
Abstract
Data Sources
Relevant literature was selected following searches using the following: Cochrane Central Register of Controlled Trials, Medline, Embase (OVID), System for Information on Grey Literature in Europe, Latin American and Caribbean Health Sciences Literature, ISI Web of Science; and searches were made by hand of: Journal of the American Academy of Pediatric Dentistry, Anaesthesia, British Dental Journal, British Journal of Anaesthesia, Dental Update, International Journal of Paediatric Dentistry, Journal of American Dental Association, Journal of Dentistry for Children and Pediatric Dentistry.
Study selection
Reports were selected if they described randomised controlled clinical trials (RCT) of sedative agents compared with general anaesthesia in children and adolescents aged up to 18 years who were having dental treatment: complex surgical procedures and pseudo-randomised trials were excluded. There were no language restrictions.
Data extraction and synthesis
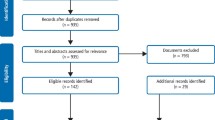
Titles and abstracts were assessed for inclusion by two authors with relevant information recorded in a specially designed data extraction form.
Results
Fifteen studies were identified for potential inclusion after searching the available databases and screening the titles and abstracts, and a further study was found through personal contacts. Following retrieval of the full text of the studies, it was concluded that none was eligible.
Conclusions
RCT that compare the use of dental general anaesthesia with sedation to quantify differences such as morbidity and cost are required.
Similar content being viewed by others


Commentary
It is disappointing, though not surprising to those working in this field, that no RCT were found that compared sedation with general anaesthesia (GA) for children. The decision to carry out treatment under sedation or GA depends on a whole range of factors, not all of which are dental and not all of which are easily quantifiable. There are often significant subjective and qualitative aspects involved in the decision-making process. Much depends upon local resources: difficulty in accessing GA can result in more patients being treated with sedation, or the converse when easy access to GA leads to no sedation provision. Parents' expectations influence the decision: many parents want or even demand that their child is asleep for dental care. Such parental bias can influence the child's behaviour. In the UK, intravenous sedation techniques in children have been viewed with suspicion, confirmed by guidance which limited the use of intravenous sedation to those over 16 years of age.1 The training and experience of the clinician and the prevailing local ethos also play a part. There is also understandable reluctance on the part of clinicians, when faced with an anxious child in pain, to suggest sedation techniques which may or may not be successful in allowing effective treatment of dental pain.
The UK's National Institute for Health and Clinical Excellence (NICE) is currently considering sedation for diagnostic and therapeutic procedures in children and young people (http://guidance.nice.org.uk/CG/Wave18/52). Their remit is to prepare clinical guidelines which will, no doubt, lead to changes in the provision of dental sedation for this group.
The authors' suggestion that, “carefully designed and well run RCTs are required” is an admirable one but may not be practicable. It will be very difficult to match patients' dental needs, medical problems and anxiety and then randomly assign them to GA or sedation groups.
The authors also hope that it will be possible to compare costs for sedation and GA: this may be possible in one setting but the figures will not necessarily be useful in other settings. For example, a session in a primary care environment is likely to be less expensive than sedation administered in a hospital where the staffing requirements are probably similar to that required for GA.
What is required for the optimal treatment of children is careful assessment of each individual and the availability of a range of techniques to control pain and anxiety, implemented in accordance with the principle of minimal intervention.
References
Scottish Intercollegiate Guidelines Network (SIGN) Guideline no. 58. Safe Sedation of Children Undergoing Diagnostic and Therapeutic Procedures. Edinburgh: SIGN; 2004.
Author information
Authors and Affiliations
Additional information
Address for correspondence: Paul F Ashley, Unit of Paediatric Dentistry, UCL Eastman Dental Institute, 256 Grays Inn Road, London, WC1X 8LD, UK. p.ashley@eastman.ucl.ac.uk
Ashley PF, Williams CECS, Moles DR, Parry J. Sedation versus general anaesthesia for provision of dental treatment in under 18 year olds. Cochrane Database Syst Rev 2009; issue 1
Rights and permissions
About this article
Cite this article
Boyle, C. Sedation or general anaesthesia for treating anxious children. Evid Based Dent 10, 69 (2009). https://doi.org/10.1038/sj.ebd.6400662
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.ebd.6400662
This article is cited by
-
Predicting the choice of anaesthesia for third molar surgery – guideline or the easy-line?
British Dental Journal (2013)
