
Abstract
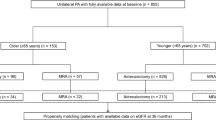
Recent studies have explored the association between primary aldosteronism and cardiovascular disease incidence. The association between specific primary aldosteronism treatments and differential improvement in cardiovascular event rates is yet to be established. This study was designed to compare the relative effects of spironolactone therapy and surgical intervention on cardiovascular outcomes among primary aldosteronism patients. This retrospective observational study included 853 primary aldosteronism patients from the First Affiliated Hospital of China Medical University between 2014 and 2022. Patients who had completed abdominal computed tomography (CT) examinations with similar metabolic characteristics and 6-month follow-up analyses were included in this study. These patients were separated into a surgical treatment group (n = 33) and a spironolactone treatment group (n = 51). Demographic data, biochemical analysis results, liver/spleen (L/S) X-ray attenuation ratio, hospitalization frequency, and cardiovascular events were compared between the two groups. The spironolactone group demonstrated significantly improved metabolic characteristics compared to the surgical group, shown by lower BMI, blood pressure, total cholesterol (TC), insulin resistance index (IRI), and reduced non-alcoholic fatty liver disease prevalence. Metabolic parameters did not differ significantly within the surgical treatment group when comparing pre- and postoperative values. The incidence of cardiovascular events was lower in the spironolactone group compared to the surgery group (23/33 vs. 20/51, P < 0.001) despite higher hospitalization rates(37/31 vs. 61/53, P < 0.001). In patients with primary aldosteronism, spironolactone treatment is more effective than surgical intervention in remediating abnormal lipid and glucose metabolism while improving cardiovascular outcomes. Chinese clinical trial registry registration number: ChiCTR2300074574.

This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout


Similar content being viewed by others


References
Reincke M, Bancos I, Mulatero P, Scholl UI, Stowasser M, Williams TA. Diagnosis and treatment of primary aldosteronism. Lancet Diabetes Endocrinol. 2021;9:876–92.
Paschos P, Tziomalos K. Nonalcoholic fatty liver disease and the renin-angiotensin system: implications for treatment. World J Hepatol. 2012;4:327–31.
Luther JM, Luo P, Kreger MT, Brissova M, Dai C, Whitfield TT, et al. Aldosterone decreases glucose-stimulated insulin secretion in vivo in mice and in murine islets. Diabetologia. 2011;54:2152–63.
Shibayama Y, Wada N, Baba S, Obara S, Sakai H, Usubuchi H, et al. The risk factors for hepatic steatosis in patients with primary aldosteronism. Endocr J. 2020;67:623–9.
Wu VC, Chueh SJ, Chen L, Chang CH, Hu YH, Lin YH, et al. Risk of new-onset diabetes mellitus in primary aldosteronism: a population study over 5 years. J Hypertens. 2017;35:1698–708.
Rossi GP, Maiolino G, Flego A, Belfiore A, Bernini G, Fabris B, et al. Adrenalectomy lowers incident atrial fibrillation in primary aldosteronism patients at long term. Hypertension. 2018;71:585–91.
Hundemer GL, Curhan GC, Yozamp N, Wang M, Vaidya A. Cardiometabolic outcomes and mortality in medically treated primary aldosteronism: a retrospective cohort study. Lancet Diabetes Endocrinol. 2018;6:51–59.
Catena C, Colussi G, Nadalini E, Chiuch A, Baroselli S, Lapenna R, et al. Cardiovascular outcomes in patients with primary aldosteronism after treatment. Arch Intern Med. 2008;168:80–5.
Reincke M, Fischer E, Gerum S, Merkle K, Schulz S, Pallauf A, et al. Observational study mortality in treated primary aldosteronism: the German Conn’s registry. Hypertension. 2012;60:618–24.
Plouin PF, Amar L, Chatellier G. Trends in the prevalence of primary aldosteronism, aldosterone-producing adenomas, and surgically correctable aldosterone-dependent hypertension. Nephrol Dial Transplant. 2004;19:774–7.
Chen Y, Chen X, Chen Q, Yu C. Non-alcoholic fatty liver disease and hypokalemia in primary aldosteronism among Chinese population. Front Endocrinol (Lausanne). 2021;12:565714.
Wang J, Ma L, Chen S, Xu L, Miao M, Yu C, et al. Risk for the development of non-alcoholic fatty liver disease: a prospective study. J Gastroenterol Hepatol. 2018;33:1518–23.
Fallo F, Dalla Pozza A, Tecchio M, Tona F, Sonino N, Ermani M, et al. Nonalcoholic fatty liver disease in primary aldosteronism: a pilot study. Am J Hypertens. 2010;23:2–5.
Funder JW, Carey RM, Mantero F, Murad MH, Reincke M, Shibata H, et al. The management of primary aldosteronism: case detection, diagnosis, and treatment: an Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab. 2016;101:1889–916.
Wang K, Hu J, Yang J, Song Y, Fuller PJ, Hashimura H, et al. Development and validation of criteria for sparing confirmatory tests in diagnosing primary aldosteronism. J Clin Endocrinol Metab. 2020;105:2449–56.
Hung A, Ahmed S, Gupta A, Davis A, Kline GA, Leung AA, et al. Performance of the aldosterone to renin ratio as a screening test for primary aldosteronism. J Clin Endocrinol Metab. 2021;106:2423–35.
Williams TA, Lenders JWM, Mulatero P, Burrello J, Rottenkolber M, Adolf C, et al. Outcomes after adrenalectomy for unilateral primary aldosteronism: an international consensus on outcome measures and analysis of remission rates in an international cohort. Lancet Diabetes Endocrinol. 2017;5:689–99.
Xu C, Chen Y, Xu L, Miao M, Li Y, Yu C. Serum complement C3 levels are associated with nonalcoholic fatty liver disease independently of metabolic features in Chinese population. Sci Rep. 2016;6:23279.
Lewandowski KC, Skowronska-Jozwiak E, Lukasiak K, Galuszko K, Dukowicz A, Cedro M, et al. How much insulin resistance in polycystic ovary syndrome? Comparison of HOMA-IR and insulin resistance (Belfiore) index models. Arch Med Sci. 2019;15:613–8.
Castera L, Friedrich-Rust M, Loomba R. Noninvasive assessment of liver disease in patients with nonalcoholic fatty liver disease. Gastroenterology. 2019;156:1264–1281.e4.
Milliez P, Girerd X, Plouin PF, Blacher J, Safar ME, Mourad JJ. Evidence for an increased rate of cardiovascular events in patients with primary aldosteronism. J Am Coll Cardiol. 2005;45:1243–8.
Zennaro MC, Boulkroun S, Fernandes-Rosa FL. Pathogenesis and treatment of primary aldosteronism. Nat Rev Endocrinol. 2020;16:578–89.
Son DH, Lee HS, Lee YJ, Lee JH, Han JH. Comparison of triglyceride-glucose index and HOMA-IR for predicting prevalence and incidence of metabolic syndrome. Nutr Metab Cardiovasc Dis. 2022;32:596–604.
Adler GK, Murray GR, Turcu AF, Nian H, Yu C, Solorzano CC, et al. Primary aldosteronism decreases insulin secretion and increases insulin clearance in humans. Hypertension. 2020;75:1251–9.
Ipsen DH, Lykkesfeldt J, Tveden-Nyborg P. Molecular mechanisms of hepatic lipid accumulation in non-alcoholic fatty liver disease. Cell Mol Life Sci. 2018;75:3313–27.
Tetti M, Gong S, Veglio F, Reincke M, Williams TA. Primary aldosteronism: Pathophysiological mechanisms of cell death and proliferation. Front Endocrinol (Lausanne). 2022;13:934326.
van der Heijden C, Bode M, Riksen NP, Wenzel UO. The role of the mineralocorticoid receptor in immune cells in cardiovascular disease. Br J Pharmacol. 2022;179:3135–51.
Hosoya K, Minakuchi H, Wakino S, Fujimura K, Hasegawa K, Komatsu M, et al. Insulin resistance in chronic kidney disease is ameliorated by spironolactone in rats and humans. Kidney Int. 2015;87:749–60.
Mato JM, Alonso C, Noureddin M, Lu SC. Biomarkers and subtypes of deranged lipid metabolism in non-alcoholic fatty liver disease. World J Gastroenterol. 2019;25:3009–20.
Velema M, Dekkers T, Hermus A, Timmers H, Lenders J, Groenewoud H, et al. Quality of life in primary aldosteronism: a comparative effectiveness study of adrenalectomy and medical treatment. J Clin Endocrinol Metab. 2018;103:16–24.
Amar L, Plouin PF, Steichen O. Aldosterone-producing adenoma and other surgically correctable forms of primary aldosteronism. Orphanet J Rare Dis. 2010;5:9.
Katsiki N, Mikhailidis DP, Mantzoros CS. Non-alcoholic fatty liver disease and dyslipidemia: an update. Metabolism. 2016;65:1109–23.
Munoz-Durango N, Arrese M, Hernandez A, Jara E, Kalergis AM, Cabrera D. A mineralocorticoid receptor deficiency in myeloid cells reduces liver steatosis by impairing activation of CD8(+) T cells in a nonalcoholic steatohepatitis mouse model. Front Immunol. 2020;11:563434.
Alqarni I, Bassiouni YA, Badr AM, Ali RA. Telmisartan and/or chlorogenic acid attenuates fructose-induced non-alcoholic fatty liver disease in rats: Implications of cross-talk between angiotensin, the sphingosine kinase/sphingoine-1-phosphate pathway, and TLR4 receptors. Biochem Pharmacol. 2019;164:252–62.
Bakris GL, Agarwal R, Anker SD, Pitt B, Ruilope LM, Rossing P, et al. Effect of finerenone on chronic kidney disease outcomes in type 2 diabetes. N Engl J Med. 2020;383:2219–29.
Targher G, Corey KE, Byrne CD. NAFLD, and cardiovascular and cardiac diseases: factors influencing risk, prediction and treatment. Diabetes Metab. 2021;47:101215.
Amar L, Lorthioir A, Azizi M, Plouin PF. Progress in primary aldosteronism. Mineralocorticoid antagonist treatment for aldosterone-producing adenoma. Eur J Endocrinol. 2015;172:R125–9.
Acknowledgements
The original data used in this article will be provided by the authors.
Funding
Liaoning Provincial Health Commission Xingliao Talents Program - Young Medical Master Project (YXMJ-QN-01).
Author information
Authors and Affiliations
Contributions
Professor Yanli Cao proposed the initial concept. Dr. Jing Liu collected clinical data. Dr. Zhuo Li, Mingfeng Yang, Ruohe Sha, Ruike Yan, and Xinxin Wang collected medical records, and Shiting Zhou designed the research protocol, collected demographic data, and conducted statistical analysis. Throughout the entire research process, Professor Yanli Cao provided supervision and consultation. All authors contributed to this article and approved the submitted version.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no competing interests.
Ethical approval
This study was reviewed and approved by the Ethics Committee of the First Affiliated Hospital of China Medical University.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Zhou, S., Liu, J., Li, Z. et al. The effect of different treatment strategies on glycolipid metabolism disorders and cardiovascular events in primary aldosteronism. Hypertens Res (2024). https://doi.org/10.1038/s41440-024-01648-0
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41440-024-01648-0
