
Abstract
In this controlled before-after study based on data from the Norwegian Prescription Database, we examine whether starting off-label use of Low Dose Naltrexone (LDN) is followed by changes in the consumption of psychotropic medicines including antiepileptics. Patients that collected LDN for the first time in 2013 (N = 11247) were included and stratified into three groups based on LDN exposure. We compared differences in means of cumulative number of defined daily doses (DDD) as well as changes in the number of users one year before and one year after starting LDN. There was a dose-response association between increasing LDN exposure and reductions in the number of users of antiepileptics, antipsychotics and antidepressants. There were significant difference-in-differences in DDDs between the groups with the lowest and highest LDN exposure of antipsychotics (1.4 DDD, 95% CI 0.4 to 2.3, p = 0.007), and in number of users of antiepileptics (3.1% points, 95% CI 1.6% to 4.6%, p < 0.001), antipsychotics (2.1% points, 95% CI 1.2% to 3%, p < 0.001), and antidepressants (2.8% points, 95% CI 1.1% to 4.4%, p = 0.001). The findings show an association between the initiation of persistent LDN use and reduced consumption of several psychotropic medicines and antiepileptics. Beneficial effects of LDN in the treatment of psychiatric diseases cannot be ruled out.
Similar content being viewed by others

Introduction
Off-label use of low dose naltrexone (LDN), typically <5 mg/day, is by some patients, doctors and researchers believed to have therapeutic effects in several conditions such as autoimmune diseases1 and chronic pain. LDN could be a cheap and safe2 alternative to standard treatments, but the evidence of effect is limited. The main use of naltrexone within psychiatry has so far been as treatment of opioid and alcohol addiction3, but a recent report suggests that LDN may be helpful in other psychiatric conditions4. Some of the beneficial effects in patients with autoimmune diseases have been improvements in quality of life5,6 and improvements in symptoms associated with depression, such as sleep and mood7. In a study on major depressive disorder where the authors randomized 12 patients to naltrexone 1 mg/day or placebo, there were borderline significant improvements in some clinical depression measures4. These results are part of the documentation in a patent application on the use of LDN in depression and other mental health issues8. In a randomized study on Gulf war illness (N = 37), there were improvements in general disability, depression and confusion in users of LDN9. There have been promising results in a small, randomized study in fibromyalgia, a condition where psychiatric symptoms may be prominent6.
A sudden and large increase in LDN consumption in Norway during 201310 has enabled nationwide quasi-experimental register studies on change in medicine use associated to initiation of LDN use. Previously we have demonstrated an association between starting LDN and changes in medication for inflammatory bowel disease11 and rheumatoid and seropositive arthritis12, but not in multiple sclerosis13. We have shown almost halving of the opioid consumption among persistent LDN users14. If there are beneficial effects of LDN in psychiatric disease, it is plausible that this will be reflected in the consumption of medicines. We aimed to test the hypothesis that initiation of LDN use is associated with reductions in the dispensing of psychotropic and antiepileptic medicines.
Materials and Methods
Study design and setting
We performed a pharmacoepidemiological nationwide quasi-experimental controlled before-after study using data from the Norwegian Prescription Database (NorPD). NorPD contains individual data on all prescriptions dispensed since 2004 to the entire Norwegian population living outside hospitals. Details on NorPD are published previously15. Each prescription in NorPD contains a unique pseudonym for the personal identifier, demographic data on patient and prescriber, the specialty of the prescriber, the Anatomical Therapeutic Chemical classification (ATC) code and the amount of medicine in defined daily doses (DDD), date of dispensing, and location of the dispensing pharmacy16. It is possible to follow dispensing to individuals on both reimbursed and non-reimbursed prescriptions. The Norwegian Institute of Public Health hosts the database17. We used the following variables in this study: personal identifier, age and sex for the patient, ATC code and product identifying number for all prescribed medicines, date of dispensing, and dispensed volume in DDDs. For a fee, NorPD provided a data file according to their data access procedures.
Participants
We included all Norwegian residents with at least one LDN prescription in 2013 according to NorPD. The date of the first dispense is the index date, and we recorded all dispensed prescriptions on psychotropic and antiepileptic medicines 365 days before the index date, and from the index date +364 days.
We stratified the patients into three subgroups depending on the number of collected LDN prescriptions after the index date. Patients were included in the persistent user subgroup (LDN × 4+) if they collected four or more LDN prescriptions. The other subgroups were one-time users (LDN × 1), and intermediate LDN users (LDN × 2–3). The patients served as their own controls (before data) and between groups that reflect LDN exposure. The LDN × 1, who likely used LDN for a short time, served as a control group compared to the LDN × 4+ group. The LDN × 2–3 group enabled dose-response comparisons.
The total observation time was 2 years for all participants. The first observation date was theoretically January 1, 2012, and the last observation date was December 31, 2014.
Outcome variables
Main outcome was difference between the cumulative collected amounts of DDDs and number of users on antiepileptics (ATC N03A), antipsychotics (N05A), anxiolytics (N05B), hypnotics (N05C), antidepressants (N06A) and psychostimulants (N06B) during the 365 days preceding the index date throughout the 364 days succeeding the first LDN dispense. We expressed the difference for each patient by subtracting the number of collected DDDs within all ATC groups the year following the first LDN dispense from the number of DDDs in the year preceding the first LDN dispense.
As secondary outcome, we used equivalent changes in DDD and number of users of some subgroups: Tricyclic antidepressants (N06AA), Selective serotonin inhibitors (N06AB), other antidepressants (N06AX), benzodiazepines (N05BA, N05CD, N03AE01) and z hypnotics (benzodiazepine like) (N05CF), gabapentin and pregabalin (N03AX12, N03AX16), lithium (N05AN) and lamotrigine (N05AX09).
Statistical methods
The number of patients in NorPD collecting a prescription on LDN in 2013 determined the study size. We used SPSS 25 and Excel 2013 for data analysis, and analyzed all data on an individual level. We used a pairwise two-sided t-test to determine the significance of mean changes in the sum of the DDDs per patient in each group for all examined medicines, and calculated 95% confidence intervals (CI) for difference of means. Change in the number of users was expressed as the proportion (% points) of each cohort, together with the 95% CI for the difference of proportion (in % points)18. Difference-in-difference of DDDs and proportion of users with 95% CI were calculated. The graphical representation of the cumulative difference in dispensing between the groups with the highest and the lowest LDN exposure (LDN × 4+–LDN × 1) before and after the index date is based on dispensing data.
Ethics statement
The Regional Committee for Medical and Health Research Ethics of Northern Norway reviewed the study protocol. Due to the encrypted data, the committee concluded that disclosure was not mandatory. The local privacy ombudsman for research at the University Hospital of Northern Norway approved the project. Consent from individual patients is by law not required for research based on NorPD.
Results
Patients
The inclusion of patients and dispenses of outcome medicines is shown in Fig. 1. In total, 11247 patients were included, and the observation period before and after index date constituted 69928 patient-months. The analyses on the examined medicines include 57951 prescriptions dispensed before and 61778 prescriptions dispensed after the index date.

Flow diagram of patient inclusion.
Descriptive data
Table 1 displays baseline data of the three subgroups. There were three percentage points more women in the LDN × 4+ group, and the mean age was approximately one year higher in this group. There were no missing data on age or sex among the included. The numbers of dispenses of all outcome medicines were comparable in all groups.
Outcome data
Mean number of dispensed DDDs before and after the first LDN prescription are summarized in Table 2, and changes in the number of users are presented in Table 3. The cumulative differences between LDN × 1 and LDN × 4+ in dispensed DDDs of the main outcomes before and after index date are shown in Fig. 2. Secondary outcomes are presented in Table 4 (DDDs) and Table 5 (number of users).

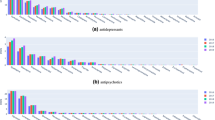
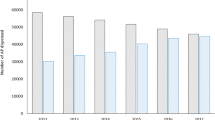
Cumulative difference in dispensed defined daily doses (DDD) of psychotropics and antiepileptics. The curves display difference in DDD between persistent LDN users (LDN × 4+, N = 5103) and patients that collected LDN only once (LDN x1, N = 3590), (LDN × 4+ minus LDN x1). Cumulative differences relative to Index date (Time = 0). Cumulative dose difference >0 means more dispensing to persistent LDN users than to LDN x1. Asymmetry of curve across index date means difference-in-difference before and after starting LDN, this was statistically significant for antipsychotics only. LDN: Low dose naltrexone.
For all medicines being examined, there were a 6% relative increase in DDD in both LDN × 1 and LDN × 2–3, and a significant difference in-difference of 11 DDD (95% CI 1.7 to 20.3, p = 0.027) between LDN x1 and LDN × 4+. The number of users of any examined medicine showed a 6% reduction in LDN × 4+, a significant difference-in-difference compared to LDN × 1 (3.8% points, 95% CI 2.0 to 5.6, p < 0.001).
Antiepileptics
In the LDN × 1 group, there was an 11% relative increase in the use of antiepileptics (DDD), in contrast to a non-significant reduction in the LDN × 4+ group. In number of users, there was a significant difference-in-difference between these two groups (3.1% points (95% CI 1.6 to 4.6, p < 0.001)). Significant increase in number of users was seen in both LDN x1 (+10%) and LDN × 2–3 (+14%) compared to LDN × 4+ (−11%). This is mainly attributable to changes in the dispensing of gabapentin and pregabalin, which was the dominating antiepileptics used by the included patients (73% of observed antiepileptic DDDs).
Antipsychotics
The dispensing of antipsychotics before the index date was similar in all groups, but there was a significant 11% relative DDD increase in the LDN × 1 group, which represent a significant difference-in-difference compared to LDN × 4+ (1.4 DDD, 95% CI 0.4 to 2.3, p = 0.007). There was a 17% relative reduction in the number of antipsychotic users for the LDN × 4+ group and a 25% relative increase in LDN × 1, representing a significant difference-in-difference between these groups (2.1% points, 95% CI 1.2 to 3.0, p < 0.001).
Benzodiazepines and Z hypnotics
There were increases in cumulative number of DDDs of benzodiazepine-like hypnotics (Z-hypnotics) in all groups, but no change in number of users. There was a significant increase in benzodiazepine DDDs for LDNx4+.
For benzodiazepines (including clonazepam), a significant increase in DDDs was seen only in LDN × 4 (+9%, relative). For all benzodiazepines and z-hypnotics combined, there was an increase in number of users in LDN × 1 (+1.3% points) compared with LDN × 4+ (−0.7% points), difference-in-difference was significant (1.9% points (95% CI 0.2 to 3.7, p = 0.035)).
Antidepressants
There were no significant differences in DDDs of antidepressants in any group. For the number of users of antidepressants, there was a significantly larger reduction in LDN × 4+ (−21%, relative) than in LDN × 1 (−2%), which also constituted a significant difference-in-difference (2.8% points, 95% CI 1.1 to 4.4, p = 0.001).
For LDN × 4+, there were significant reductions in DDD in tricyclic antidepressants (−8% relative), and in the number of users of tricyclic antidepressants (−21%) and SSRI (−6%). There was difference-in-difference in number of users (2.1% points, 95% CI 0.8 to 3.5, p = 0.003) of tricyclic antidepressants between LDN × 1 (−0.2% points) and LDN × 4 + (−2.4% points).
Psychostimulants
There were no changes in the dispensing of psychostimulants following the initiation of LDN use.
Mood stabilizers
There was a 13% relative increase in the number of DDDs for gabapentin and pregabalin in the LDN × 1 group, but no difference in cumulative sum of DDDs for lithium and lamotrigine in any group. There was a relative 70% increase in the number of lamotrigine users in LDN x1 and a significant difference-in-difference from LDN × 4+ (0.8% points (95% CI 0.4 to 1.3, p = 0.001).
For gabapentin and pregabalin, there was also a significant difference-in-difference in the number of users (2.4% points, 95% CI 1.0 to 3.8, p = 0.001) between. LDN × 1 (+0.6% points) and LDN × 4+ (−1.8% points).
Discussion
We have shown that starting LDN was followed by changes in the dispensing of several psychotropic medicines. When comparing persistent LDN users (LDN × 4+) with individuals who collected LDN only once (LDN x1), there were significant difference-in-differences in DDDs of antipsychotics, and in the number of users of antiepileptics, antipsychotics, antidepressants, tricyclic antidepressants, lamotrigine and gabapentin and pregabalin. In all of these groups, the reductions in number of users were larger in LDN × 4+. There was a dose-response relationship between reduction in number of users and increasing LDN exposure for antiepileptics, antipsychotics and antidepressants.
Major strengths of this study are the number of included participants, the completeness of the data, and the extended observation period. The number of participants was larger than in any other study on LDN, and the NorPD is a reliable, comprehensive, and complete register of all dispenses of prescription medicines to all Norwegian residents. The observations are from a real-world setting, and should be relevant for how LDN affect the use of other medicines at a population level.
Before-after studies have some limitations. Participants are not randomly recruited or assigned to groups, and there is risk of both inclusion and assignment bias. The differences in sex and age were minor, but as there were major differences in the dispensing of medicines before starting LDN (e.g. anxiolytics) that may indicate differences in psychiatric morbidity between groups. We still believe the analyses are valuable since before-after comparisons were made both within groups and between groups. By choosing differences in DDDs and number of users as main outcome measures, and also analyzing for difference-in-difference between groups also increase the generalizability of the study. Ideally, a control group unexposed to LDN should have been included, but our ethics data privacy approvals did not allow this.
Quasi-experimental studies are prone to deviation to a mean, and examples were present in this study (e.g. antiepileptic DDD)19. However, there were also several examples that the results deviated away from the pre-LDN mean of the total study population.
The analyses include multiple comparisons, and the findings should, therefore be interpreted with caution. It is likely some significant results found were caused by chance. However, the magnitude of some of the findings and the presence of dose-effect relationships suggest other explanations than chance alone.
NorPD records all dispenses outside hospitals and institutions. Dispenses to hospitalized patients could potentially lead to bias. We believe this is negligible since most LDN was prescribed in general practice. Less than 1% of LDN prescribers in Norway were psychiatrists10.
It is also important to remind that the NorPD contains very little clinical information. We focused on the dispensing of medicines, not indications for use or clinical condition. Assessment of compliance was impossible.
In a previous study, we showed that opioid use was reduced by 47% after starting LDN. This was not compensated by increased use of NSAID or other non-opioid analgesics13. In this study, we find that the number of users of adjuvant pain medication, such as gabapentin, pregabalin and tricyclic antidepressants, was reduced in persistent LDN users. This further substantiates assumptions that LDN may have therapeutic benefits in chronic pain conditions. However, it is possible that quitting opioids could be a part of the observed effects on psychotropic medicines more than actual therapeutic effects.
We did not observe any reduction in the dispensing of anxiolytics or hypnotics. On the contrary, there were increases in the cumulative dose for z-hypnotics for all groups. Sleep disturbances are among the most frequently reported adverse effects of LDN, and may contribute together with opioid withdrawal to an increased need for hypnotics.
One explanation to our findings is that patients experience beneficial effects that lead to reduced need for psychotropic drugs. It is plausible that naltrexone could influence mental health by interfering with the endogenous opioids, which may have a direct role in depression via the mesolimbic system20. Indications of a relationship between inflammation and psychiatric conditions such as depression21 and schizophrenia22 have paved the way for a separate field of research: Psychoneuroimmunology. The suggested immunomodulary effects of LDN could have implications for psychiatry.
In conclusion, the reductions in the use of antiepileptics and psychotropics following the initiation of persistent LDN use suggest that efficacy of LDN in depression and other psychiatric conditions cannot be ruled out. Due to the limitations of this pharmacoepidemiological study, the results should not directly lead to changes in clinical practice. Randomized clinical studies on LDN in psychiatry should be conducted. LDN could be an efficacious, safe and affordable treatment alternative.
Data availability
Data is available from the Norwegian Prescription Database (NorPD) for researchers who after application meet the criteria for access to prescription data. This includes Ethics Committee evaluation and a fee will be charged. For further details, please see https://www.fhi.no/en/op/data-access-from-health-registries-health-studies-andbiobanks/norwegian-prescription-database/Access-data-norpd/. We did not have any special privileges accessing the data, we obtained the data through the same application and fee payment process as outlined here. Our approvals do not allow the publication of raw data used in this study. In accordance with NorPD’s requirements, we had to delete all original data by 31 December 2018.
References
Li, Z., You, Y., Griffin, N., Feng, J. & Shan, F. Low-dose naltrexone (LDN): A promising treatment in immune-related diseases and cancer therapy. Int Immunopharmacol. 61, 178–184, https://doi.org/10.1016/j.intimp.2018.05.020 (2018).
Bolton, M. et al. Serious adverse events reported in placebo randomised controlled trials of oral naltrexone: a systematic review and meta-analysis. BMC Med. 17, 10, https://doi.org/10.1186/s12916-018-1242-0 (2019).
Pullen, L., Abbott, A., Lawhorn, A. & Harder, S. A review of the use of oral and injectable naltrexone for alcohol and opioid addiction treatment. Mental Health Pract, https://journals.rcni.com/mental-health-practice/evidence-and-practice/a-review-of-the-use-of-oral-and-injectable-naltrexone-for-alcohol-and-opioid-addiction-treatment-mhp.2018.e1263/abs, https://doi.org/10.7748/mhp.2018.e1263 (2018).
Mischoulon, D. et al. Randomized, proof-of-concept trial of low dose naltrexone for patients with breakthrough symptoms of major depressive disorder on antidepressants. J. Affect Disord. 208, 6–14, https://doi.org/10.1016/j.jad.2016.08.029 (2017).
Cree, B. A., Kornyeyeva, E. & Goodin, D. S. Pilot trial of low-dose naltrexone and quality of life in multiple sclerosis. Ann Neurol. 68, 145–150, https://doi.org/10.1002/ana.22006 (2010).
Smith, J. P. et al. Low-dose naltrexone therapy improves active Crohn’s disease. Am J. Gastroenterol. 102, 820–828 (2007).
Younger, J., Noor, N., McCue, R. & Mackey, S. Low-dose naltrexone for the treatment of fibromyalgia: findings of a small, randomized, double-blind, placebo-controlled, counterbalanced, crossover trial assessing daily pain levels. Arthritis Rheum. 65, 529–538, https://doi.org/10.1002/art.37734 (2013).
Bear, D. M. & Kessler, R. M. Treatments for depression and other diseases with a low dose agent. U.S. Patent Application No. 16/031,662. (2018).
Brewer, K. L., Mainhart, A. & Meggs, W. J. Double-blinded placebo-controlled cross-over pilot trial of naltrexone to treat Gulf War Illness. Fatigue. 6, 132–140, https://doi.org/10.1080/21641846.2018.1477034 (2018).
Raknes, G. & Småbrekke, L. A sudden and unprecedented increase in low dose naltrexone (LDN) prescribing in Norway. Patient and prescriber characteristics, and dispense patterns. A drug utilization cohort study. Pharmacoepidemiol Drug Saf. 26, 136–42, https://doi.org/10.1002/pds.4110 (2017).
Raknes, G., Simonsen, P. & Småbrekke, L. The Effect of Low-Dose Naltrexone on Medication in Inflammatory Bowel Disease: A Quasi Experimental Before-and-After Prescription Database Study. J. Crohns Colitis. 12, 677–686, https://doi.org/10.1093/ecco-jcc/jjy008 (2018).
Raknes, G. & Småbrekke, L. Low dose naltrexone: Effects on medication in rheumatoid and seropositive arthritis. A nationwide register-based controlled quasi-experimental before-after study. PLoS ONE. 14, e0212460, https://doi.org/10.1371/journal.pone.0212460 (2019).
Raknes, G. & Småbrekke, L. Low dose naltrexone in multiple sclerosis: Effects on medication use. A quasi-experimental study. PLoSONE. 12, e0187423, https://doi.org/10.1371/journal.pone.0187423 (2017).
Raknes, G. & Småbrekke, L. Low-dose naltrexone and opioid consumption: a drug utilization cohort study based on data from the Norwegian prescription database. Pharmacoepidemiol Drug Saf. 26, 685–693, https://doi.org/10.1002/pds.4201 (2017).
Furu, K. Establishment of the nationwide Norwegian Prescription Database (NorPD)–new opportunities for research in pharmacoepidemiology in Norway. Nor J. Epidemiol. 18, 129–136, https://doi.org/10.5324/nje.v18i2.23 (2008).
WHO Collaborating Centre for Drug Statistics Methodology. Guidelines for ATC classification and DDD assignment 2019, https://www.whocc.no/filearchive/publications/2019_guidelines_web.pdf (2019).
Norwegian Institute of Public Health. Norwegian Prescription Database, https://www.fhi.no/en/hn/health-registries/norpd/ (2019).
Altman, D. G. Comparing groups—categorical data. In Altman DG, editor. Practical Statistics for Medical Research (ed. Altman, D. G.) 234–241 (Chapman & Hall, 1991).
Torgerson, D. J. & Torgerson, C. J. The limitations of before and after designs. In Designing Randomised Trials in Health, Education and the Social Sciences (ed. Torgerson, D. J & Torgerson, C. J.) 9–16) (Palgrave Macmillan UK, 2008).
Peciña, M. et al. Endogenous opioid system dysregulation in depression: implications for new therapeutic approaches. Mol Psychiatry. 24, 576–587 (2019).
Khandaker, G. M. et al. Inflammation and immunity in schizophrenia: implications for pathophysiology and treatment. Lancet Psychiatry. 2, 258–270, https://doi.org/10.1038/s41380-018-0117-2 (2015).
Miller, A. H. & Raison, C. L. The role of inflammation in depression: from evolutionary imperative to modern treatment target. Nat Rev Immunol. 16, 22–34, https://doi.org/10.1038/nri.2015.5 (2016).
Acknowledgements
We would like to thank Frode Skjold for preparing the data files.
Author information
Authors and Affiliations
Contributions
G.R. contributed to the conception of the study, designed the study, performed statistical analyses and drafted the manuscript. L.S. contributed to the design of the study and to statistical analyses. Both authors participated in revising the manuscript and approving the final version.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Raknes, G., Småbrekke, L. Changes in the consumption of antiepileptics and psychotropic medicines after starting low dose naltrexone: A nation-wide register-based controlled before-after study. Sci Rep 9, 15085 (2019). https://doi.org/10.1038/s41598-019-51569-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-019-51569-z
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
