
Abstract
This study aimed to compare the effects of knee strengthening exercises to those of polyvagal theory–based exercises combined with knee strengthening exercises on selected outcomes in women with grade II knee osteoarthritis (OA). A randomized controlled trial was conducted, in which 60 female participants diagnosed with grade II knee OA, with a mean age of 57.27 ± 7.81 years and knee pain rated between 4 and 7 on the visual analog scale (VAS), were assigned to either the knee strengthening exercise group (Group 1, n = 30) or the polyvagal theory–based exercise plus knee strengthening exercise group (Group 2, n = 30). Pre- and posttreatment assessment of outcome variables, including WOMAC scores (joint pain, joint stiffness, functional limitations, and the overall index), WHOQOL scores (overall quality of life, general health, physical, psychological, social, and environmental domains), and heart rate variability (HRV, time and frequency domains), were analyzed. Group 2 demonstrated significantly greater reductions in joint pain, stiffness, and functional limitations than Group 1 after the intervention. Group 2 presented with significantly improved WOMAC scores, indicating better overall outcomes. Group 2 showed significant improvements in the psychological and social domains regarding quality of life. There were no significant differences in the physical domain or the environmental domain. Group 2 showed a significant increase in high-frequency power (HF) and a significant decrease in the LF/HF ratio, suggesting improved autonomic regulation. A combination of polyvagal exercise and knee strengthening training resulted in superior outcomes compared to knee strengthening exercises alone in women with grade II knee OA. These findings support the potential effectiveness of incorporating polyvagal exercises as an adjunctive intervention for osteoarthritis management.
Similar content being viewed by others

Introduction
Osteoarthritis (OA) is one of the most prevalent degenerative conditions resulting in disability, particularly among the elderly population. OA is the most common articular disease in the developed world and a leading cause of chronic disability, primarily due to knee OA and hip OA1. The prevalence of osteoarthritis (OA) is significantly higher in women than in men, and the disease significantly affects both physical and autonomic functions2.
Women are particularly susceptible to OA, accounting for approximately 60% of all OA patients3. Age is a major risk factor, with the prevalence in women escalating from approximately 10% at ages 25–34 to over 50% at ages 75 and older2. Exercise plays a pivotal role in sustaining overall well-being and enhancing quality of life, particularly among older women4. The physical implications of OA in women include pain, stiffness, limited mobility, and a reduced capacity to perform daily activities, leading to compromised quality of life5. Autonomic dysfunction, characterized by irregularities in heart rate variability and blood pressure, has been reported in patients with OA, suggesting a link between chronic pain and cardiovascular risk 6.
The pathogenesis of knee OA involves a complex interplay of mechanical, genetic, and biochemical factors. It typically begins with cartilage degradation, leading to changes in the subchondral bone, inflammation, and alterations in joint tissues. As the cartilage wears down, the joint space narrows, bone spurs (osteophytes) may form, and the synovium (joint lining) may become inflamed. These processes collectively contribute to pain, stiffness, and functional limitations associated with knee OA7. The inflammatory response can be sustained by the release of additional pro-inflammatory factors from immune cells that have infiltrated the site, specifically neutrophils and monocytes. The persistent inflammatory response is a factor contributing to the degradation of cartilage and other joint components, exacerbating the discomfort and functional limitations associated with knee OA8. Grade II OA is characterized by mild to moderate joint damage. At this stage, the joint deterioration and functional limitations are significant enough to warrant intervention, yet the condition has not progressed to the extent that more invasive treatments, such as surgery, become necessary. Strengthening exercises can help improve muscle strength and joint stability, while vagal nerve stimulation may aid in regulating the autonomic nervous system and reducing pain perception9.
Strength training exercises effectively manage knee OA by improving muscle strength and function, thereby reducing pain and enhancing quality of life10. Studies consistently reveal increased rates of depression among individuals with OA compared to the general population. The chronic pain, functional limitations, and reduced quality of life associated with OA can contribute to the development or exacerbation of depressive symptoms11. According to the polyvagal theory, the vagus nerve plays a role in a hierarchical model of reactions to stress and social interaction, which consists of two primary branches: the ventral vagus and the dorsal vagus. Vagal nerve stimulation (VNS) is employed to regulate the vagus nerve's function, aiming to achieve equilibrium between the ventral and dorsal vagus responses9. VNS has demonstrated the capacity to modulate neural activity, influence neurotransmitter release, and facilitate neuroplasticity. The research that has been conducted to date on VNS not only offers valuable insights into the complex interplay involving the vagus nerve, autonomic regulation, and social behavior but also sheds light on the intricate connection between VNS and the activity of norepinephrine, serotonin, and other neurotransmitters implicated in mood disorders and depression, which are common in patients with knee OA12.
Strengthening exercises and vagal nerve stimulation are noninvasive interventions that can be implemented without the need for medications or surgical procedures. This makes them attractive treatment options for individuals with grade II knee OA who prefer a conservative approach or have contraindications for other treatments. Combining strengthening exercises with polyvagal exercises may offer potential synergistic effects in the management of OA symptoms. Strengthening exercises can help improve joint stability, reduce stress on the joint, and enhance overall physical function. Vagal nerve stimulation techniques following polyvagal exercises may help regulate autonomic function, reduce pain perception, and promote relaxation and emotional well-being. This study hypothesized that the combination of these interventions would lead to improved overall outcomes for individuals diagnosed with grade II knee OA.
Based on the above, the primary objective of this study was to investigate the potential benefits of combining strengthening exercises with polyvagal theory–based exercises as a noninvasive intervention for females diagnosed with grade II knee OA. Specifically, we aimed to assess whether the synergistic effects of these interventions could lead to improved joint stability, reduced pain perception, enhanced autonomic regulation, and improved overall physical function and emotional well-being among females with Grade II knee OA.
Materials and methods
Study design
The study employed a two-arm parallel-group randomized comparative design. In this study, females (n = 60) diagnosed with grade II knee OA according to the Kellgren-Lawrence (KL) scale13 were randomized into two groups: Group 1 was assigned to perform knee strengthening exercises (n = 30), and Group 2 was assigned to perform both knee strengthening exercises and exercises based on polyvagal theory to stimulate the vagal nerve (n = 30).
Sample size
G*Power software version 3.1.9.4 (Heinrich-Heine-Universität Düsseldorf, Germany) was used to calculate the sample size. An a priori power analysis was performed for a repeated-measures analysis of variance examining within-groups and between-groups interactions with two groups and two repeated measures. For an effect size = 0.25, α = 0.05 and power = 0.95, the required sample size was n = 54 in total or 27 participants in each group. Considering an anticipated dropout rate of 10%, our study was designed to include a total of n = 60 participants at the start, distributed evenly (n = 30 individuals in each group).
Procedure
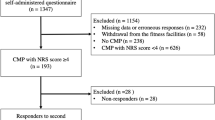
Ninety-four patients with complaints of knee pain underwent screening for grade II knee OA. However, thirty-four patients were excluded during the initial evaluation because they did not meet the inclusion criteria. The remaining 60 patients were randomly allocated into two intervention groups (with each group consisting of 30 patients): Group 1 performed only knee strengthening exercises, and Group 2 performed both knee strengthening exercises and polyvagal theory–based exercises. Randomization was performed at a 1:1 allocation ratio using sealed envelopes. Figure 1 illustrates the study procedures comprehensively through a CONSORT (2010) flow chart, outlining key stages such as assessment, enrollment, randomization, intervention allocation, follow-up, and data analysis.

A CONSORT (2010) flow chart of the study design.
Study participants
Inclusion criteria
This study included women between 45 and 60 years of age who had knee pain and were diagnosed with grade II unilateral knee OA. The decision was made to exclusively enroll female patients in this study because the incidence of knee osteoarthritis is higher in women than in men. Additionally, this approach was taken to address the potential impact of sex-related differences in critical factors such as muscle strength and mass.
Exclusion criteria
The criteria for exclusion were as follows: (i) engagement in physical exercise training within the previous year; (ii) the presence of cardiovascular diseases and/or musculoskeletal disorders that would hinder participation in exercises; (iii) a radiographic grade of 1 or > 2 according to the Kellgren-Lawrence scale; (iv) a history of knee joint surgery; (v) consumption of nonsteroidal anti-inflammatory drugs within the preceding three months for knee pain; and (vi) intra-articular administration of hyaluronic acid and/or corticosteroids within the preceding six months.
Outcome measures
Range of motion
The angle of knee flexion was measured using an app-based goniometer (DrGoniometers, CDM S.r.L), a tool that has been established as reliable and validated14. The participants lay in a supine position with the hip and knee of the affected limb flexed to a 90-degree angle while the feet were relaxed. The smartphone containing the accelerometer-based goniometer application was placed on the middle third of the anterior tibia and held in place by the examiner during the movement from the initial position to the final position. The "initial position" refers to the starting point where the hip and knee of the affected limb are flexed to a 90-degree angle, while the feet remain relaxed. A touch on the screen at this position established the 0-degree reference point. Subsequently, as the leg is moved in flexion, the examiner touches the screen again, representing the "terminal position." This terminal position signifies the final point of knee flexion in the movement and is measured while the hip maintains the same 90-degree angle of flexion.
Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC)
The WOMAC is a self-administered validated questionnaire used for the assessment of hip and knee OA15. The WOMAC consists of 24 items divided into three subscales: pain (5 questions), stiffness (2 questions), and physical function (17 questions). The subscale scores can vary from 0 to 20 for pain, 0– to 8 for stiffness, and 0–68 for physical function, with higher scores (out of a maximum score of 96) indicating worse outcomes16. After signing the consent form, the patients filled out the questionnaire questions related to pain, function and stiffness at 0 days and after 6 weeks.
Abbreviated WHO quality of life scale (WHOQOL-Bref)
To assess patients’ quality of life, the WHOQOL-Bref questionnaire was used17. This contains questions focusing on QoL related to the physical, psychological, social and environmental domains. The questionnaire comprises 26 questions on the individual's self-perceived health and well-being over the previous two weeks. Responses to questions are on a 1–5 Likert scale, where 1 represents “disagree” or “not at all” and 5 represents “completely agree” or “extremely”. The possible score in each case ranges from 0 to 100 points, with 100 points indicating no restrictions at all due to the affected knee, while a score of 0 points indicates the worst possible health status.
Resting heart rate
Resting heart rate (RHR) was assessed using the Omron HEM 742 automated oscillometric sphygmomanometer18. Participants followed specific instructions, including resting quietly for at least five minutes in a calm environment with an empty bladder. They were also advised not to engage in any physical activity; smoke; or consume alcohol, coffee, or tea for specific timeframes before the measurement. During RHR measurement, participants sat with their backs supported and arms at a 90° angle. RHR was measured twice, 15 min apart, and we used the average of these two measurements in beats per minute (bpm).
Heart rate variability
On the day of the assessment, participants were asked to lie supine for 10 min or more to attain complete relaxation. Their skin was prepared by using a razor to remove the hair from the intended site of the HR sensor (in males only), cleaning the skin and drying it with gauze. They were asked to sit in a chair with armrests. The participants were instructed to wear an HR sensor on an elastic chest strap around the thorax in direct contact with the skin. RR intervals (the time elapsed between two successive R-waves of the QRS signal on the electrocardiogram) were recorded at a sampling frequency of 1000 Hz using the HR sensor (Polar H7, Polar Electro Oy, Kempele, Finland), which was connected via Bluetooth to an Android smartphone application (Elite HRV, Asheville, NC, USA). A digital electrocardiogram (ECG) was recorded for 5 min, and blood pressure was assessed in a sitting position19.
Time-domain analysis of HRV offers insights into the heart rate's temporal characteristics and the autonomic nervous system's influence on cardiac regulation. The time-domain measures of HRV were derived from a series of RR intervals. Various time-domain HRV indices were examined, including the mean of the normal-to-normal RR interval (MeanRR), the root mean square of successive differences between adjacent RR intervals (RMSSD), and the standard deviation of normal-to-normal RR intervals (SDNN). Additionally, frequency-domain indices were explored to analyze the distribution of power spectra across different frequency bands, revealing sympathetic-parasympathetic balance and autonomic heart rate control. These indices included total power (TP), reflecting overall signal variability (0.003–0.4 Hz); low-frequency spectral power (LF), associated with both sympathetic and parasympathetic activity (0.04 and 0.15 Hz); high-frequency spectral power (HF), mainly linked to parasympathetic activity (0.15 and 0.4 Hz); normalized unit of low frequency (nuLF), representing the percentage of total power in the LF band and indicating the sympathetic-parasympathetic balance; normalized unit of high frequency (nuHF), expressing the percentage of total power in the HF band and signifying parasympathetic activity; and the ratio of low frequency to high frequency (LF/HF), frequently employed as an indicator of sympathetic-parasympathetic balance. A higher LF/HF ratio implies greater sympathetic activity, while a lower ratio indicates higher parasympathetic activity. Collectively, these HRV variables provide comprehensive insights into the relative contributions of the sympathetic and parasympathetic branches of the autonomic nervous system to heart regulation. All HR recordings underwent meticulous visual inspection to ensure stationarity and were corrected for artifacts and ectopic beats using Kubios' built-in piecewise cubic spline interpolation19.
Interventions
Knee strengthening exercise program
The targeted muscles, levels, types of exercises, and progression strategies are presented in Table 1. Each exercise was performed in 3 sets, and each repetition was held for 3 s. Both groups performed the exercises under the active supervision of the therapist 5 days a week for 6 weeks. The exercises were discontinued if an increase in pain was reported. The knee extensors, knee flexors, and gluteal muscles were targeted to improve the symptoms related to knee OA20.
Polyvagal exercise protocol
The polyvagal exercises were aimed at activating and regulating the autonomic nervous system, which plays a crucial role in physiological and emotional responses. These exercises were tailored and customized to stimulate the vagus nerve and thereby promote relaxation and improve social interaction following the principles of polyvagal theory9,21. The domains of exercise, types of exercise, procedure and duration of polyvagal exercise are presented in Table 2.
Statistical analysis
In this study, data analysis was conducted using SPSS version 23.0 (IBM Corp, Armonk, NY). Descriptive statistics, such as the mean and standard deviation (SD), were employed to present quantitative variables. The normality of data was assessed using the Shapiro‒Wilk test. An independent t test was applied to assess whether the means of the two groups were significantly different from each other, given the variation within each group. Cohen's d was employed to estimate effect size, with a confidence interval of 95% and a significance level of p < 0.05. Based on Cohen's d as a measure of effect size, the differences were classified as small (d < 0.2), moderate (0.2 < d < 0.5) and large (d ≥ 0.5). Additionally, a 2 (group) × 2 (time) repeated-measures ANOVA was utilized to examine the simple effects of time and group as well as the time × group interaction effect on outcome variables. Subsequently, post hoc pairwise comparisons were conducted to further investigate significant findings.
Ethical approval and consent to participate
The study protocol conformed to the ethical guidelines of the 1975 Declaration of Helsinki and was reviewed and approved by the ethics subcommittee of King Saud University, Riyadh, Saudi Arabia, under file ID RRC-2019-14, dated 22-04-2019. In addition, the Institutional Ethical Committee at Manav Rachna International Institute of Research & Studies approved the study protocol under reference number EC/2023-24/033, since the participants included patients visiting the OPD. Each participant was asked to submit a signed informed consent form as proof of consent to participate in the study. To ensure transparency and accountability, the study protocol was registered in the clinical trial registry at https://www.ctri.nic.in/ with the identifier CTRI/2023/08/056055.
Results
Table 3 presents the results of an independent t test to assess whether the mean values of the two groups (Group 1 and Group 2) were significantly different from each other for various outcome variables, specifically WOMAC (Western Ontario and McMaster Universities Osteoarthritis Index) and WHOQOL (World Health Organization Quality of Life) scores. On a comparison of the mean values of WOMAC subscales, although there was no significant difference in joint pain (t = − 1.06, p = 0.30), joint stiffness (t = − 1.08, p = 0.29) or functional limitations (t = − 1.38, p = 0.17) before the intervention, Group 2 demonstrated significantly greater reductions in joint pain (t = 11.55, p < 0.001), joint stiffness (t = 2.5, p = 0.02) and functional limitations (t = 5.17, p < 0.001) than Group 1 after the intervention. The effect size suggests a large difference, with Group 2 experiencing more substantial decreases in joint pain (d = 3.27), joint stiffness (d = 0.71) and functional limitations (d = 1.46). There was no significant difference in the mean WOMAC Index scores between Group 1 (68.60 ± 5.07) and Group 2 (71.32 ± 5.93) before the intervention (t = − 2.00, p = 0.05). However, after the intervention, Group 2 (30.60 ± 5.55) showed a significantly greater improvement in WOMAC scores than Group 1 (43.72 ± 5.12) (t = 8.69, p < 0.001). The effect size (Cohen's d) was 2.46, indicating a large difference between the groups. This suggests that Group 2 exhibited outcomes that were more favorable and were more effective in reducing the impact of the condition being assessed.
Furthermore, independent t tests were conducted to compare the mean values of the WHOQOL variable; there were no significant differences in the ratings of overall quality of life and general health between the pre- and post-intervention timepoints in Group 1 and Group 2. In a comparison of the physical and environmental subdomains of the WHOQOL between Group 1 and Group 2, the difference was not significant for either pre- or post-intervention assessments. In a comparison of the psychological subdomain of the WHOQOL between Group 1 and Group 2, for the pre-intervention assessment, the difference in the mean scores was not statistically significant (t = − 1.39, p = 0.17), and the effect size was small. However, for the post-intervention assessment, there was a significant difference in the mean scores for the psychological domain between Group 1 and Group 2 (t = − 6.72, p < 0.001), with a large effect size (Cohen's d = − 1.9). Additionally, in the social domain of the WHOQOL, the two groups presented similar results in the pre-intervention assessment, with no significant difference in the mean scores (t = 0.12, p = 0.91) between Group 1 and Group 2. However, for the post-intervention assessment, there was a significant difference in the mean scores for the social domain between Group 1 and Group 2 (t = − 8.89, p < 0.001), with a large effect size (Cohen's d = − 2.51), indicating a substantial difference.
The t test results indicate that there were no significant differences in resting HR between Group 1 and Group 2 at either the pre-intervention or post-intervention assessment (Table 4). There were significant differences in the RR interval between Group 1 and Group 2 at both the pre- (t = 3.3, p < 0.001) and post-intervention (t = − 2.65, p = 0.01) assessments. Furthermore, the independent t test results indicated no significant differences between Group 1 and Group 2 in terms of SDNN or RMSSD measures at either timepoint.
Independent t tests showed that there were no significant differences between Group 1 and Group 2 in LF, TP, nuLF, or nuHF at either the pretreatment or posttreatment timepoint. There was no significant difference in the pre-intervention comparison of HF between Group 1 (295.23 ± 72.19) and Group 2 (286.68 ± 90.47) (t = 0.37, p = 0.71, d = 0.1). However, Group 2 showed a significant increase in HF compared to Group 1 (t = − 4.08, p < 0.001, d = − 1.15) in the post-intervention assessment.
Before the intervention, there was no significant difference in the LF/HF ratio between Group 1 (1.89 ± 0.42) and Group 2 (2.04 ± 0.52) (t = − 1.1, p = 0.28, d = − 0.31). However, after the intervention, there was a significant difference in the LF/HF ratio between the groups (t = 3.87, p < 0.001, d = 1.09). Before the intervention, there were no significant differences in nuHF (Group 1: 21.56 ± 3.64, Group 2: 21.09 ± 4.03) between the groups (nuHF: t = 0.44, p = 0.66, d = 0.12). This suggests that the two groups initially had similar normalized HF values. After the intervention, there was a significant difference in nuHF (t = − 3.87, p < 0.001, d = − 1.1) between the groups.
Table 5 presents the results of repeated-measures ANOVA comparing outcome measures between Group 1 and Group 2, with time (pre- or post-intervention measurement) as the within-subjects factor and the outcome measure as the between-subjects factor.
Both groups showed significant improvements in range of motion (ROM) after the intervention, with the mean difference in ROM being greater in Group 2. There was a significant effect of time, suggesting an overall improvement in ROM. Both Group 1 and Group 2 experienced significant improvements in joint pain, stiffness, functional limitations, and the WOMAC index. Group 2 exhibited larger mean differences and more substantial improvements in all assessed outcome measures than Group 1.
Both groups showed significant improvements in overall quality of life; general health; and the physical, psychological, social, and environmental domains. The time effects were significant, indicating an overall improvement in quality of life across all domains. Group effects were significant for the psychological domain and the social domain.
For resting HR (beats/min), there was a significant time effect between the pre- and post-intervention timepoints; however, the group effect (Group 1 vs. 2) was not significant. Regarding the time-domain HRV measures of Mean RR (ms), SDNN (ms), and RMSSD, both Group 1 and Group 2 showed significant improvements (a time effect) after the intervention. The interaction effects were significant for Mean RR, indicating that the change in Mean RR differed between the two groups. Comparing the mean differences, it appears that Group 2 had larger improvements in Mean RR, SDNN, and RMSSD than Group 1. Therefore, Group 2 generally showed changes that were more favorable in the HRV time domain variables, indicating a potential improvement in cardiovascular health. In the HRV frequency-domain analysis, there were no significant time or group effects for LF or HF. There was a significant time effect of TP but no group effect or time × group interaction. There was a significant time effect as well as a significant time × group interaction for the LF/HF ratio. There was a significant time effect for nuLF but no significant group or interaction effect. On the other hand, nuHF showed a significant time effect, group effect and time × group interaction.
Discussion
This study aimed to compare the effects of knee strengthening exercises (Group 1) and exercises based on polyvagal theory combined with knee strengthening exercises (Group 2) in females with grade II knee OA. The study assessed various outcome variables, including WOMAC scores (joint pain, joint stiffness, functional limitations, and the overall index) and WHOQOL scores measuring QoL; general health; and the physical, psychological, social, and environmental domains. Additionally, autonomic function was measured by heart rate variability (HRV) measures, which were analyzed in the time and frequency domains.
Polyvagal theory, proposed by Porges, suggests that the vagus nerve plays a crucial role in regulating the autonomic nervous system and influencing emotional states, stress responses, and social engagement. Engaging in activities that stimulate the vagus nerve, such as the exercises described, may promote relaxation, reduce anxiety, and enhance emotional regulation. These outcomes could ultimately contribute to a reduction in perceived pain and an increase in quality of life in patients with knee osteoarthritis9. Vagus nerve stimulation has multifaceted mechanisms that could explain its potential benefits for individuals with knee osteoarthritis. It activates the parasympathetic nervous system, increasing vagal tone while reducing sympathetic activity, which might lead to pain reduction and enhanced well-being9. Moreover, vagal stimulation exhibits anti-inflammatory effects, regulating immune responses and potentially alleviating arthritic joint inflammation, thus contributing to pain relief22. Additionally, by influencing central pain mechanisms and neural pathways, VNS can modulate pain perception and processing, thereby potentially enhancing pain relief22. Finally, vagal stimulation's impact on neuroplasticity could lead to lasting improvements in pain and quality of life for those with knee osteoarthritis5.
The WOMAC assessment for knee OA is a sensitive tool, well suited for detecting changes in symptoms and function over time or in response to interventions. This evaluation captures the patient's perspective, facilitating a comprehensive assessment of the impact of knee OA on daily life and functioning16. In the present study, both groups displayed effects as measured by WOMAC subscales; however, the group that performed VNS exercises demonstrated notable improvements in pain, stiffness and functional limitations. Notably, the results indicated that Group 2 exhibited significantly greater reductions in joint pain, joint stiffness, and functional limitations than Group 1 after 6 weeks. Group 2 also exhibited significant improvements in the WOMAC index scores, reflecting favorable overall outcomes. In terms of quality of life, Group 2 demonstrated marked enhancements in the psychological and social domains compared to Group 1. However, there were no significant differences observed in the physical domain or the environmental domain.
Muscle and skeletal problems constitute over a quarter of nonlethal health losses, with pain being the most significant contributor23. Chronic pain related to OA not only restricts social functioning but also heightens the risk of psychological issues24, depression25 and diminished work capabilities26. The finding of this study underscores the favorable response observed with polyvagal exercises, which predominantly focus on relaxation. As a nonpharmacological intervention, relaxation is increasingly employed to alleviate pain and enhance pain management27. This finding aligns with Turk and Winter’s research, illustrating that achieving a state of physical and mental relaxation influences psychological and bodily well-being, fostering calmness and contributing to the reduction of pain28. Further reinforcement is derived from a study by Onivea-Zefra et al., who demonstrate the potential of guided imagery relaxation in reducing pain levels among fibromyalgia patients. Through the utilization of visualizations and mental imagery techniques, this approach promotes relaxation and helps in alleviating pain perception29.
Another study by Morone and Greco reinforces the findings that guided imagery and relaxation offer clinical pain management benefits for individuals with knee OA30. The reduction in pain, functional limitations and stiffness could also be attributed to the effects of strengthening exercises. Strength training has been linked to potential disease-modifying impacts in OA. Regular exercise can promote joint health, stimulate cartilage metabolism, and improve muscle strength and joint stability31.
In individuals with osteoarthritis, pain is the most prevalent complaint and a primary contributor to reduced health-related quality of life (HRQoL). In this study, both groups demonstrated significant improvements across various domains of quality of life, including overall quality; general health; and physical, psychological, social, and environmental aspects. Notably, Group 2 exhibited more substantial enhancements in overall quality of life, general health, psychological, social, and environmental domains than Group A, which underwent vagal nerve stimulation-based exercise. The improvement in the physical domain is attributed to the 6-week exercise regimen, a sentiment that aligns with Smith et al.’s findings, emphasizing the efficacy of a scalable exercise program in enhancing the well-being and function of hip and knee OA patients32. Various techniques, including deep breathing, meditation, relaxation exercises, and specific physical activities, can stimulate the vagus nerve and enhance its functionality. These exercises may facilitate relaxation, stress reduction, and overall well-being. Goff et al.’s findings agree with ours, suggesting that patient education positively impacts conservative treatment and can be productively used in concert with it33. Our results are corroborated by Ebenezer et al.’s study, which revealed that patients treated with yoga experienced substantial improvements in QoL, paralleling the effects of therapeutic exercise on OA patients. The shared impact of yoga on emotional stability and quality of life, a factor pivotal in pain reduction and enhanced quality of life, is a significant highlight of their research34.
Vagal stimulation, in line with the polyvagal theory, is also emphasized by Wang et al., who suggest that practices such as yoga—a form of physical and relaxation exercise—have a systemic effect. By stimulating parasympathetic pathways, yoga reduces perceived pain and improves QoL35. Regarding heart rate variability (HRV), Group 2 exhibited a notable increase in high-frequency power (HF) and a significant decrease in the LF/HF ratio, indicating enhanced autonomic regulation. These outcomes imply that the combination of polyvagal exercises and knee-strengthening training yields a favorable impact on HRV, reflecting improved cardiovascular health. Interestingly, a positive correlation exists between disability and cardiovascular health in patients with knee OA. This is underscored by Tsubio et al.’s discovery of a connection between degenerative diseases and causes of death in Japan, revealing that individuals with knee OA are at an elevated risk of heart attacks leading to mortality36. This underscores the imperative for enhanced autonomic regulation in knee OA patients.
The observed changes in HRV parameters can be attributed to the stimulation of the vagal nerve. This emphasizes the contention of the polyvagal theory that the physiological state is not merely a correlate but a fundamental component of emotions and moods. Within this theoretical framework, the autonomic state functions as an intermediary variable that influences our perception and evaluation of environmental stimuli. The reflexive assessment of cues as neutral, positive or threatening can vary based on an individual's physiological state. Functionally, changes in an individual’s state can lead to a shift in the accessibility of different brain structures, facilitating social communication or eliciting defensive responses such as fight/flight or shutdown37. Goldbeck et al. also emphasized the importance of yoga-based exercises in enhancing HRV parameters, consequently improving parasympathetic activity38.
The study had a few limitations that should be noted. It had a small sample size, exclusively female participants, and a lack of long-term follow-up. While generalization to the wider population should be approached with caution, the study's findings still contribute to a broader understanding of the potential benefits of the interventions within this specific subset of patients. The decision to include female participants only was driven by the fact that knee osteoarthritis is more commonly observed in females than in males. Evaluating the sustainability and durability of the benefits conferred by polyvagal exercises in the long term could provide a more comprehensive understanding of their effects and guide clinical recommendations. Furthermore, there was no control group, and blinding procedures were not implemented. The inability to implement blinding in this study is attributable to the nature of the interventions employed, which made it a practical challenge to blind participants and researchers to the group assignments, as the participants themselves needed to be aware of the specific exercises they were performing. The study relied on self-reported measures and did not use objective measures. A total reliance on self-reported measures, without the use of objective assessments, introduces the potential for measurement bias due to participants' subjective perceptions and recall biases. Integrating objective measures such as biomechanical assessments or biomarkers would offer a more comprehensive understanding of the interventions' effects. Finally, the dropout rate was 10%, which may have affected the representativeness of the final sample and introduced potential bias.
Conclusions
The study highlights the potential benefits of combining strengthening exercises with exercises based on polyvagal theory in the management of grade II knee OA. Strengthening exercises can improve joint stability and reduce stress on the joint, while exercises based on polyvagal therapy may help regulate autonomic function, reduce pain perception, and promote relaxation and emotional well-being. The combination of these interventions may lead to superior overall outcomes and improved quality of life for individuals with knee osteoarthritis. These results support the potential effectiveness of incorporating polyvagal exercise as an adjunctive intervention for osteoarthritis management.
Future scope
The study opens up several potential avenues for future research. First, conducting a larger-scale study with a more diverse participant pool, including both genders, would help establish the generalizability of the findings. Long-term follow-up assessments could be incorporated to examine the sustainability and durability of the effects observed. Additionally, incorporating a control group and implementing blinding procedures would enhance the study's internal validity. Objective measures, such as physiological recordings, could be used in conjunction with self-report measures to provide a more comprehensive understanding of the outcomes. Exploring different stimulation parameters and investigating the mechanisms underlying vagal nerve stimulation could further elucidate its therapeutic potential. Overall, future research should build upon these limitations to strengthen the evidentiary base and better inform clinical applications of VNS.
Data availability
All data generated or analyzed during this study are presented in the manuscript. Please contact the corresponding author for access to the data from this study.
References
Grazio, S. & Balen, D. Obesity: Risk factor and predictor of osteoarthritis. Lijec. Vjesn. 131(1–2), 22–26 (2009).
Cui, A., Li, H., Wang, D., Zhong, J., Chen, Y. & Lu, H. Global, regional prevalence, incidence and risk factors of knee osteoarthritis in population-based studies. EClinicalMedicine. 29 (2020).
Kaur, R., Ghosh, A. & Singh, A. Prevalence of knee osteoarthritis and its determinants in 30–60 years old women of Gurdaspur, Punjab. Int. J. Med. Sci. Public Health 7(10), 825–831 (2018).
Taheri, M., Farzian, S., Esmaeili, A. & Shabani, E. The effect of water therapy and jogging exercises on the health-related factors of physical fitness of elderly women. Int. J. Sport Stud. Health. 3(2) (2020).
Alves, J. C. & Bassitt, D. P. Quality of life and functional capacity of elderly women with knee osteoarthritis. Einstein (Sao Paulo). 11, 209–215 (2013).
Arslan D, ÜNAL ÇEVİK I. Interactions between the painful disorders and the autonomic nervous system. Agri J. Turk. Soc. Algol. 34(3) (2022).
Mora, J. C., Przkora, R., Cruz-Almeida, Y. Knee osteoarthritis: Pathophysiology and current treatment modalities. J. Pain Res. 2189–2196 (2018).
Richebé, P., Capdevila, X. & Rivat, C. Persistent postsurgical pain: Pathophysiology and preventative pharmacologic considerations. Anesthesiology 129(3), 590–607 (2018).
Porges, S. W. & Dana, D. Clinical Applications of the Polyvagal Theory: The Emergence of Polyvagal-Informed Therapies (Norton Series on Interpersonal Neurobiology) (WW Norton & Company, 2018).
Farr, J. N. et al. Progressive resistance training improves overall physical activity levels in patients with early osteoarthritis of the knee: A randomized controlled trial. Phys. Ther. 90(3), 356–366 (2010).
Wang, S.-T. & Ni, G.-X. Depression in osteoarthritis: Current understanding. Neuropsychiatr. Dis. Treat. 18, 375 (2022).
Ruffoli, R. et al. The chemical neuroanatomy of vagus nerve stimulation. J. Chem. Neuroanat. 42(4), 288–296 (2011).
Kumar, H., Pal, C. P., Sharma, Y. K., Kumar, S. & Uppal, A. Epidemiology of knee osteoarthritis using Kellgren and Lawrence scale in Indian population. J. Clin. Orthop. Trauma 11, S125–S129 (2020).
Dunlevy, C., Cooney, M. & Gormely, J. Procedural considerations for photographic-based joint angle measurements. Physiother. Res. Int. 10(4), 190–200 (2005).
Salaffi, F. et al. Reliability and validity of the Western Ontario and McMaster Universities (WOMAC) Osteoarthritis Index in Italian patients with osteoarthritis of the knee. Osteoarthr. Cartil. 11(8), 551–60 (2003).
Pollard, B., Johnston, M. & Dixon, D. Exploring differential item functioning in the Western Ontario and McMaster universities osteoarthritis index (WOMAC). BMC Musculoskelet. Disord. 13(1), 1–10 (2012).
Snell, D. L., Siegert, R. J., Surgenor, L. J., Dunn, J. A. & Hooper, G. J. Evaluating quality of life outcomes following joint replacement: Psychometric evaluation of a short form of the WHOQOL-Bref. Qual. Life Res. 25, 51–61 (2016).
Christofaro, D. G. D. et al. Validation of the Omron HEM 742 blood pressure monitoring device in adolescents. Arq. Bras. Cardiol. 92, 10–5 (2009).
Garg, S. et al. The cardiac comeback-beating stronger: Exploring the remarkable resilience of the heart in COVID-19 recovery through cardiac autonomic analysis. Medicina 59(8), 1397 (2023).
Abbott, J. H. Management of osteoarthritis: A guide to non-surgical intervention. Centre for Musculoskeletal Outcomes Research (2014).
Porges, S. W. & Lewis, G. F. The polyvagal hypothesis: Common mechanisms mediating autonomic regulation, vocalizations and listening. In Handbook of Behavioral Neuroscience: 255–264 (Elsevier, 2010).
Bassi, G. S. et al. Modulation of experimental arthritis by vagal sensory and central brain stimulation. Brain Behav. Immun. 64, 330–343 (2017).
Agaliotis, M., Mackey, M. G., Jan, S. & Fransen, M. Burden of reduced work productivity among people with chronic knee pain: A systematic review. Occup. Environ. Med. 71(9), 651–659 (2014).
Jank, R., Gallee, A., Boeckle, M., Fiegl, S. & Pieh, C. Chronic pain and sleep disorders in primary care. Pain Res. Treat. 2017 (2017).
Bair, M. J., Robinson, R. L., Katon, W. & Kroenke, K. Depression and pain comorbidity: A literature review. Arch. Intern. Med. 163(20), 2433–2445 (2003).
Landmark, T. et al. Chronic pain: One year prevalence and associated characteristics (the HUNT pain study). Scand. J. Pain 4(4), 182–187 (2013).
Bushnell, M. C., Čeko, M. & Low, L. A. Cognitive and emotional control of pain and its disruption in chronic pain. Nat. Rev. Neurosci. 14(7), 502–511 (2013).
Turk, D. C. & Winter, F. The Pain Survival Guide: How to Reclaim Your Life. American Psychological Association (2006).
Onieva-Zafra, M. D., García, L. H. & Del Valle, M. G. Effectiveness of guided imagery relaxation on levels of pain and depression in patients diagnosed with fibromyalgia. Holist. Nurs. Pract. 29(1), 13–21 (2015).
Morone, N. E. & Greco, C. M. Mind–body interventions for chronic pain in older adults: A structured review. Pain Med. 8(4), 359–375 (2007).
Bartels, E. M., Juhl, C. B., Christensen, R., Hagen, K. B., Danneskiold‐Samsøe, B., Dagfinrud, H. et al. Aquatic exercise for the treatment of knee and hip osteoarthritis. Cochrane Database Syst. Rev. 2016(3).
Smith, J. L., Innes, A. Q., Burns, D. S., Deniszczyc, D., Selfe, J., MacConville, S. et al. A scalable 12-week exercise and education programme reduces symptoms and improves function and wellbeing in people with hip and knee osteoarthritis. Front. Rehabil. Sci. 4 (2023).
Goff, A. J. et al. Patient education improves pain and function in people with knee osteoarthritis with better effects when combined with exercise therapy: A systematic review. J. Physiother. 67(3), 177–189 (2021).
Ebnezar, J., Nagarathna, R., Bali, Y. & Nagendra, H. R. Effect of an integrated approach of yoga therapy on quality of life in osteoarthritis of the knee joint: A randomized control study. Int. J. Yoga 4(2), 55 (2011).
Wang, Y., Lu, S., Wang, R., Jiang, P., Rao, F., Wang, B. et al. Integrative effect of yoga practice in patients with knee arthritis: A PRISMA-compliant meta-analysis. Medicine 97(31) (2018).
Tsuboi, M. et al. Do musculoskeletal degenerative diseases affect mortality and cause of death after 10 years in Japan?. J. Bone Miner. Metab. 29, 217–223 (2011).
Groves, D. A. & Brown, V. J. Vagal nerve stimulation: A review of its applications and potential mechanisms that mediate its clinical effects. Neurosci. Biobehav. Rev. 29(3), 493–500 (2005).
Goldbeck, F., Xie, Y. L., Hautzinger, M., Fallgatter, A. J., Sudeck, G. & Ehlis, A.-C. Relaxation or regulation: The acute effect of mind-body exercise on heart rate variability and subjective state in experienced Qi Gong practitioners. Evid.-Based Complement. Altern. Med. 2021 (2021).
Acknowledgements
The authors are grateful to the Researcher Support Project (number RSP2023R382), King Saud University, Riyadh, Saudi Arabia, for funding this research.
Funding
This study was funded by the Researcher Support Project (number RSP2023R382), King Saud University, Riyadh, Saudi Arabia.
Author information
Authors and Affiliations
Contributions
M.R.R., A.S., S.H., F.A. A.H.A. and M.R.A. proposed the study concept and design. M.R.R. and A.S. planned the methodology. A.S. collected data. A.I., A.H.A., and F.A. contributed to the data analysis. S.H., A.H.A., F.A., M.R.A. and A.I. contributed to the data interpretation. A.S. M.R.A. S.H. and A.I. prepared the manuscript’s initial draft. M.R.R., S.H., F.A. and A.H.A. critically reviewed and edited the manuscript for intellectual content. All authors have read, understood, reviewed, and approved the manuscript’s final version to be submitted/published and take responsibility for the intellectual content of the same manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Rizvi, M.R., Sharma, A., Hasan, S. et al. Exploring the impact of integrated polyvagal exercises and knee reinforcement in females with grade II knee osteoarthritis: a randomized controlled trial. Sci Rep 13, 18964 (2023). https://doi.org/10.1038/s41598-023-45908-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-023-45908-4
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
