
Results
Following tropicamide administration mean pupil diameter increased from 4.1 mm to 7.2 mm (P<0.001), and mean BCVA was reduced by 0.07 LogMar units (P<0.001).
Achromatic contrast sensitivity was significantly reduced following tropicamide administration at 2.20 cycles per degree (cpd) (P=0.01), 3.40 cpd (P=0.01), 10 cpd (P=0.04), 17 cpd (P=0.04), and 25 cpd (P<0.01). There was no difference in contrast sensitivity at lower spatial frequencies (0.33 and 0.66 cpd). Chromatic contrast sensitivity was not significantly altered when tested along the red–green and tritan confusion axes.
Conclusions
Achromatic contrast sensitivity is significantly reduced following tropicamide administration at intermediate and high spatial frequencies. No significant changes were seen at low spatial frequencies and in chromatic contrast sensitivities.
Similar content being viewed by others

Introduction
Tropicamide is commonly used in ophthalmic practice to achieve pupillary dilation prior to the examination of the ocular fundus. Patients often wish to drive, or return to work, after consultation, and seek advice as to how the drops will affect their ability to do so.
There are multiple theoretical reasons for why tropicamide can be expected to affect visual function. Some aspects of daytime driving and visual performance have been observed to be altered following tropicamide administration.1 However, others studies have shown only limited effects on high-contrast acuity and Pelli–Robson contrast threshold and no significant effects on low-contrast visual acuity and field of vision.2, 3, 4
The aims of this study were to determine the effects of pupil dilatation on colour discrimination, and on contrast sensitivity over a wide range of spatial frequencies.
Methods
The subjects for this study were all members of staff in the Sussex Eye Hospital who had volunteered to take part. All were given a full explanation of the experimental procedures and informed consent was obtained, with the option to withdraw from the study at any time.
A full ophthalmic history was taken for each subject, and spectacle lens focimetry was performed for all subjects who wore glasses or contact lenses. One eye was chosen, at random, to be examined and all tests were performed monocularly. If the subject normally wore a distance correction, it was used for all the tests. All subjects had two sets of tests done, one without dilatation and another 30 min after dilatation with one drop of 1% tropicamide . The first 13 subjects to be examined had their pre-dilation recordings taken first, followed by administration of tropicamide and the post-dilation measurements. The subsequent 13 patients to be examined were given tropicamide straightaway and had their ‘dilated’ tests performed, before returning for the pre-dilation measurements at least 48 h later. This arrangement was chosen to limit any effects of familiarity with the testing regime on the results.
The visual acuity was checked using a Bailey–Lovie chart at a distance of 4 m under standard testing conditions. The subject was instructed to guess the letters when unsure until a full line of letters was incorrectly read; each correct letter scored −0.02 log units. Additionally, the pupil diameter was measured using a millimetre pupil rule. Subsequently, the subject's colour contrast and achromatic contrast thresholds were tested using the Sussex Grating Machine.
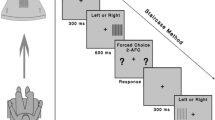
The Sussex Grating Machine has been described previously;5, 6, 7 in brief, it is a computerised cathode-ray-tube (CRT)-based gratings system that produces both achromatic and chromatic sinusoidal gratings on a high-resolution colour monitor. The luminance of the screen and its immediate surroundings is constant. The subject is seated 2 m from the screen, such that the stimulus field subtends a central visual angle of 4°. Subjects who normally used refractive correction wore their normal distance prescription for the duration of the examination.
The achromatic contrast sensitivity was measured at six spatial frequencies (0.66, 2.2, 3.4, 10.0, 17.0, and 26.0 cpd). The contrast threshold is the point at which the subject can just perceive the gratings on the screen. Contrast sensitivity is defined as the reciprocal of contrast threshold for a particular spatial frequency.
Colour contrast threshold (CCT) was measured, using the same computerised system, along the red–green (constant S-cone) and tritan (constant L/M-cone) confusion axes. The system randomly produces a series of standardised equiluminant, sinusoidal, chromatic gratings on the screen. The chromaticity of the gratings is changed automatically along either a tritan or a red–green confusion axes about a neutral white point under software control.
A modified double staircase reversal algorithm is used to accurately determine threshold.8 Two staircases are used for each chromatic or spatial-frequency grating that is tested, and are randomly interlaced with one another. The contrast of the stimulus is increased or decreased until the subjects change their response. When this occurs, the contrast is recorded and the direction of the stimulus sequence is reversed (eg from ascending to descending). The algorithm not only randomises the staircase selection at a particular chromatic axis or spatial frequency but also the chromatic axis or spatial frequency selection. This procedure is continued until five reversal points have been determined for each chromatic axis or spatial frequency tested. The first reversal point is discarded and the mean of the remaining four reversal points is taken as the final contrast threshold of the grating tested.
The subjects are instructed to press a hand-held button when they can see a grating pattern on the screen following an auditory warning tone. They are instructed not to press a button if gratings are not seen or if they are unsure. To ensure that a subject understands the procedure, a short practice routine is performed binocularly. The test is then performed monocularly. The mean differences in the pre- and post-dilation measurements were tested for statistical significance at the 95% level using one-tail paired t-tests.
Results
A total of 26 healthy volunteers took part in the study: 19 were female, and seven were male. Their ages ranged from 20 to 56 years, with a mean age of 32 years. None of the subjects had a history of ocular disease, apart from refractive error. Eight of the subjects wore myopic corrections (mean spherical equivalent of −2.71) and one wore a hypermetropic correction (spherical equivalent of +1.75). The mean best corrected visual acuity (BCVA), prior to dilation, in the eye examined had a LogMar score of −0.04. None of the subjects had a pre-dilation BCVA of less than 0.16.
The mean pupil diameter for the pre-dilation recordings was 4.1 mm. 30 min following 1% tropicamide administration; the mean pupil diameter was 7.2 mm.
The mean BCVAs, and contrast sensitivities at each spatial frequency, before and after 1% tropicamide are shown in Table 1. A significant reduction in BCVA was found at 30 min following 1% tropicamide administration (mean pre-dilation −0.04; mean post-dilation: 0.03; P<0.05). The mean change in BCVA following tropicamide administration was a reduction of 0.07 (equivalent to 3.5 letters on the LogMar chart). In seven of the 26 subjects, there was no reduction in LogMar acuity with tropicamide administration.
The achromatic contrast sensitivity was measured at seven spatial frequencies both pre- and post-dilation with tropicamide. A plot of the mean contrast sensitivity at each spatial frequency is shown in Figure 1. The differences were significant at 2.20 cpd (P=0.01), 3.40 cpd (P=0.01), 10.00 cpd (P=0.04), 17.00 cpd (P=0.03), and 25.00 cpd (P=0.001). No significant difference was found at the lowest spatial frequencies (0.33 and 0.66 CPD).

Mean achromatic contrast sensitivity at each spatial frequency, measured before and after dilation with 1% tropicamide.
Colour contrast thresholds measured along the red–green and tritan confusion axes were not found to be significantly altered following tropicamide administration.
Discussion
Tropicamide is a topical antimuscarinic widely used by health practitioners to achieve pupillary dilation. It is often the preferred agent owing to its short duration of action and its relatively greater mydriatic than cycloplegic effect. It takes approximately 30 min to achieve maximum mydriasis and the effects last for up to 4 h.9 We began examining our patients 30 min following tropicamide administration, to coincide with the time of maximum drug action.
Theoretically, the instillation of tropicamide might be expected to impair vision by a number of mechanisms. Mydriasis will reduce the depth of field and increase glare and optical aberrations. It may also manifest uncorrected refractive error because of loss of the stenopaeic effect of a small pupil. The cycloplegic effect of tropicamide is weak, but the reduction in accommodation will be sufficient to impair near vision in some patients.10 Loss of accommodation could also be expected to reduce distance acuity in uncorrected hypermetropes.
In practice, the effect of tropicamide on corrected high-contrast distance acuity is small, if at all, in most subjects. In our population of young and healthy volunteers, there was no deterioration in best-corrected distance acuity in 27% (7/26) of subjects. Overall, the mean deterioration was only equivalent to 3.5 LogMar letters. A limited effect is also seen in the more elderly population, with known morbidity, that is typically seen in clinic; Montgomery et al3 studied 100 consecutive clinic patients and found Snellen acuity to be unchanged in 55 eyes, with only 41 eyes dropping one line, and only four eyes dropping two lines of Snellen acuity.
Fewer studies have looked at the effects of tropicamide on visual function with low contrast or coloured targets. Potatmitis et al4 did examine low-contrast threshold and Pelli–Robson contrast threshold both pre- and post-dilation with 1% tropicamide. They found no significant effect on low-contrast acuity but did find a deterioration in Pelli–Robson Contrast Threshold. The Pelli–Robson chart consists of letters that progressively decrease in contrast but not in size,11 and thus contrast sensitivity is examined at just one fixed spatial frequency.
Machines that are similar to the Sussex Grating Machine have been used in research laboratories for many years but less frequently in clinical practice. These machines project computer-generated sinusoidal gratings on cathode-ray oscilloscopes. One advantage they have over the Pelli–Robson chart is that threshold contrast can readily be measured at multiple closely spaced spatial frequencies. This can be done over the entire visible range, and the results can then be plotted as a contrast-sensitivity function. Furthermore, more sophisticated approaches to testing can be used.
Our results have shown that the application of tropicamide significantly reduces contrast sensitivity in healthy volunteers. The reduction occurs at intermediate and high spatial frequencies, but not at lower spatial frequencies within the visible range. In the younger subjects, this will be due to the mydriatic effect of tropicamide alone; the cycloplegic effect is weak, and previous studies have found subjects to retain a mean of 3 dioptres of accommodation following administration of 1% tropicamide.3 Our subjects will only have needed to retain 0.5 dioptres of accommodation in order to view the Sussex Grating Machine screen at a distance of 2 m. A small cycloplegic effect would be more significant in any presbyopic uncorrected hypermetropes.
The application of tropicamide did not affect the ability of our subjects to discriminate coloured gratings along the red–green and tritan confusion axes. Pupil dilation has previously been shown to alter chromatic aberrations, causing differently coloured objects lying in the same plane to be perceived at different distances to one another.12 Colour discrimination remains unaffected.
Conclusion
Tropicamide administration certainly impairs visual function. Limited deteriorations in high-contrast acuity and accommodative amplitude, in particular, have been established previously. This study demonstrates that contrast sensitivity is also significantly impaired, and is so over a wide range of intermediate and high spatial frequencies.
Current Driving and Vehicle Licensing Agency (DVLA) regulations in the UK require specified standards of high-contrast distance acuity and field of vision to be reached.13 It has been demonstrated already that giving individuals lenses to simulate the effects of cataracts can lead to reduced contrast sensitivity and functioning in driving performance tests even though sufficient acuity to drive legally may be preserved.14 Pupillary dilation can also impair aspects of driving performance, and reduced contrast sensitivity is likely to be a contributing factor to this.1, 4 We believe patients should be warned that even if they satisfy the current legal requirements for driving after tropicamide administration, their vision can still be significantly impaired. The extent to which this affects their safety, and the safety of others, is still to be definitely answered and may vary between individuals.
References
Wood JM, Garth D, Grounds G, McKay P, Mulvahil A . Pupil dilatation does affect some aspects of daytime driving performance. Br J Ophthalmol 2003; 87: 1387–1390.
Nelson ME, Orton HP . Counteracting the effects of mydriatics. Does it benefit the patient? Arch Ophthalmol 1987; 105: 486–489.
Montgomery DM, MacEwan CJ . Pupil dilatation with tropicamide. The effects on acuity, accommodation and refraction. Eye 1989; 3: 845–848.
Potamitis T, Slade SV, Fitt AW, McLaughlin J, Mallen E, Auld RJ et al. The effect of pupil dilation with tropicamide on vision and driving simulator performance. Eye 2000; 14: 302–306.
Tregear SJ, Ripley LG, Knowles PJ, Gilday RT, de Alwis DV, Reffin JP . Automated tritan discrimination sensitivity: a new clinical technique for the effective screening of severe diabetic retinopathy. Int J Psychophysiol 1994; 16: 191–198.
Jackson TL, Ong GL, McIndoe MA, Ripley LG . Monocular chromatic contrast threshold and achromatic contrast sensitivity in children born prematurely. Am J Ophthalmol 2003; 136: 710–719.
Tregear SJ, Knowles PJ, Ripley LG, Casswell AG . Chromatic-contrast threshold impairment in diabetes. Eye 1997; 11: 537–546.
Cornsweet TN . The staircase method in psychophysics. Am J Psychophys 1962; 75: 485–491.
Hiatt RL, Jerkins G . Comparisons of Atropine and Tropicamide in Esotropia. Ann Ophthalmol 1983; 4: 341–343.
Gilmartin B, Amer AC, Ingleby S . Reversal of tropicamide mydriasis with single instillations of pilocarpine can induce substantial pseudo-myopia in young adults. Ophthal Physiol Opt 1995; 15: 475–479.
Pelli DG, Robson JG, Wilkins AJ . The design of a new letter chart for measuring contrast sensitivity. Clin Visci Sci 1988; 2: 187–199.
Sundet JM . The effect of pupil size variations on the colour stereoscopic phenomenon. Vision Res 1972; 12: 1027–1032.
Wood JM, Troutbeck R . Elderly drivers and simulated visual impairment. Optom Vis Sci 1995; 72: 115–124.
Acknowledgements
A summary of this work was presented as a poster presentation at the Association for Research in Vision and Ophthalmology (ARVO) in May 2005. No grants or sponsoring organizations have been involved in the work for this submission. The authors have no proprietary or commercial interests related to the manuscript.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Lee, E., Ong, G., Rajak, S. et al. Changes in chromatic and achromatic contrast sensitivities following tropicamide administration. Eye 21, 187–190 (2007). https://doi.org/10.1038/sj.eye.6702160
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.eye.6702160
