
Abstract
Precision medicine focuses on DNA abnormalities, but not all tumors have tractable genomic alterations. The WINTHER trial (NCT01856296) navigated patients to therapy on the basis of fresh biopsy-derived DNA sequencing (arm A; 236 gene panel) or RNA expression (arm B; comparing tumor to normal). The clinical management committee (investigators from five countries) recommended therapies, prioritizing genomic matches; physicians determined the therapy given. Matching scores were calculated post-hoc for each patient, according to drugs received: for DNA, the number of alterations matched divided by the total alteration number; for RNA, expression-matched drug ranks. Overall, 303 patients consented; 107 (35%; 69 in arm A and 38 in arm B) were evaluable for therapy. The median number of previous therapies was three. The most common diagnoses were colon, head and neck, and lung cancers. Among the 107 patients, the rate of stable disease ≥6 months and partial or complete response was 26.2% (arm A: 23.2%; arm B: 31.6% (P = 0.37)). The patient proportion with WINTHER versus previous therapy progression-free survival ratio of >1.5 was 22.4%, which did not meet the pre-specified primary end point. Fewer previous therapies, better performance status and higher matching score correlated with longer progression-free survival (all P < 0.05, multivariate). Our study shows that genomic and transcriptomic profiling are both useful for improving therapy recommendations and patient outcome, and expands personalized cancer treatment.
This is a preview of subscription content, access via your institution
Access options
Access Nature and 54 other Nature Portfolio journals
Get Nature+, our best-value online-access subscription
$29.99 / 30 days
cancel any time
Subscribe to this journal
Receive 12 print issues and online access
$209.00 per year
only $17.42 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout


Similar content being viewed by others

Data availability
The availability of the data is described in the Nature Research Reporting Summary. Detailed clinical and biological information for each patient is available in Supplementary Table 4; further biological data are available at www.winconsortium.org, containing: (1) tumor mutations data in XML format; and (2) expression data in a table format (providing information about tumor versus normal fold change and tumor intensity alone for all of the cases for which mRNA was analyzed). The BAM and XML files for normal tissue are deposited in dbGaP with a controlled access mechanism for private information.
Code availability
No custom code or mathematical algorithm was used. Statistical analysis was performed using standard software including SAS and R.
References
Schwaederle, M. et al. Association of biomarker-based treatment strategies with response rates and progression-free survival in refractory malignant neoplasms: a meta-analysis. JAMA Oncol. 2, 1452–1459 (2016).
Jardim, D. L. et al. Impact of a biomarker-based strategy on oncology drug development: a meta-analysis of clinical trials leading to FDA approval. J. Natl. Cancer Inst. 107, djv253 (2015).
Schwaederle, M. et al. Impact of precision medicine in diverse cancers: a meta-analysis of phase II clinical trials. J. Clin. Oncol. 33, 3817–3825 (2015).
Goodman, A. M. et al. Tumor mutational burden as an independent predictor of response to immunotherapy in diverse cancers. Mol. Cancer Ther. 16, 2598–2608 (2017).
Tsao, M. S. et al. Erlotinib in lung cancer—molecular and clinical predictors of outcome. N. Engl. J. Med. 353, 133–144 (2005).
Demetri, G. D. et al. Efficacy and safety of imatinib mesylate in advanced gastrointestinal stromal tumors. N. Engl. J. Med. 347, 472–480 (2002).
Chapman, P. B. et al. BRIM-3 study group: improved survival with vemurafenib in melanoma with BRAF V600E mutation. N. Engl. J. Med. 364, 2507–2516 (2011).
Solomon, B. J. et al. First-line crizotinib versus chemotherapy in ALK-positive lung cancer. N. Engl. J. Med. 371, 2167–2177 (2014).
Rodon, J. et al. Challenges in initiating and conducting personalized cancer therapy trials: perspectives from WINTHER, a Worldwide Innovative Network (WIN) Consortium trial. Ann. Oncol. 26, 1791–1798 (2015).
Von Hoff, D. D. et al. Pilot study using molecular profiling of patients’ tumors to find potential targets and select treatments for their refractory cancers. J. Clin. Oncol. 28, 4877–4883 (2010).
Wheler, J. J. et al. Cancer therapy directed by comprehensive genomic profiling: a single center study. Cancer Res. 76, 3690–3701 (2016).
Schwaederle, M. et al. Precision oncology: the UC San Diego Moores Cancer Center PREDICT experience. Mol. Cancer Ther. 15, 743–752 (2016).
Frampton, G. M. et al. Development and validation of a clinical cancer genomic profiling test based on massively parallel DNA sequencing. Nat. Biotechnol. 31, 1023–1031 (2013).
Tsimberidou, A. M. et al. Initiative for molecular profiling and advanced cancer therapy (IMPACT): an MD Anderson precision medicine study. JCO Precis. Oncol. 2017, 2017 (2017).
Lazar, V. et al. A simplified interventional mapping system (SIMS) for the selection of combinations of targeted treatments in non-small cell lung cancer. Oncotarget 6, 14139–14152 (2015).
Janjigian, Y. Y. et al. Dual inhibition of EGFR with afatinib and cetuximab in kinase inhibitor-resistant EGFR-mutant lung cancer with and without T790M mutations. Cancer Discov. 4, 1036–1045 (2014).
Le, D. T. et al. Mismatch repair deficiency predicts response of solid tumors to PD-1 blockade. Science 357, 409–413 (2017).
Koscielny, S. Why most gene expression signatures of tumors have not been useful in the clinic. Sci. Transl. Med. 2, 14ps2 (2010).
Tsimberidou, A. M. et al. Personalized medicine in a phase I clinical trials program: the MD Anderson Cancer Center initiative. Clin. Cancer Res. 18, 6373–6383 (2012).
Massard, C. et al. High-throughput genomics and clinical outcome in hard-to-treat advanced cancers: results of the MOSCATO 01 trial. Cancer Discov. 7, 586–595 (2017).
Le Tourneau, C. et al. Molecularly targeted therapy based on tumour molecular profiling versus conventional therapy for advanced cancer (SHIVA): a multicentre, open-label, proof-of-concept, randomised, controlled phase 2 trial. Lancet Oncol. 16, 1324–1334 (2015).
ECOG-ACRIN Cancer Research Group & National Cancer Institute Executive Summary: Interim Analysis of the NCI-MATCH Trial (ECOG-ACRIN Cancer Research Group & National Cancer Institute, 2016); http://ecog-acrin.org/nci-match-eay131/interim-analysis
Gerlinger, M. et al. Intratumor heterogeneity and branched evolution revealed by multiregion sequencing. N. Engl. J. Med. 366, 883–892 (2012).
Ciriello, G. et al. Emerging landscape of oncogenic signatures across human cancers. Nat. Genet. 45, 1127–1133 (2013).
Bieg-Bourne, C. C. et al. Next-generation sequencing in the clinical setting clarifies patient characteristics and potential actionability. Cancer Res. 77, 6313–6320 (2017).
Kandoth, C. et al. Mutational landscape and significance across 12 major cancer types. Nature 502, 333–339 (2013).
Martincorena, I. & Campbell, P. J. Somatic mutations in cancer and normal cells. Science 349, 1483–1489 (2015).
Kato, S. M. et al. Utility of genomic analysis in circulating tumor DNA from patients with carcinoma of unknown primary. Cancer Res. 77, 4238–4246 (2017).
Janku, F. et al. Assessing PIK3CA and PTEN in early-phase trials with PI3K/AKT/mTOR inhibitors. Cell Rep. 6, 377–387 (2014).
Ganesan, P. et al. Target-based therapeutic matching in early-phase clinical trials in patients with advanced colorectal cancer and PIK3CA mutations. Mol. Cancer Ther. 12, 2857–2863 (2013).
Holsinger, F. C. et al. Biomarker-directed therapy of squamous carcinomas of the head and neck: targeting PI3K/PTEN/mTOR pathway. J. Clin. Oncol. 31, e137–e140 (2013).
Janku, F. et al. PIK3CA mutations in advanced cancers: characteristics and outcomes. Oncotarget 3, 1566–1575 (2012).
Janku, F. et al. PIK3CA mutation H1047R is associated with response to PI3K/AKT/mTOR signaling pathway inhibitors in early-phase clinical trials. Cancer Res. 73, 276–284 (2013).
Garrido-Laguna, I. et al. KRASness and PIK3CAness in patients with advanced colorectal cancer: outcome after treatment with early-phase trials with targeted pathway inhibitors. PLoS ONE 7, e38033 (2012).
Janku, F. et al. PIK3CA mutations frequently coexist with RAS and BRAF mutations in patients with advanced cancers. PLoS ONE 6, e22769 (2011).
Janku, F. et al. PI3K/AKT/mTOR inhibitors in patients with breast and gynecologic malignancies harboring PIK3CA mutations. J. Clin. Oncol. 30, 777–782 (2012).
Rodon, J., Dienstmann, R., Serra, V. & Tabernero, J. Development of PI3K inhibitors: lessons learned from early clinical trials. Nat. Rev. Clin. Oncol. 10, 143–153 (2013).
Yao, J. C. et al. RAD001 in advanced neuroendocrine tumours, fourth trial (RADIANT-4) study group. Everolimus for the treatment of advanced, non-functional neuroendocrine tumours of the lung or gastrointestinal tract (RADIANT-4): a randomised, placebo-controlled, phase 3 study. Lancet 387, 968–977 (2016).
Benjamini, Y. & Hochberg, Y. Controlling the false discovery rate: a practical and powerful approach to multiple testing. J. R. Stat. Soc. 57, 289–300 (1995).
Ioannidis, J. P. Why most published research findings are false. PLoS Med. 2, e124 (2005).
Acknowledgements
Dr John Mendelsohn, President Emeritus of The University of Texas, MD Anderson Cancer Center, Director of Sheikh Khalifa Bin Zayad Al Nahyan Institute for Personalized Cancer Therapy (IPCT), Houston, TX, USA, Chairman of the WIN Association—WIN Consortium, Villejuif, France, and co-author of the Letter died on 7 January 2019. Dr Mendelsohn was a brilliant scientist and visionary, an optimist and a truly inspirational leader. The WINTHER study was one of his very last projects. The research leading to these results has received funding from the European Union Seventh Framework Program (FP7/2007–2013 under grant agreement no. 306125). This work was funded in part by the ARC Foundation for Cancer Research (France), Pfizer Oncology, Lilly France SAS and Novartis Pharmaceuticals Corporation. This work was also funded in part by The Fero/J.P. Morgan Private Bank Clinical Oncology Research Grant, the National Cancer Institute grant P30 P30-CA023100 (R.K.), the Israeli Science Foundation grant 1188/16 (E.R.), Instituto Salud Carlos III—Programa Rio Hortega Contract grant CM15/00255 (I.B.), the Canadian Institutes for Health Research (grant MOP-142281 to W.H.M.) and the Canadian Cancer Society (grant 703811 to W.H.M.).
Author information
Authors and Affiliations
Contributions
J.-C.S., R.K., V.L., J.M., R.L.S. and J.J.L. contributed with conception of the presented idea and the design and funding of this project. J.Rodon, J.-C.S., R.B., W.H.M., P.S., A.A., I.B. and Y.L. contributed to implementation of the project and with patient enrollment. J.J.L., E.R., A.K. and V.L. performed the bioinformatic computations and statistical analysis. V.L., M.A. and V.M. carried out the genomic experiments. F.W., C.B. and A.O. contributed with the logistics of the trial and quality control. J.-F.M. and J.Raynaud contributed with funding and conception of the idea. J.Rodon, J.-C.S., R.B., W.H.M., P.S., A.A., I.B., Y.L., G.B., R.K., E.R., V.L., J.J.L., F.W., C.B., A.O., A.T. and J.T. contributed to the interpretation of the results. R.K. and V.L. took the lead in writing the manuscript. All authors provided critical feedback and helped to shape the research, analysis and manuscript and approved the final version.
Corresponding author
Ethics declarations
Competing interests
J.Rodon reports non-financial support and reasonable reimbursement for travel from the European Journal of Cancer, Vall d’Hebron Institut of Oncology, the Chinese University of Hong Kong, SOLTI, Elsevier, GlaxoSmithKline; receives consulting and travel fees from Novartis, Eli Lilly, Orion Pharmaceuticals, Servier Pharmaceuticals, Peptomyc, Merck Sharp & Dohme, Kelun Pharmaceutical/Klus Pharma, Spectrum Pharmaceuticals, Pfizer, Roche Pharmaceuticals and Ellipses Pharma (including serving on the scientific advisory board from 2015 to present); receives research funding from Bayer and Novartis; and serves as investigator in clinical trials with Spectrum Pharmaceuticals, Tocagen, Symphogen, BioAtla, Pfizer, GenMab, CytomX, Kelun Pharmaceutical/Klus Pharma, Takeda-Millenium, GlaxoSmithKline and Ipsen. J.-C.S. received consultancy fees from AstraZeneca, Roche, Sanofi, Servier, Pierre Fabre and is a full-time employee of Medimmune/AstraZeneca since September 2017. W.H.M. receives speaking and/or consulting fees from BMS, Merck, Roche, Novartis and Amgen. E.R. received consultant fees from Teva, Carmentix and Hinoman, is receiving consultant fees from Equinom and has ownership interest in Carmentix. A.O. receives consulting fees from Roche Israel, MSD Israel, Boehringer Ingelheim and AstraZeneca. A.T. received consultant fees from Roche and receives research funding from EMD Serono, Baxter, Foundation Medicine, ONYX and Bayer. P.S. collaborates in research with Roche, AstraZeneca, BMS and Novartis. I.B. receives consultant fees from Orion Pharma, receives speaking fees from BMS, AstraZeneca and Merck Serono, and is principal investigator and receives funding for clinical trials from AstraZeneca, BMS, Celgene, Gliknik, GSK, Janssen, KURA, MSD, Novartis, Orion Pharma and Pfizer. Y.L. collaborates in research with Merck, Roche, AstraZeneca, Sanofi, Pfizer, Janssen, Astellas and BMS. M.A. is an employee and shareholder of Ariana Pharmaceuticals. V.M. is an employee (salary and equity) of Foundation Medicine. J.-F.M. is a full-time employee and stockholder of Pfizer. G.B. collaborates in formal clinical trial contracts, investigator initiated trials (IITs) and in joint grants funded by the Canadian and Québec governments with Roche, Merck, Novartis, AstraZeneca, Bayer, Esperas, Aurka, Caprion and MRM-P. J.T. declares a scientific consultancy role for Array Biopharma, AstraZeneca, Bayer, BeiGene, Boehringer Ingelheim, Chugai, Genentech, Genmab A/S, Halozyme, Imugene, Inflection Biosciences, Ipsen, Kura Oncology, Lilly, MSD, Menarini, Merck Serono, Merrimack, Merus, Molecular Partners, Novartis, Peptomyc, Pfizer, Pharmacyclics, ProteoDesign SL, Rafael Pharmaceuticals, F. Hoffmann-La Roche, Sanofi, SeaGen, Seattle Genetics, Servier, Symphogen, Taiho, VCN Biosciences, Biocartis, Foundation Medicine, HalioDX SAS and Roche Diagnostics. R.K. has research funding from Incyte, Genentech, Merck Serono, Pfizer, Sequenom, Foundation Medicine, Guardant Health, Grifols, Konica Minolta and OmniSeq, as well as consultant fees from LOXO, X-Biotech, Actuate Therapeutics, Roche and NeoMed. She serves as an advisor to Soluventis. She receives speaker fees from Roche and also has equity in IDbyDNA, CureMatch and Soluventis. F.W., C.B. and V.L. are full-time employees of WIN Association–WIN Consortium. WIN Association–WIN Consortium is the owner of the patent family entitled ‘Method for predicting efficacy of drugs in a patient’ (WINTHER). The inventors are V.L., J.-C.S., Michel Ducreux and Thomas Tursz.
Additional information
Publisher’s note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Extended data
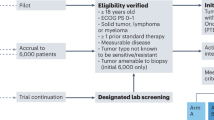
Extended Data Fig. 1
Consort diagram.
Extended Data Fig. 2 Kaplan–Meier curves of various factors influencing PFS and OS.
a, Kaplan–Meier curves of PFS for arm A by cancer site (lung site, N = 17 versus other site, N = 52). PFS2 denotes the PFS of the WINTHER treatment. P = 0.0204 by two-sided log-rank test. b, Kaplan–Meier curves of PFS for arm A by ECOG performance status at treatment (PS = 0, N = 21 versus PS = 1, N = 48). PFS2 denotes the PFS of the WINTHER treatment. P = 0.0002 by two-sided log-rank test.
Extended Data Fig. 3 Kaplan–Meier curves of various factors influencing PFS and OS.
a, Kaplan–Meier curves of PFS for arm B by age group. Age >60 yr, N = 17 versus age ≤60 yr, N = 21. PFS2 denotes the PFS of the WINTHER treatment. P = 0.0361 by two-sided log-rank test. b, Kaplan–Meier curves of PFS for arm B by sex. Sex = female, N = 12 versus sex = male, N = 26. PFS2 denotes the PFS of the WINTHER treatment. P = 0.0252 by two-sided log-rank test. c, Kaplan–Meier curves of PFS for arm B by the number of previous treatments. For the number of previous treatments of ≤2, N = 11 versus >2, N = 27. PFS2 denotes the PFS of the WINTHER treatment. P = 0.0066 by two-sided log-rank test.
Extended Data Fig. 4 Kaplan–Meier curves of various factors influencing PFS and OS.
a, Kaplan–Meier curves of PFS all patients by ECOG PS at treatment. PS = 0, N = 36 versus PS = 1, N = 71. PFS2 denotes the PFS of the WINTHER treatment. P = 0.0007 by two-sided log-rank test. b, Kaplan–Meier curves of PFS of all of the patients by the number of previous treatments. The number of previous treatments of ≤2, N = 34 versus >2, N = 73. PFS2 denotes the PFS of the WINTHER treatment. P = 0.0025 by two-sided log-rank test.
Extended Data Fig. 5 Kaplan–Meier curves of various factors influencing PFS and OS.
a, Kaplan–Meier curves of OS of all patients by ECOG PS at treatment. PS = 0, N = 36 versus PS = 1, N = 71 (P < 0.0001 by two-sided log-rank test). b, Kaplan–Meier curves of OS all patients by the number of previous treatments (Tx). The number of prior Tx of ≤ 2, N = 34 versus >2, N = 73 (P = 0.0009 by two-sided log-rank test). c, Kaplan–Meier curves of OS of all patients by matching score. MS high, N = 80 versus MS low, N = 27 (P = 0.0103 by two-sided log-rank test).
Extended Data Fig. 6 Effect of individual variability of normal VEGFA RNA expression on the assessment of VEGFA levels in tumors.
On the y axis, the transcript intensity in tumors is shown, and on the x axis the transcript intensity in matched normal biopsies is shown. Intensities are measured as a relative fluorescence unit (RFU) signal as assessed with Agilent microarray technology. Overexpression in the tumor is denoted in turquoise points, underexpression is denoted in red and no change is denoted in black. The twofold threshold (both high and low) is indicated by two dotted black lines. All 101 patients of the WINTHER study with evaluable RNA data were considered. Example 1 shows a patient with a low level of basal expression (300 RFU) in the tumor and 300 RFU in the normal biopsies, with no differential expression between the normal and tumor biopsies. Example 2 shows a patient with a high level of basal expression of 6,000 RFU in the tumor versus 6,000 RFU in the normal biopsies, but again no differential expression between the tumor and normal counterpart. Example 3 marked in turquoise shows the pattern of a higher expression in tumor versus normal tissue. Example 4 marked in red shows the pattern of a lower expression in tumor versus normal tissue. This current study hypothesizes that simultaneously investigating the matched phenotypically normal tissue can help to optimize transcriptomic data. With this approach, each patient serves as his or her own control, hence avoiding the use of pooled tumor or normal tissues. Our data demonstrate that the level of basal gene expression is highly variable between individuals. All patients presented with black points had no differential expression between tumor and normal tissue, but others show a large variability between individuals in the basal level of normal expression of VEGFA.
Supplementary information
Supplementary Information
Supplementary Tables 1–4
Rights and permissions
About this article

Cite this article
Rodon, J., Soria, JC., Berger, R. et al. Genomic and transcriptomic profiling expands precision cancer medicine: the WINTHER trial. Nat Med 25, 751–758 (2019). https://doi.org/10.1038/s41591-019-0424-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41591-019-0424-4
This article is cited by
-
DNA-based molecular classifiers for the profiling of gene expression signatures
Journal of Nanobiotechnology (2024)
-
New regulatory thinking is needed for AI-based personalised drug and cell therapies in precision oncology
npj Precision Oncology (2024)
-
The molecular interaction pattern of lenvatinib enables inhibition of wild-type or kinase-mutated FGFR2-driven cholangiocarcinoma
Nature Communications (2024)
-
Molekularpathologische Untersuchungen im Wandel der Zeit
Die Pathologie (2024)
-
Omics-based molecular classifications empowering in precision oncology
Cellular Oncology (2024)
