
Abstract
Morbidity and mortality in hospitalized patients can be increased due to errors that are caused by inadequate knowledge and unsatisfactory practice of intravenous (IV) fluid therapy among healthcare workers. The knowledge and practice of nurses are very critical to IV fluid therapy because they are the cornerstone of a subject. This study assessed nurse's knowledge and practice of IV fluid therapy. A cross-sectional study design was employed at four selected public hospitals in Addis Ababa, Ethiopia. Data were collected from 112 nurses using a structured questionnaire for knowledge and using an observational checklist for practice. Data were analyzed using SPSS version 26 computer programs. Most respondents (67%) were males; the mean age of respondents was 31.2 ± 4.3. Among participated nurses, 42% (95% CI 32.8, 51.2) and 56.3% (95% CI 47.1, 65.6) had inadequate knowledge and satisfactory practice regarding IV fluid therapy in children, respectively. A significant association was observed between nurses' intravenous fluid therapy knowledge and in-service training that nurses who had training on fluid therapy in children had 4 times adequate knowledge than those who had no training (P = 0.01), an educational qualification that master degree holders had 4.8 times adequate knowledge than first-degree holders (P = 0.04) and training institution that nurse who had taken training in governmental teaching institution had 4 times adequate knowledge than who had taken training in private teaching institution (P = 0.011). No statistically significant association was found between practice level and independent variables regarding IV fluid therapy. Nurses’ knowledge of IV fluid therapy was inadequate and practice was relatively satisfactory. Continuous education and training of nurses on IV fluid therapy should be conducted regularly to improve their knowledge and practice. Further research should be employed involving other hospitals and focusing on risk factors for knowledge and practice inadequacy that are not discussed in this study.
Similar content being viewed by others

Introduction
Intravenous fluid therapy is among the most common routine nursing care procedures and has been practiced for more than 180 years globally1. It involves the administration of intravenous (IV) fluids, to nearly all hospitalized patients, for body fluid and electrolyte maintenance and as diluents for medications2. Relative benefits of crystalloids and colloid fluid resuscitation were controversial more than in the treatment of patients with hypovolemic shock3. Rapid intravenous fluid administration guidelines implementation contributed to the reduction of mortality due to hypovolemic shock over the years4.
Rapid and appropriate fluid resuscitation with crystalloids is very important to improve outcomes and to reduce the death of children in emergency departments as well as wards for admitted children. Different guidelines and management protocols recommend initial fluid bolus at a rate of 20 ml/kg of normal saline over 20 min5,6. Intravenous fluid therapy is a collaboration activity of health professionals, especially nurses and physicians. Nurses’ knowledge of age-specific considerations during the administration of IV fluids is critical in promoting patient safety and preventing complications for positive patient outcomes7.
About 70% of all intravenous administrations including fluid and medication had at least one clinical error that could be minimized by nurses' correct procedures and enough nurses. These errors have been associated with inadequate knowledge of nurses and other healthcare workers about IV fluid therapy8. According to a report by the National Institute of Health Care, Excellence guidance, 39% of intravenous fluid therapy errors were made by nurses only and 36% jointly by nurses and emergency physicians9.
According to empirical evidence globally, about 20% of the patients had errors in IV fluid therapy that are attributable to inadequate knowledge among healthcare workers including nurses (Enquiry, 201110). Studies to assess the knowledge of nurses regarding intravenous therapy predominantly recorded that the majority of nurses had adequate knowledge of intravenous fluid therapy11. Poor knowledge of IV infusion decreases the quality for patients which can cause a poor outcome. According to one study conducted in Kenya, 17% of deaths among hospitalized patients were caused by inappropriate IV fluid therapy12.
The Royal College of Nursing (2016) standards of practice direct that the nurses involved in the administration of IV infusions should be trained in infusion therapy, including IV fluid types, clinical judgment assessment, administration, monitoring, and complications13. One descriptive study showed that there was no consensus regarding best practices to achieve pediatric fluid resuscitation goals among nurses, and other specialty and sub-specialty groups, and the study recommended further investigation of this problem14. The majority of the studies conducted globally, in Africa and Ethiopia did not address the title of this study rather they studied health professionals' knowledge and practice of fluid therapy in adults.
In Ethiopia, elsewhere, there is no study conducted on the assessment of nurses' knowledge and practice of intravenous fluid therapy in children. The purpose of this study was to describe nurses' knowledge and practice working in the pediatric emergency department regarding intravenous fluid therapy in children and to correlate between knowledge and practice level of nurses with selected independent variables. The study further aimed to establish the relationship between nurses' knowledge, practice, and sociodemographic characteristics. The study will provide important information for other researchers to conduct further studies focusing on risk factors for inadequacy of knowledge and unsatisfactory practice such as work overload, job satisfaction and promotion. Furthermore, based on the findings of the study the health facilities will take gap-filling actions.
Materials and methods
Study area
The study was conducted in selected public hospitals in Addis Ababa, capital city of Ethiopia. In Addis Ababa, there are 43 hospitals (11 public hospitals and 32 private hospitals) out of which selected for this study.
Study design and study period
An institutional based cross-sectional study was conducted from March, 2022 to April, 2022.
Population and eligibility criteria
The source population was all nurses working in the pediatric emergency department of public hospitals in Addis Ababa, Ethiopia, with a study population of all nurses working in the pediatric emergency department of selected hospitals. All nurses who had 6 months and more work experience, who were available during data collection, and who had the interest to participate were included in the study. However, nurses on annual and sick leave during the study period were excluded.
Sampling procedure
There are 11 public hospital out of which four hospitals were selected purposively for this study by considering the pediatric emergency department they have and several nurses working in the department to get an adequate sample size. The consecutive sampling was used to collect data from all the nurses. Because of the small number of nurses working in the pediatric emergency department of selected hospitals, consecutive sampling is used to include all nurses and to get a relatively adequate sample size. The total number of nurses working in a pediatric emergency at selected hospitals was 126, 117 nurses participated in the study and 112 nurses responded to all questionnaires with a response rate of 95.7%.
Tikur-Anbessa Specialized Hospital = 42
St. Peters Hospital = 21
Zewuditu Memorial Hospital = 24
Yekatit 12 Hospital = 25
Data collection procedure
The study tools were adopted from other literature13,15 with some modifications according to the objectives of the study to assess the knowledge and practice of nurses towards intravenous fluid therapy in children. The tools for data collection have three parts which were socio-demographic characteristics of study participants (9 items), knowledge (11 items), and practice (10 items observational checklists) of nurses regarding intravenous fluid therapy in children. There were 11 knowledge question items and the level of knowledge of nurses was calculated out of 29 because five questions had multiple responses. Tools were applied by using well-structured questionnaires through a self-administered response method for the knowledge test and by observation of nurses using observational checklists to assess practice. To assess the practice the nurses gave their consent but they were not allowed to know the contents of the observational checklist before being observed to minimize bias.
Data quality control
The questionnaire was pre-tested by the principal investigator on 10% (n = 11) of the study population 2 weeks before actual data collection at St. Paulos Millennium Medical College Hospital to check its clarity, understandability, and reliability. Accordingly, the Cronbach's Alpha result of the pre-test was 0.710. Two days of short training were given for the data collectors and supervisors to enhance the quality of data and to ensure that all the data collectors have the same information about the study tools, and follow the same survey procedures. In addition, during the actual data collection process, supervisors were cross-checking consistency, completeness, and any missing data. Data cleaning for inconsistencies, missing values, and amendments were considered as needed before data analysis.
Data management and analysis
Data were collected and checked for completeness and accuracy, then coded and entered by the investigator into the Epi data version 4.6 computer program. Subsequently, the data was transmitted to SPSS version 26 computer programs for analysis. Data analysis was performed using descriptive and inferential statistics. Univariate statistics were calculated to summarize respondents' socio-demographic characteristics knowledge and practice scores. Bivariate analysis was used to assess for statistically significant associate factors for knowledge and practice. Multivariate analysis was conducted for those variables that had a P value < 0.25 in binary logistic regression. A P value less than 0.05 was considered significant. The analyzed data were presented on charts, tables, and narrative text.
Ethical approval
Ethical clearance was obtained from the Departmental of Emergency Medicine Research Ethics Committee of Addis Ababa University, College of Health Science, and submitted to hospitals. All methods were performed in accordance with the relevant guidelines and regulations of ethical procedures according to the Declaration of Helsinki with confidentiality and data privacy maintained to the maximum. After getting permission from these hospitals, informed consent was obtained after an information sheet on the objective of the study, the voluntariness of the participant, benefits, and risks of the study, and confidentiality of the study participant's information was provided to the participant nurses, and the collection of data was started.
Operational definitions
Knowledge
Intravenous fluid therapy knowledge was measured as a two-score in the validated test for knowledge16.
Adequate knowledge: Nurses who score more than the mean knowledge score.
Inadequate knowledge: Nurses who score less than the mean knowledge score.
Practice
Intravenous fluid therapy practice was measured as a two-score in the validated test for practice16.
Satisfactory practice: Nurses who score more than the mean of practice score.
Unsatisfactory practice: Nurses who score less than the mean of practice score.
Result
Sample characteristics of the respondents
Of the total 117 study participants, 112 were involved in this study with a response rate of 95.7%. Most respondents (67%) were males; the mean age of respondents was 31.2 with an SD of 4.3. About half (51.8%) had 6 months to 5 years of experience. The majority of them (72.3%) were first-degree holders, and only 32.1% of nurses had taken training regarding intravenous fluid therapy in children (Table 1).
Knowledge level of nurses
Of all respondents 42% (95% CI 32.8%, 51.2%) of them had adequate knowledge whereas more than half (58%) of them had inadequate knowledge about intravenous fluid therapy in children by scoring more than and less than the mean score of knowledge, respectively (Fig. 1).

Distribution of samples according to the knowledge level regarding IV fluid therapy in children among nurses working in the emergency department, Addis Ababa, 2022.
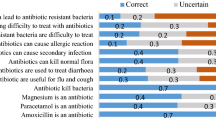
The minimum score for knowledge assessment was 8 (27.6%) and the maximum score was 24 (82.8%) out of 29 questions and by 100%, respectively. Over half of the nurses (58.9%, n = 66) correctly identified crystalloids as initial fluid therapy compared to colloids. Only 23.3 (n = 26) of them correctly selected Lactated Ringer's as the most physiological IV fluid than other types of IV fluid. Among all participants, only 21.4% (n = 24) were able to correctly identify at least three ions contained in Lactated Ringer's Solution. Only 15.2% (n = 17) of participants correctly identified the composition of maintenance fluid in IV fluid therapy. Regarding parameters to be monitored during IV fluid therapy, 22.3% (n = 25) of nurses correctly identified all listed options. Concerning the two body systems mainly monitored during IV fluid therapy 33.9% (n = 38) of them correctly selected circulatory and renal systems. The least correctly answered knowledge question was a complication of IV fluid therapy which was 9.8% (n = 11) (Table 2).
Practice level of nurses
The practice level of nurses on IV fluid therapy in children was classified based on the mean score of practice as satisfactory (more than the mean) and unsatisfactory (less than the mean). Accordingly, more than half of the study respondents 56.3% (95% CI 47.1%, 65.6%) had satisfactory practice and the remaining 43.8% (n = 49) of them had an unsatisfactory practice of IV fluid therapy in children with 3 and 10 minimum and maximum scores, respectively (Fig. 2).

Distribution of samples according to the practice level regarding IV fluid therapy in children among nurses working in the emergency department, Addis Ababa, Ethiopia, 2022.
Nurses' practice of IV fluid therapy in children
There were 10 observational checklists prepared to assess the level of nurses’ practice on intravenous fluid therapy in children. According to the result of practice observation, more than 85% of nurses checked the type and amount of IV fluid against the physician's order (89.3%) and accurately adjusted the flow rate (86.6%). Of all observed nurses, 69.6% and 63.4% checked for signs of infiltration and site for signs of phlebitis, respectively. Only 33.9% of observed nurses were inspecting the rate of flow and function of the IV line at least every hour. The least frequently practiced observation was checking respiration and auscultates lung sounds periodically which was seen in 25.9% of nurses (Table 3).
Factors associated with knowledge
Multivariate logistic regression analysis showed that nurses who had training on fluid therapy were 4.1 times more likely to belong to the adequate knowledge group than the inadequate knowledge group compared to those who had not taken training [AOR = 4.137; 95% CI (3993–0.241); P = 0.01]. Female respondents had 2.5 times more adequate knowledge than male respondents but the difference was not statistically significant at a P value < 0.05 [AOR = 2.092; 95% CI (0.940–4.656); P = 0.058]. The result further showed masters master-holder respondents had 4.8 times more adequate knowledge of IV fluid therapy in children compared with those who were first-degree owners which was statistically significant at P value < 0.05 [AOR = 4.838; 95 CI (1.654–14.153); P = 0.04]. Nurses who had graduated from the governmental institute had 4 times more adequate knowledge group than the inadequate knowledge group compared to those who had graduated from private institute [AOR = 4.042; 95% CI (1.382–11.822); P = 0.011] (Table 4).
Factors associated with practice
The Association of practice level and independent variables was not statically significant at a P value < 0.05. However, some variables were more predictors than the other variables within the same group. Respondents who had work experience of ≤ 5 years had 1.2 times more satisfactory practice than those who had greater than 5 years of work experience [AOR = 1.189; 95% CI (0.239–1.594); P = 0.319], nurses who had taken training had 2 times more satisfactory skill of IV fluid therapy than those who had not taken training [AOR = 1.968; 95% CI (0.757–5.113); P = 0.165] and nurses who had been trained in the governmental teaching institute had about 2 times more satisfactory practice than those trained in private teaching facility [AOR = 1.902; 95% CI (0.782–4.622); P = 0.156] (Table 5).
Discussion
The current study showed that only 41.96% of respondents had adequate knowledge of IV fluid therapy. In line with this, the study done in Nepal to assess nurses’ knowledge and practice regarding intravenous fluid therapy in children showed that only 49.1% of respondents had adequate knowledge of IV fluid therapy16. Contrary to this one study conducted in Dhaka city to assess the level of knowledge and practice on intravenous fluid therapy among staff nurses found that 54.7% had good knowledge of IV fluid therapy17. This difference could be attributed to that the researcher included only nurses having more than 2 years of work experience.
The finding of our study showed that the majority of nurses (58.04%) had inadequate knowledge of intravenous fluid therapy in children. This study result agrees with a study conducted in Iraq in which 63.3% of nurses had inadequate knowledge of intravenous fluid therapy18.
The current study showed that only 58.9% of respondents correctly selected crystalloid fluid for initial fluid therapy in children compared to colloids. Contrary to this, a study conducted in the Australia and Netherlands to assess fluid resuscitation in pediatrics showed that 98% of health professional respondents' first choice of fluid for pediatric resuscitation was crystalloid specifically normal saline19. The present study showed that only 21.4% of nurses correctly identified the ions composition of Lactated Ringer's solution. In line with this, a study performed in Kenya showed that very few (15.4%) of the participants were able to correctly identify a minimum of three ions13.
In the current study, there was no statistically significant association between years of experience and knowledge scores. Contrary to our finding one study conducted in Denmark to assess the knowledge of nurses about IV fluid therapy found that there was a significant association between years of experience of nurses and knowledge score20. This difference may have been due to more number of nurses specializing in emergency nursing after becoming registered nurses in the later study area.
In the present study, there was no statistically significant association between age group, sex, and knowledge scores. This result was supported by the study conducted in Kenya to assess nurses’ knowledge of IV therapy in which there was a negative correlation between respondents’ gender, age group, and IV fluid therapy knowledge at P < 0.0513.
The current study showed that educational qualification was a statistically significant predictor of the knowledge level of respondents at a P value < 0.05. The result of our finding contradicts the study conducted in Iraq to compare nurses’ knowledge and practice in which there was no significant association between educational qualification and the knowledge level of participants with a P < 0.0521. This disagreement may have been due to the presence of respondents holding master's levels in our study. Our study found that the knowledge score of nurses was significantly associated with in-service training on IV fluid therapy at a P value < 0.05. Likewise, a study conducted in Nepal to assess nurses' knowledge and practice regarding intravenous therapy found that training on IV fluid therapy was a major predictor factor knowledge of nurses16.
Our study identified that only 25.9% of nurses correctly checked respiration, and auscultated lung sounds periodically. Similarly, a study conducted in Egypt to assess the nursing efficiency of IV fluid therapy in pediatrics revealed that few nurses (18%) correctly checked respiration, and auscultated lungs periodically22.
The current study showed that training, level of education of nurses, and work experience had no significant association with the practice level of nurses regarding IV fluid therapy. Opposite to this result study conducted in Kenya to assess nurses' Competence in intravenous fluid therapy in under-fives with dehydration reported that training affected their competence in IV fluid therapy in 75%, and work experience in 56.5%12.
The current study showed that 56.3% of respondents had a satisfactory practice of IV fluid therapy in children. This result was consistent with one study on nurses' KAP concerning intravenous fluid therapy in children in which 60.4% of nurses had a satisfactory practice. Contrary to our report one study showed that only 7% of nurses had good practice in IV fluid therapy in children. This difference could be attributed to the researcher's inclusion of nurses working in a private hospital in the study23.
The present study also showed that the majority (89.3%) of studied nurses correctly checked physician orders, and 84.8% of them documented any additives to IV fluid. This result was aligned with the study employed in Trivandrum to assess the knowledge and practices of staff nurses regarding fluid in cardiac ICU and surgical wards in which about 91.8% of nurses checked physician orders, and 76.7% documented any additives added to IV fluid24.
In the present study, there was no statistically significant association between gender and the practice level of a nurse with P < 0.05. Consistently studies conducted in Iraq showed that there was no association between the practices of nurses and their gender concerning fluid therapy in children. This study also reported that there was a significant association between nurses' age, years of experience, and level of education at a P value of < 0.05. However, our study found that there was no significant relationship between age, years of experience, and practice level of respondents regarding IV fluid therapy in children23. The difference may have been due to lower in-service training in our study setup.
The present study revealed that there was no statistically significant association found between nurses' knowledge scores and practice scores. The result contradicts the study employed in Kenya on the assessment of nurses’ competence on intravenous fluid therapy in under-fives with dehydration that showed a significant association between knowledge and practice of IV fluid therapy with a P < 0.0512. This could be attributed to educational and/or training strength in the coordination of practice and knowledge in the latter study.
Limitations of the study
The study has small sample size for further generalization. The study did not include private hospitals. It was limited to only nurses working in the pediatric emergency department.
Conclusion and recommendations
More than half of nurses had inadequate knowledge regarding intravenous fluid therapy in children. Nurses' practice was relatively satisfactory concerning fluid therapy in children. A significant association was observed between nurses' intravenous fluid therapy knowledge and in-service training on intravenous fluids, educational qualification, and training institute. There should be targeted educational intervention strategies on IV fluid therapy through continuing education sessions, and on-site and off-site training with a specific focus on IV fluid therapy in children, their indications, and monitoring for associated complications. There is a need for further studies incorporating nurses working in private hospitals and other wards of the hospitals. Other study should also be performed to investigate other associated factors that cause nurses’ inadequacy of knowledge and unsatisfactory practice such as work overload, job satisfaction and promotion.
Clinical significance and relevance
Adequate knowledge and satisfactory practice regarding intravenous fluid therapy among nurses are crucial in ensuring quality healthcare, reducing intravenous-related morbidity and mortality, and improving patient outcomes.
Data availability
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Abbreviations
- AOR:
-
Adjusted odd ratio
- CI:
-
Confidence interval
- COR:
-
Crude odd ratio
- ED:
-
Emergency Department
References
Finfer, S., Myburgh, J. & Bellomo, R. Intravenous fluid therapy in critically ill adults. Nat. Rev. Nephrol. 14(9), 541–557 (2018).
Severs, D., Hoorn, E. J. & Rookmaaker, M. B. A critical appraisal of intravenous fluids: From the physiological basis to clinical evidence. Nephrol. Dial. Transplant. 30(2), 178–187 (2015).
Garnacho-Montero, J. et al. Crystalloids and colloids in critical patient resuscitation. Med. Intensiva (Engl. Ed.) 39(5), 303–315 (2015).
De Caen, A. R. et al. Part 12: Pediatric advanced life support: 2015 American Heart Association guidelines update for cardiopulmonary resuscitation and emergency cardiovascular care (reprint). Pediatrics 136(2), S176–S195 (2015).
Kight BP, Waseem M. Pediatric fluid management; 2020.
Santillanes, G. & Rose, E. Evaluation and management of dehydration in children. Emerg. Med. Clin. 36(2), 259–273 (2018).
Gorski, L. The 2016 infusion therapy standards of practice. Home Healthc. Now 35, 10–18 (2017).
Westbrook, J. I., Rob, M. I., Woods, A. & Parry, D. Errors in the administration of intravenous medications in hospital and the role of correct procedures and nurse experience. BMJ Qual. Saf. 20(12), 1027–1034 (2011).
Sherratt, R. NICE guidance on giving intravenous fluids. Nurs. Times 110(6), 12–13 (2014).
Hoste, E. A. et al. Four phases of intravenous fluid therapy: A conceptual model. Brit. J. Anesth. 113(5), 740–747 (2014).
Anjani Devi, N. et al. A study to assess the knowledge regarding intravenous fluids and drug administration among staff nurses working in Narayana General Hospitals at Nellore. Indian J. Public Health Res. Dev. 7, 4 (2016).
Abwalaba, R. A. Nurses’ Competence on Intravenous Fluid Therapy in Under-Fives with Dehydration in Kakamega County HospitalsKenya; 2018.
Njung’e, W. W. & Kamolo, E. K. Nurses’ knowledge regarding intravenous fluid therapy at a County hospital in Kenya. Int. J. Afr. Nurs. Sci. 14, 100305 (2021).
Parker, M. J. & Manan, A. Translating resuscitation guidelines into practice: Health care provider attitudes, preferences and beliefs regarding pediatric fluid resuscitation performance. PLoS One 8(3), e58282 (2013).
O'Brien, T.K., et al. Pediatric Emergency Department Nurse’s Knowledge and Attitudes of Pediatric Fluid Resuscitation; 2021.
Lamsal, S. & Shrestha, R. Nurses’ knowledge and practice regarding intravenous therapy in a teaching hospital, Bharatpur. J. Chitwan Med. Coll. 9(1), 13–19 (2019).
Hossain, A., Hasan, M. & Haque, M. Assessment of the level of knowledge and practice on intravenous cannulization among staff nurses of selected tertiary care hospital in Dhaka city. MOJ Public Health 4(5), 00095 (2016).
Musa, M. H. & Mahmood, M. H. Assessment, of nurse’s knowledge and skill about intravenous fluid administration. J. Duhok Univ. 25(2), 531–536 (2022).
Long, E. et al. Fluid resuscitation for pediatric sepsis: A survey of senior emergency physicians in Australia and New Zealand. Emerg. Med. Australas. 27(3), 245–250 (2015).
Sindahl, P. et al. A cross-sectional survey of knowledge about IV fluid therapy and hyponatremia among nurses working at emergency departments in Denmark. Int. Emerg. Nurs. 57, 101010 (2021).
Othman, N. R. & Ahmed, A. A. Nurses knowledge, attitude, and practice concerning fluid therapy in Children Hospital in Erbil City, Kurdistan Region Iraq. Indian J. Forensic Med. Toxicol. 13, 4 (2019).
El Sayed, H. I. & El Sayed, A. I. Nursing efficiency in maintaining fluid and electrolyte balance at pediatric intensive care units. Am. J. Nurs. Sci. 10(6), 254–263 (2021).
Othman, N. R. & Ahmed, A. A. A comparative study of nurses’ knowledge, attitudes, and practices concerning fluid therapy in children in public versus private hospitals in Erbil city. Erbil J. Nurs. Midwifery 3(1), 22–30 (2020).
Vijayan, A. A study to assess the knowledge and practices of staff nurses regarding fluid and electrolyte administration in post-operative cardiac surgical patients admitted in cardiac surgical ICU and cardiac surgical ward, SCTIMST, Trivandrum. 2011.
Acknowledgements
We would like to express our deepest thanks to Addis Ababa University, the College of Health Science, and the Department of Emergency Medicine for allowing us to conduct this study. We have grateful gratitude to the Addis Ababa Health Bureau and Public Hospitals in which the study was employed for their continuous support. Finally, we would like to appreciate data collectors, supervisors, and study participants.
Funding
Addis Ababa University College of Health Sciences covered the funding.
Author information
Authors and Affiliations
Contributions
All authors contributed to data analysis, drafting, or revising the manuscript. All authors read and approved the final version of the manuscript, and they agree to be accountable for all of the work.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Tolera, G.G., Kasaye, B.M. & Abicho, T.B. Knowledge and practice towards intravenous fluid therapy in children among nurses in the pediatrics emergency department of selected public hospitals. Sci Rep 14, 2503 (2024). https://doi.org/10.1038/s41598-024-52921-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-52921-8
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
