
Abstract
Aneurysmal bone cyst and giant cell tumor of bone are relatively rare bone tumors that sometimes coexist. We examined the karyotypes of 3 aneurysmal bone cysts, 12 giant cell tumors, and 3 combined lesions. All aneurysmal bone cysts showed involvement of chromosome segments 17p11–13 and/or 16q22. In addition, in 1 of the 3 giant cell tumors with secondary aneurysmal bone cyst, both chromosome bands were rearranged as well, albeitnot in a balanced translocation. Seven out of 12 giant cell tumors were characterized by telomeric associations. One giant cell tumor showed a dup(16)(q13q22), suggesting the presence of a (minor) secondary aneurysmal bone cyst component, despite the absence of histological proof. Our results, combined with literature data further substantiate that segments 16q22 and 17p11–13 are nonrandomly involved in at least some aneurysmal bone cysts, irrespective of subtype (primary, secondary, intra/extraosseous, solid or classic). These findings strongly suggest that some aneurysmal bone cysts are true neoplasms. In addition, telomeric associations are the most frequent chromosomal aberrations in giant cell tumor of bone, the significance of which remains elusive. In combined giant cell tumor/aneurysmal bone cyst each component seems to retain its own karyotypic abnormality.
Similar content being viewed by others

INTRODUCTION
Aneurysmal bone cysts are benign, but often rapidly expanding osteolytic multicystic lesions. They usually occur in young patients (first 3 decades), and exhibit a slight female predominance. The metaphysial region of long bones and vertebrae account for 70 to 80% of the cases, with the distal femur and proximal tibia being the most common sites (1). Aneurysmal bone cysts are generally considered of reactive nature, and about 50% of them are ‘secondary’, i.e., associated with other entities, the most frequent being giant cell tumor, chondroblastoma and fibrous dysplasia. Giant cell tumor of bone is about twice as common as aneurysmal bone cyst and typically involves the epiphysis of tubular bones of skeletally mature patients over the age of 20 years (2). In contrast to aneurysmal bone cyst, giant cell tumor of bone is generally regarded as a neoplastic process. This assumption is partly based on the fact that giant cell tumors can be locally invasive and metastasize.
In 1994, an international collaborative group (the CHromosomes And MorPhology study group), comprising cytogeneticists, pathologists and surgeons was established to carry out a systematic study of a variety of solid tumors. The aim of the present study is to analyze the karyotypic changes in aneurysmal bone cyst, giant cell tumor and combined lesions, to correlate these changes with the morphology, and to compare the findings with those in the literature.
MATERIALS AND METHODS
From a variety of primary bone tumors which were successfully karyotyped in Leuven and Lund between 1989 and 1999, 3 primary aneurysmal bone cysts, 12 giant cell tumors and 3 giant cell tumors with secondary aneurysmal bone cyst (combined lesions) were retrieved. For cytogenetic analysis, fresh tumor specimens were disaggregated with collagenase, cultured (for less than 10 days), harvested and characterized by G- band staining. Chromosomal aberrations were reviewed without knowledge of the final diagnosis, and described according to the International System for Human Cytogenetic Nomenclature (3). The histologic features were reexamined separately by four group members (HD, CDMF, JR, GT) without knowledge of the clinical or karyotypic data. In all cases standard radiographs and CT or MRI data, when available, were also reevaluated (PB, KJ). Group members met subsequently and correlated the morphologic, karyotypic and clinical data in each case.
RESULTS
The clinical, histopathologic and cytogenetic findings are summarized in Table 1. The karyotype of one aneurysmal bone cyst was published previously (case 1) (4). The mean age of the 3 patients with primary aneurysmal bone cyst was 21 years (range 13–33 years), and the tibia or fibula were involved in all cases. In case 1, the lesion recurred after 6 months. Among the 15 patients (8 women, 7 men) with a giant cell tumor with or without secondary aneurysmal bone cyst, the mean age was 30 years (range 19 to 51 years). The epiphyses of femur and tibia were the most frequent locations. Three tumors were localized in the small bones of the hand or foot. Three tumors recurred, but none metastasized.
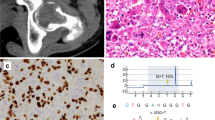
Histologically, all 3 primary aneurysmal bone cysts showed the typical irregular pseudovascular spaces, separated by fibrous septa containing fibroblasts, histiocyte-like cells, multinucleated giant cells and reactive bone lamellae (Fig. 1). Imaging studies confirmed the presence of a multilocular radiolucent ‘blown-out’ picture and of fluid/fluid levels.

Aneurysmal bone cyst showing the characteristic irregular vascular spaces and septa with giant cells (hematoxylin and eosin stain, original magnification, 325 ×).
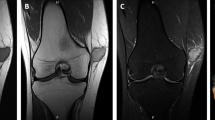
The 12 pure giant cell tumors were characterized by numerous osteoclast-like multinucleated giant cells regularly scattered among mononuclear ‘stromal’ cells with round to oval nuclei (Fig. 2). Three tumors were localized in the small bones of the hands/feet. In this location a giant cell reparative granuloma is more likely, but the tumors were histologically identical to the giant cell tumors in the more classic locations. Although a clearcut distinction between giant cell reparative granuloma and giant cell tumor is not always evident, the uniform distribution of the giant cells, the diffuse presence of characteristic stromal mononuclear cells and the lack of a fibrotic/hemorrhagic stroma, render the diagnosis of a giant cell reparative granuloma unlikely. No tumor showed histologic evidence of sarcomatous transformation. In 4 cases, an associated fibrohistiocytic reaction was present, with foamy cells, lymphocytes and histiocytes. Imaging studies showed a typical, purely lytic, destructive lesion involving the end of the bone, often abutting the articular cartilage. Some cases showed cortical erosion. In 2 giant cell tumors (cases 4 and 5) a secondary aneurysmal bone cyst was documented on histology. In a third case (case 6), the secondary aneurysmal bone cyst component was strongly suspected on radiologic grounds, but not on histology. On plain radiographs, the fractured lesion had the appearance of a giant cell tumor, consisting in a relatively well delineated lytic lesion in the lateral femoral condyle. It involved both the metaphysis and the epiphysis and measured 10 × 6 × 5 cm. There seemed to be sclerotic septations. On MRI, a component strongly suggestive of aneurysmal bone cyst became evident, with several fluid/fluid levels, without fairly well demarcated septa.

Giant cell tumor, characterized by numerous osteoclast-like giant cells and surrounding mononuclear cells with similar nuclei (hematoxylin and eosin stain, original magnification, 325 ×).
In the 3 cases of aneurysmal bone cyst, chromosome segment 17p11–13 was involved in translocations, band 16q22 being the translocation partner in case 1. Telomeric associations were the most frequent chromosomal aberrations in the pure giant cell tumors, being detected in 7 of the 12 cases. Telomeric associations represent the end to end fusion of cytogenetically-appearing ‘whole’ or ‘intact’ chromosomes (5). Various numerical and/or structural anomalies were present in the remaining cases, and in four tumors with telomeric associations. Interestingly, one giant cell tumor showed involvement of 16q22, albeit not in a balanced translocation (dup(16(q13q22), case13). In 1 of the 3 combined lesions (case 5), both the 16q22 and 17p13 rearrangements were detected, as del(16(q22) and add (17)(p13), respectively. None of these 2 tumors had telomeric associations.
DISCUSSION
There are only limited data in the literature on chromosomal aberrations in aneurysmal bone cyst. In fact, the initial reports only revealed normal karyotypes (6, 7). Of the 7 published cases with an abnormal karyotype, including the 3 cases presented here, one appeared as a soft tissue mass and one corresponded to the so-called ‘solid variant’ of aneurysmal bone cyst (Tables 1 and 2) (4, 8). Interestingly, all cases showed involvement of 17p11–13 and/or 16q22. In 2 cases both 17p13 and 16q22 were involved in a balanced translocation. In 3 cases only 17p11–13 was involved, with other chromosomal segments as the translocation partner. Solitary involvement of 16q22 was seen in two cases, presenting as a deletion in one case and as a balanced translocation in another. In addition, among the 3 cases of secondary aneurysmal bone cyst in the present series, one showed 16q22 and 17p13 involvement (case 5), albeit not in a balanced translocation. Thus, it appears from these, admittedly limited data, that chromosome bands 16q22 and/or 17p11–13 are nonrandomly rearranged in aneurysmal bone cyst, irrespective of subtype (classic, solid, primary, secondary) and location (osseous or extraosseous). It seems likely that one or both regions harbor(s) a gene of primary importance in the development of aneurysmal bone cyst.
The most widely accepted pathogenetic hypothesis for aneurysmal bone cyst is some local circulatory disturbance, leading to markedly increased venous pressure and the development of a dilated and enlarged vascular bed within the affected bone area (9). However, the consistent chromosomal pattern suggests that at least some of these lesions are in fact neoplastic. Interestingly, one previously published case of combined aneurysmal bone cyst and giant cell tumor showed an increased telomeric association, typical of giant cell tumor (6). Aneurysmal bone cyst and giant cell tumor seem to retain their karyotypic characteristics in the combined lesions, and the result of the cytogenetic analysis is probably determined by whether the sample is derived from the aneurysmal bone cyst component of the tumor or from the giant cell tumor component.
The results from the analysis of the 12 giant cell tumors confirm that telomeric association is the most frequent chromosomal aberration in this entity (5). Telomeres are guanine rich structures capping the chromosome termini. They prevent aberrant recombination and protect chromosomes against exonucleolytic DNA degradation. In addition, telomeres are supposed to be involved in senescence and immortalisation of normal cells (10, 11). The role of telomeric association in giant cell tumor and the molecular consequences of this phenomenon have not been fully elucidated. A reduction in telomere length (average loss of 500 base pairs) has been demonstrated in giant cell tumor cells when compared to leukocytes from the same patients (12). The telomeres most commonly affected are 11p, 15p, 19q, 20q and 21p (5, 13). Except for a clonal telomeric association affecting 11q and 19q, none of these chromosome termini were involved in structural aberrations in the present cases.
It is of interest that the giant cell tumors with a fibrohistiocytic reaction did not differ karyotypically from the others. This finding supports the hypothesis that these lesions are true giant cell tumors rather than a different entity like a fibroxanthoma. None of the tumors here studied showed a malignant behavior or a malignant histological picture, so a possible correlation between an eventually unfavorable outcome and chromosomal changes other than telomeric association could not be studied. In case 13, chromosome band 16q22 was involved in a dup(16)(q13q22). The finding of a 16q duplication may be coincidental, but it cannot be exluded that a minor secondary aneurysmal bone cyst component was present, the absence of histological or radiological support for this hypothesis notwithstanding. It is of interest that three previously published cases of giant cell tumor also showed rearrangements in 16q22 or 17p13 (14, 15). Obviously, the crucial question in these cases concerns the possible presence of an associated aneurysmal bone cyst.
In conclusion, the presented data and reviewed data from the literature confirm that 16q2 and/or 17p1 are nonrandomly involved in all types of aneurysmal bone cyst, a finding that should facilitate identification of specific genes involved. Giant cell tumor of bone is characterized by telomeric associations, the significance of which remains somewhat enigmatic, although a major role for telomeres and telomerase in oncogenesis is increasingly being recognized. Although additional cases should be studied, it appears that in combined giant cell tumor and secondary aneurysmal bone cyst, each lesion can retain its characteristic chromosomal aberration.
References
Dorfman HD, Czerniak B, editors. Cystic lesions. In: Dorfman HD, Czerniak B, editors. Bone tumors. St. Louis, MO: Mosby; 1998. p. 855–912.
Dorfman HD, Czerniak B, Leditors. Giant cell lesions. In: Dorfman HD, Czerniak B, editors. Bone tumors. St. Louis, MO: Mosby; 1998. p. 559–606.
Mitelman F, editor. ISCN (1995): An International System for Human Cytogenetic Nomenclature. Basel, Switzerland: S. Karger; 1995.
Panoutsakopoulos G, Pandis N, Kyriazoglou I, Gustafson P, Mertens F, Mandahl N . Recurrent t(16;17)(q22;p13) in aneurysmal bone cysts. Genes Chromosomes Cancer 1999; 26: 265–266.
Sandberg AA, Bridge JA, editors. The cytogenetics of bone and soft tissue tumors. Austin: RG Landes Company; 1994. p. 35–74.
Pfeiffer FM, Bridge JA, Neff JR, Mouron BJ . Cytogenetic findings in aneurysmal bone cysts. Genes Chromosomes Cancer 1991; 3: 416–419.
Tarkkanen M, Kaipainen A, Karaharju E, Bšhling T, Szymanska J, et al. Cytogenetic study of 249 consecutive patients examined for a bone tumor. Cancer Genet Cytogenet 1993; 68: 1–21.
Dal Cin P, Kozakewich HP, Goumnerova L, Mankin HJ, Rosenberg AE, Fletcher JA . Variant translocations involving 16q22 and 17p13 in solid and extraosseous forms of aneurysmal bone cyst. In press, Genes Chromosomes Cancer.
Schajowicz F . Tumorlike lesions. In: Schajowicz F, editor. Tumors and tumorlike lesions of bone. Berlin: Springer-Verlag; 1994. p. 505–612.
Soria JC, Vielh P, El-Naggar AK . Telomerase activity in cancer: a magic bullet or a mirage. Adv Anat Pathol 1998; 5: 86–94.
Wynford-Thomas D . Cellular senescence and cancer. J Pathol 1999; 187: 100–111.
Schwartz HS, Dahir GA, Butler MG . Telomeric reduction in giant cell tumor of bone and with aging. Cancer Genet Cytogenet 1993; 71: 132–138.
Mandahl N, Mertens F, Willen H, Rydholm A, Kreicbergs A, Mitelman F . Nonrandom pattern of telomeric associations in atypical lipomatous tumors with ring and giant marker chromosomes. Cancer Genet Cytogenet 1998; 103: 25–34.
Molenaar WM, Van den Berg E, Dolfin AC, Zorgdrager H, Hoekstra HJ . Cytogenetics of fine needle aspiration biopsies of sarcomas. Cancer Genet Cytogenet 1995; 84: 27–31.
Bridge JA, Neff JR, Mouron BJ . Giant cell tumor of bone. Chromosomal analysis of 48 specimens and review of the literature. Cancer Genet Cytogenet 1992; 58: 2–13.
Author information
Authors and Affiliations
Corresponding author
Additional information
This text presents research results of the Belgian program on Interuniversity Poles of Attraction initiated by the Belgian State, Prime Minister's Office, Science Policy Programming. The scientific responsibility is assumed by the authors.
Rights and permissions
About this article
Cite this article
Sciot, R., Dorfman, H., Brys, P. et al. Cytogenetic-Morphologic Correlations in Aneurysmal Bone Cyst, Giant Cell Tumor of Bone and Combined Lesions. A Report from the CHAMP Study Group. Mod Pathol 13, 1206–1210 (2000). https://doi.org/10.1038/Modpathol.3880224
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/Modpathol.3880224
Keywords
This article is cited by
-
Surgical Management and Denosumab for Aneurysmal Bone Cysts of the Spine in an Australian Tertiary Paediatric Centre
Calcified Tissue International (2023)
-
Rare aneurysmal bone cysts: multifocal, extraosseous, and surface variants
European Journal of Orthopaedic Surgery & Traumatology (2020)
-
Aneurysmal bone cyst: results of an off label treatment with Denosumab
BMC Musculoskeletal Disorders (2019)
-
Morphologisches Spektrum USP6-rearrangierter Läsionen
Der Pathologe (2018)
-
Aktueller Stand der Molekularpathologie von Knochentumoren
Der Onkologe (2013)
