
Abstract
Panic disorder is characterized by sudden, repeated, and unexpected attacks of intense fear and overwhelming anxiety about when another attack may strike. Patients with panic disorder and healthy individuals with a history of panic attacks show a hypersensitivity to unpredictable threats, suggesting a possible link between panic and sustained anxiety. The purpose of this study was to determine the degree to which induced symptoms of panic relate to fear and anxiety, as well as activity in the neural systems that mediate and regulate these affective states. Psychological and physiological symptoms of panic were assessed during an 8-min 7.5% CO2 challenge task. Psychological, physiological, and neural symptoms of fear and anxiety were measured during two sessions (one psychophysiology and one functional magnetic resonance imaging where subjects experienced several blocks of no threat (N), predictable shock (P), and unpredictable shock (U; NPU threat task). We used a principle component analysis to characterize panic susceptibility (PS), and found that PS significantly predicted dorsolateral prefrontal cortex (dlPFC) activity to the unpredictable cue during the NPU threat task. When examining the weighted beta coefficients from this analysis, we observed that self-reported fear/anxiety during the CO2 challenge negatively loaded onto dlPFC activity during the NPU task. Consistent with this observation, dlPFC activity during the unpredictable cue was also negatively correlated with anxiety during the NPU sessions. Together, these results suggest that panic symptoms and anxiety are regulated by the same prefrontal cognitive control system.
Similar content being viewed by others

Introduction
Panic disorder is characterized by sudden, repeated, and unexpected attacks of intense fear and anxiety1. Not only do individuals with panic disorder suffer from these paralyzing attacks, but they also express intense worry and overwhelming anxiety about when another attack may strike1. Although this disorder may profoundly impact the quality of life of the affected individuals, we know little about the etiology of this disorder, or the neural and cognitive systems that maintain and regulate panic symptoms2.
Many symptoms of panic attacks, such as breathing problems, dizziness, and numbness, can be traced to the respiratory system2. Accordingly, elevated CO2 blood levels are thought to contribute to panic attacks2. To study panic attacks, researchers have developed a CO2 challenge to experimentally induce panic symptoms. During this challenge, enriched air (5–7.5% CO2) is inhaled for up to 20 min, resulting in elevated symptoms of anxiety and panic, especially in those susceptible to panic disorder3,4,5,6,7. Although effective for identifying panic susceptibility (i.e., elevated psychophysiological arousal and intense feelings of fear/anxiety in response to the CO2 administration), little is known about how CO2-induced panic symptoms relate to fear and anxiety.
Responses to threats are heterogeneous. One recognized distinction is that between fear, an emergency reaction to a proximal and/or predictable threat, and anxiety, a more sustained state of apprehension in response to a distal and/or unpredictable threat8,9, which are mediated by distinct core neural systems9. Acute fear is supported by the amygdala, while sustained anxiety is supported by the bed nucleus of the stria terminalis (BNST)9. There is evidence to suggest that panic symptoms may be more related to sustained anxiety than to acute fear. For instance, panic disorder patients10,11 and individuals with a history of panic attack12 show hypersensitivity to unpredictable but not predictable threats, and patients with Urbach–Wiethe disease can experience panic attacks, even without a healthy amygdala13,14. These results suggest that CO2-induced panic symptoms may not be mediated by the canonical acute fear circuit; however, less is known about CO2-induced panic and sustained anxiety. The so-called “NPU threat task” is the gold standard for experimentally studying fear and anxiety in humans15, and is part of the Research Domain Criteria matrix put forth by the National Institute of Mental Health (NIMH)16. The NPU threat task consists of periods of No shock, Predictable shocks, and Unpredictable shocks. The predictable condition can evoke acute fear, while the unpredictable condition can evoke anxiety.
In spite of these core neural differences, fear and anxiety also engage common neural systems. For instance, both acute fear and sustained anxiety recruit a large network of structures important for emotional expression (fear network; FN), including the dorsal anterior cingulate cortex/dorsomedial prefrontal cortex (dmPFC), the anterior insula, and the thalamus17,18,19,20,21,22,23,24. Similarly, both fear and anxiety disengage regions of the default mode network (DMN), which may play a key role in planning and self-referential processing25,26,27,28. Finally, fear and anxiety are both regulated by similar cognitive systems29,30,31,32,33,34,35,36,37,38,39,40,41,42. For instance, tasks that engage regions of the cognitive control network, such as the dorsolateral prefrontal cortex (dlPFC), reduce fear and anxiety possibly through implicit emotion regulation43,44,45,46,47. Therefore, although the core systems mediating fear and anxiety are different, these emotional states rely on similar auxiliary systems.
Because the amygdala may not be necessary for panic, it is clear that panic, like anxiety, is mediated by a core system separate from the fear system13,14. Given that individuals with panic disorder or a history of panic attack show heightened anxiety to unpredictable threat10,11, one might hypothesize that anxiety and panic share common core systems. In addition, the contributions of these other, auxiliary, systems to the expression of panic symptoms are less clear. Therefore, one might hypothesize that the ability to engage, disengage, and regulate activity in these canonical networks (e.g., FN, DMN, cognitive control, etc.) may represent a core component of these similar emotional states, and thus the disorders are characterized by overexpression of these states48,49. Therefore, the purposes of this study are to (1) determine the degree to which panic-susceptible individuals show elevated measures of fear and anxiety during the NPU threat task, and (2) determine the degree to which panic-susceptible individuals show abnormal reactivity in the neural systems that mediate or regulate fear and anxiety. Accordingly, we recruited healthy subjects, and screened them for panic susceptibility using a maintained 7.5% CO2 challenge, and then used their self-report and physiological responses to predict behavioral and neural responses in the NPU threat task.
Materials and methods
Participants
Eighty-four healthy, right-handed volunteers from the Washington DC area were recruited by advertisements, word of mouth, and medical referrals into the present study. Sample size was maximized based on available scanning resources, and it surpassed the minimum sample size needed to obtain the effects described in Schmitz and Grillon15. Potential participants were given a comprehensive evaluation by the clinical staff at the National Institute of Health Clinical Center in Bethesda, MD. Participants were excluded if they had (1) current or past history of any axis I psychiatric disorder as assessed by SCID-I/NP (2) first-degree family history of mania, schizophrenia, or other psychoses, (3) current or past history of any psychotropic or illicit drug use confirmed by a negative urine screen, (4) brain abnormalities on MRI as assessed by a licensed radiologist, or (5) medical conditions or that interfered with the objectives of the study.
Nine participants withdrew or could not be scheduled for all three experimental sessions. Two participants were excluded on the basis of performance (e.g., falling asleep or not paying attention), six participants were excluded on the basis of contaminated data sets (e.g., movement, excessive noise, etc.), and 4 participants were excluded on the basis of missing self-reports, leaving 63 completers (28 female; M (SD): 27 (5.7) yo). All participants gave written informed consent approved by the NIMH Combined Neuroscience Institutional Review Board and received financial compensation.
Procedure
Overview
The purpose of this study was to identify relationships between panic susceptibility and psychological, psychophysiological, and neural measures of fear and anxiety. To characterize panic susceptibility, we administered a 7.5% CO2 challenge and collected several psychological and psychophysiological measures of panic symptomology. To characterize the psychological and psychophysiological aspects of fear and anxiety, we administered a laboratory version of the NPU threat task, during which shocks are delivered predictably or unpredictably. Fear was defined as the response to the cue during the predictable blocks, and anxiety was defined as the response during the unpredictable blocks compared to the neutral blocks. Finally, to characterize the neural aspects of fear and anxiety, we administered a functional magnetic resonance imaging (fMRI) version of the NPU threat task. The study consisted of two visits on separate days. During the laboratory visit, subjects completed the CO2 challenge and NPU threat task. During the MRI visit, subjects completed the NPU threat task without startle probes. Separate NPU visits for psychophysiology and fMRI recordings were conducted because the hardware to administer the white-noise probes or collect the appropriate psychophysiological measures (i.e., the acoustic startle response) in the MRI scanner were not available. Visit and NPU block orders were counterbalanced across participants. Additional methodological details can be found in the Supplementary Methods.
CO2 challenge procedure
Subjects were seated and affixed with a silicone facemask (Hans Rudolph Inc.) that covered their mouth and nose. The facemask was connected through gas-impermeable tubing to a non-diffusing gas bag (Hans Rudolph Inc.), via a three-way stop cock, which allowed the researcher to manually switch from room air to the 7.5% CO2 mixture. Once fitted with mask, participants breathed 5 min of room air (Pre-CO2), followed by 8 min of 7.5% CO2 (CO2-inhalation), followed by 5 min of room air (recovery). The mask was removed after the recovery period. Subjects were blind to CO2 onset, but informed that they could withdraw at any point.
NPU laboratory session
Electrodes to measure the startle response and deliver the shocks were attached to the subject, and the subject was given headphones for the startle response. Next, the subjects underwent a standard startle habituation block where they received nine unsignaled white-noise presentations (used to probe the acoustic startle reflex). Afterward, a shock workup procedure was done to set the level of shock (used to induce anxiety).
The NPU task consisted of three types of blocks: Neutral (N), Predictable (P), and Unpredictable (U). During each block, an 8-s cue was presented three times. The cues were simple geometric shapes with three, four, or five sides that were colored orange (RGB color: 255, 128, 0), teal (RGB color: 0, 128, 255), or purple (RGB color: 128, 0, 255). Different cues were used for the N, P, and U blocks, and both the color and the shape of the cues were determined randomly for each subject at the start of the experiment. During the N blocks, subjects were informed that they would not receive a shock, regardless of the presence or absence of the cue. During the P blocks, subjects were informed that they could receive a shock, but only during the cue. During the U blocks, subjects were informed that they could receive a shock anytime. This information was provided both before the experiment and throughout each block via text prompts. Throughout, subjects were informed that they would receive periodic white-noise presentations (for startle measurements). Subjects were instructed to continuously rate their anxiety using an online likert-type scale.
There were two runs consisting of alternating N, P, and U blocks with the following sequences: PNUNUNP or UNPNPNU. Six white-noise probes were administered (three during the cue and three during the Intertrial Interval (ITI)). Ten shocks were randomly distributed across the predictable (during the cue) and unpredictable blocks, with five shocks occurring in each block type. The run order was counterbalanced across subjects.
NPU fMRI session
Subjects were prepped to go into the MRI scanner (given earplugs, situated on the scanner table, etc). Afterward, a shock workup procedure was done to set the level of shock. Once situated, subjects received a structural scan (T1), an 8-min pre-NPU resting EPI scan, 2 EPI scans during the NPU threat task, and an 8-min post-NPU resting EPI scan. The procedure for the NPU threat task was identical to that of the laboratory session, with the exception that no startle probes were presented. The resting scans were not analyzed for this study.
Materials
For the CO2 challenge, we collected several psychological (Diagnostic Symptom Questionnaire (DSQ)1, Subjective Units of Distress Scale (SUDS)50) and psychophysiological (tidal lung volume (LV), capnography (CO2%), heart rate (HR), heart rate variability (HRV), skin conductance, and respiratory rate (RR)) measures of panic symptomology. During the NPU laboratory session we collected startle and anxiety ratings. During the NPU fMRI session we collected BOLD and analyzed the cue-evoked activity for the N, P, and U conditions. For a full discussion of the methods see the Supplementary Methods.
Analysis
The analysis strategy was 2-fold. First, we considered the effects of each manipulation on the corresponding dependent measures. For the CO2 challenge we examined the change in each measure from Pre-CO2 period to CO2 period. For the NPU laboratory session, we identified behavioral measures that reflected sustained anxiety during the unpredictable blocks by calculating anxiety-potentiated startle (APS) and anxiety-potentiated ratings (APR). We also calculated behavioral measures that reflected acute fear by calculating fear-potentiated startle (FPS) and fear-potentiated ratings (FPRs). For the NPU fMRI session, we conducted a one-way ANOVA on the cue-evoked betas, corrected for multiple comparisons using cluster thresholding, and examined the post hoc pairwise comparisons at the cluster level.
Next, we examined the relationship between the measures of each experiment. The goal was to explain as much variability in the data using the fewest possible comparisons. Accordingly, we first reduced the data from each experiment using a principal component analysis (PCA), and used the component scores (regressors of interest) in a general linear model (GLM) to predict anxiety and/or panic symptoms for the two remaining experiments. Finally, to characterize each GLM we combined the PCA item loadings for each component with that component’s coefficient, yielding weighted coefficients for each item entered into the GLM. For a complete discussion of data processing and analysis, see the Supplementary Materials.
Results
CO2
To determine the effectiveness of the CO2 challenge, we created CO2−Pre-CO2 difference scores for variables reflecting: breathing (RR, LV, end-tidal CO2), physiological arousal (HR, HRV, and EDA), subjective panic symptoms (DSQ), and subjective emotional state (SUDS: Unpleasant, Anxious, Awake, Tense; see Fig. 1). As expected, subjects showed increased breathing (RR: t(62) = 8.24; p < 0.001; d = 1.05, LV: t(62) = 13.57; p < 0.001; d = 1.72, CO2: t(62) = 22.41; p < 0.001; d = 2.85), increased arousal (HR: t(62) = 8.04; p < 0.001; d = 1.02, HRV: t(62) = −7.75; p < 0.001; d = −0.98, EDA: t(62) = 8.46; p < 0.001; d = 1.07), elevated symptoms of panic (DSQ: t(62) = 8.01; p < 0.001; d = 1.02), and an increase in negative emotional state (Unpleasant: t(62) = 9.04; p < 0.001; d = 1.15, Anxious: t(62) = 9.6; p < 0.001; d = 1.22, Awake: t(62) = 2.08; p = 0.042; d = 0.26, Tense: t(62) = 8.88; p < 0.001; d = 1.13).

a Schematic demonstrating timeline of the CO2 challenge. During the pre-CO2 and recovery periods, subjects breathe room air. During the CO2 administration period, subjects breathe room air enriched with 7.5% CO2. b–k Physical b–g and psychological h–l symptoms of CO2 administration. Bars represent the mean CO2 − Pre-CO2 values ± SEM
NPU laboratory
To determine the effectiveness of the laboratory session of the NPU threat task, we analyzed the online ratings and startle magnitudes for the N, P, and U blocks using 3 (Block: N, P, U) × 2 (Interval: Cue vs. ITI) repeated-measures ANOVA (See Fig. 2). For both ratings and startle, we found a significant main effect for both block (Ratings: F(2, 124) = 97.99; p < 0.001, Startle: F(2, 124) = 73.46; p < 0.001) and interval (Ratings: F(1, 62) = 54.14; p < 0.001, Startle: F(1, 62) = 95.58; p < 0.001), as well as a significant Block × Interval Interaction (Ratings: F(2, 124) = 48.25; p < 0.001, Startle: F(2, 124) = 41.81; p < 0.001).

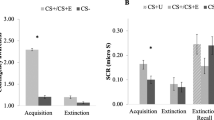
a Schematic demonstrating design of the NPU paradigm. Colored lines indicate blocks of neutral, predictable, and unpredictable threat. Geometric shapes indicate visual cues presented during blocks. Lightning bolts represent timing of shock delivery. b Average anxiety ratings during the fMRI session for the neutral (N), predictable (P), and unpredictable (U) blocks when the cue was present (Cue) or absent (ITI) from the screen. c Startle magnitude (t-scores) during the laboratory session for the neutral (N), predictable (P), and unpredictable (U) blocks when the cue was present (Cue) or absent (ITI) from the screen. d Average anxiety ratings during the laboratory session for the neutral (N), predictable (P), and unpredictable (U) blocks when the cue was present (Cue) or absent (ITI) from the screen. Bars represent the mean ± SEM
To characterize the interaction, we quantified fear and anxiety from the ratings and startle measures. For fear, we subtracted the rating (i.e., FPR) and startle (i.e., FPS) magnitude during the predictable ITI period from the predictable cue period. For anxiety, we subtracted the rating (i.e., APR) and startle (i.e., APS) magnitude during the unpredictable blocks from the neutral blocks during both the cue and ITI. As expected, both ratings and startle increased during the predictable cue compared to the predictable ITI, indicating an acute increase in fear brought on by the predictable cue (FPR: t(62) = 7.36; p < 0.001; d = 0.93, FPS: t(62) = 10.3; p < 0.001; d = 1.3). Similarly, both ratings and startle increased during the unpredictable cue (APR-CUE: t(62) = 11; p < 0.001, d = 1.39; APS-CUE: t(62) = 7.78; p < 0.001; d = 0.98) and ITI periods (APR-ITI: t(62) = 11.1; p < 0.001; d = 1.4, APS-ITI: t(62) = 8.37; p < 0.001; d = 1.05), indicating a sustained increase in anxiety that was present for the entire unpredictable blocks.
NPU fMRI session
For the fMRI data, we performed one-way (N, P, U) repeated-measures voxelwise ANOVA on the cue-evoked activity, and extracted the clusters that survived correction for multiple comparisons (see Supplementary Table 1). We then grouped these clusters into two co-activation networks based on their pattern of activity across conditions (see Fig. 3).

a Statistical parametric map and corresponding graphic representation for regions of the fear network (FN). b Statistical parametric map and corresponding graphic representation for regions of the DMN. c Statistical parametric map and corresponding graphic representation for regions of the right dorsolateral prefrontal cortex (dlPFC). Bars represent the mean ± SEM
Regions in the first co-activation network (FN), including the dmPFC and bilateral insula, showed a pattern of activity consistent with fear only (i.e., P ≠ N and U). Specifically, these regions showed significantly more activity to the predictable than the unpredictable cue (P > U: t(62) = 7.99; p < 0.001; d = 1) or neutral cue (P > N: t(62) = 11.75; p < 0.001; d = 1.45).
Regions in the second co-activation network (DMN), including the ventromedial prefrontal cortex and posterior cingulate cortex, showed a pattern of activity consistent with both fear and anxiety (i.e., P and U ≠ N). However, unlike the FN, there was significantly less activity to the predictable cue (P > N: t(62) = −7.89; p < 0.001; d = −0.97) and the unpredictable cue (U > N: t(62) = −4.96; p < 0.001; d = −0.62) compared to the neutral cue. Although not reported, the pattern of results for each cluster matches that of the corresponding co-activation network.
The final cluster (Right dlPFC) showed a pattern of activity consistent with both fear and anxiety (i.e., P and U ≠ N), but unlike the regions in the DMN this cluster exhibited significantly more activity to the predictable cue (P > N: t(62) = 7.28; p < 0.001; d = 0.91) and unpredictable cue (U > N: t(62) = 4.38; p < 0.001; d = 0.55) compared to the neutral cue.
We did not observe any significant effects in the BNST.
PCA
To identify regressors of interest, we conducted independent PCAs including all variables from a given experiment. For the CO2 experiment, we entered 26 variables into the PCA, and identified six components with an eigenvalue >1 (see Fig. 4a). These six components explained 69.09% of the variability. For the NPU laboratory session, we entered 12 variables into the PCA, and identified three components with an eigenvalue >1 (see Supplementary Fig. 2). These three components explained 69.77% of the variability. For the NPU fMRI session, we entered 33 variables into the PCA, and identified 7 components with an eigenvalue >1 (see Supplementary Fig. 2). These seven components explained 79.25% of the variability.

a Screenplot demonstrating outcome of the principal components analyses for the CO2 challenge. Components with an eigenvalue >1 are considered signal components, while those with an eigenvalue <1 are considered noise components. b Variability (r 2) in dependent measures from the NPU sessions accounted for by the signal components in the CO2 challenge. Filled bars are significant after correcting for multiple comparisons. Hatched bars are trends, but not significant after correcting for multiple comparisons. c Weighted beta coefficients showing contributions of specific items from the CO2 challenge to the PCA/regression model predicting anxiety-related dlPFC activity. d Correlation between anxiety-related dlPFC activity and anxiety (as derived via PCA from NPU startle and ratings during fMRI and laboratory sessions)
GLMs
To determine whether the primary outcome measures of each experiment were affected by individual differences in responding in the other experiments, we conducted a series of GLMs (One per measure, see Supplementary Fig. 3) using the subject scores for the signal components from one experiment to predict the outcome measures from another experiment. This was done in a systematic fashion, whereby the signal components from each experiment were used to predict each outcome measure for the remaining experiments. The subsequent r 2 values are plotted in Supplementary Fig. 3. Although several of these GLMs were significant at the 0.05 level (see hatched bars in Supplementary Fig. 3), only one GLM (CO2 challenge components → Anxiety-related dlPFC activity) was significant after correcting for multiple comparisons (see shaded bar in Fig. 4b).
Weighted beta coefficients
To characterize the relationship between predictor variables from the CO2 challenge and anxiety-related dlPFC activity, we computed weighted coefficients for this GLM (see Fig. 4c). CO2 challenge items related to fear or negative affect tended to load negatively on anxiety-related dlPFC activity (f(6, 56) = 4.02; p = 0.002; FDR = 0.016; r 2 = 0.3), suggesting that individuals with high anxiety-related dlPFC activity report less fear during the CO2 challenge. A similar but less robust pattern was observed for fear-related dlPFC activity (f(6, 56) = 2.35; p = 0.043; FDR = 0.17; r 2 = 0.2; see Supplementary Fig. 4).
Anxiety/dlPFC correlations
Because individuals who exhibited larger anxiety-related dlPFC responses during the NPU fMRI session reported less anxiety during the CO2 challenge, we hypothesized that these dlPFC responses may regulate anxiety more generally. Thus, we correlated anxiety ratings from the unpredictable condition during both sessions and startle from the NPU Laboratory session with dlPFC responses from the NPU fMRI session. For all measures we calculated Unpredictable > Neutral difference scores. Because the dlPFC responses were cue-evoked, we included separate scores for the cue and ITI periods for the anxiety ratings and startle measures. Importantly, across measures (Ratings vs. Startle), studies (fMRI session vs. Laboratory session), and intervals (Cue vs. ITI), the correlations with anxiety-related dlPFC responses were negative (see Supplementary Table 2). Although many of these correlations were only trends, the pattern is consistent across measures, and these measures themselves were likely correlated. Therefore, we combined the measures using a PCA and extracted a single value component to anxiety (eigenvalue = 3.6). As expected, the anxiety component was significantly negatively correlated with anxiety-related dlPFC activity (r(62) = −0.29; p = 0.023; see Fig. 4d). When applying a similar approach to fear and fear-related dlPFC activity, no significant correlations were found (all p values > 0.05).
Discussion
The purpose of this study was to determine the degree to which panic susceptibility is related to (1) fear and anxiety during the NPU threat task and (2) reactivity in the neural systems that mediate fear and anxiety. Accordingly, we exposed individuals to a 7.5% CO2 challenge and two versions (laboratory and fMRI) of the NPU threat task. Contrary to our first hypothesis, we did not find evidence that panic symptoms were mediated by the same core neural system as anxiety. However, we did find evidence that panic symptoms to CO2 may be regulated by the same neural system that regulates anxiety to unpredictable threat. When comparing across experimental sessions, we found that CO2-related behavioral changes were associated only with dlPFC activity during the unpredictable cue (see Fig. 4b). The activity of the dlPFC is commonly considered to mediate cognitive control51,52, and our results suggest that the dlPFC regulates anxiety in these paradigms48. Weighted coefficients from our analysis showed that fear-related DSQ symptom items negatively loaded onto dlPFC activity (see Fig. 4c). Similarly, anxiety-related dlPFC was negatively correlated with anxiety during the NPU sessions (see Fig. 4d). Together, these results suggest that panic symptoms and anxiety are regulated by the same prefrontal cognitive control system48.
In addition to this novel finding, we replicate many previous reports about the CO2 challenge and the NPU threat task. During the CO2 challenge, subjects showed increased respiration, physiological arousal, and self-reported anxiety (see Fig. 1). During the laboratory NPU session, subjects showed the traditional pattern of elevated startle and self-reported anxiety during the predictable cue (fear), and unpredictable cue and ITI periods (anxiety)8,15,53,54,55 (see Fig. 2). During the NPU fMRI session, subjects showed distinct patterns of BOLD activity related to fear and anxiety22,56,57,58,59,60,61 (see Fig. 3). During both predictable and unpredictable cues, subjects showed decreased DMN activity (see Fig. 3b), and increased dlPFC activity (see Fig. 3c). However, only the predictable cue increased FN activity (see Fig. 3a). This FN result is consistent with the fact that only the predictable cue informed the probability of shock15.
Previous research has shown that panic attacks are not necessarily mediated by the same mechanisms as fear14,62. However, there is evidence that history of panic attacks is related to startle magnitude during unpredictable threat10,11,12. There are two possible explanations for this observation. First, panic susceptibility may be driven by elevated responding in anxiety-related neural systems22,56,57,58,59,60,61. Alternatively, panic susceptibility may be driven by attenuated responding in anxiety-regulating neural systems63,64,65. We found that panic symptoms can predict dlPFC activity, which is negatively associated with anxiety, which supports the second hypothesis, and suggests that the dlPFC regulates panic symptoms and anxiety. Consistent with this, anxiety patients show dlPFC deficits during complex working memory (WM) tasks27. In contrast, we found no evidence that panic symptoms are associated with anxiety-related regions, which fails to support the expression hypothesis (see Fig. 4b). Thus, more work is needed to understand the distinct neural systems mediating the expression of anxiety and panic.
These findings can explain the previously counterintuitive finding that CO2 administration actually reduces startle magnitude66,67,68. According to our results, one could argue that the dlPFC is a common regulatory system engaged by 7.5% CO2 and by unpredictable threat because these challenges evoke a similar defensive response. Thus, evoking either defensive response should lead to the regulation of both responses. According to this hypothesis, startle is reduced during CO2 administration because 7.5% CO2 administration engages the dlPFC, which regulates the ongoing activity in the neural system engaged by unpredictable threat. Therefore, it should also be possible to reduce CO2-related panic symptoms using sustained unpredictable threat, as a proof of concept. This hypothesis is testable within the context of the rapid 35% CO2 challenge. In this paradigm, subjects inhale a single breath of air with 35% CO2, which results in panic attacks in susceptible individuals69,70,71. Therefore, using unpredictable threat to engage the system that mediates anxiety should reduce the likelihood of experiencing a panic attack in this paradigm.
It may also be possible to test the regulation hypothesis using other techniques to drive dlPFC activity72,73,74,75,76,77,78,79,80,81,82. We have shown previously that WM, known to activate the dlPFC, is sufficient to reduce APS during threat83,84. We know of no studies examining the effect of WM on panic symptoms. Future studies might accomplish this by administering single breaths of 35% CO2 during periods of low vs. high WM load69,70,71. According to the regulation hypothesis, subjects should experience fewer panic attacks during high WM blocks compared to low WM blocks. The N-back WM task would be ideal because it provides long durations of steady-state WM engagement, where WM load can be parametrically manipulated within subjects79,80,81,82. It may also be possible to test the regulation hypothesis using noninvasive neuromodulation. For instance, one could administer single breaths of 35% CO2 while the subject receives electrical (transcranial direct current stimulation; tDCS72,73,74) or magnetic (transcranial magnetic stimulation; TMS75,76,77,78) to the right dlPFC. According to the regulatory hypothesis, subjects should experience fewer panic attacks during excitatory (i.e., anodal tDCS or high-frequency TMS) compared to inhibitory (i.e., cathodal tDCS or low-frequency TMS) or sham stimulation of the dlPFC.
Strengths and limitations
There were a number of strengths and limitations with current work that should be noted. Among the primary strengths, we used well-validated, experimental, translational techniques for inducing symptoms of fear (predictable shock threat), anxiety (unpredictable shock threat), and panic (7.5% CO2 inhalation)4,15, and included an adequate sample size (n = 63) to test the hypotheses. Among the primary limitations, we did not directly assay neural activity during the CO2 challenge, and we did not report the findings related to sustained anxiety from the unpredictable blocks in the fMRI study. For a full discussion of these strengths and limitations, see the Supplementary Materials.
Conclusions
The purpose of this study was to determine the degree to which panic symptoms correlated with fear, anxiety, and the neural systems that mediate/regulate fear and anxiety. We found evidence that panic symptoms and anxiety may be regulated by similar prefrontal cognitive control mechanisms. Accordingly, these results raise several testable hypotheses about the effect of cognitive control on panic symptoms, and warrant future studies on this topic.
References
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: Dsm-5 (Amer Psychiatric Pub Incorporated, Arlington, VA, 2013).
Battaglia, M., Ogliari, A., D’Amato, F. & Kinkead, R. Early-life risk factors for panic and separation anxiety disorder: insights and outstanding questions arising from human and animal studies of CO2 sensitivity. Neurosci. Biobehav. Rev. 46, 455–464 (2014).
Bailey, J. E., Kendrick, A., Diaper, A., Potokar, J. P. & Nutt, D. J. A validation of the 7.5% CO2 model of GAD using paroxetine and lorazepam in healthy volunteers. J. Psychopharmacol. 21, 42–49 (2007).
Bailey, J. E., Dawson, G. R., Dourish, C. T. & Nutt, D. J. Validating the inhalation of 7.5% CO2 in healthy volunteers as a human experimental medicine: a model of generalized anxiety disorder (GAD). J. Psychopharmacol. 25, 1192–1198 (2011).
Seddon, K. et al. Effects of 7.5% CO2 challenge in generalized anxiety disorder. J. Psychopharmacol. 25, 43–51 (2011).
Bailey, J. E., Argyropoulos, S. V., Kendrick, A. H. & Nutt, D. J. Behavioral and cardiovascular effects of 7.5% CO2 in human volunteers. Depress. Anxiety 21, 18–25 (2005).
Bystritsky, A., Craske, M., Maidenberg, E., Vapnik, T. & Shapiro, D. Autonomic reactivity of panic patients during a CO2 inhalation procedure. Depress. Anxiety 11, 15–26 (2000).
Grillon, C. Models and mechanisms of anxiety: evidence from startle studies. Psychopharmacology 199, 421–437 (2008).
Davis, M., Walker, D. L., Miles, L. & Grillon, C. Phasic vs sustained fear in rats and humans: role of the extended amygdala in fear vs anxiety. Neuropsychopharmacology 35, 105–135 (2010).
Grillon, C. et al. Increased anxiety during anticipation of unpredictable but not predictable aversive stimuli as a psychophysiologic marker of panic disorder. Am. J. Psychiatry 165, 898–904 (2008).
Grillon, C., Ameli, R., Goddard, A., Woods, S. W. & Davis, M. Baseline and fear-potentiated startle in panic disorder patients. Biol. Psychiatry 35, 431–439 (1994).
Grillon C. et al. Distinct responses to predictable and unpredictable threat in anxiety pathologies: effect of panic attack. Biol. Psychiatry Cogn. Neurosci. Neuroimaging 1–7 (2016).Grillon C, O’Connell K, Lieberman L, Alvarez G, Geraci M, Pine DS et al. Distinct Responses to Predictable and Unpredictable Threat in Anxiety Pathologies: Effect of Panic Attack. Biol Psychiatry Cogn Neurosci Neuroimaging 2, 575-581 (2016).
Khalsa, S. S. et al. Panic anxiety in humans with bilateral amygdala lesions: pharmacological induction via cardiorespiratory interoceptive pathways. J. Neurosci. 36, 3559–3566 (2016).
Feinstein, J. S. et al. Fear and panic in humans with bilateral amygdala damage. Nat. Neurosci. 16, 270–272 (2013).
Schmitz, A. & Grillon, C. Assessing fear and anxiety in humans using the threat of predictable and unpredictable aversive events (the NPU-threat test). Nat. Protoc. 7, 527–532 (2012).
Insel, T. et al. Research Domain Criteria (RDoC): toward a new classification framework for research on mental disorders. Am. J. Psychiatry 167, 748–751 (2010).
Fullana, M. A. et al. Neural signatures of human fear conditioning: an updated and extended meta-analysis of fMRI studies. Mol. Psychiatry 21, 500–508 (2015).
Vytal, K. E., Overstreet, C., Charney, D. R., Robinson, O. & Grillon, C. Sustained anxiety increases amygdala-dorsomedial prefrontal coupling: a mechanism for maintaining an anxious state in healthy adults. J. Psychiatry Neurosci. 39, 1–9 (2014).
Hasler, G. et al. Cerebral blood flow in immediate and sustained anxiety. J. Neurosci. 27, 6313–6319 (2007).
Etkin, A. & Wager, T. D. Functional neuroimaging of anxiety: a meta-analysis of emotional processing in PTSD, social anxiety disorder, and specific phobia. Am. J. Psychiatry 164, 1476–1488 (2007).
Baur, V., Hänggi, J., Langer, N. & Jäncke, L. Resting-state functional and structural connectivity within an insula-amygdala route specifically index state and trait anxiety. Biol. Psychiatry 73, 85–92 (2013).
Andreatta, M. et al. Initial and sustained brain responses to contextual conditioned anxiety in humans. Cortex 63, 352–363 (2015).
Robinson, O., Charney, D. R., Overstreet, C., Vytal, K. E. & Grillon, C. The adaptive threat bias in anxiety: amygdala-dorsomedial prefrontal cortex coupling and aversive amplification. Neuroimage 60, 523–529 (2012).
Wheelock, M. D. et al. Threat-related learning relies on distinct dorsal prefrontal cortex network connectivity. Neuroimage 102, 904–912 (2014).
Tao, Y. et al. The structural connectivity pattern of the default mode network and its association with memory and anxiety. Front. Neuroanat. 9, 152 (2015).
Broyd, S. J. et al. Default-mode brain dysfunction in mental disorders: a systematic review. Neurosci. Biobehav. Rev. 33, 279–296 (2009).
Balderston, N. L. et al. Anxiety patients show reduced working memory related Dlpfc activation during safety and threat. Depress. Anxiety 12, 1–12 (2016).
Tomasi, D. & Volkow, N. D. Functional connectivity hubs in the human brain. Neuroimage 57, 908–917 (2011).
Reinholdt-Dunne, M. L., Mogg, K. & Bradley, B. P. Attention control: relationships between self-report and behavioural measures, and symptoms of anxiety and depression. Cogn. Emot. 9931, 1–11 (2012).
Reinholdt-Dunne, M. L., Mogg, K. & Bradley, B. P. Effects of anxiety and attention control on processing pictorial and linguistic emotional information. Behav. Res. Ther. 47, 410–417 (2009).
Grillon, C., Robinson, O., Mathur, A. & Ernst, M. Effect of attention control on sustained attention during induced anxiety. Cogn. Emot. 9931, 1–13 (2015).
Braver, T. S., Cole, M. W. & Yarkoni, T. Vive les differences! Individual variation in neural mechanisms of executive control. Curr. Opin. Neurobiol. 20, 242–250 (2010).
Derryberry, D. & Reed, Ma Anxiety-related attentional biases and their regulation by attentional control. J. Abnorm. Psychol. 111, 225–236 (2002).
Eysenck, M. W., Derakshan, N., Santos, R. & Calvo, M. G. Anxiety and cognitive performance: attentional control theory. Emotion 7, 336–353 (2007).
Berggren, N. & Derakshan, N. Attentional control deficits in trait anxiety: why you see them and why you don’t. Biol. Psychol. 92, 440–446 (2013).
Berggren, N. & Derakshan, N. The role of consciousness in attentional control differences in trait anxiety. Cogn. Emot. 27, 923–931 (2013).
Coombes, S. A., Higgins, T., Gamble, K. M., Cauraugh, J. H. & Janelle, C. M. Attentional control theory: anxiety, emotion, and motor planning. J. Anxiety Disord. 23, 1072–1079 (2009).
Armstrong, T., Zald, D. H. & Olatunji, B. O. Attentional control in OCD and GAD: specificity and associations with core cognitive symptoms. Behav. Res. Ther. 49, 756–762 (2011).
Price, R. B., Eldreth, Da & Mohlman, J. Deficient prefrontal attentional control in late-life generalized anxiety disorder: an fMRI investigation. Transl. Psychiatry 1, e46 (2011).
Najmi, S., Amir, N., Frosio, K. E. & Ayers, C. The effects of cognitive load on attention control in subclinical anxiety and generalised anxiety disorder. Cogn. Emot. 9931, 1–14 (2014).
Najmi, S., Kuckertz, J. M. & Amir, N. Attentional impairment in anxiety: inefficiency in expanding the scope of attention. Depress. Anxiety 29, 243–249 (2012).
Morrison, A. S. & Heimberg, R. G. Attentional control mediates the effect of social anxiety on positive affect. J. Anxiety Disord. 27, 56–67 (2013).
Cieslik, E. C. et al. Is there one DLPFC in cognitive action control? Evidence for heterogeneity from Co-activation-based parcellation. Cereb. Cortex 23, 2677–2689 (2013).
Basten, U., Stelzel, C. & Fiebach, C. J. Trait anxiety and the neural efficiency of manipulation in working memory. Cogn. Affect. Behav. Neurosci. 12, 571–588 (2012).
Harding, I. H., Yücel, M., Harrison, B. J., Pantelis, C. & Breakspear, M. Effective connectivity within the frontoparietal control network differentiates cognitive control and working memory. Neuroimage 106, 144–153 (2015).
Fales, C. L. et al. Anxiety and cognitive efficiency: differential modulation of transient and sustained neural activity during a working memory task. Cogn. Affect. Behav. Neurosci. 8, 239–253 (2008).
Peers, P. V., Simons, J. S. & Lawrence, A. D. Prefrontal control of attention to threat. Front. Hum. Neurosci. 7, 24 (2013).
Cole, M. W., Repovš, G. & Anticevic, A. The frontoparietal control system: a central role in mental health. Neuroscientist 20, 652–664 (2014).
Sylvester, C. M. et al. Functional network dysfunction in anxiety and anxiety disorders. Trends Neurosci. 35, 527–535 (2012).
Wolpe J. The practice of behavior therapy, 2nd ed. Pergamon: New York, NY, 1973.
Levy, B. J. & Anderson, M. C. Purging of memories from conscious awareness tracked in the human brain. J. Neurosci. 32, 16785–16794 (2012).
Koechlin, E., Ody, C. & Kouneiher, F. The architecture of cognitive control in the human prefrontal cortex. Science 302, 1181–1185 (2003).
Schmitz, A. et al. Measuring anxious responses to predictable and unpredictable threat in children and adolescents. J. Exp. Child Psychol. 110, 159–170 (2011).
Nelson, B. D., Hajcak, G. & Shankman, S. A. Event-related potentials to acoustic startle probes during the anticipation of predictable and unpredictable threat. Psychophysiology 52, 887–894 (2015).
Kaye, J. T., Bradford, D. E. & Curtin, J. J. Psychometric properties of startle and corrugator response in NPU, affective picture viewing, and resting state tasks. Psychophysiology 53, 1241–1255 (2016).
Robinson, O., Krimsky, M. & Grillon, C. The impact of induced anxiety on response inhibition. Front. Hum. Neurosci. 7, 69 (2013).
Robinson, O. et al. Anxiety-potentiated amygdala–medial frontal coupling and attentional control. Transl. Psychiatry 6, e833 (2016).
Alvarez, R. P., Chen, G., Bodurka, J., Kaplan, R. & Grillon, C. Phasic and sustained fear in humans elicits distinct patterns of brain activity. Neuroimage 55, 389–400 (2011).
Cornwell, B. R., Echiverri, A. M., Covington, M. F. & Grillon, C. Modality-specific attention under imminent but not remote threat of shock. Psychol. Sci. 19, 615–622 (2008).
Gold, A. L., Morey, Ra & McCarthy, G. Amygdala-prefrontal cortex functional connectivity during threat-induced anxiety and goal distraction. Biol. Psychiatry 77, 1–9 (2014).
Torrisi, S. et al. The neural basis of improved cognitive performance by threat of shock. Soc. Cogn. Affect. Neurosci. 11, 1677–1686 (2016).
Wiest, G., Lehner-Baumgartner, E. & Baumgartner, C. Panic attacks in an individual with bilateral selective lesions of the amygdala. Arch. Neurol. 63, 1798–1801 (2006).
Forster, S., Nunez Elizalde, A. O., Castle, E., Bishop, S. J. & Elizalde, A. O. N. Unraveling the Anxious Mind: Anxiety, Worry, and Frontal Engagement in Sustained Attention Versus Off-Task Processing. Cereb. Cortex 25, 609–618 (2015).
Ironside, M., O’Shea, J., Cowen, P. J. & Harmer, C. J. Frontal cortex stimulation reduces vigilance to threat: implications for the treatment of depression and anxiety. Biol. Psychiatry 79, 823–830 (2016).
Shackman, A. J. et al. Right dorsolateral prefrontal cortical activity and behavioral inhibition. Psychol. Sci. 20, 1500–1506 (2014).
Pappens, M., De Peuter, S., Vansteenwegen, D., Van den Bergh, O. & Van Diest, I. Psychophysiological responses to CO2 inhalation. Int. J. Psychophysiol. 84, 45–50 (2012).
Ceunen, E., Vlaeyen, J. W. S. & Van Diest, I. Atypical modulation of startle in women in face of aversive bodily sensations. Int. J. Psychophysiol. 88, 157–163 (2013).
Pinkney, V., Wickens, R., Bamford, S., Baldwin, D. S. & Garner, M. Defensive eye-blink startle responses in a human experimental model of anxiety. J. Psychopharmacol. 28, 874–880 (2014).
Nardi, A. E. et al. Psychopathological profile of 35% CO2 challenge test-induced panic attacks: a comparison with spontaneous panic attacks. Compr. Psychiatry 47, 209–214 (2006).
Wetherell, M. A. et al. The four-dimensional stress test: psychological, sympathetic-adrenal-medullary, parasympathetic and hypothalamic-pituitary-adrenal responses following inhalation of 35% CO2. Psychoneuroendocrinology 31, 736–747 (2006).
Battaglia, M. & Perna, G. The 35% CO2 challenge in panic disorder: optimization by receiver operating characteristic (ROC) analysis. J. Psychiatr. Res. 29, 111–119 (1995).
Balconi, M. & Vitaloni, S. The tDCS effect on alpha brain oscillation for correct vs. incorrect object use. The contribution of the left DLPFC. Neurosci. Lett. 517, 25–29 (2012).
Fregni, F. et al. Anodal transcranial direct current stimulation of prefrontal cortex enhances working memory. Exp. Brain Res. 166, 23–30 (2005).
Brunoni, A. R. & Vanderhasselt, M. A. Working memory improvement with non-invasive brain stimulation of the dorsolateral prefrontal cortex: a systematic review and meta-analysis. Brain Cogn. 86, 1–9 (2014).
Rogasch, N. C., Daskalakis, Z. J. & Fitzgerald, P. B. Cortical inhibition of distinct mechanisms in the dorsolateral prefrontal cortex is related to working memory performance: a TMS-EEG study. Cortex 64, 68–77 (2015).
Gratton, C., Lee, T. G., Nomura, E. M. & D’Esposito, M. The effect of theta-burst TMS on cognitive control networks measured with resting state fMRI. Front. Syst. Neurosci. 7, 124 (2013).
Schicktanz, N. et al. Continuous theta burst stimulation over the left dorsolateral prefrontal cortex decreases medium load working memory performance in healthy humans. PLoS ONE 10, 1–10 (2015).
Shajahan, P. M. et al. Left dorso-lateral repetitive transcranial magnetic stimulation affects cortical excitability and functional connectivity, but does not impair cognition in major depression. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 26, 945–954 (2002).
Carlson, S. et al. Distribution of cortical activation during visuospatial n-back tasks as revealed by functional magnetic resonance imaging. Cereb. Cortex 8, 743–752 (1998).
Owen, A. M., McMillan, K. M., Laird, A. R. & Bullmore, E. N-back working memory paradigm: a meta-analysis of normative functional neuroimaging studies. Hum. Brain Mapp. 25, 46–59 (2005).
León-Domínguez, U., Martín-Rodríguez, J. F. & León-Carrión, J. Executive n-back tasks for the neuropsychological assessment of working memory. Behav. Brain Res. 292, 167–173 (2015).
Jaeggi, S. M., Buschkuehl, M., Perrig, W. J. & Meier, B. The concurrent validity of the N-back task as a working memory measure. Memory 18, 394–412 (2010).
Vytal, K. E., Cornwell, B. R., Letkiewicz, A. M., Arkin, N. E. & Grillon, C. The complex interaction between anxiety and cognition: insight from spatial and verbal working memory. Front. Hum. Neurosci. 7, 93 (2013).
Balderston, N. L. et al. Working memory maintenance is sufficient to reduce state anxiety. Psychophysiology 53, 1660–1668 (2016).
Acknowledgments
Financial support of this study was provided by the Intramural Research Program of the National Institute of Mental Health, ZIAMH002798 (ClinicalTrial.gov Identifier: NCT00047853: Protocol ID 02-M-0321).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare that they have no competing financial interests.
Additional information
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Balderston, N.L., Liu, J., Roberson-Nay, R. et al. The relationship between dlPFC activity during unpredictable threat and CO2-induced panic symptoms. Transl Psychiatry 7, 1266 (2017). https://doi.org/10.1038/s41398-017-0006-5
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41398-017-0006-5
This article is cited by
-
Interleaved TMS/fMRI shows that threat decreases dlPFC-mediated top-down regulation of emotion processing
NPP—Digital Psychiatry and Neuroscience (2024)
-
Intermittent theta-burst stimulation to the right dorsolateral prefrontal cortex may increase potentiated startle in healthy individuals
Neuropsychopharmacology (2024)
-
Proof of concept study to develop a novel connectivity-based electric-field modelling approach for individualized targeting of transcranial magnetic stimulation treatment
Neuropsychopharmacology (2022)
-
Low-frequency parietal repetitive transcranial magnetic stimulation reduces fear and anxiety
Translational Psychiatry (2020)
-
Modeling anxiety in healthy humans: a key intermediate bridge between basic and clinical sciences
Neuropsychopharmacology (2019)
