
Abstract
The aims of this study were to evaluate the feasibility of the New Zealand White (NZW) rabbit for studying implanted biomaterials in pelvic reconstructive surgery; and to compare the occurrence of graft-related complications of a commercial polypropylene (PP) mesh and new developed human dermal matrix implanted at vaginal and abdominal level. 20 white female NZW rabbits were randomized into two groups, experimental group (human acellular dermal matrices-hADM-graft) and control group (commercial PP graft). In each animal, grafts were surgically implanted subcutaneously in the abdominal wall and in the vaginal submucosa layer for 180 days. The graft segments were then removed and the surgical and clinical results were analyzed. The main surgical challenges during graft implantation were: (a) an adequate vaginal exposure while maintaining the integrity of the vaginal mucosa layer; (b) to keep aseptic conditions; (c) to locate and dissect the breast vein abdominal surgery; and (d) to withdraw blood samples from the ear artery. The most abnormal findings during the explant surgery were found in the PP group (33% of vaginal mesh extrusion) in comparison with the hADM group (0% of vaginal graft extrusion), p = 0.015. Interestingly, macroscopic observation showed that the integration of the vaginal grafts was more common in the hADM group (40%) than in the PP group, in which the vaginal mesh was identified in 100% of the animals (p = 0.014). The NZW rabbit is a good model for assessing materials to be used as grafts for pelvic reconstructive surgery and vaginal surgery. Animals are easily managed during the procedures, including surgical intervention and vaginal mucosa approach. Additionally, hADM is associated with fewer clinical complications, as well as better macroscopic tissue integration, compared to PP mesh.
Similar content being viewed by others


Introduction
Pelvic floor dysfunctions (PFD) such as pelvic organ prolapse (POP), or urinary incontinence (UI) are common conditions that affect a third of the adult female population1. In these frequent dysfunctions, surgical treatment has shown good results. The surgical repair may involve the use of non-absorbable, synthetic prostheses, usually polypropylene (PP). PP meshes have been associated with severe complications such as erosion, retraction, and pain2.
In July 2018, the use of mesh implants to treat stress urinary incontinence was suspended by the National Health Service (NHS) of the United Kingdom3. And in April 2019 the United States (US) Food and Drug Administration (FDA) banned vaginally-placed mesh implants for treating pelvic organ prolapse4. With this growing concern for safety, there is a worldwide agreement on the need for research and innovation to find alternative materials to be used in pelvic reconstructive surgery.
This need of new materials with an effective and safe mesh design has approached the development of acellular matrices (AM). AMs represent a new generation of biocompatible materials processed to obtain a decellularized scaffold of fibers whose architecture and extracellular matrix remain intact5,6,7.
In recent years, many different types of biological meshes have been marketed and their efficacy evaluated8,9. Specifically, human acellular dermal matrices (hADM), available in the US for more than 15 years, have been used in more than 2 million implant procedures and information is available on its clinical safety and efficacy in different clinical applications10,11. Reconstructive surgeries such as chronic wounds closure, immediate breast reconstruction, abdominal wall and hernia repair, and tendon reinforcement are likely to use dermal matrices10,12,13.
However, the gynecological application of dermal matrices has been poorly evaluated14, and there is limited information about the behaviour of vaginally applied hADM. Therefore, it is required to carry out preclinical studies to assess hADM in the repair of PFD. In this way, international associations such as the International Urogynecological Association (IUGA) have presented a consensus document that specify the steps to follow for the introduction of new devices to be used in prolapse surgery, and they recommend to previously perform preclinical studies in animals for the evaluation of the host's inflammatory response15.
The election of the most suitable animal model to obtain clinical results after placing the hADM at the vaginal level requires to fulfill different objectives and conditions. The most studied animals are mice, rat, rabbit, sheep, pig, and non-human primates (NHP). Published studies show that several models can be used, and there is no animal that is perfect for this purpose. Each one has its own benefits and weakness16,17,18.
We selected the New Zealand White (NZW) rabbit as animal model because of its adequate life expectancy for the duration of the study, it has perineal musculature associated with the urogenital tract similar to humans19,20, and has appropriate vaginal size to perform a vaginal graft placement. Additionally, the rabbits are economical and easily housed, handled and anaesthetized.
Another advantage of this model is that it allows the study of implants in the vaginal and abdominal location in the same animal concomitantly, with the aim of evaluating whether clinical changes appear depending on the implant location.
Other animals have a reproductive and urinary pathophysiology more similar to humans than rabbits, such as ewes or NHP16,17,18. These models would probably be better for studying the physiology of POP or UI. However, this research does not pretend to study the therapeutic efficacy of hADM. Instead, it is dedicated to demonstrating the occurrence of local complications, such as exposure or infection, especially at vaginal location. Additionally, the scientific literature shows many examples of experimental studies using NZW rabbits for the evaluation of new biomaterials for the treatment of PFD21,22,23,24,25,26,27,28,29,30,31.
This study aims to describe the surgical complexity of the NZW rabbit model, their clinical monitoring, as well as the standardization of the model. It includes the description of the surgical difficulties of implanting prostheses at the vaginal and abdominal level in rabbits, as well as the difficulties in housing them, and the occurrence of graft-related complications in different locations.
This information could guide future works designed to test devices for vaginal application and will help other groups that focus their research in the urogynecology area.
Material and methods
Experimental design and subjects of study
The study was performed by Barcelona Tissue Bank (BTB), the Hospital de la Santa Creu i Sant Pau, and at the Research Institute of the Hospital de Sant Pau-IIB Sant Pau.
The study protocol was approved by the Internal Animal Care and Use Committee (CEEA-IRHSCSP) and the competent government authority (Generalitat de Catalunya, Animal Experimentation Commission, project number 9669). All animal procedures were carried out in strict accordance with the guidelines of Directive 2010/63/EU of the European Parliament on the protection of animals used for scientific purposes. In addition, we followed the ARRIVE guidelines and committed ourselves to the 3Rs of laboratory animal research. The animal experimental project was performed in the Animal Experimental Service of the accredited IRHSCSP, ISO 9001:2015 accredited.
This study followed the ethical precepts of the Declaration of Helsinki and was approved by local ethics committee. Human tissue was processed according to guidance for clinical use (EEC regulations 2004/23/CE and 2006/17/CE) and to the legal requirements for the use of biological samples for research in Spain (Law 14/2007 and RD 1716/2011). Ethics institutional review board (IRB) approval was obtained (CEIm Hospital Valle Hebrón, Barcelona; PR (BST)314/2019). In all cases, informed consent was obtained from the donors' relatives.
A total of 20 female multiparous NZW rabbits were randomly allocated to receive control (PP mesh) or experimental (hADM) grafts.
Each rabbit received 4 grafts: 2 grafts in the vaginal submucosa layer and two in the subcutaneous tissue of the abdominal wall, over the muscular fascia.
Regarding the vaginal grafts, one (5 × 5 mm) was placed in the anterior vaginal wall and used for histological and immunohistochemical studies. The other one (10 × 5 mm) was placed in the submucosa of the posterior vaginal wall and was used to perform the biomechanical study.
The size of the abdominal grafts was the same as that of the vaginal grafts, but both were stitched together in the right caudal quarter of the abdominal wall.
The implants were removed 180 days later, at which time the animals were also humanely euthanized.
Graft preparation
Preparation of hADM samples
hADM was obtained from skin tissue procured from the back and lower limbs of a human cadaveric donor by manual dermatome. The tissue was processed in clean rooms in accordance with Good Manufacturing Practices (GMP) regulations in the BTB. The processing consisted of, first, the selection of the homogeneous fragments in thickness and their decontamination in antibiotic solution for 16–24 h, and then their decellularization. Decellularization was achieved by chemical, biological and mechanical treatment as follows: the skin was incubated in hypertonic solution, which led to the cellular lysis, then an incubation in a proteolytic enzyme, resulting in the removal of the genetic material, and a final incubation in anionic surfactant for the washing out of the cellular debris. In order to remove any reagent, 10 washes were carried out in 0.9% NaCl. The 10 × 5 mm samples were prepared and stored in glycerol solution in a double bag at room temperature until use. To ensure strict microbiological control, several microbiological controls were performed throughout the graft processing.
PP graft preparation
The material (Gyneband, Mallanets, Spain) was delivered in a commercial sterile container, ready for medical use in humans. Under conditions of surgical asepsis, it was removed from the container and cut into 10 × 5 mm and 5 × 5 mm pieces immediately before proceeding to the implant surgery.
Surgical procedure
Animals were anesthetized with ketamine (15 mg/kg subcutaneous; sc) and medetomidine (0.5 mg/kg sc). Each rabbit received a prophylactic antibiotic dose (Ceftiofur 50 mg/kg sc) and nonsteroidal anti-inflammatory drug (meloxicam 1 mg/kg intramuscular -im-).
Before starting the surgery, the areas of surgical incision were shaved and disinfected, and blood samples (6 cc) were obtained from the ear artery to study inflammatory markers. Serial blood samples were obtained on days: 0 (day of implantation surgery, 7, 30 and 180 (day of euthanasia).
Abdominal implants
A transverse incision was made in the abdominal midline, at the level of the intermammary line of the last two nipples on the right side of the rabbit, to expose the anterior abdominal fascia. Both fragments of the graft (hADM or PP) were positioned and fixed with prolene (Ethicon) 5/0 discontinuous suture (Fig. 1C). The abdominal wall was closed with 4/0 vicryl rapide (Ethicon) thread in two layers: continuous suture for subcutaneous tissue, and continuous intradermal suture for skin tissue.

Vaginal and abdominal implant placement in NSW rabbit model. (A) hADM fixed in posterior vaginal submucosal layer. (B) hADM fixed in anterior vaginal submucosal layer. (C) hADM fixed in the subcutaneous tissue of the abdominal wall.
Vaginal implants
A transverse incision was made in the anterior vaginal wall, approximately 1 cm from the vaginal entrance. The vaginal mucosa layer was dissected and the 5 × 5 mm graft was implanted and fixed with the same procedure as in the abdominal implant (Fig. 1B). The same procedure was repeated on the posterior vaginal wall, using the 10 × 5 mm graft (Fig. 1A).
The vaginal mucosa was closed with a 4/0 vicryl thread using an interrupted suture.
Once the implants had been placed, a preventive dose of buprenorphine (0.01 mg/kg, sc) was administered. To avoid licking and infection of the wound, rabbits wore a protective collar for 7 days after surgery. Animals could move freely in their pens and were under a strict veterinary control. During the entire period of study animals were supervised daily and weighted weekly and complications related to the implant were closely monitored.
After 180 days, rabbits were anesthetized as described before and the grafts were explanted, removing the prosthesis together with surrounding tissue.
Animals were euthanized under deep anesthesia according to the protocol by administration of 150 mg/kg intravenous pentobarbital.
Variables and parameters investigated at surgery and at follow-up
Surgical variables
Surgical time duration, complications and difficulties were collected by the investigator during the implant surgery.
Clinical complications during animal follow-up
Signs of pain/stress in the animals were evaluated by the Grimace Scale. This scale allows an objective evaluation of animals' pain and distress through their facial expression, especially orbital closure, the flattening of the cheeks, angulation of the nostrils, stiffness of the whiskers and subsequent rectification of the ears. Each item was scored from 0 to 3, as follows: 0 = not present, 1 = moderately present and 2 = obviously present.
Pain/discomfort (any value > 1) was treated with an additional painkiller dose (buprenorphine, 0.01 mg/kg, sc).
Signs of loss of well-being: anxiety, depression, inactivity, restlessness, shrieks, or groans, grinding of teeth, tonic immobility, rejection of water and/or food, weight loss were also surveyed. Clinical signs of surgical site complication were equally inspected and registered.
Macroscopic observation of explants
During explant surgery, the macroscopic aspect of the explants was evaluated with particular interest in the presence of: (a) evidence of seroma (accumulation of serous fluid around the graft); (b) signs of local infection (erythema or purulent suppuration); and, (c) evidence of extrusion of the graft (skin necrosis or dehiscence of the surgical wound with exposure of the graft).
Statistical analysis
As descriptive data analysis we used the median, and also the mean with standard deviation. The relationship between categorical variables was analyzed using the corresponding contingency tables, calculating the percentage in each group and application of chi-square test with the approximation of the probability ratio. In the ordinal variables, the comparison between two groups was made with non-parametric Mann–Whitney test. In all cases, the usual level of significance was 5% (alpha = 0.05). All analyses were performed with the statistical IBM-SPSS package (V25).
Results
Twenty animals were included, 10 in the experimental group (hADM), and 10 in the control group (PP). During the study (83 days after surgery), one rabbit in the control group died due to causes not related to the grafts.
Surgical challenges during surgical graft implantation
Exposure of the vaginal surgical field
Due to the small size of the surgical field, a recurring difficulty was the vaginal exposure. This challenge was overcome by placing an eyelid retractor in the vaginal introitus. The rest of the instruments used were the standard microsurgical devices.
Integrity of the vaginal mucosa layer
Grafts were implanted at the level of the vaginal submucosa layer, so a meticulous vaginal dissection was needed. Because it is an extremely thin layer, another difficulty in most of the surgeries performed was to maintain the integrity of the vaginal mucosa layer during the graft implantation. The maintenance of this layer is crucial to reduce the risk of future implant extrusions. Despite these difficulties, the preservation of the mucosa was successfully obtained in all animals.
Aseptic conditions
It was difficult to keep aseptic conditions due to the large amount of hair in this animal model. The methods used to achieve adequate asepsis in the surgical field were an extensive shaving of the NZW’s abdomen and external genitalia, and a careful and precise handling of the animals during surgeries.
Location and dissection of the breast vein during abdominal surgery
During abdominal surgery, the last two nipples on the right side of the animal were used as anatomical reference to locate the explant position during its surgical removal.
The breast vein is located at the intermammary line. This situation required a careful dissection to avoid accidental damage during implantation surgery. In one case, the vein was damaged and resulted in an extensive bleeding that was resolved with a hemostatic stitch; however, the animal presented postoperatively an abdominal wall hematoma that was resolved spontaneously after few days.
Blood extraction from the ear artery
Blood withdrawal from the ear artery may be a difficult procedure. Blood was obtained in 79 occasions. In 6 cases (4.74%) we experienced difficulties that led to the collection of insufficient blood volume to complete the studies. These difficulties occurred in both groups.
Surgical variables, clinical findings during the animal follow-up and macroscopic study of explants are described in Table 1.

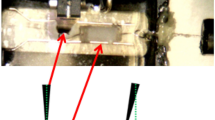
Multiple purulent collections arranged around the mesh, during explant removal surgery.
Surgical complications of implant surgery
Only one animal suffered a mild hemorrhage in the subcutaneous tissue during abdominal surgery, which was resolved with a hemostatic suture.
Clinical complications during follow-up
Clinical complications occurred, and actions taken during follow-up and are described in Table 2. The Grimace scale was 0 in all animals and in all evaluations during follow-up.
Discussion
This research has evaluated the feasibility of the rabbit as an animal model for the study of biological grafts placed in the abdominal and vaginal locations, and it shows that the NZW is a good model for studying the behaviour of biomaterials in either locations.
The hADM used in this study is an acellular biological matrix, obtained from human dermis, produced to improve the biocompatibility of grafts over that of current synthetic alternatives. hADM is free of allergens, DNA and other pathogens. In this study, the hADMs were implanted in the abdominal fascia and in the vaginal submucosa layer of rabbits. The aim was to evaluate clinical complications during and after graft implantation surgery and macroscopic findings after graft explantation surgery, in different in vivo settings. We used the rabbit as a model on the basis of previous publications, as well as on the characteristics of the animal: adequate life expectancy for the duration of the study; perineal musculature associated with the urogenital tract like humans; enough vaginal ability to perform a vaginal and abdominal implant at the same time; easy and economical animal accommodation; and the availability of investigators trained in handling these animal species.
Other animal models besides the rabbit have been used to study biomaterials in urogynecology17. Rats32,33,34,35,36,37,38,39,40 were used; however, due to its small body size studies at vaginal level are very difficult to be performed. The same for mice18, where most studied materials are implanted subcutaneously, rather than vaginally41,42,43.
Reviewing studies with large animal models, authors such as Endo et al.44, Tayrac et al.45, or Feola et al.46 studied biological prostheses at vaginal level in sheep. Endo M. compared a cross-linked acellular collagen matrix with a PP mesh, placed simultaneously at vagina and abdomen, also demonstrating greater degradation of vaginal implants (70%). Tayrac compared a noncoated PP mesh against a coated PP mesh with an absorbable hydrophilic film, placed vaginally. In this case, an increase in vaginal exposure rate was also demonstrated in the noncoated PP group (33.3%). Finally, Feola A. compared a PP mesh, a collagen-coated mesh and the native tissue implanted in the vagina and abdomen. This study also showed 22% vaginal erosion rate associated with PP mesh group. These results are consistent with our findings. However, ewes are a more complicated and expensive model that many research centers cannot afford.
Regarding the pig model47, the drawbacks are similar to those of sheep: although it has enough size to perform vaginal surgery, and its anatomy is appropriated to the human being, the time required to perform the explants (180 days) makes the sows to increase their weight over 150 kg, which means that the handling of these animals and the costs of the study, even using minipigs, preclude their use in some groups. In the case of the dogs48 and NHP, one should add the ethical and legal conflicts concerns.
There are several authors that have used the rabbit model to study different biomaterials in gynecology21,22,23,24,25,26,27,28,29,30,31; therefore, we strongly believe that the rabbit is a good model for the study of biomaterials for abdominal and vaginal application.
Graft implantation at the level of the abdominal subcutaneous tissue and in the anterior and posterior vaginal submucosa layer of rabbits was technically simple, and it was associated with very minor surgical complications. However, adequate exposure of the vaginal field is difficult due to its small size. Hence, appropriated training of an assistant and the specific surgical material (suitable for microsurgery) are needed.
Ear blood extraction was also challenging, especially after successive extractions in the same animal because of the narrowing of the vascular lumen secondary to consecutive punctures. Therefore, it is advisable to have the help of trained personnel to perform this technique. Another cause of difficulty in blood withdrawal is the arterial vasoconstriction associated with the decrease in the body temperature of the animals, as well as pain at the puncture site if adequate anesthesia is not achieved.
Complications during the clinical monitoring consisted in minor facial injuries due to accidental incorrect position of the protective collar. To avoid other similar types of injury, protective collars were removed after observing there were no self-inflicted injuries in the surgical wound area. Animals did not show signs of pain during follow-up, so we concluded that a quick, low-invasive, and uncomplicated surgical manipulation is associated with low postoperative pain allowing the avoidance of protective collar placement.
In both groups, stereotypical self-injuries appeared, so it is very important to add environmental enrichment measures in these animals. It is also very important to maintain strict hygiene measures to avoid complications derived from dirtiness.
The occurrence of graft-related complications of implants showed a very different behavior between two groups, especially in the vaginal location.
The clinical complications associated with the graft (wound infection and exposure) were more common in the control (PP synthetic mesh) group, especially in the vaginal location where mesh exposure occurred in 33% of cases (p = 0.024). Conversely, in the experimental group, macroscopic hADM degradation at the vaginal level occurred in 40% of cases as compared with 0% in the PP group (p = 0.014) whereas in the abdominal location the macroscopic characteristics of the hADM graft remained intact in all cases. These results are consistent with the publications of: Hilger et al.25, Pierce et al.27 and Higgins et al.49. Hilger compared human dermis, porcine dermis, porcine collagen-coated PP mesh, and autologous fascia, implanted in the abdomen and the vagina of a rabbit, also demonstrating greater degradation of the implants in the vaginal location. Pierce compared PP mesh with porcine dermis placed in the vagina and abdomen in a rabbit and observed a 30% degradation rate of the biological graft in the vaginal location. Higgins studied the behavior of PP mesh at the vaginal level in relation to estrogenic levels of a rabbit, demostrating 18% erosion rate in hypoestrogenic group.
Therefore, these latter results show that the rabbit model mimics what is actually observed in humans: graft materials behave differently when implanted in the abdominal wall (i.e., for hernia repair) or in the vaginal submucosa (i.e., for pelvic reconstructive surgery)50,51. More extrusion of PP was observed in the vaginal location, whereas more degradation of the hADM was observed in the same location. Higher extrusion suggests a greater inflammatory response after PP implants; while high degradation of hADM suggests better biocompatibility but questions the long-term efficacy for pelvic surgery. The rabbit model allows the study of potential reasons that lead to these differences. Further analysis based on the inflammatory response to different materials in different locations observed in the present study will follow in the future to enable a better understanding of the whole process and to help guiding the development of biomaterials to be used in a human clinical scenario.
The main limitation of the project is the translation of the results from an animal model to a human situation. In this specific case hADM is a heterologous matrix to the rabbit, since is prepared from human material; therefore studies are needed to verify cross-species effects.
None withstanding this is the first experimental model approximation, subsequent clinical studies in women with this hADM will be necessary to verify the results obtained.
Conclusions
The NZW rabbit is a good model for assessing materials to be used as grafts for pelvic reconstructive surgery and vaginal surgery. The hADM is associated with fewer clinical complications, as well as better macroscopic tissue integration, compared to PP mesh. Additional research is needed to investigate the long-term safety and efficacy of hADM used in women for pelvic reconstructive surgery.
References
Abrams, A. et al. Evaluation and treatment of urinary incontinence, pelvic organ prolapse, and faecal incontinence. Report of the International Scientific Committee. Neurourol Urodyn 37, 2271–2272. https://doi.org/10.1002/nau.23551 (2018).
Unger, C. A. & Barber, M. D. Vaginal mesh in pelvic reconstructive surgery: controversies, current use, and complications. Clin Obstet Gynecol 58(4), 740–753. https://doi.org/10.1097/GRF.0000000000000148 (2015).
Vaginal mesh: high vigilance restriction period: Immediate action required, all cases should be postponed if it is clinically safe to do so. https://www.rcog.org.uk/globalassets/documents/guidelines/safety-alerts/mesh-letter-to-acute-ceos-mds-july-2018.pdf.
FDA takes action to protect women’s health, orders manufacturers of surgical mesh intended for transvaginal repair of pelvic organ prolapse to stop selling all devices. https://www.fda.gov/news-events/press-announcements/fda-takes-action-protect-womens-health-orders-manufacturers-surgical-mesh-intended-transvaginal
Badylak, S. F., Freytes, D. O. & Gilbert, T. W. Reprint of: extracellular matrix as a biological scaffold material: structure and function. Acta Biomater 23(Suppl), S17-26. https://doi.org/10.1016/j.actbio.2015.07.016 (2015).
Nieto-Nicolau, N. et al. Effective decellularization of human nerve matrix for regenerative medicine with a novel protocol. Cell Tissue Res https://doi.org/10.1007/s00441-020-03317-3 (2021).
Bondioli, M. et al. Development and evaluation of a decellularized membrane from human dermis. J Tissue Eng Regen Med 8(4), 325–36. https://doi.org/10.1002/term.1530 (2014).
Juhasz, I. et al. Long-term followup of dermal substitution with acellular dermal implant in burns and postburn scar corrections. Dermatol Res Pract https://doi.org/10.1155/2010/210150 (2010).
Weichman, K. E. et al. The use of acellular dermal matrix in immediate two-stage tissue expander breast reconstruction. Plast Reconstr Surg 129(5), 1049–1058. https://doi.org/10.1097/PRS.0b013e31824a2acb (2012).
Salzberg, C. A., Ashikari, A. Y., Koch, R. M. & Chabner-Thompson, E. An 8-year experience of direct-to-implant immediate breast reconstruction using human acellular dermal matrix (AlloDerm). Plast Reconstr Surg 127(2), 514–524. https://doi.org/10.1097/PRS.0b013e318200a961 (2011).
Guo, X., Mu, D. & Gao, F. Efficacy and safety of acellular dermal matrix in diabetic foot ulcer treatment: a systematic review and meta-analysis. Int J Surg 40, 1–7. https://doi.org/10.1016/j.ijsu.2017.02.008 (2017).
Silverman, R. P., Li, E. N., Holton, L. H. III., Sawan, K. T. & Goldberg, N. H. Ventral hernia repair using allogenic acellular dermal matrix in a swine model. Hernia 8(4), 336–342. https://doi.org/10.1007/s10029-004-0241-6 (2004).
Griffey, S., Schwade, N. D. & Wright, C. G. Particulate dermal matrix as an injectable soft tissue replacement material. J Biomed Mater Res 58(1), 10–15. https://doi.org/10.1002/1097-4636(2001)58:1%3c10::aid-jbm20%3e3.0.co;2-e (2001).
Merriman, A. L. & Kennelly, M. J. Biologic grafts for use in pelvic organ prolapse surgery: a contemporary review. Curr Urol Rep 21(12), 52. https://doi.org/10.1007/s11934-020-01013-x (2020).
Slack M, Ostergard D, Cervigni M, Deprest J. A standardized description of graft-containing meshes and recommended steps before the introduction of medical devices for prolapse surgery. Consensus of the 2nd IUGA Grafts Roundtable: optimizing safety and appropriateness of graft use in transvaginal pelvic reconstructive surgery. Int Urogynecol J. 2012;23 Suppl 1:S15–26. https://doi.org/10.1007/s00192-012-1678-2
Abramowitch, S. D., Feola, A., Jallah, Z. & Moalli, P. A. Tissue mechanics, animal models, and pelvic organ prolapse: a review. Eur J Obstet Gynecol Reprod Biol 144(Suppl 1), S146–S158. https://doi.org/10.1016/j.ejogrb.2009.02.022 (2009).
Couri, B. M. et al. Animal models of female pelvic organ prolapse: lessons learned. Expert Rev Obstetr Gynecol 7(3), 249–260. https://doi.org/10.1586/eog.12.24 (2012).
Mackova, K., Da Cunha, M. G. M. C. M., Krofta, L., Albersen, M. & Deprest, J. The importance of developing relevant animal models to assess existing and new materials. Curr Opin Urol 29(4), 400–406. https://doi.org/10.1097/MOU.0000000000000625 (2019).
Martínez-Gómez, M., Lucio, R. A., Carro, M., Pacheco, P. & Hudson, R. Striated muscles and scent glands associated with the vaginal tract of the rabbit. Anat Rec. 247(4), 486–495. https://doi.org/10.1002/(SICI)1097-0185(199704)247:4%3c486::AID-AR7%3e3.0.CO;2-P (1997).
McKenna, K. E. & Nadelhaft, I. The organization of the pudendal nerve in the male and female rat. J Comp Neurol 248(4), 532–549. https://doi.org/10.1002/cne.902480406 (1986).
Dora, C. D., Dimarco, D. S., Zobitz, M. E. & Elliott, D. S. Time dependent variations in biomechanical properties of cadaveric fascia, porcine dermis, porcine small intestine submucosa, polypropylene mesh and autologous fascia in the rabbit model: implications for sling surgery. J Urol 171(5), 1970–1973. https://doi.org/10.1097/01.ju.0000121377.61788.ad (2004).
Huffaker, R. K. et al. Histologic response of porcine collagen-coated and uncoated polypropylene grafts in a rabbit vagina model. Am J Obstet Gynecol 198(5), 582.e1-582.e7. https://doi.org/10.1016/j.ajog.2007.12.029 (2008).
Harrell, A. G. et al. Prospective histologic evaluation of intra-abdominal prosthetics four months after implantation in a rabbit model. Surg Endosc 21(7), 1170–1174. https://doi.org/10.1007/s00464-006-9147-y (2007).
Krambeck, A. E. et al. Time-dependent variations in inflammation and scar formation of six different pubovaginal sling materials in the rabbit model. Urology 67(5), 1105–1110. https://doi.org/10.1016/j.urology.2005.11.036 (2006).
Hilger, W. S. et al. Histological and biomechanical evaluation of implanted graft materials in a rabbit vaginal and abdominal model. Am J Obstet Gynecol 195(6), 1826–1831. https://doi.org/10.1016/j.ajog.2006.07.006 (2006).
Pierce, L. M. et al. Biomechanical properties of synthetic and biologic graft materials following long-term implantation in the rabbit abdomen and vagina. Am J Obstet Gynecol 200(5), 549.e1-549.e5. https://doi.org/10.1016/j.ajog.2008.12.041 (2009).
Pierce, L. M. et al. Long-term histologic response to synthetic and biologic graft materials implanted in the vagina and abdomen of a rabbit model. Am J Obstet Gynecol. 200(5), 546.e1-546.e5. https://doi.org/10.1016/j.ajog.2008.12.040 (2009).
Claerhout, F. et al. Fate of collagen-based implants used in pelvic floor surgery: a 2-year follow-up study in a rabbit model. Am J Obstet Gynecol 198(1), 94.e1-94.e9. https://doi.org/10.1016/j.ajog.2007.05.032 (2008).
Endo, M. et al. Mesh contraction: in vivo documentation of changes in apparent surface area utilizing meshes visible on magnetic resonance imaging in the rabbit abdominal wall model. Int Urogynecol J 25(6), 737–743. https://doi.org/10.1007/s00192-013-2293-6 (2014).
Fan, X. et al. Histological response to and immunogenicity of different material patches implanted in rabbit abdominal walls. Biomed Tech 58(4), 323–331. https://doi.org/10.1515/bmt-2012-0112 (2013).
Jangö, H. Tissue-engineering as an adjunct to pelvic reconstructive surgery. Dan Med J 64(8), B5378 (2017).
Rice, R. D. et al. Comparison of surgisis®, alloderm®, and vicryl woven mesh® grafts for abdominal wall defect repair in an animal model. Aesthetic Plast Surg 34(3), 290–296. https://doi.org/10.1007/s00266-009-9449-2 (2010).
Zheng, F. et al. Host response after reconstruction of abdominal wall defects with porcine dermal collagen in a rat model. Am J Obstet Gynecol 191(6), 1961–1970. https://doi.org/10.1016/j.ajog.2004.01.091 (2004).
Zheng, F., Verbeken, E., De Ridder, D. & Deprest, J. Improved surgical outcome by modification of porcine dermal collagen implant in abdominal wall reconstruction in rats. Neurourol Urodyn 24(4), 362–368. https://doi.org/10.1002/nau.20148 (2005).
Hympanova, L. et al. Physiologic musculofascial compliance following reinforcement with electrospun polycaprolactone–ureidopyrimidinone mesh in a rat model. J Mech Behav Biomed Mater 74, 349–357. https://doi.org/10.1016/j.jmbbm.2017.06.032 (2017).
Junge, K., Klinge, U., Rosch, R., Klosterhalfen, B. & Schumpelick, V. Functional and morphologic properties of a modified mesh for inguinal hernia repair. World J Surg 26(12), 1472–1480. https://doi.org/10.1007/s00268-002-6444-z (2002).
Junge, K. et al. Influence of polyglecaprone 25 (Monocryl) supplementation on the biocompatibility of a polypropylene mesh for hernia repair. Hernia 9(3), 212–217. https://doi.org/10.1007/s10029-004-0315-5 (2005).
Kim, H. L., LaBarbera, M. C., Patel, R. V., Cromie, W. J. & Bales, G. T. Comparison of the durability of cadaveric and autologous fascia using an in vivo model. Urology 58(5), 800–804. https://doi.org/10.1016/S0090-4295(01)01315-2 (2001).
Konstantinovic, M. L. et al. Biomechanical findings in rats undergoing fascial reconstruction with graft materials suggested as an alternative to polypropylene. Neurourol Urodyn 29(3), 488–493. https://doi.org/10.1002/nau.20755 (2010).
Ozog, Y. et al. Experimental comparison of abdominal wall repair using different methods of enhancement by small intestinal submucosa graft. Int Urogynecol J 20(4), 435–441. https://doi.org/10.1007/s00192-008-0793-6 (2009).
DeGeorge, B. R. Jr. et al. Advanced imaging techniques for investigation of acellular dermal matrix biointegration. Plast Reconstr Surg 139(2), 395–405. https://doi.org/10.1097/PRS.0000000000002992 (2017).
Cottler, P. S. et al. Fenestration improves acellular dermal matrix biointegration: an investigation of revascularization with photoacoustic microscopy. Plast Reconstr Surg 143(4), 971–981. https://doi.org/10.1097/PRS.0000000000005410 (2019).
Mukherjee, S. et al. Electrospun nanofiber meshes with endometrial MSCs modulate foreign body response by increased angiogenesis, matrix synthesis, and anti-inflammatory gene expression in mice: implication in pelvic floor. Front Pharmacol. 24(11), 353. https://doi.org/10.3389/fphar.2020.00353 (2020).
Endo, M. et al. Cross-linked xenogenic collagen implantation in the sheep model for vaginal surgery. Gynecol Surg 12(2), 113–122. https://doi.org/10.1007/s10397-015-0883-7 (2015).
Tayrac, R., Alves, A. & Thérin, M. Collagen-coated vs noncoated low-weight polypropylene meshes in a sheep model for vaginal surgery. A pilot study. Int Urogynecol J 18(5), 513–520. https://doi.org/10.1007/s00192-006-0176-9 (2007).
Feola, A. et al. Host reaction to vaginally inserted collagen containing polypropylene implants in sheep. Am J Obstet Gynecol 212(4), 474.e1-474.e8. https://doi.org/10.1016/j.ajog.2014.11.008 (2015).
Kolb, C. M., Pierce, L. M. & Roofe, S. B. Biocompatibility comparison of novel soft tissue implants vs commonly used biomaterials in a pig model. Otolaryngol Head Neck Surg (US) 147(3), 456–461. https://doi.org/10.1177/0194599812450855 (2012).
Probst, M., Piechota, H. J., Dahiya, R. & Tanagho, E. A. Homologous bladder augmentation in dog with the bladder acellular matrix graft. BJU Int 85(3), 362–371. https://doi.org/10.1046/j.1464-410X.2000.00442.x (2000).
Higgins, E. W. et al. Effect of estrogen replacement on the histologic response to polypropylene mesh implanted in the rabbit vagina model. Am J Obstet Gynecol 201(5), 505.e1–9. https://doi.org/10.1016/j.ajog.2009.05.050 (2009).
Mahon J., Varley D., Glanville J. Summaries of the safety/adverse effects of vaginal tapes/slings/meshes for stress urinary incontinence and prolapse. Medicines and Healthcare products Regulatory Agency. 2012.
Chen, D. C. & Morrison, J. State of the art: open mesh-based inguinal hernia repair. Hernia 23(3), 485–492. https://doi.org/10.1007/s10029-019-01983-z (2019).
Author information
Authors and Affiliations
Contributions
M.P.: project development, data collection, manuscript writing. L.C.: project development, data collection, manuscript writing. C.C.-S.: project development, data collection, manuscript writing. M.L.P.: project development, data collection, manuscript writing. E.M.N.: project development, data collection, manuscript writing. O.J.-B.: project development, data collection, manuscript writing. L.A.DeL.: data collection, manuscript writing. P.L.-C.: project development, manuscript writing. A.V.S.: project development, manuscript writing. L.B.: supervision. O.P.R.: project development, data collection, manuscript writing.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Peró, M., Casani, L., Castells-Sala, C. et al. Rabbit as an animal model for the study of biological grafts in pelvic floor dysfunctions. Sci Rep 11, 10545 (2021). https://doi.org/10.1038/s41598-021-89698-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-021-89698-z
This article is cited by
-
The use of animal models in preclinical investigations for the development of a surgical mesh for pelvic organ prolapse
International Urogynecology Journal (2024)
-
Comparison of a human acellular dermal matrix and a polypropylene mesh for pelvic floor reconstruction: a randomized trial study in a rabbit model
Scientific Reports (2022)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
