
Abstract
Reports from Arabian Gulf countries have demonstrated emergence of novel methicillin resistant Staphylococcus aureus (MRSA) strains. To address the lack of data from the United Arab Emirates (UAE), genetic characterisation of MRSA identified between December 2017 and August 2019 was conducted using DNA microarray-based assays. The 625 MRSA isolates studied were grouped into 23 clonal complexes (CCs) and assigned to 103 strains. CC5, CC6, CC22 and CC30 represented 54.2% (n/N = 339/625) of isolates with other common CCs being CC1, CC8, CC772, CC361, CC80, CC88. Emergence of CC398 MRSA, CC5-MRSA-IV Sri Lanka Clone and ST5/ST225-MRSA-II, Rhine-Hesse EMRSA/New York-Japan Clone in our setting was detected. Variants of pandemic CC8-MRSA-[IVa + ACME I] (PVL+) USA300 were detected and majority of CC772 strains were CC772-MRSA-V (PVL+), “Bengal- Bay Clone”. Novel MRSA strains identified include CC5-MRSA-V (edinA+), CC5-MRSA-[VT + fusC], CC5-MRSA-IVa (tst1+), CC5-MRSA-[V/VT + cas + fusC + ccrA/B-1], CC8-MRSA-V/VT, CC22-MRSA-[IV + fusC + ccrAA/(C)], CC45-MRSA-[IV + fusC + tir], CC80-MRSA-IVa, CC121-MRSA-V/VT, CC152-MRSA-[V + fusC] (PVL+). Although several strains harboured SCC-borne fusidic acid resistance (fusC) (n = 181), erythromycin/clindamycin resistance (ermC) (n = 132) and gentamicin resistance (aacA-aphD) (n = 179) genes, none harboured vancomycin resistance genes while mupirocin resistance gene mupR (n = 2) and cfr gene (n = 1) were rare. An extensive MRSA repertoire including CCs previously unreported in the region and novel strains which probably arose locally suggest an evolving MRSA landscape.
Similar content being viewed by others


Introduction
Methicillin resistant Staphylococcus aureus (MRSA) is an important cause of nosocomial infections worldwide and is associated with significant patient morbidity, mortality and healthcare costs. The epidemiology of MRSA has been dynamic and with an evolution towards increasing predominance of community associated MRSA lineages (CA-MRSA) as agents of hospital acquired MRSA (HA-MRSA) infections1,2. In recent years, emerging data on the molecular characterisation of S. aureus isolates in the hospital and community setting in countries of the Arabian Gulf region has contributed to changing our understanding of the diversity of isolates present3,4,5,6,7,8,9. In accordance with reports from other parts of the world, community associated MRSA (CA-MRSA) lineages have overtaken HA-MRSA lineages as aetiological agents also of nosocomial infections. Interestingly, MRSA isolates circulating in the region represent a wide clonal diversity3,8,10,11,12. Furthermore, emergence of novel and variant MRSA strains including those with novel SCCmec elements or with complex elements that include mecA as well as a gene associated with fusidic acid resistance (fusC) continue to be reported3,8,10.
Although MRSA contributes to the burden of S. aureus infections in the United Arab Emirates (UAE), there remains a paucity of data on the molecular characterization of circulating strains. The UAE is a global tourist hub and home to a large expatriate population including those from regions from where there are hardly any data on MRSA prevalence and population structure. With this dynamic population, it is plausible that a diversity of MRSA clones can be found that includes highly transmissible pandemic clones as well as local strains from different regions from which tourists and expatriates might come to the UAE. Therefore, this study was carried out to determine the genotypes of MRSA isolates in the UAE and to differentiate closely related strains using a high-resolution typing method.
Results
CC diversity, virulence and antibiotic resistance genes
A total of 625 isolates obtained from wound/pus swabs (n = 459), blood cultures (n = 95), respiratory sites (endotracheal aspirates/sputum) (n = 50) and urine (n = 21) were included in the study. Based on DNA microarray analysis, these 625 MRSA isolates were grouped into 23 clonal complexes (CCs) which were assigned to 102 strains (Table 1) with “strains” being defined based on their CC affiliation, toxin gene carriage and SCCmec type (see Supplementary Table S1 online for details of strain assignment). The CCs were identified across study sites and there was no clustering observed of any specific CC based on study site or type of clinical specimen. Four predominant CCs accounted for 54.2% (n/N = 339/625) of isolates. These were CC30 (n = 91; 14.6%), CC5 (n = 89; 14.2%), CC22 (n = 82; 13.1%) and CC6 (n = 77; 12.3%) (Table 1). Other commonly identified CCs were CC1 (n = 48), CC8 (n = 40), CC772 (n = 36), CC361 (n = 35), CC80 (n = 27) and CC88 (n = 19). A majority of the strains belonged to CA-MRSA lineages harbouring SCCmec types IV and V (n/N = 610/625; 97.6%), (Supplementary Table S1 online). There was concordance between MRSA phenotypic and genotypic identification (data not shown).
We detected isolates harbouring SCC-borne fusidic acid resistance (fusC) gene (n = 181), erythromycin/clindamycin resistance (ermC) gene (n = 132), and bifunctional enzyme gentamicin resistance (aacA-aphD) (n = 179). In addition, 25 isolates carried the fusidic acid resistance gene fusB (also known as far1). Carriage of the mupirocin resistance gene mupR (n = 2) and 23S rRNA methyltransferase cfr gene (n = 1) was rare while none of our strains carried vancomycin / teicoplanin resistance genes (vanA, vanB, vanZ). The Panton Valentine leukocidin (pvl) genes were present in 49% of all isolates studied while 13.8% were positive for the toxic shock syndrome (tst-1) gene. The prevalence rates of the antibiotic resistance and virulence genes are shown in Tables 2 and Table 3 respectively.
Emerging clonal complexes
Our findings document the first identification of CC398 MRSA in the Arabian Gulf region. The detection of pvl genes and SCCmec typing using a second array revealed it to belong to the Asian, human adapted lineage rather than to the European livestock-associated one. Among CC5, we report the emergence of CC5-MRSA-IV Sri Lanka Clone and a second identification of ST5/ST225-MRSA-II, Rhine-Hesse EMRSA/New York-Japan Clone in the region (Supplementary Table S1 online). The CC5-MRSA-IV, Sri Lanka Clone is a CC5-MRSA carrying a SCCmec IVc element and pvl genes as well as, variably, the enterotoxin genes sed, sej and ser. In CC8, different variants of the pandemic CC8-MRSA-[IVa + ACME I] (PVL+) USA300 strain were detected including one that lost arc genes and speG while retaining opp and copA2-SCC (copper resistance), as well as putative PVL-deletion mutants (Supplementary Table S1 online). For the first time in our region, we report identification of the ACME-negative/PVL-positive CC8-MRSA-[SCCmec IVc + Hg], which is a strain frequently described from Spain and Latin America (Supplementary Table S1 online). Another emerging strain was CC22-MRSA-IV harbouring pvl and tst1 genes. A majority of the CC772 MRSA was assigned to CC772-MRSA-V (PVL+), "Bengal Bay Clone" while some of the CC772 isolates presented with other, unusual SCCmec variants.
Novel variant MRSA strains
We identified novel variant MRSA strains from 9 CCs, namely:
- CC5:
-
Four novel variant strains were identified, three of which carried SCCmec type V. All the strains carried regulatory and capsular genes agrII and cap5 respectively. Although all harboured the egc cluster enterotoxin genes, the edinA and tst-1 genes were found in single strains respectively. The CC5-MRSA-IVa (tst1+) was the only one with SCCmec type IV and it uniquely harboured SCCmec IVa instead of usual IVc. Both CC5-MRSA-[VT + fusC] and CC5-MRSA-[V/VT + cas + fusC + ccrA/B-1] carried the fusC gene. The CC5-MRSA-[VT + fusC] with SCCmec VT + fusC was identified as an unknown CC5/72 strain. A novel SCCmec element was exhibited by CC5-MRSA-[V/VT + cas + fusC + ccrA/B-1] which also carried the highest repertoire of antibiotic resistance genes among the novel strains (Table 3).
- CC8:
-
The novel variant strain in this CC was the CC8-MRSA-V/VT which uniquely harboured a SCCmec V sub-type (as in WIS; GenBank AB121219.1) and harboured the cassette chromosome recombinase genes ccrC on the SCCmec element. No toxin associated genes were identified in this strain.
- CC22:
-
The CC22-MRSA-[IV + fusC + ccrAA/(C)] had a new SCCmec element characterised by carriage of SCCmec type IV with ccrAA/C recombinase genes and fusC gene. In addition to egc cluster which is usually found in CC22 MRSA, this strain also harboured tst1 gene.
- CC45:
-
The CC45-MRSA-[IV + fusC + tir] harboured the combination of fusC and tirS genes on the SCCmec element making is a novel CC45 variant strain.
- CC80:
-
CC80-MRSA nearly always harbour PVL and SCCmec IVc while lacking enterotoxin genes. However, this novel variant had SCCmec IVa, harboured enterotoxin genes (seb, sek, seq) and was negative for pvl genes.
- CC121:
-
Subtyping of the CC121 strains revealed the presence of a variant CC121-MRSA- VT strain with the SCCmec VT (GR1).
- CC152:
-
The CC152-MRSA-[V + fusC] (PVL+) is the only novel variant strain harbouring the pvl genes. The carriage of SCC [mec V + fusC] is novel in this CC.
- CC361:
-
One CC361 strain uniquely carried an SCCmec V / cas composite element. It also harboured tst1 gene and a complement of enterotoxin genes (sec, sel, egc cluster).
- CC1153:
-
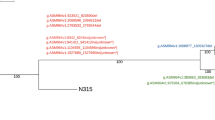
Two PVL-positive CC1153-MRSA isolates were observed that presented with a mec complex B, ccrA/B1 recombinase genes and the fusC gene. Table 4 shows the genetic characterization of the novel strains.
Table 4 Characterization of novel methicillin-resistant Staphylococcus aureus strains.
Discussion
In recent years, emerging data globally and specifically in the Arabian Gulf region, have shown an evolving MRSA epidemiology with a shift to predominance of CA-MRSA lineages in nosocomial infections and an emergence of novel strains leading to an increased biological diversity of MRSA strains as well as to a greater diversity of SCCmec elements and variants thereof. In the UAE, MRSA contributes to the burden of infection and 30% of MRSA isolates identified at a tertiary care facility between 2011 and 2012 were CA-MRSA lineages13. Indeed, Sonnevend et al. also reported a trend of increasing CA-MRSA lineages between 2003 and 2008 at another tertiary care facility in the UAE14. However, data on the molecular characterization and strain assignments of circulating MRSA in the UAE are lacking. With the rapidly evolving changes reported in neighbouring countries and the dynamic population of the UAE, this study provides a much-needed snapshot of the genetic make-up of MRSA strains circulating in the UAE. Our findings demonstrate that an extensive MRSA repertoire of predominantly CA-MRSA lineage including CCs previously unreported in the region, plus rare and novel strains are present in the UAE. While the predominance of CC5, CC6, CC22 and CC30 is in accordance with reports from other countries in the region, identification of several pandemic MRSA strains and their variants such as CC8-MRSA-[IVa + ACME I] (PVL+), USA300, CC22-MRSA-IV UK-EMRSA-15/Barnim EMRSA; CC30-MRSA-IV (PVL+), Southwest Pacific Clone and the HA-MRSA lineage CC239-MRSA-[mec III + Cd/Hg + ccrC] is of concern in light of enhanced virulence, fitness and survivability of these strains. Furthermore, the first identification of CC398 MRSA heralds ominously the appearance of yet another previously unreported clonal complex in our region. The CC398 MRSA identified is the PVL-positive human variant of MRSA CC398 which is believed to have originated in South East Asia and is a frequent cause of infections in China and Vietnam15,16,17. In Europe, links to South East Asia were demonstrated in cases of infections and outbreaks associated with this CC398-MRSA strain15,18. It is therefore highly likely that this strain was introduced to the UAE from South East Asia or even possibly via Europe.
CC5-MRSA are globally common19 with CC5-MRSA-IV (PVL + /edinA+), WA MRSA-121, CC5-MRSA-[IV + fus + ccrAB], “Maltese Clone” and CC5-MRSA-IV (tst1+), being the prevalent strains in the Arabian Gulf region3,4,6,20. Recently, the emergence of CC5-MRSA-VI strain including a novel variant which harboured the Staphylococcal TIR-protein binding protein gene (tirS) as additional payload on SCCmec was reported in Saudi Arabia 8. Identification of eight CC5-MRSA-[VI + fusC] including two with tirS in the current study suggests dissemination of this strain in the region. It has been postulated that the tirS gene confers enhanced bacterial survival and because it is located on a mobile genetic element in S. aureus, in this case an SCC element together with fusC, horizontal gene transfer among MRSA strains is likely8,21. In addition to the CC5-MRSA we also identified two other strains with tirS namely a novel CC45 variant, CC45-MRSA-[IV + fusC + tir], and CC1-MRSA [VT + fusC + tir + ccrAB1]. These findings are supportive of the notion for on-going horizontal gene transfer among MRSA strains in our setting.
The occurrence of antibiotic resistance and virulence genes on MRSA SCCmec/fus genetic elements is suggestive of novel adaptive mechanisms22. A high consumption of fusidic acid in the population confers a selective advantage for the emergence and proliferation of strains carrying the fusC gene23. When fusC and mecA co-exist on the SCC element, fusidic acid use could promote MRSA in the community while beta-lactam use promotes fusidic acid resistance in the hospital. Hence, MRSA strains with SCCmec + SCCfus composite elements have a selective advantage in both the hospital and community settings. The high prevalence of MRSA strains with fusC gene plus presence of CC80 MRSA (which usually harbour fusB) suggests on-going community misuse of fusidic acid as a driving factor for MRSA evolution in our setting. Therefore, future emergence of MRSA strains with increased bacterial fitness, resistance and virulence is possible, hence continued surveillance for early detection and responsible use of antibiotics is necessary.
Recently reported phylogenetic analysis of CC5 PVL-positive MRSA from four continents showed geographical clustering with the identification of the ST5-PVL-positive MRSA-IVc Sri Lanka clone24. Wider geographical spread of this clone was demonstrable with its identification in England and Australia where demonstrable links to Sri Lanka were not consistently established24. Our study documents the first report of CC5-MRSA-IV Sri Lanka Clone with two distinct variants based on carriage or absence of enterotoxin genes (sed, sej, ser) in our setting. The detection of CC5-MRSA-IV Sri Lanka Clone also underscores the need for continued surveillance to keep track of introduction of new MRSA strains into the population. While it is likely that this strain was introduced rather than arising de novo in the UAE, we were unable to establish direct travel links with Sri Lanka probably because this information was sought retrospectively and patients might have acquired the strains through contact with healthcare workers or carriers with epidemiological links. The ST5/ST225-MRSA-II, Rhine-Hesse EMRSA/New York-Japan Clone identified in this study is a HA-MRSA lineage pandemic strain which has been reported in Europe, Asia, North America and Australia19,25. It has previously been identified in Kuwait and our findings demonstrate the second report in our region. Although variants of this MRSA strain harbouring arginine catabolic mobile element (ACME) have been reported, this was not evident in the strain found in this study25. Further identification of novel strains within CC5 including edinA + variant, and strains with new SCCmec elements including SCC [VT + fusC] and SCC-[V/VT + cas + fusC + ccrA/B-1] are suggestive of ongoing genetic modification and recombination, among CC5-MRSA strains circulating in the UAE, or of importation from yet unidentified sources.
CC22 is a widespread clonal group which is prevalent in this region. Using high-resolution typing methods with SCCmec subtyping we had previously identified the regional presence of six distinct C22-MRSA-IV strains11 and recently an additional novel variant with SCCmec V/VT + fusC and pvl was reported from Saudi Arabia8. In this study, these previously reported strains as well as the European pandemic strain CC22-MRSA-IV (UK-EMRSA-15/Barnim EMRSA) were detected, indicative of strong links to Middle East, India and Europe for the evolution of CC22-MRSA in the UAE. In addition, our findings reflect on-going expansion of the diversity of CC22 MRSA strains with the identification of the previously undescribed CC22-MRSA-[IV + fusC + ccrAA/(C) which harboured a novel SCCmec element.
The CC772-MRSA-V (PVL+), Bengal Bay Clone is believed to have emerged in the Indian subcontinent from the same lineage as the widespread CC1 and CC5 strains 26,27,28. In a recent report from Pakistan, a majority of the characterised MRSA strains belonged to this CC29. In Western Europe, infections with CC772-MRSA are commonly associated with previous travel or patient´s ethnic origin from the Indian sub-continent 26. Having been previously reported in Saudi Arabia, Oman and Kuwait, its identification in the UAE is not surprising giving the dynamic population movement with the Indian subcontinent4,9,30.
MRSA CC121, CC152, CC361, and CC1153 are considered to be emerging in our region as variant strains belonging to these CCs are continually reported. It is therefore not surprising that other novel variant strains identified in this study belonged to these CCs 3,8. CC152-MRSA-V has been reported from Germany, Australia, Sweden, Switzerland, the Balkans, Saudi Arabia and Kuwait3,8,19,31. In accordance with reported literature, the CC152-MRSA-V identified in this study harbour the pvl and edinB genes, and lacked enterotoxin genes19. This strain carried erythromycin/clindamycin resistance ermC gene which was not present in previously described strains3,8.
The first identification of CC361 in Saudi Arabia was recently reported with detection of variant strains similar to those previously described in Kuwait indicative of regional spread3,8. Although CC361-MRSA had previously been described as a rare strain in the UAE19, and only one CC361-MRSA-[V/VT + fusC] was found as nasal colonizer in a recent study from UAE dental clinics32, the current findings suggest a wider occurrence of this CC. Similar to our findings, a recent report from Kuwait describing 102 novel MRSA variants identified 32 as CC361 strains3. With up to 5% (n/N = 35/625) of our isolates belonging to CC361-MRSA inclusive of a novel strain with SCCmec V / cas composite element, it appears that we can no longer consider this as a rare MRSA lineage in our setting.
In conclusion, an extensive MRSA repertoire which includes CCs previously unreported in the region, plus pandemic, rare and novel variant strains are present in the UAE. Some strains detected occur in other countries, so a travel connection is possible. Others which have not been described elsewhere, probably evolved within the region. The lack of documentation of travel history for our patients is a limitation of this study as such information would have been helpful in mapping the travel connections. However, in a population as diverse as the UAE, it should be noted that importation of a strain from abroad could have multiple sources and prior travel by the patient represents only one piece of the puzzle. An on-going, sustained transmission of at least some of the “imported” clones might have already started within the UAE population and affecting individuals who previously did not travel. Nevertheless, our findings provide the first detailed information on the genotyping of MRSA isolates in the UAE, providing important baseline data for future surveillance work and whole genome sequencing of novel strains to help understand MRSA evolution and epidemiology in the UAE.
Materials and methods
Specimen collection and bacterial strains: MRSA isolates were identified between December 2017 and August 2019 at four diagnostic microbiology laboratories associated with secondary and tertiary care facilities, across three Emirates (Dubai, Abu Dhabi and Umm Al Quwain) in the UAE, with no routine inter-hospital transfer of patients. Apart from Abu Dhabi isolates which were obtained between December 2017 and August 2018, those from other Emirates were identified between December 2017 and August 2019. Only consecutive MRSA isolates associated with clinical infection were included with only one isolate per patient. There was no restriction on patient age for inclusion of isolates. However, all isolates obtained from specimens (nasal/axillary swabs) collected for MRSA screening were excluded. Identification of S. aureus and confirmation of methicillin resistance were performed using the Vitek automated platform (bioMérieux, Marcy-l'Étoile, France) in the diagnostic laboratory in accordance with manufacturer’s instructions and Clinical and Laboratory Standards Institute guidelines33. Ethical approval was obtained from Mohammed Bin Rashid University, Dubai Scientific Research and Mediclinic Hospitals ethics committees (MBRU-IRB-2018–019; DSREC-05/2018_11 and CR/2018/42). As the study involved use of MRSA isolates already identified as part of routine diagnostic investigation, waiver of informed consent was granted by the above-mentioned ethics committees. All methods in the study were carried out in accordance with relevant guidelines and regulations. All MRSA isolates were stored at -80 °C pending molecular characterisation.
Molecular characterisation of isolates was carried out using the StaphyType DNA microarray (Abbott [Alere Technologies GmbH], Jena, Germany). The previously described probes, primers, and procedures were used for the detection of species markers, virulence and resistance genes as well as for SCCmec subtyping19,34,35. Microarray images were taken and analysed using the dedicated reader and software (Alere Technologies). The analysis of presence or absence of target gene, assignment to clonal complex, sequence type and strains as well as SCCmec type was carried out as previously described19,34,35. Selected isolates were further characterised using a second array that facilitated assignment to SCCmec subtypes35.
Data availability
Data generated or analysed during this study are included in this published article.
References
Deurenberg, R. H. et al. The molecular evolution of methicillin-resistant Staphylococcus aureus. Clin. Microbiol. Infect. 13, 222–235. https://doi.org/10.1111/j.1469-0691.2006.01573.x (2007).
Turner, N. A. et al. Methicillin-resistant Staphylococcus aureus: an overview of basic and clinical research. Nat. Rev. Microbiol. 17, 203–218. https://doi.org/10.1038/s41579-018-0147-4 (2019).
Boswihi, S. S. et al. Emerging variants of methicillin-resistant Staphylococcus aureus genotypes in Kuwait hospitals. PLoS ONE 13, e0195933. https://doi.org/10.1371/journal.pone.0195933 (2018).
Monecke, S. et al. Characterisation of MRSA strains isolated from patients in a hospital in Riyadh, Kingdom of Saudi Arabi. BMC Microbiol. 12, 146. https://doi.org/10.1186/1471-2180-12-146 (2012).
Sarkar, A. et al. Antimicrobial resistance and virulence markers in methicillin sensitive Staphylococcus aureus isolates associated with nasal colonization. Microb. Pathog. 93, 8–12. https://doi.org/10.1016/j.micpath.2016.01.008 (2016).
Senok, A., Ehricht, R., Monecke, S., Al-Saedan, R. & Somily, A. Molecular characterization of methicillin-resistant Staphylococcus aureus in nosocomial infections in a tertiary-care facility: emergence of new clonal complexes in Saudi Arabia. New Microbes New Infect. 14, 13–18. https://doi.org/10.1016/j.nmni.2016.07.009 (2016).
Senok, A. et al. Genotyping of Staphylococcus aureus associated with nasal colonization among healthcare workers using DNA microarray. J. Infect. Dev. Ctries 12, 321–325. https://doi.org/10.3855/jidc.10328 (2018).
Senok, A. et al. Emergence of novel methicillin-resistant Staphylococcus aureus strains in a tertiary care facility in Riyadh, Saudi Arabia. Infect. Drug Resist. 12, 2739–2746. https://doi.org/10.2147/IDR.S218870 (2019).
Udo, E. E., Al-Lawati, B. A., Al-Muharmi, Z. & Thukral, S. S. Genotyping of methicillin-resistant Staphylococcus aureus in the Sultan Qaboos University Hospital, Oman reveals the dominance of Panton-Valentine leucocidin-negative ST6-IV/t304 clone. New Microbes New Infect 2, 100–105. https://doi.org/10.1002/nmi2.47 (2014).
Senok, A. et al. Characterisation of a novel SCCmec VI element harbouring fusC in an emerging Staphylococcus aureus strain from the Arabian Gulf region. PLoS ONE 14, e0223985. https://doi.org/10.1371/journal.pone.0223985 (2019).
Senok, A. et al. Diversity of methicillin-resistant Staphylococcus aureus CC22-MRSA-IV from Saudi Arabia and the Gulf region. Int. J. Infect. Dis. 51, 31–35. https://doi.org/10.1016/j.ijid.2016.08.016 (2016).
Senok, A. C. et al. Investigating a rare methicillin-resistant Staphylococcus aureus strain: first description of genome sequencing and molecular characterization of CC15-MRSA. Infect. Drug Resist. 10, 307–315. https://doi.org/10.2147/IDR.S145394 (2017).
Dash, N., Panigrahi, D., Al Zarouni, M., Yassin, F. & Al-Shamsi, M. Incidence of community-acquired methicillin-resistant Staphylococcus aureus carrying Pantone-Valentine leucocidin gene at a referral hospital in United Arab Emirates. APMIS 122, 341–346. https://doi.org/10.1111/apm.12150 (2014).
Sonnevend, A. et al. Change in meticillin-resistant Staphylococcus aureus clones at a tertiary care hospital in the United Arab Emirates over a 5-year period. J. Clin. Pathol. 65, 178–182. https://doi.org/10.1136/jclinpath-2011-200436 (2012).
Moller, J. K. et al. International travel as source of a hospital outbreak with an unusual meticillin-resistant Staphylococcus aureus clonal complex 398, Denmark, 2016. Euro Surveill. 24, 14. https://doi.org/10.2807/1560-7917.ES.2019.24.42.1800680 (2019).
Ngoc Thi, Vu. et al. Population structure of colonizing and invasive Staphylococcus aureus strains in northern Vietnam. J. Med. Microbiol. 65, 298–305. https://doi.org/10.1099/jmm.0.000220 (2016).
Yu, F. et al. Prevalence of Staphylococcus aureus carrying Panton-Valentine leukocidin genes among isolates from hospitalised patients in China. Clin. Microbiol. Infect. 14, 381–384. https://doi.org/10.1111/j.1469-0691.2007.01927.x (2008).
Nurjadi, D. et al. Import of community-associated, methicillin-resistant Staphylococcus aureus to Europe through skin and soft-tissue infection in intercontinental travellers, 2011–2016. Clin. Microbiol. Infect. 25, 739–746. https://doi.org/10.1016/j.cmi.2018.09.023 (2019).
Monecke, S. et al. A field guide to pandemic, epidemic and sporadic clones of methicillin-resistant Staphylococcus aureus. PLoS ONE 6, e17936. https://doi.org/10.1371/journal.pone.0017936 (2011).
El-Mahdy, T. S., El-Ahmady, M. & Goering, R. V. Molecular characterization of methicillin-resistant Staphylococcus aureus isolated over a 2-year period in a Qatari hospital from multinational patients. Clin. Microbiol. Infect. 20, 169–173. https://doi.org/10.1111/1469-0691.12240 (2014).
Askarian, F. et al. A Staphylococcus aureus TIR domain protein virulence factor blocks TLR2-mediated NF-kappaB signaling. J. Innate Immun. 6, 485–498. https://doi.org/10.1159/000357618 (2014).
Ellington, M. J. et al. Emergent and evolving antimicrobial resistance cassettes in community-associated fusidic acid and meticillin-resistant Staphylococcus aureus. Int. J. Antimicrob. Agents 45, 477–484. https://doi.org/10.1016/j.ijantimicag.2015.01.009 (2015).
Williamson, D. A. et al. High usage of topical fusidic acid and rapid clonal expansion of fusidic acid-resistant Staphylococcus aureus: a cautionary tale. Clin. Infect. Dis. 59, 1451–1454. https://doi.org/10.1093/cid/ciu658 (2014).
McTavish, S. M. et al. Genomic and epidemiological evidence of a dominant panton-valentine leucocidin-positive methicillin resistant Staphylococcus aureus lineage in Sri Lanka and presence among isolates from the United Kingdom and Australia. Front. Cell Infect. Microbiol. 9, 123. https://doi.org/10.3389/fcimb.2019.00123 (2019).
Schulte, B., Bierbaum, G., Pohl, K., Goerke, C. & Wolz, C. Diversification of clonal complex 5 methicillin-resistant Staphylococcus aureus strains (Rhine-Hesse clone) within Germany. J. Clin. Microbiol. 51, 212–216. https://doi.org/10.1128/JCM.01967-12 (2013).
Blomfeldt, A. et al. Emerging multidrug-resistant Bengal Bay clone ST772-MRSA-V in Norway: molecular epidemiology 2004–2014. Eur. J. Clin. Microbiol. Infect. Dis. 36, 1911–1921. https://doi.org/10.1007/s10096-017-3014-8 (2017).
Goering, R. V. et al. Molecular epidemiology of methicillin-resistant and methicillin-susceptible Staphylococcus aureus isolates from global clinical trials. J. Clin. Microbiol. 46, 2842–2847. https://doi.org/10.1128/JCM.00521-08 (2008).
Monecke, S. et al. Genome sequencing and molecular characterisation of Staphylococcus aureus ST772-MRSA-V, “Bengal Bay Clone”. BMC Res. Notes 6, 548. https://doi.org/10.1186/1756-0500-6-548 (2013).
Jamil, B. et al. Hospital-acquired methicillin-resistant Staphylococcus aureus (MRSA) from Pakistan: molecular characterisation by microarray technology. Eur. J. Clin. Microbiol. Infect. Dis. 37, 691–700. https://doi.org/10.1007/s10096-017-3161-y (2018).
Boswihi, S. S., Udo, E. E. & Al-Sweih, N. Shifts in the clonal distribution of methicillin-resistant Staphylococcus aureus in Kuwait Hospitals: 1992–2010. PLoS ONE 11, e0162744. https://doi.org/10.1371/journal.pone.0162744 (2016).
Francois, P. et al. Methicillin-resistant Staphylococcus aureus, Geneva, Switzerland, 1993–2005. Emerg. Infect. Dis. 14, 304–307. https://doi.org/10.3201/eid1402.070229 (2008).
Senok, A. et al. Molecular characterization of Staphylococcus aureus isolates associated with nasal colonization and environmental contamination in academic dental clinics. Microb. Drug Resist. https://doi.org/10.1089/mdr.2019.0318 (2020).
Clinical and Laboratory Standards Institute. Performance Standard for Antimicrobial Susceptibility Testing, M100 27th edn. (CLSI, Wayne, 2017).
Monecke, S. et al. Microarray-based genotyping of Staphylococcus aureus isolates from camels. Vet. Microbiol. 150, 309–314. https://doi.org/10.1016/j.vetmic.2011.02.001 (2011).
Monecke, S. et al. Diversity of SCCmec elements in Staphylococcus aureus as observed in South-Eastern Germany. PLoS ONE 11, e0162654. https://doi.org/10.1371/journal.pone.0162654 (2016).
Funding
The project was funded by internal research grant from the College of Medicine, Mohammed Bin Rashid University of Medicine and Health Sciences, UAE (Ref#: MBRU-CM-RG2018-07).
Author information
Authors and Affiliations
Contributions
A.S., R.N., S.M., R.E. conceived and designed the study. H.C., A.N., M.A., S.W., I.R. contributed to sample collection and isolate identification. R.N., D.G., E.M., A.R., carried out the DNA microarrays. A.S., S.M., R.E. contributed to analysis and interpretation of DNA microarray data. All authors contributed to the data interpretation, preparation and critical revision of the manuscript. All authors approved the final manuscript and take responsibility for the published manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Senok, A., Nassar, R., Celiloglu, H. et al. Genotyping of methicillin resistant Staphylococcus aureus from the United Arab Emirates. Sci Rep 10, 18551 (2020). https://doi.org/10.1038/s41598-020-75565-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-020-75565-w
This article is cited by
-
Sequencing a CC239-MRSA-III with a novel composite SCC mec element from Kuwait
European Journal of Clinical Microbiology & Infectious Diseases (2024)
-
Characterisation of S. aureus/MRSA CC1153 and review of mobile genetic elements carrying the fusidic acid resistance gene fusC
Scientific Reports (2021)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
