
Abstract
The study aimed to determine the accuracy of diagnosing periodontal conditions using the developed web-based PocketPerio application and evaluate the user’s perspective on the use of PocketPerio. First, 22 third-year dental students (DS3) diagnosed ten cases without PocketPerio (control) and with PocketPerio (test) during a mock examination. Then, 105 DS3, 13 fourth-year dental students (DS4), and 32 senior second-year International Standing Program students (ISP2) used PocketPerio chairside. Statistical analysis was performed using a non-parametric paired two-tailed test of significance with the Wilcoxon matched-pairs signed rank test. The null hypothesis that PocketPerio did not increase the accuracy of periodontal diagnoses was rejected at α < 0.01. Periodontal diagnoses made using PocketPerio correlated with those made by periodontics faculty (“gold standard") in all cases. During the mock examination, PocketPerio significantly increased the accuracy of periodontal diagnoses compared to the control (52.73 vs. 13.18%, respectively). Chairside, PocketPerio significantly increased the accuracy of primary (100 vs. 40.0%) and secondary (100 vs. 14.25%) periodontal diagnoses compared to the respective controls. Students regardless of their training year felt more confident in diagnosing periodontal conditions using PocketPerio than their current tools, provided positive feedback on its features, and suggested avenues for its further development.
Similar content being viewed by others


Introduction
In 2017, the joint Workshop of the American Academy of Periodontology (AAP) and the European Federation of Periodontology (EFP) proposed the updated classification of periodontal and peri-implant diseases and conditions1. The classification introduced several key changes to definitions of periodontitis aimed to better reflect both biological and clinical disease dimensions with the intended use in clinical practice, clinical research, and epidemiologic studies1,2,3. These changes included but were not limited to (i) combining “chronic” and ”aggressive” phenotypes of periodontitis into a single “periodontitis” disease entity; (ii) defining periodontitis as the presence of interproximal clinical attachment loss (CAL) in ≥ 2 non-adjacent teeth or ≥ 3 mm buccal or lingual CAL in ≥ 2 teeth associated with inflammatory periodontal breakdown, and (iii) introducing the concepts of staging (reflecting the severity of periodontal breakdown) and grading (reflecting the rate of periodontal breakdown progression). Based on the severity, periodontitis was classified as stage I (initial periodontal breakdown—defined as a combination of 1-2 mm CAL and 4 mm pocket depth, PD), stage II (moderate periodontal breakdown – defined as a combination of 3-4 mm CAL and 5 mm PD), and stages III/IV (severe periodontal breakdown – defined as a combination of ≥ 5 mm CAL and ≥ 6 mm PD). Based on the progression rate, periodontitis was classified into grades A (the slow rate of progression), B (the moderate rate of progression), and C (the rapid rate of progression). The proposed updates were reflected in patient characteristics and the diagnostic accuracy of periodontal conditions4 and demonstrated a similar or greater diagnostic accuracy compared to diagnostic determinants proposed by the Community Periodontal Index and AAP together with the Centers for Disease Control and Prevention (CDC)5,6,7,8,9.
Accepting and using the updated classification in daily practice has been a continuous process, especially due to the presence of various “gray zone” clinical scenarios with overlapping clinical and radiographic findings10,11,12. A retrospective study using referral letters showed that although most patients (85%) were diagnosed using the updated disease definitions, the accuracy of periodontal diagnosis was relatively low (50.7 and 57.3% agreement for staging and grading, respectively)13. Other recent studies have shown that inter-participant agreement was 68.7–76.6, 75.5–82.0, and 82.4–84.8% for periodontitis staging, grading, and extent, respectively14,15. However, the agreement with all three diagnosis components (stage, grade, and extent) was low (47.2%)16. Furthermore, dental providers with limited exposure to periodontics found a differential diagnosis of periodontal conditions using the updated classification even more challenging compared to periodontists17,18. In addition, disparities in preexisting didactic and clinical knowledge can influence the performance of trainees diagnosing periodontal conditions chairside. Therefore, it is essential for dental educators to comprehensively understand the classification and effectively teach future dental providers to apply it chairside. This, in turn, requires the development of a straightforward approach to recognize and perform a differential diagnosis of periodontal conditions.
Several AAP/EFP Workshop-based diagrams and tables were developed to allow for a better understanding of clinical determinants of periodontal conditions and ensure their accurate diagnosis1,2. Several studies have described illustrative charts to improve the accuracy of periodontal diagnosis19,20,21. In our previous study, predoctoral dental students provided positive feedback on the use of the flowcharts and suggested developing a software application that would use a similar decision-tree approach to diagnose a wide variety of periodontal conditions21. Therefore, the goals of the present study were three-fold: (i) to address the needs of the educational community by developing a software application as a tool to assist in diagnosing a wide spectrum of periodontal conditions, (ii) to determine its accuracy in diagnosing periodontal conditions, and (iii) to evaluate the feedback of application users.
Methods
Ethics
All experimental protocols were approved by the Committee for the Protection of Human Subjects of the Institutional Review Board (IRB) of the University of Texas Health Science Center at Houston, School of Dentistry (UTSD, protocol #HSC-DB-18–0663 from October 28, 2020) and Colorado Multiple IRB of the University of Colorado Anschutz Medical Campus, School of Dental Medicine (CUSDM, protocol #22–2206 from January 6, 2023). For the mock examination held in March 2021 and to provide feedback, all students consented to participate in the respective activities by following respective invitation links. For the chairside use of PocketPerio in January–May 2023, an Information sheet/Postcard consent was used to obtain verbal consent since the IRB found that all criteria for waving the documentation of consent were met. The study was conducted in accordance with relevant IRB guidelines and regulations and principles of the 1975 Declaration of Helsinki, as revised in 201322. The results were reported according to the 2016 Standards for Reporting of Diagnostic Accuracy Studies statement23.
Technical specifications of PocketPerio
PocketPerio is a web-based application developed leveraging the Flutter software development kit and the Dart programming language. The implementation of both Flutter and Dart allows for PocketPerio portability across different platforms and web applications and the simplification of the application content and code updates. For future updates, PocketPerio is built to take advantage of update tools within the Flutter and Dart architecture, allowing for the classification changes to be implemented promptly. PocketPerio can be used on any mobile device running Android (version 4.1.x and above) or iOS (version 8 and above) and any device running Google Chrome, Microsoft Edge, Mozilla Firefox, or Safari web browsers. The decision-tree structure allows for a more expanded set of guidelines or amendments to the current guidelines to be inserted without incurring significant development time or overusing valuable development resources.
The questions and answer choices in the decision-tree algorithm of PocketPerio were based on the published Workshop guidelines in the “Resources” section of the application (Fig. 1A). In addition to a proposed periodontal diagnosis, PocketPerio includes definitions of periodontal terms (Fig. 1B), information icons with further explanations to clarify questions and answer choices (Fig. 1C and D), and suggested treatment options. Representative decision-tree approaches to diagnose clinical gingival health on intact periodontium and peri-implant health are shown in Fig. 1E and F, respectively. The process of arriving at the diagnosis of generalized periodontitis stage IV grade C and tooth- and prostheses-related factors is shown in Video 1.

The interface and features of PocketPerio. (A) The “Resources” section of the application includes the list of peer-reviewed publications used to develop the decision-tree algorithm of questions and answers. (B) The “Definitions” section includes definitions of the most common conditions and abbreviations used throughout the application. (C) One of the main pages of the application that guides a user to answer questions. (D) The information icons contain a more detailed explanation and supportive material that helps users accurately understand the questions and choose the most appropriate answer. (E) and (F) Representative questions and answers are shown that lead to the diagnosis of clinical gingival health on an intact periodontium and peri-implant health, respectively. Note that each diagnosis follows by the suggested treatment options.
Eligibility criteria
The following participants met the inclusion criteria: (i) predoctoral dental students providing patient care at the UTSD and CUSDM and who (ii) completed didactic periodontics course(s) that taught the 2017 periodontal classification, and (iii) consented to participate in the study.
Study design and methodology
The first part represented a crossover study conducted among UTSD third-year dental students (DS3) in the form of a mock examination/diagnosis. All participants received an online invitation to participate in the study and were informed that their decision to participate in the study was voluntary and would have no impact on their academic performance. The consented students (n = 22) took a classroom examination that consisted of ten clinical periodontal cases described previously21. The participants first diagnosed periodontal conditions using their curriculum-based knowledge and any available curriculum-based study materials including but not limited to lecture notes, decision-tree flowcharts21, and Workshop-based tables and diagrams24 that served as reference standards (control). Immediately after that, the participants diagnosed the same clinical cases using PocketPerio (test). Students recorded their answers, and the duration of their examination was recorded; however, no other identifiers were recorded. The elapsed time was not suspended once the participants started the examination. The participants were also asked to provide optional anonymous feedback on the use of PocketPerio.
The second part of the study represented a longitudinal study conducted among CUSDM DS3, fourth-year dental students (DS4), and 32 senior second-year International Standing Program students (ISP2) performing clinical chairside periodontal diagnosis of new patients who presented for the comprehensive periodontal examination. The patients had no history of periodontal treatment. The participants were asked to diagnose periodontal conditions using any available curriculum-based study materials that served as reference standards (control). Immediately afterwards, they were asked to diagnose periodontal conditions using PocketPerio (test). The same student could see more than one patient, but no patient was diagnosed more than once throughout the study. The accuracy of chairside diagnosis was calculated as the ratio between the diagnosis made without PocketPerio to that made using PocketPerio. Periodontics faculty supervising students' patient care also recorded their diagnosis(es) that served as reference “gold standards.” All faculty were calibrated through a series of departmental calibration sessions on the periodontal classification. A five-point Likert scale was used to evaluate the chairside participant’s responses to the following two questions: “How difficult was it for you to diagnose periodontal conditions without PocketPerio?” and “How difficult was it for you to diagnose periodontal conditions with PocketPerio?” Possible answers included “very easy/score 5”, “easy/score 4”, “moderate/score 3”, “difficult/score 2”, and “very difficult/score 1”). All responses were de-identified; however, the year of training was recorded for further stratification purposes. The survey was run using the Qualtrics software.
All students who used PocketPerio chairside were also asked to use Qualtrics software and provide additional anonymous feedback by answering six questions: “How difficult was it for you to diagnose periodontal conditions without PocketPerio?”, “How difficult was it for you to diagnose periodontal conditions with PocketPerio?”, “What feature(s) of PocketPerio did you like the best?”, “What feature(s) of PocketPerio did you find not helpful?”, “If you were to make updates to PocketPerio, what would you change?”, and “Would you use PocketPerio in your practice?” The participants were also allowed to add optional free-text comments. Although the responses were anonymous, the participants were asked to provide their years of training for further stratification purposes.
Study outcomes
For the first part of the study (mock examination), the accuracy of periodontal diagnosis served as the study's primary outcome, and the duration of the examination was the secondary outcome. For the second (chairside) part of the study, the diagnostic accuracy of primary periodontal conditions served as the primary outcome. The diagnostic accuracy of secondary periodontal conditions and the duration of time needed to diagnose these conditions served as secondary outcomes. Periodontal conditions were stratified into primary and secondary diagnoses. Primary conditions included dental biofilm-induced periodontitis2. Secondary diagnoses included periodontitis as a manifestation of systemic diseases24, tooth- and prosthesis-related factors25, traumatic occlusal forces26, periodontal abscess27, and endodontic-periodontal lesions27.
Null hypothesis
The use of PocketPerio did not increase the accuracy of diagnosing periodontal conditions.
Power calculation
The determine the sample size, the MKPower program in R was used to simulate power for the Wilcoxon signed-rank test. First, a range of sample sizes from 10 to 100 was considered to estimate the range of sample sizes needed to achieve a power of at least 0.8. Second, power for the sample sizes within this range was calculated to identify the smallest sample size for obtaining a power of 0.8. The proportion of correct diagnoses was assumed to have a normal distribution with a mean of 20% and a standard deviation of 10%. In the first step, to consider a range of sample sizes, the sim.ssize.wilcox.test function in MKPower was used assuming that the true value of the difference in correct diagnoses between control and test conditions was 10%, the test was a two-sided paired test, sample sizes were between 10 and 100, and the significance level was 0.01. Simulations from 10,000 iterations resulted in a power of 0.47 for a sample size of 10 and a power of 0.92 for a sample size of 20. In the second step, to determine the minimum sample size needed for a power of 0.8, the sim.ssize.wilcox.test function in MKPower was used to calculate the power for sample sizes between 10 and 25, assuming the same parameters as in the first step. Simulations from 10,000 iterations showed that power ranged from 0.47 to 0.97 for these sample sizes. A power of 0.81 could be achieved with a sample size of 16, which was the minimum sample size considered for the study. In the simulations, a power of 0.95 could be obtained with a sample size of 22 participants.
Statistical analysis
The comparison between control and test groups was performed using a non-parametric paired two-tailed test of significance with the Wilcoxon matched-pairs signed rank test. Statistical analysis was performed using GraphPad Prism 10 (GraphPad Software, San Diego, CA, USA), and the null hypothesis was rejected at α < 0.01. The word “significant” throughout the text refers to statistical significance.
Results
The use of PocketPerio during the mock examination
The mock examination was performed among UTSD DS3s in the middle of their academic year. The students were provided with instructions on how to use PocketPerio prior to the examination. Figure 2A shows that PocketPerio significantly increased the percentage of accurate diagnoses of both primary and secondary conditions (52.73 vs. 13.18%, respectively; p = 0.0000). No significant differences were observed between (i) test and control groups regarding the accuracy of diagnosing the primary condition when the diagnosis of the secondary condition was missing (38.18 vs. 31.82%, respectively; p = 0.10; Fig. 2B) and (ii) the duration of the examination (13.60 vs. 12.75 min, respectively; p = 0.36; Fig. 2C). Post-examination survey demonstrated that 75% of students were comfortable diagnosing periodontal conditions using their didactic knowledge and available supplemental resources (Fig. 2D). Almost all students (95%) were comfortable diagnosing periodontal diseases using PocketPerio (Fig. 2E). Several participants provided positive feedback on the use of PocketPerio (all responses are listed in Fig. 2F).

The accuracy and duration of the mock examination. DS3 who participated in the mock examination reviewed ten clinical cases first using their didactic knowledge and any additional tools (without PocketPerio, control) and then using PocketPerio (test). The participants had a brief overview of PocketPerio before the examination. PocketPerio significantly improved the accuracy of diagnosing both primary and secondary diagnoses (52.73 ± 2.88 vs. 13.18 ± 2.82, respectively, p = 0.0000; Panel A); however, the accuracy of diagnosing secondary conditions (38.18 ± 2.99 vs. 31.82 ± 2.84, respectively, p = 0.103; Panel B) and the duration of the examination (13.60 ± 0.93 vs. 12.75 ± 0.61 min, respectively, p = 0.36; Panel C) were similar between the control and test groups. In Panels A-C, the numbers above each bar represent the respective percentages in each category. Most students (75%) were comfortable with diagnosing periodontal conditions using their didactic knowledge without PocketPerio (Panel D); however, almost all students (95%) were comfortable doing so using PocketPerio (Panel E). Several participants provided their feedback on the use of PocketPerio during the mock examination. Representative unedited comments are shown in Panel F. DS3 Third-year dental students.
The chairside use of PocketPerio
A total of CUSDM 150 students (105 DS3, 13 DS4, and 32 ISP2) participated in the chairside use of PocketPerio. Table 1 shows the frequencies of periodontitis diagnosed chairside. The most common diagnoses were generalized periodontitis stage IV grade C (43/150 cases, or 41.86%) followed by localized periodontitis stage III grades B and C (25/150 cases, or 16.67% for both diagnoses). No patients were diagnosed with generalized periodontitis stage II grade C, generalized periodontitis stage III grade A, generalized periodontitis stage IV grade A, and molar-incisor pattern periodontitis stage III grades A and B. When stratified by each diagnosis component separately, the most common disease extent was generalized followed by the localized and molar-incisor patterns (66.67, 32.67, and 0.67%, respectively). The most common stage was IV followed by III, and II (46.0, 42.0, and 12.0%, respectively). No patients were diagnosed with stage I (0%). Grade B was the most common one followed by grades C and A (52.67, 44.0, 3.33%, respectively).
Table 1 also shows that the overall accuracy of diagnosis was 40.00 and 100% for the control and test groups. For the control group, the highest accuracy was demonstrated in diagnosing generalized periodontitis stage III grade B (73.33% of correct diagnoses) and localized periodontitis stage III grade B (68.0% of correct diagnoses). The lowest accuracy was observed while diagnosing localized periodontitis stage III grade C (6.67% of correct diagnoses). When stratified based on the year of training, ISP2 students had the highest diagnostic accuracy among control group students, followed by DS4 and DS3 (46.88, 38.46, and 38.10%, respectively). For DS3, the easiest diagnoses were generalized and localized periodontitis stage III grade B (87.5 and 66.67% of accurate diagnoses, respectively). For DS4, the easiest diagnoses were localized periodontitis stage III grades A and C and generalized periodontitis stage III grade B (100% accuracy for all diagnoses).
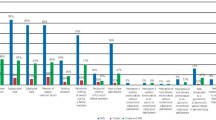
All 150 patients (100%) presented with at least one secondary periodontal condition identified while using PocketPerio. Table 2 shows that tooth- and prostheses-related factors were the most common condition followed closely by occlusal trauma, mucogingival deformities and conditions around teeth, periodontitis as a manifestation of systemic diseases, endodontic-periodontal lesions, and periodontal abscess (86.0, 84.67, 30.67, 29.33, 11.33, and 8.67%, respectively). Without using PocketPerio, secondary periodontal conditions were noted in 54 cases (14.25%), and only in two cases they were as complete as with PocketPerio. Among them, mucogingival deformities and conditions around teeth were the easiest condition to diagnose followed by endodontic-periodontal lesions, occlusal trauma, periodontitis as a manifestation of systemic diseases, and tooth- and prosthesis-related factors (57.7, 11.11, 11.0, 8.16, and 3.88%, respectively). No cases of periodontal abscess were diagnosed. When stratified based on the year of training, frequencies of diagnosing secondary conditions were the highest among DS4 followed by ISP2, and DS3 (25.89%, 17.72, and 12.03%, respectively). It is important to note that even if the secondary condition was identified by control students, no diagnosis was verbalized precisely according to the 2017 classification.
The participant’s feedback on the use of PocketPerio
The participants who used PocketPerio chairside were also asked to provide optional anonymous feedback on their comfort level of diagnosing periodontal conditions without and with PocketPerio (Supplementary Table 1). A total of 18 students (7, 6, and 5 DS3, DS4, and ISP2, respectively) completed the survey. The 5-point Likert scale was used to evaluate students’ comfort level while diagnosing periodontitis chairside without and with PocketPerio. Without PocketPerio, average scores were 3.86 (range 3–5), 4.2 (range 4–5), and 3.4 (range 2–5) for DS3, DS4, and ISP2, respectively (the average score for all classes was ~ 3.81). With PocketPerio, average scores were 4.29 (range 4–5), 4.5 (range 4–5), and 4.4 (range 3–5) for DS3, DS4, and ISP2, respectively (the average score for all classes was ~ 4.38).
The same students were also asked to comment on PocketPerio features (Supplementary Table 2). When asked, “What feature(s) of PocketPerio did you like the best?” fourteen students chose “The ability to accurately diagnose periodontal conditions,” nine students chose “The interface”, eleven students chose “The included proposed treatment options,” and eight students chose “The included information icons.” When asked, "What feature(s) of PocketPerio did you find not helpful?”, three students said that they found terminology and verbalization of questions and answers to be not as straightforward, one student found the interface to be not too easy to navigate, and another student felt that some features of PocketPerio were redundant (but did not provide additional detail). When asked, “If you were to make updates to PocketPerio, what would you change?”, most students asked to make a more advanced, machine-learning version of PocketPerio. Some students asked for updated terminology and verbalization of questions and answers, a simplified version of PocketPerio with fewer diagnostic choices, and an updated interface. When asked, “Would you use PocketPerio in your practice?”, fourteen students responded “Yes” and three students responded, “Maybe, if there is an updated version.” No student chose “No” as an answer. Some students also provided written comments outside the proposed answer options.
Discussion
In the present study, we reported on the accuracy of the PocketPerio application in diagnosing various periodontal conditions in both classroom and clinical settings. Mock examination results showed that PocketPerio did not decrease the duration of time required for students to arrive at the diagnosis compared to the control. The participants were given only brief instructions on using PocketPerio before the mock examination, and it is expected that users using PocketPerio regularly will find it intuitive and spend less time arriving at the diagnosis. It is important to note that the application requires a manual selection of answers, the process of arriving at the diagnosis is not automatic and requires time to read questions, answer options, and make an accurate selection. At least to some extent, this lack of user familiarity using PocketPerio could explain why test students did not accurately diagnose all cases (the accuracy was 52.73%).
It is also important to highlight differences in the prevalence of severe periodontitis in patients attending academic dental clinics reported in the present study compared to the general U.S. population. In the present study, severe periodontitis corresponding to stages III and IV (defined as CAL ≥ 5 mm and PD ≥ 6 mm on ≥ 2 non-adjacent teeth based on the 2017 periodontal classification1) was 88.67% (42.67 and 46.0% for stages III and IV, respectively). A large-scale, 2009–2014 National Health and Nutrition Examination Survey-based study that included 10,683 adult patients (aged ≥ 30 years) showed that the prevalence of severe periodontitis (defined as ≥ 2 interproximal sites with CAL ≥ 6 mm on ≥ 2 non-adjacent teeth and ≥ 1 interproximal site with PD ≥ 5 mm, based on the 2012 AAP/CDC periodontitis case definition28) was 7.8% of all participants that corresponded to ~ 18.4% of all periodontitis cases5. Using the 2012 AAP/CDC periodontitis case definition28, the retrospective analysis of 10,544 electronic health records (EHRs) at East Carolina rural practice-based clinics demonstrated that the prevalence of severe periodontitis was ~ 35.0%29. Several other studies reported on the prevalence of severe periodontitis in an academic setting. The retrospective analysis of 2,137 EHRs at Western University (Pomona, CA, USA) showed that the prevalence of severe periodontitis (defined as CAL ≥ 5 mm based on the 1999 periodontal classification30) was 24.5%31. The retrospective analysis of 1,131 EHRs at Harvard University showed that the prevalence of severe periodontitis (defined as > 30% of root length or > 5 mm of alveolar bone loss based on the 2015 Task Force Report on the Update to the 1999 Classification32) was 2.8%33. Overall, differences in the prevalence of severe periodontitis among these studies (including the present study) could be due to different definitions and cut-offs of the disease and different study populations. The geospatial distribution of severe periodontitis throughout the United States was reported previously34,35 and should be considered. Although Colorado state was not among the states with the highest prevalence of severe periodontitis, some state counties had a high prevalence of the disease. To note, our unpublished data showed that the prevalence of stages III and IV periodontitis at the UTSD ranged from 50 to 84.6%.
Although the participants in the present study were able to accurately diagnose ~ 43% of periodontitis cases, some clinical cases posed significant challenges, resulting in decreasing the accuracy of periodontal diagnosis to as low as 0%. These data demonstrate a high variability in the diagnosis accuracy and highlight the need for tools like PocketPerio to assist and complement students’ knowledge. Another important finding of the study was that an overwhelming majority of secondary periodontal diagnoses (~ 85%) remained undiagnosed. Since all patients had at least one secondary diagnosis, it is essential to emphasize the importance of these conditions, especially while developing a comprehensive treatment plan. For example, studies demonstrated the added benefit of occlusal therapy in slowing the progression of periodontitis and improving therapeutic tooth prognosis. The presence of tooth- and prostheses-related factors (such as defective restorations) can be associated with the retention of dental biofilm and negatively impact periodontal conditions and tooth prognosis36. Although it is possible that students noted these and other secondary conditions during their periodontal evaluation, it is important to educate students to document them properly to teach them to be competent independent providers.
PocketPerio also increased the students’ confidence in accurately diagnosing periodontal conditions regardless of the end-user’s level of knowledge. For example, ISP2 were much less comfortable diagnosing periodontal conditions without PocketPerio than DS3 and DS4, whereas their confidence level became comparable while using PocketPerio. Importantly, during both mock examination and chairside, the participants were able to navigate through the application and use it even without previous knowledge of its interface and features. Overall, the students provided positive and encouraging feedback on the interface and features of PocketPerio; however, some changes were also suggested (updated terminology, improved verbalization of some questions and answers, and the development of a simplified application version).
Interestingly, most suggestions for future changes to PocketPerio were related to the development of its more advanced, machine-learning version. This suggestion reflects an emerging use of machine-learning-assisted approaches in the daily teaching process. Artificial intelligence (AI) and machine-learning-assisted approaches have been continuously implicated in dentistry to detect a wide variety of radiographic findings37,38, perform and analyze immune profiling to assist with the diagnosis of peri-implantitis39, enhance the interdisciplinary interaction between medical and dental professionals40, and assist with diagnosis of periodontitis41. Nevertheless, limitations in study design and the associated high risk of bias make the use of these applications in dental practice challenging42,43. The development of an AI version of PocketPerio will be considered in the future. It is encouraging that almost all responders to the anonymous survey said they would use PocketPerio in their future clinical practice.
PocketPerio is not the first published application aimed at diagnosing periodontal conditions. A recent study reported that the Android-based PerioSmart application improved the accuracy of diagnosing periodontitis in a time-effective manner44. Although both PerioSmart and PocketPerio are aimed to improve the accuracy of periodontal diagnosis, there are a few differences between these applications. First, PocketPerio assists with the diagnosis of a wide scope of periodontal conditions and not only periodontitis. Additionally, PocketPerio provides suggested treatment options for each diagnosis. Finally, PocketPerio is a web-based application, which is available on any device connected to the Internet and is not limited to a specific operating system. The free access to PocketPerio can be requested by contacting the corresponding author.
There are several strengths of the study. First, it is the development of a novel educational application that we expect to meet several essential educational goals and has the potential to be converted into educational enduring material. This accomplishment would help maintain educational standards and patient care in both academic and private clinical settings. Second, the study was performed in two dental schools and included researchers from several other research institutions, which allows for more intense inter-institutional collaboration and, to some extent, generalization of the results. In addition, the participants of the study represent dental students of various years of training, including those trained internationally. Finally, the study provides a foundation for further updates of PocketPerio and possibly creating an AI version of this tool.
There are several limitations of the present study. PocketPerio was used only by dental students, and therefore its effectiveness among other dental providers (such as general dentists and other dental specialists) remains to be explored. The scope of periodontal conditions encountered in predoctoral clinics was quite limited (for example, there were no cases of generalized periodontitis stage II grade C, generalized periodontitis stage III grade A, and molar-incisor pattern periodontitis except stage III grade C); therefore, the effectiveness of PocketPerio to diagnose conditions rarely encountered in clinical practice remains to be explored. The participants’ feedback on PocketPerio and their perception of its interface could, at least to some extent, be influenced by their year of training (and, consequently, by the level of knowledge of the periodontal classification) and the frequency of using the application. Since the mock examination and chairside use of PocketPerio were performed in only a single school (UTSD and CUSDM, respectively) and sample sizes were modest (n = 22 and 150, respectively), our results may not allow for their generalization. Finally, sample sizes varied in different experimental approaches. For example, the number of participating DS4 was ~ 10 times lower than DS3, which could influence study outcomes and interpretation of the data.
Conclusions
PocketPerio offers a straightforward approach to improving the accuracy of diagnosing a wide spectrum of periodontal conditions, especially among users with limited exposure to periodontics.
Data availability
The raw datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request and subject to clearance by the respective IRB of the UTSD (Houston, TX, USA) and the CUSDM (Aurora, CO, USA).
References
Caton, J. G. et al. A new classification scheme for periodontal and peri-implant diseases and conditions - Introduction and key changes from the 1999 classification. J. Clin. Periodontol. 45(Suppl 20), S1–S8. https://doi.org/10.1111/jcpe.12935 (2018).
Papapanou, P. N. et al. Periodontitis: consensus report of workgroup 2 of the 2017 World Workshop on the classification of periodontal and peri-implant diseases and conditions. J. Periodontol. 89(Suppl 1), S173-s182. https://doi.org/10.1002/jper.17-0721 (2018).
Tonetti, M. S., Greenwell, H. & Kornman, K. S. Staging and grading of periodontitis: Framework and proposal of a new classification and case definition. J. Periodontol. 89(Suppl 1), S159–S172. https://doi.org/10.1002/jper.18-0006 (2018).
Graetz, C. et al. Comparison of periodontitis patients’ classification in the 2018 versus 1999 classification. J. Clin. Periodontol. 46, 908–917. https://doi.org/10.1111/jcpe.13157 (2019).
Eke, P. I. et al. Periodontitis in US adults. National Health and Nutrition Examination Survey 2009–2014. J. Am. Dent. Assoc. 149, 576–588 (2018).
Botelho, J., Machado, V., Proença, L. & Mendes, J. J. The 2018 periodontitis case definition improves accuracy performance of full-mouth partial diagnostic protocols. Sci. Rep. 10, 7093. https://doi.org/10.1038/s41598-020-63700-6 (2020).
Ortigara, G. B. et al. EFP/AAP periodontitis case classification demonstrates high agreement with the 2012 CDC/AAP criteria. J. Clin. Periodontol. 48(886–895), 2021. https://doi.org/10.1111/jcpe.13462 (2018).
Brito, L. F., Taboza, Z. A., Silveira, V. R., Teixeira, A. K. & Rego, R. O. Diagnostic accuracy of severe periodontitis case definitions: Comparison of the CDC/AAP, EFP/AAP, and CPI criteria. J. Periodontol. 93, 867–876. https://doi.org/10.1002/jper.21-0365 (2022).
Morales, A. et al. Performance of the 2017 AAP/EFP case definition compared with the CDC/AAP definition in population-based studies. J. Periodontol. 93, 1003–1013. https://doi.org/10.1002/jper.21-0276 (2022).
Kornman, K. S. & Papapanou, P. N. Clinical application of the new classification of periodontal diseases: Ground rules, clarifications and “gray zones”. J. Periodontol. 91, 352–360. https://doi.org/10.1002/jper.19-0557 (2020).
Sirinirund, B., Di Gianfilippo, R., Yu, S. H., Wang, H. L. & Kornman, K. S. Diagnosis of stage III periodontitis and ambiguities of the “gray zones" in between stage III and stage IV. Clin. Adv. Periodont. 11, 111–115. https://doi.org/10.1002/cap.10153 (2021).
Steigmann, L., Sommer, C., Kornman, K. S. & Wang, H. L. Staging and grading discussion of borderline cases in gray zones. Clin. Adv. Periodont. 11, 98–102. https://doi.org/10.1002/cap.10129 (2021).
Jayawardena, D. S., Yates, R., West, N. X. & Pollard, A. J. Implementing the 2017 classification of periodontal and peri-implant diseases - how are we doing in the South West region of the UK?. Br. Dent. J. https://doi.org/10.1038/s41415-021-3716-2 (2021).
Ravidà, A. et al. Agreement among international periodontal experts using the 2017 World Workshop classification of periodontitis. J. Periodontol. 92, 1675–1686. https://doi.org/10.1002/jper.20-0825 (2021).
Abrahamian, L. et al. Intra- and inter-examiner reliability in classifying periodontitis according to the 2018 classification of periodontal diseases. J. Clin. Periodontol. 49, 732–739. https://doi.org/10.1111/jcpe.13618 (2022).
Marini, L. et al. The staging and grading system in defining periodontitis cases: consistency and accuracy amongst periodontal experts, general dentists and undergraduate students. J. Clin. Periodontol. 48, 205–215. https://doi.org/10.1111/jcpe.13406 (2021).
Oh, S. L., Yang, J. S. & Kim, Y. J. Discrepancies in periodontitis classification among dental practitioners with different educational backgrounds. BMC Oral Health 21, 39. https://doi.org/10.1186/s12903-020-01371-5 (2021).
Abou-Arraj, R. V. et al. The new periodontal disease classification: Level of agreement on diagnoses and treatment planning at various dental education levels. J. Dent. Educ. 85, 1627–1639. https://doi.org/10.1002/jdd.12636 (2021).
Tonetti, M. S. & Sanz, M. Implementation of the new classification of periodontal diseases: decision-making algorithms for clinical practice and education. J. Clin. Periodontol. 46, 398–405. https://doi.org/10.1111/jcpe.13104 (2019).
Sutthiboonyapan, P., Wang, H. L. & Charatkulangkun, O. Flowcharts for easy periodontal diagnosis based on the 2018 new periodontal classification. Clin. Adv. Periodont. 10, 155–160. https://doi.org/10.1002/cap.10095 (2020).
Parsegian, K., Ayilavarapu, S., Patel, T., Henson, H. A. & Angelov, N. Flowcharts improve periodontal diagnosis by dental and dental hygiene students. Can. J. Dent. Hyg. 55, 137–147 (2021).
World Medical Association Declaration of Helsinki. ethical principles for medical research involving human subjects. JAMA 310, 2191–2194. https://doi.org/10.1001/jama.2013.281053 (2013).
Cohen, J. F. et al. STARD 2015 guidelines for reporting diagnostic accuracy studies: explanation and elaboration. BMJ Open 6, e012799. https://doi.org/10.1136/bmjopen-2016-012799 (2016).
American Academy of Periodontology. 2017 classification of periodontal and peri-implant diseases and conditions. https://www.perio.org/research-science/2017-classification-of-periodontal-and-peri-implant-diseases-and-conditions/.
Jepsen, S. et al. Periodontal manifestations of systemic diseases and developmental and acquired conditions: consensus report of workgroup 3 of the 2017 World Workshop on the classification of periodontal and peri-implant diseases and conditions. J. Periodontol. 89(Suppl 1), S237–S248. https://doi.org/10.1002/jper.17-0733 (2018).
Fan, J. & Caton, J. G. Occlusal trauma and excessive occlusal forces: Narrative review, case definitions, and diagnostic considerations. J. Periodontol. 89(Suppl 1), S214–S222. https://doi.org/10.1002/jper.16-0581 (2018).
Herrera, D., Retamal-Valdes, B., Alonso, B. & Feres, M. Acute periodontal lesions (periodontal abscesses and necrotizing periodontal diseases) and endo-periodontal lesions. J. Periodontol. 89(Suppl 1), S85–S102. https://doi.org/10.1002/jper.16-0642 (2018).
Eke, P. I., Page, R. C., Wei, L., Thornton-Evans, G. & Genco, R. J. Update of the case definitions for population-based surveillance of periodontitis. J. Periodontol. 83, 1449–1454. https://doi.org/10.1902/jop.2012.110664 (2012).
Gillone, A. et al. Racial and ethnic disparities in periodontal health among adults seeking dental care in rural North Carolina communities: A retrospective study. J. Periodontol. 94, 364–375. https://doi.org/10.1002/jper.22-0137 (2023).
Armitage, G. C. Development of a classification system for periodontal diseases and conditions. Ann. Periodontol. 4, 1–6. https://doi.org/10.1902/annals.1999.4.1.1 (1999).
Rhee, E. S., Sekhon, P. K. & Boehm, T. K. Prevalence of periodontal disease among dental school patients. J. Taibah. Univ. Med. Sci 9, 126–131 (2014).
American Academy of Periodontology Task Force report on the Update to the 1999 classification of periodontal diseases and conditions. J. Periodontol. 86(7), 835–838 (2015).
Helmi, M. F. et al. Prevalence of periodontitis and alveolar bone loss in a patient population at Harvard School of Dental Medicine. BMC Oral Health 19, 254. https://doi.org/10.1186/s12903-019-0925-z (2019).
Eke, P. I., Borgnakke, W. S. & Genco, R. J. Recent epidemiologic trends in periodontitis in the USA. Periodontol 2000(82), 257–267. https://doi.org/10.1111/prd.12323 (2020).
Eke, P. I. et al. Periodontitis prevalence in adults ≥65 years of age, in the USA. Periodontol 2000(72), 76–95. https://doi.org/10.1111/prd.12145 (2016).
Ercoli, C. & Caton, J. G. Dental prostheses and tooth-related factors. J Clin. Periodontol 45(Suppl 20), S207–S218. https://doi.org/10.1111/jcpe.12950 (2018).
Ekert, T. et al. Deep learning for the radiographic detection of apical lesions. J. Endod. 45, 917-922.e915. https://doi.org/10.1016/j.joen.2019.03.016 (2019).
Putra, R. H., Doi, C., Yoda, N., Astuti, E. R. & Sasaki, K. Current applications and development of artificial intelligence for digital dental radiography. Dentomaxillofac. Radiol. 51, 20210197. https://doi.org/10.1259/dmfr.20210197 (2022).
Wang, C. W. et al. Machine learning-assisted immune profiling stratifies peri-implantitis patients with unique microbial colonization and clinical outcomes. Theranostics 11, 6703–6716. https://doi.org/10.7150/thno.57775 (2021).
Seitz, M. W. et al. Development and evaluation of a mobile patient application to enhance medical-dental integration for the treatment of periodontitis and diabetes. Int. J. Med. Inform. 152, 104495. https://doi.org/10.1016/j.ijmedinf.2021.104495 (2021).
Ossowska, A., Kusiak, A. & Świetlik, D. Evaluation of the progression of periodontitis with the use of neural networks. J. Clin. Med. 11, 4667. https://doi.org/10.3390/jcm11164667 (2022).
Mohammad-Rahimi, H. et al. Deep learning in periodontology and oral implantology: A scoping review. J. Periodontal. Res. 57, 942–951. https://doi.org/10.1111/jre.13037 (2022).
Schwendicke, F., Samek, W. & Krois, J. Artificial intelligence in dentistry: chances and challenges. J. Dent. Res. 99, 769–774. https://doi.org/10.1177/0022034520915714 (2020).
Sánchez-Otálvaro, L. M., Jiménez-Rivero, Y., Velasquez, R. A. & Botero, J. E. Development and testing of a mobile application for periodontal diagnosis. J. Clin. Exp. Dent. 14, e269–e273. https://doi.org/10.4317/jced.59338 (2022).
Acknowledgements
The authors would like to thank Mr. Gordon Finnerty Jr. (Technology Services and Informatics, UTSD, Houston, TX, USA) and Michael Lampe (Office of Academic Affairs and Innovation, CUSDM, Aurora, CO, USA) for their technical support with the Qualtrics platform. The authors would also like to thank all predoctoral dental students who participated in the study.
Author information
Authors and Affiliations
Contributions
K. P. and N. A. contributed to the conception, design, data acquisition, and interpretation. T. C. and N. S. contributed to the biostatistical analysis and data interpretation. S. C. and Y. K. contributed to data acquisition. D. O. and S. F. contributed to the data interpretation. All authors contributed to the manuscript preparation, critically revised it for important intellectual content, approved the final version, and agreed to be accountable for all aspects of the study including questions related to the accuracy or integrity of any part of the work. No part of this manuscript was generated using AI or AI-assisted technology.
Corresponding author
Ethics declarations
Competing interests
The study was funded by the UTSD Dean's Academy Small Grants Program (no grant number was provided to the grantee). The funders of the study had no role in the study design, data collection, data analysis, data interpretation, or writing of the manuscript. The authors and PocketPerio developers declare no commercial relationships that may pose a potential conflict of interest with respect to this article's authorship and/or publication. The views expressed in this manuscript are those of the authors and do not necessarily reflect the official policy of the UTSD (Houston, TX, USA) and the CUSDM (Aurora, CO, USA).
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Supplementary Video 1.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Parsegian, K., Okano, D.K., Chandrasekaran, S. et al. The PocketPerio application significantly increases the accuracy of diagnosing periodontal conditions in didactic and chairside settings. Sci Rep 14, 10189 (2024). https://doi.org/10.1038/s41598-024-59394-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-59394-9
Keywords
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
