
Abstract
We investigated possible seasonal variation of births among children <20 years with a central nervous system tumour in Denmark (N=1640), comparing them with 2 582 714 children born between 1970 and 2003. No such variation was seen overall, but ependymoma showed seasonal variation.
Similar content being viewed by others
Main
Tumours of the central nervous system (CNS) are the second most frequent malignancy in childhood and the leading cause of death from childhood cancer (Little, 1999). The aetiology is in most cases unknown, and likely to differ among the different morphological subgroups. Approximately 5% are associated with genetic syndromes such as neurofibromatosis and tuberous sclerosis (Little, 1999). The only well-established environmental risk factor is ionising radiation (Wakeford, 2004).
A few studies have reported marked and significant seasonality of birth among patients with a CNS tumour (Yamakawa et al, 1982; Heuch et al, 1998; Feltbower et al, 2001; McNally et al, 2002; Brenner et al, 2004; Halperin et al, 2004; Koch et al, 2006; Mainio et al, 2006; Hoffman et al, 2007). However, there is considerable variability across studies with respect to which histological subgroup showed the effect. Differences in study design and statistical methods may have contributed to the observed differences.
Seasonal variation in birth of patients diagnosed with a specific disease, which differs from the underlying seasonality of births in the general population, suggests an environmental factor operating at conception, during pregnancy or in the neonatal period. Such a seasonal pattern may reflect for example variation in exposure to sunlight or to infections or variation of the diet.
We used nationwide cancer and population registers to determine whether there is a seasonal pattern in the births of children who later develop a CNS tumour compared with the distribution of births of the general population in Denmark.
Materials and methods
All children 0–19 years of age, who were diagnosed with a primary CNS tumour in the period 1970–2003 and registered in the Danish Cancer Registry, were included. Secondary tumours were excluded as treatment of a primary cancer is a known risk factor for secondary cancers (Maule et al, 2007). We included only tumours with a topography and morphology code defined in the International Childhood Cancer Classification second edition (ICCC-2; Kramarova and Stiller, 1996). In the period 1980–1996, all cases were validated using their medical records (Thorsteinsson et al, 2005).
The reference group included children born in 1970–2003, identified in the national Central Population Register (CPR) established in 1968 and subsequently used for all official personal registration of Danish citizens and residents. All live-born children are assigned a unique 10-digit CPR number, including the date of birth and gender code. A test for a sinusoidal variation was applied to evaluate changes of CNS tumour incidence by month of birth, adjusted for the background distribution of births (Walter and Elwood, 1975). The deviation of observed from expected numbers of cases was compared with a χ2-distribution with 2 degrees of freedom, and the timing of the peak was calculated. For comparison with a recent study (Hoffman et al, 2007), we defined the same subgroups by gender and age, young children aged 0–4 years at diagnosis and older children (5–19 years).
Results
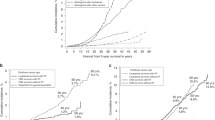
We identified 1640 eligible CNS tumour patients (Table 1) and the reference group comprised 2 582 714 children. Figure 1 illustrates the distributions of births in the general population, among patients with CNS tumours, and among ependymoma patients. Overall, no statistically significant evidence of seasonal variation of births was observed among patients with CNS tumour (Table 1). When stratifying by histology, we found a significant variation related to month of birth among children with ependymoma, with a peak in early January and a summer trough (Table 1). When examined by age and sex, ependymoma, showed a significant seasonal variation only at ages 5–19 years, and among girls (Table 1), but numbers in subgroups were small.

Distribution of births per month among patients with Central nervous system (CNS) tumours, ependymoma and among children in Denmark.
Discussion
The major strength of our study is its base in high quality population-based administrative registers, ensuring complete case ascertainment and an appropriate unbiased reference group. The Walter and Edwood test may perform poorly when numbers are small (St Leger, 1976), as in our analyses by gender and age. If the aetiologically relevant exposure period is during pregnancy, then differences in gestational age at birth might dilute a possible seasonality effect. As the proportion of premature births (gestational age <37 weeks) only is 6% (The Danish National Board of Health, 2007), this is unlikely to have had a significant influence on our findings.
Examination of seasonal variation of birth in CNS tumours have had inconsistent results (Yamakawa et al, 1982; Heuch et al, 1998; Feltbower et al, 2001; McNally et al, 2002; Halperin et al, 2004; Hoffman et al, 2007), and overall, no seasonal pattern of birth is suggested. Seasonal variations sometimes seen for diagnostic subgroups were not consistent, so chance may have operated. Such random effects may also explain the significant seasonality for ependymomas in children aged 5–19 years and at all ages in girls, as no aetiological differences in the ependymomas are known in these subsets. As associations in the same direction were found for younger children and for boys, the absence of statistical significance may reflect a lack of power.
Notably, all previous positive findings regardless of subgroup have concerned a peak of births in the fall or winter, but most lacked an appropriate population-based comparison group.
Ependymoma showed seasonality in only one previous study (McNally et al, 2002), although the peak observed in February was not statistically significant (Edwards test P=0.10). Astrocytoma showed a seasonal pattern in two studies (Heuch et al, 1998; McNally et al, 2002), and medulloblastoma seasonality by month of birth in three (Yamakawa et al, 1982; Heuch et al, 1998; Hoffman et al, 2007).
Studies of the risk of adult brain tumours have, as with children, all found a peak of birth in winter (Brenner et al, 2004; Halperin et al, 2004; Koch et al, 2006; Mainio et al, 2006), although no studies from the southern hemisphere are available.
Dates of diagnosis showed seasonal variation and strong evidence of space-time clustering in the United Kingdom among children with astrocytoma and ependymoma, also supporting a role of infections in their aetiology (McNally et al, 2002); however, in Sweden clustering was not observed (Hjalmars et al, 1999). When interpreting these results one should keep in mind that the interval between the onset of disease and diagnosis is variable and often long because of a combination of unspecific or initially few symptoms, patients' delay, as well as doctors' delay.
Seasonal variation of birth is a fairly crude proxy measure for more specific exposures that vary seasonally around the time of conception, during pregnancy or in the neonatal period. It is unclear whether this seasonal variation of births in CNS tumour reflects variations in exposure to specific infections, variable levels of the burden of community infections or other factors. Some studies have suggested that exposure to infections of the mother or the child around the time of birth may be associated with increased risk of certain CNS tumours in children (Linet et al, 1996; Linos et al, 1998; Dickinson et al, 2002; McNally et al, 2002). In addition, three polyomaviruses have shown oncogenic properties when injected into the brain of newborn laboratory animals (White et al, 2005). Also seasonal changes in hours of sunlight per month, especially at Northern latitudes, subsequently leads to fluctuation in vitamin-D levels. Vitamin-D has antiproliferative and pro-apoptotic properties and may be involved in carcinogenesis (Holick, 2007). However, little is known about any role of D-vitamin in CNS tumours (Ko et al, 2005). Dietary habits may also be related to season, but relevant data for Denmark are lacking.
Little is known of ependymoma aetiology, partly because they only account for approximately 10% of CNS tumours in children, and most studies lack sufficient numbers. A considerable fraction of spinal ependymoma is associated with mutations in the neurofibromatosis type 2 gene (NF2; Ebert et al, 1999). An inverse association between maternal consumption of vitamin supplements during pregnancy and ependymoma risk has been observed (Bunin et al, 1993), whereas no association with birth weight has been reported (Harder et al, 2008).
As potential proxy exposures to infectious diseases, space-time clustering has been noted in ependymoma (McNally et al, 2002), and one study reported an association with a high number of siblings (Altieri et al, 2006).
In conclusion our results confirm the findings from most previous studies that no seasonal variation of births is apparent, when combining all histological subgroups of childhood CNS tumours. We cannot exclude that our finding of a seasonal pattern of births among patients with ependymoma is simply due to chance. But the fact that all studies which have reported a seasonal variation of birth, even though evident for different histological subgroups of CNS tumours, show an excess of births either during fall or during winter, justifies further analysis of the seasonality of births in large scale studies.
Change history
16 November 2011
This paper was modified 12 months after initial publication to switch to Creative Commons licence terms, as noted at publication
References
Altieri A, Castro F, Bermejo JL, Hemminki K (2006) Association between number of siblings and nervous system tumors suggests an infectious etiology. Neurology 67: 1979–1983
Brenner AV, Linet MS, Shapiro WR, Selker RG, Fine HA, Black PM, Inskip PD (2004) Season of birth and risk of brain tumors in adults. Neurology 63: 276–281
Bunin GR, Kuijten RR, Buckley JD, Rorke LB, Meadows AT (1993) Relation between maternal diet and subsequent primitive neuroectodermal brain tumors in young children. N Engl J Med 329: 536–541
Dickinson HO, Nyari TA, Parker L (2002) Childhood solid tumours in relation to infections in the community in Cumbria during pregnancy and around the time of birth. Br J Cancer 87: 746–750
Ebert C, von HM, Meyer-Puttlitz B, Wiestler OD, Reifenberger G, Pietsch T, von DA (1999) Molecular genetic analysis of ependymal tumors. NF2 mutations and chromosome 22q loss occur preferentially in intramedullary spinal ependymomas. Am J Pathol 155: 627–632
Feltbower RG, Pearce MS, Dickinson HO, Parker L, McKinney PA (2001) Seasonality of birth for cancer in Northern England, UK. Paediatr Perinat Epidemiol 15: 338–345
Halperin EC, Miranda ML, Watson DM, George SL, Stanberry M (2004) Medulloblastoma and birth date: evaluation of 3 US datasets. Arch Environ Health 59: 26–30
Harder T, Plagemann A, Harder A (2008) Birth weight and subsequent risk of childhood primary brain tumors: a meta-analysis. Am J Epidemiol 168: 366–373
Heuch JM, Heuch I, Akslen LA, Kvale G (1998) Risk of primary childhood brain tumors related to birth characteristics: a Norwegian prospective study. Int J Cancer 77: 498–503
Hjalmars U, Kulldorff M, Wahlqvist Y, Lannering B (1999) Increased incidence rates but no space-time clustering of childhood astrocytoma in Sweden, 1973–1992: a population-based study of pediatric brain tumors. Cancer 85: 2077–2090
Hoffman S, Schellinger KA, Propp JM, McCarthy BJ, Campbell RT, Davis FG (2007) Seasonal variation in incidence of pediatric medulloblastoma in the United States, 1995–2001. Neuroepidemiology 29: 89–95
Holick MF (2007) Vitamin D deficiency. N Engl J Med 357: 266–281
Ko P, Eyles D, Burne T, kay-Sim A, McGrath JJ (2005) Season of birth and risk of brain tumors in adults. Neurology 64: 1317
Koch HJ, Klinkhammer-Schalke M, Hofstadter F, Bogdahn U, Hau P (2006) Seasonal patterns of birth in patients with glioblastoma. Chronobiol Int 23: 1047–1052
Kramarova E, Stiller CA (1996) The international classification of childhood cancer. Int J Cancer 68: 759–765
Linet MS, Gridley G, Cnattingius S, Nicholson HS, Martinsson U, Glimelius B, Adami HO, Zack M (1996) Maternal and perinatal risk factors for childhood brain tumors (Sweden). Cancer Causes Control 7: 437–448
Linos A, Kardara M, Kosmidis H, Katriou D, Hatzis C, Kontzoglou M, Koumandakis E, Tzartzatou-Stathopoulou F (1998) Reported influenza in pregnancy and childhood tumour. Eur J Epidemiol 14: 471–475
Little J (1999) Epidemiology of Childhood Cancer. IARC Scientific Publication: Lyon
Mainio A, Hakko H, Koivukangas J, Niemela A, Rasanen P (2006) Winter birth in association with a risk of brain tumor among a Finnish patient population. Neuroepidemiology 27: 57–60
Maule M, Scelo G, Pastore G, Brennan P, Hemminki K, Tracey E, Sankila R, Weiderpass E, Olsen JH, McBride ML, Brewster DH, Pompe-Kirn V, Kliewer EV, Chia KS, Tonita JM, Martos C, Jonasson JG, Merletti F, Boffetta P (2007) Risk of second malignant neoplasms after childhood leukemia and lymphoma: an international study. J Natl Cancer Inst 99: 790–800
McNally RJ, Cairns DP, Eden OB, Alexander FE, Taylor GM, Kelsey AM, Birch JM (2002) An infectious aetiology for childhood brain tumours? Evidence from space-time clustering and seasonality analyses. Br J Cancer 86: 1070–1077
St Leger AS (1976) Comparison of two tests for seasonality in epidemiological data. Appl Stat 25: 280–286
The Danish National Board of Health (2007) [Half-yearly report from the Danish Birthregistry] vol 15, www.sst.dk
Thorsteinsson R, Sorensen M, Jensen TL, Bernhardtsen TM, Gjerris F, Carstensen H, Schmiegelow K, Raaschou-Nielsen O (2005) [Central nervous system tumours in children. An evaluation of the completeness and validity of the Cancer Registry]. Ugeskr Laeger 167: 3782–3785
Wakeford R (2004) The cancer epidemiology of radiation. Oncogene 23: 6404–6428
Walter SD, Elwood JM (1975) A test for seasonality of events with a variable population at risk. Br J Prev Soc Med 29: 18–21
White MK, Gordon J, Reiss K, Del VL, Croul S, Giordano A, Darbinyan A, Khalili K (2005) Human polyomaviruses and brain tumors. Brain Res Brain Res Rev 50: 69–85
Yamakawa Y, Fukui M, Kinoshita K, Kano E (1982) [Seasonal variation of birth incidence of children with cerebellar medulloblastoma. A study in Fukuoka-Ohita area and in all Japan]. Neurol Med Chir (Tokyo) 22: 1002–1008
Acknowledgements
This work was supported by a grant from the Danish Cancer Society (229070559102).
Author information
Authors and Affiliations
Corresponding author
Additional information
DISCLOSURE/CONFLICT OF INTEREST
The authors declare no conflict of interest.
Rights and permissions
From twelve months after its original publication, this work is licensed under the Creative Commons Attribution-NonCommercial-Share Alike 3.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-sa/3.0/
About this article
Cite this article
Schmidt, L., Grell, K., Frederiksen, K. et al. Seasonality of birth in children with central nervous system tumours in Denmark, 1970–2003. Br J Cancer 100, 185–187 (2009). https://doi.org/10.1038/sj.bjc.6604813
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bjc.6604813
Keywords
This article is cited by
-
Population mixing for leukaemia, lymphoma and CNS tumours in teenagers and young adults in England, 1996–2005
BMC Cancer (2014)
-
Seasonal variation in the month of birth in patients with skin cancer
British Journal of Cancer (2014)
-
Infectious exposure in the first years of life and risk of central nervous system tumours in children: analysis of birth order, childcare attendance and seasonality of birth
British Journal of Cancer (2010)
