
Abstract
Design
A four-arm, single-blind, randomised controlled trial (RCT) was conducted in the US. Randomisation was stratified by duration of decreased opening of temporomandibular joint (TMJ) at baseline, as either non-chronic (≤6 months) or chronic (>6 months).
Intervention
Participants with TMJ closed lock were randomised to one of the four initial treatment modalities: medical management, rehabilitation, arthroscopic surgery with postoperative rehabilitation, or anthroplasty with postoperative rehabilitation. Clinical examinations and questionnaires were completed at baseline and at 3, 6, 12, 18, 24 and 60 months.
Outcome measure
The primary outcome measures were the Craniomandibular Index (CMI) and the modified Symptom Severity Index (SSI) for jaw function and TMJ pain respectively. Treating clinicians assessed treatment compliance during the 6-month follow-up. Medication use was also assessed from data collected at follow-up visits.
Results
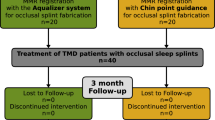
A total of 106 individuals were randomised to the four treatment modalities. Each participant received the assigned initial treatment modality for at least 3 months, after which some participants in each group needed additional interventions for persistent pain and reduced range of motion. Using an intention-to-treat analysis, no difference was observed between groups at any follow-up for CMI (P≥0.33) or SSI (P≥0.08). Both outcomes showed within-group improvement (P<0.0001) for all groups.
Conclusions
The findings of this study suggest that primary treatment for individuals with TMJ closed lock should consist of medical management or rehabilitation. The use of this approach will avoid unnecessary surgical procedures.
Similar content being viewed by others

Commentary
There is general agreement between clinicians that nonsurgical care should precede surgery for most temporomandibular disorders (TMD), the exception being the TMJ closed lock patient. The literature has failed to support this assertion, however. Studies comparing either nonsurgical options, surgical options, or nonsurgical with surgical options have found no difference in the efficacy of these therapies. Unfortunately, because of the nature and quality of published studies, the scientific evidence needed to validate there conclusions was lacking. As such, this is truly a benchmark study and hopefully a turning point in TMD research.
This is the first adequately powered randomised study to assess the effectiveness of four treatment strategies, ranging from minimal treatment to surgery, for individuals who have TMJ disc displacement without reduction and with limited opening (ie, closed lock). A very well-designed, single-blind RCT, it employs an intent-to-treat strategy. The latter approach mirrors clinical practice more closely by accepting that noncompliance and protocol deviations are likely to occur.1 In doing so, its results avoid overoptimistic estimates of treatment efficacy and are much more generalisable to the general population than studies using per-protocol or treatment-received analyses.2
Participants in this study, after being randomly assigned to an initial treatment strategy, were treated according to the preset protocols for that group for a minimum of 3 months, after which some individuals needed additional interventions to address persistent pain and limited mouth opening. Virtually all crossover of the patients in these four groups went from the medical management group into the rehabilitation group. Only two patients from these nonsurgical groups eventually required surgery and, from the initial surgery groups, three patients required additional surgery. After periodic evaluation of these patients over a 5-year period, this study found no differences between or within the any of the nonsurgical or surgical groups.
In summary, the strength of this study is that it simulates clinical practice. As pointed out, the medically managed group was not intended to be treated with medical management alone, but rather this was the approach with which treatment would be begun. Additional strategies, including surgery, were recommended as warranted, as would occur in a stepped-care approach in clinical practice.
Practice point
Initial treatment of both acute and chronic closed-lock patients should begin with medical management or rehabilitation.
References
Fisher L, Dixon D, Jerson J . Intention to treat in clinical trials. In Statistical Issues in Drug Research and Development. Edited by Peace K. New York: Marcel Dekker; 1990.
Hollis S, Campbell F . What is meant by intention to treat analysis? Survey of published randomized controlled trials. Br Med J 1999; 319:670–674.
Author information
Authors and Affiliations
Additional information
Address for correspondence: EL Schiffman, University of Minnesota School of Dentistry, Department of Diagnostic and Biological Sciences, 6-320 Moos Tower, 515 Delaware Street SE, Minneapolis MN 55455, USA. E-mail: schif001@umn.edu
Schiffman EL, Look JO, Hodges JS, et al. Randomized effectiveness study of four therapeutic strategies for TMJ closed lock. J Dent Res 2007; 86:58–63
Rights and permissions
About this article
Cite this article
Tylka, D. Non-surgical care should be the primary treatment for TMJ closed lock. Evid Based Dent 8, 112 (2007). https://doi.org/10.1038/sj.ebd.6400529
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.ebd.6400529
