
Abstract
Objective
To decrease invasive mechanical ventilation exposure in the neonatal intensive care unit (NICU) in the first week of life for preterm infants with the global aim of decreasing bronchopulmonary dysplasia (BPD).
Methods
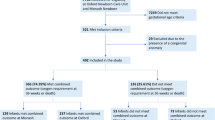
We created a quality improvement (QI) initiative to optimize early non-invasive respiratory support which launched in August 2021. Patients born at <32 weeks gestation and admitted to the NICU on non-invasive respiratory support were included.
Results
Invasive mechanical ventilation exposure decreased from 38 to 25% with evidence of special cause variation beginning in August 2022. Infants born at ≥26 weeks were most impacted, with a 50% reduction, from 34 to 17%. While BPD rates decreased, there has not yet been evidence of special cause variation.
Conclusion
Invasive mechanical ventilation exposure for infants born at <32 weeks gestation decreased following the creation of a QI initiative focused on optimization and standardization of early non-invasive respiratory support.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on SpringerLink
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout


Similar content being viewed by others


References
Stoll BJ, Hansen NI, Bell EF, Walsh MC, Carlo WA, Shankaran S, et al. Trends in care practices, morbidity, and mortality of extremely preterm neonates, 1993-2012. JAMA. 2015;314:1039–51.
Bell EF, Hintz SR, Hansen NI, Bann CM, Wyckoff MH, DeMauro SB, et al. Mortality, in-hospital morbidity, care practices, and 2-year outcomes for extremely preterm infants in the US, 2013-2018. JAMA. 2022;327:248–63.
Stevens TP, Harrington EW, Blennow M, Soll RF. Early surfactant administration with brief ventilation vs. selective surfactant and continued mechanical ventilation for preterm infants with or at risk for respiratory distress syndrome. Cochrane Database Syst Rev. 2007;2007:Cd003063.
Bahadue FL, Soll R. Early versus delayed selective surfactant treatment for neonatal respiratory distress syndrome. Cochrane Database Syst Rev. 2012;11:Cd001456.
Fischer HS, Bührer C. Avoiding endotracheal ventilation to prevent bronchopulmonary dysplasia: a meta-analysis. Pediatrics. 2013;132:e1351–60.
Van Marter LJ, Allred EN, Pagano M, Sanocka U, Parad R, Moore M, et al. Do clinical markers of barotrauma and oxygen toxicity explain interhospital variation in rates of chronic lung disease? The Neonatology Committee for the Developmental Network. Pediatrics. 2000;105:1194–201.
Soll R, Ozek E. Prophylactic protein free synthetic surfactant for preventing morbidity and mortality in preterm infants. Cochrane Database Syst Rev. 2010;2010:Cd001079.
Morley CJ, Davis PG, Doyle LW, Brion LP, Hascoet JM, Carlin JB. Nasal CPAP or intubation at birth for very preterm infants. N Engl J Med. 2008;358:700–8.
Finer NN, Carlo WA, Walsh MC, Rich W, Gantz MG, Laptook AR, et al. Early CPAP versus surfactant in extremely preterm infants. N Engl J Med. 2010;362:1970–9.
Dunn MS, Kaempf J, de Klerk A, de Klerk R, Reilly M, Howard D, et al. Randomized trial comparing 3 approaches to the initial respiratory management of preterm neonates. Pediatrics. 2011;128:e1069–76.
Rojas-Reyes MX, Morley CJ, Soll R. Prophylactic versus selective use of surfactant in preventing morbidity and mortality in preterm infants. Cochrane Database Syst Rev. 2012;3:Cd000510.
Schmölzer GM, Kumar M, Pichler G, Aziz K, O’Reilly M, Cheung PY. Non-invasive versus invasive respiratory support in preterm infants at birth: systematic review and meta-analysis. BMJ. 2013;347:f5980.
Committee on Fetus and Newborn, Papile L-A, Baley JE, Benitz W, Cummings J, Eichenwald E, et al. Respiratory support in preterm infants at birth. Pediatrics. 2014;133:171–4.
Sweet DG, Carnielli V, Greisen G, Hallman M, Ozek E, Te Pas A, et al. European consensus guidelines on the management of respiratory distress syndrome - 2019 update. Neonatology. 2019;115:432–50.
Wright CJ, Sherlock LG, Sahni R, Polin RA. Preventing continuous positive airway pressure failure: evidence-based and physiologically sound practices from delivery room to the neonatal intensive care unit. Clin Perinatol. 2018;45:257–71.
Verder H, Robertson B, Greisen G, Ebbesen F, Albertsen P, Lundstrøm K, et al. Surfactant therapy and nasal continuous positive airway pressure for newborns with respiratory distress syndrome. Danish-Swedish Multicenter Study Group. N Engl J Med. 1994;331:1051–5.
Verder H, Albertsen P, Ebbesen F, Greisen G, Robertson B, Bertelsen A, et al. Nasal continuous positive airway pressure and early surfactant therapy for respiratory distress syndrome in newborns of less than 30 weeks’ gestation. Pediatrics. 1999;103:e24.
Dani C, Bertini G, Pezzati M, Cecchi A, Caviglioli C, Rubaltelli FF. Early extubation and nasal continuous positive airway pressure after surfactant treatment for respiratory distress syndrome among preterm infants <30 weeks’ gestation. Pediatrics. 2004;113:e560–e3.
Vermont Oxford Network Homepage. Available from: https://portal.vtoxford.org/home.
Levesque BM, Burnham L, Cardoza N, Adams M, Cohen R, Mirochnick M, et al. Improving respiratory support practices to reduce chronic lung disease in premature infants. Pediatr Qual Saf. 2019;4:e193.
Bapat R, Nelin L, Shepherd E, Ryshen G, Elgin A, Bartman T. A multidisciplinary quality improvement effort to reduce bronchopulmonary dysplasia incidence. J Perinatol. 2020;40:681–7.
Dylag AM, Tulloch J, Paul KE, Meyers JM. A quality improvement initiative to reduce bronchopulmonary dysplasia in a level 4 NICU-golden hour management of respiratory distress syndrome in preterm newborns. Children. 2021;8:301.
Langley GL MR, Nolan KM, Nolan TW, Norman CL, Provost LP. The improvement guide: a practical approach to enhancing organizational performance. 2nd ed. San Francisco, CA, USA: Jossey-Bass Publishers; 2009.
Dargaville PA, Aiyappan A, De Paoli AG, Dalton RG, Kuschel CA, Kamlin CO, et al. Continuous positive airway pressure failure in preterm infants: incidence, predictors and consequences. Neonatology. 2013;104:8–14.
Gulczyńska E, Szczapa T, Hożejowski R, Borszewska-Kornacka MK, Rutkowska M. Fraction of inspired oxygen as a predictor of CPAP failure in preterm infants with respiratory distress syndrome: a prospective multicenter study. Neonatology. 2019;116:171–8.
Dani C, Berti E, Barp J. Risk factors for INSURE failure in preterm infants. Minerva Pediatr. 2010;62:19–20.
Provost LP, Murray SK. The health care data guide: learning from data for improvement. 2nd ed. Hoboken, NJ: John Wiley & Sons; 2022.
Tague NR. The Quality Toolbox. 2nd ed. Milwaukee, Wisconsin, USA: ASQ Quality Press; 2005.
Jensen EA, Dysart K, Gantz MG, McDonald S, Bamat NA, Keszler M, et al. The diagnosis of bronchopulmonary dysplasia in very preterm infants. An evidence-based approach. Am J Respir Crit Care Med. 2019;200:751–9.
QI Macros for Excel [Software]. Denver, CO: KnowWare International Inc.
Winckler B, McKenzie S, Lo H-y. A practical guide to QI data analysis: run and statistical process control charts. Hosp Pediatr. 2023;14:e83–e9.
IBM SPSS Statistics for Windows [Software]. Version 29010. Armonk, NY: IBM Corp.
Lo SC, Bhatia R, Roberts CT. Introduction of a quality improvement bundle is associated with reduced exposure to mechanical ventilation in very preterm infants. Neonatology. 2021;118:578–85.
Lee SM, Sie L, Liu J, Profit J, Lee HC. Evaluation of trends in bronchopulmonary dysplasia and respiratory support practice for very low birth weight infants: a population-based cohort study. J Pediatr. 2022;243:47–52.e2.
Acknowledgements
We thank Kelly Butler, RN, Amy Roseboom, RRT, Beth Fulford, RRT, and Jaclyn Smith, RRT for their support in project education, assistance in designing project interventions, and dissemination of project updates.
Author information
Authors and Affiliations
Contributions
Dr Welch conceptualized and designed the study, collected data, carried out the analyses, drafted the initial manuscript, and reviewed and revised the manuscript. Drs Rose and Barbato conceptualized and designed the study, supervised the data collection and analyses, drafted the initial manuscript, and reviewed and revised the manuscript. Ms Myers conceptualized and designed the study, collected data, assisted with data analysis, and reviewed and revised the manuscript. Dr Drayton Jackson designed the study, supervised data analysis, and reviewed and revised the manuscript. Dr Lien conceptualized and designed the study, supervised data collection and analysis, and reviewed and revised the manuscript. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval
This project was submitted to the Indiana University Institutional Review Board and deemed exempt (IRB #12007).
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Welch, B., Rose, R., Myers, J. et al. Decreasing early invasive mechanical ventilation exposure in preterm infants: a quality improvement initiative. J Perinatol (2024). https://doi.org/10.1038/s41372-024-02098-9
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41372-024-02098-9
