
Abstract
Several definitions of paediatric abdominal obesity have been proposed but it is unclear whether they lead to similar results. We assessed the prevalence of abdominal obesity using five different waist circumference-based definitions and their agreement with total body fat (TBF) and abdominal fat (AF). Data from 190 girls and 162 boys (Ballabeina), and from 134 girls and 113 boys (Kinder-Sportstudie, KISS) aged 5–11 years were used. TBF was assessed by bioimpedance (Ballabeina) or dual energy X-ray absorption (KISS). On the basis of the definition used, the prevalence of abdominal obesity varied between 3.1 and 49.4% in boys, and 4.7 and 55.5% in girls (Ballabeina), and between 1.8 and 36.3% in boys and 4.5 and 37.3% in girls (KISS). Among children considered as abdominally obese by at least one definition, 32.0 (Ballabeina) and 44.7% (KISS) were considered as such by at least two (out of five possible) definitions. Using excess TBF or AF as reference, the areas under the receiver operating curve varied between 0.577 and 0.762 (Ballabeina), and 0.583 and 0.818 (KISS). We conclude that current definitions of abdominal obesity in children lead to wide prevalence estimates and should not be used until a standard definition can be proposed.
Similar content being viewed by others


Introduction
Childhood obesity is increasing worldwide and represents a major public health concern. Paediatric obesity is commonly defined by comparing the child’s body mass index to gender and age-specific thresholds.1 Several thresholds of waist circumference (WC) have been proposed to define paediatric abdominal obesity.2, 3, 4, 5, 6 This multiplicity of definitions also hampers the adequate comparisons of abdominal obesity prevalence and incidence between studies. Hence, we used the data from two Swiss studies to assess the prevalence of paediatric abdominal obesity according to different WC-based criteria. We also evaluated its utility as a marker of body fat by assessing the agreement between the different definitions of abdominal obesity and (a) excess total body fat (TBF) and (b) excess abdominal fat (AF).
Materials and methods
Design and participants
Data from children aged 5–11 years of the Swiss Ballabeina (190 girls, 162 boys, ClinicaTrials.gov NCT00674544)7, 8 and Kinder-Sportstudie (KISS; 134 girls, 113 boys, ISRCTN15360785) studies9, 10 were used. Both studies were approved by the respective cantonal ethical committees and parents or legal representatives and, in the case of KISS, the children provided written informed consent. In KISS, parents and children were informed of the examination and could refuse the dual energy X-ray absorption, as a special consent was required for this examination. In the consent, it was mentioned that the irradiation from the DEXA (6–20 μSv) corresponds to the daily background irradiation exposure in Switzerland (yearly exposure 3000–4000 μSv).
Anthropometric measurements
In both studies, standing height was measured by a wall-mounted stadiometer (Seca, Basel, Switzerland; accuracy 0.2 cm) and body weight was measured using an electronic scale (Seca; accuracy 0.05 kg). WC was measured midway between the iliac crest and the lowest border of the rib cage using a flexible tape. Supra-iliac skin-fold thickness was measured in triplicate to the nearest 0.5 mm with Harpenden callipers (HSK-BI, British Indicators Ltd, West Sussex, UK). In Ballabeina, the intra- and interobserver Spearman’s rank correlations were 0.95 (P<0.001) and 0.90 (P<0.001), respectively, for WC, and 0.98 (P<0.001) and 0.96 (P<0.001), respectively, for skin-fold measurement.7 In KISS, interobserver coefficient of variation for skin-fold measurement was 7.5%. For both studies, supra-iliac skin-fold thickness was used as a measure of AF.11 A child was considered as presenting excess AF if his/her skin-fold thickness was ⩾90th Swiss age- and gender-specific thresholds.11
Body fat percentage was used as the measure for TBF. In Ballabeina, TBF was estimated by a four-polar single frequency bioimpedance analysis (BIA) device (RJL Systems, Model 101A; Detroit, MI, USA) and was calculated from lean mass assessed by an equation (lean mass=((0.77 × gender)+(0.46 × age)+(0.32 × weight)+(0.41 × height2/resistance)−0.77), with boys=1 and girls=0; age in years, weight in kg and height in cm) previously validated against dual energy X-ray absorption.12 In KISS, body fat was estimated using dual energy X-ray absorption assessed by a Hologic QDR-4500 densitometer coupled with paediatric software (Hologic, Waltham, MA, USA). Excess TBF was defined according to gender- and age-specific thresholds for body fat.13
Abdominal obesity
Abdominal obesity was defined using five different published criteria.2, 3, 4, 5, 6 As one study presented data according to ethnicity,6 the results for white children were used, as this corresponds to the majority of children in Switzerland.
Statistical analysis
Statistical analysis was conducted using Stata version 12 (Stata Corp, College Station, TX, USA). Prevalence of abdominal obesity was presented as percentage and 95% confidence interval, supposing a binomial distribution. Comparisons between genders were performed using Student’s t-test for quantitative values and χ2 or Fisher’s exact test for qualitative values. Associations between WC and TBF or AF were assessed using nonparametric Spearman’s correlation. For each definition of abdominal obesity, we assessed the area under the receiver operating curve as well as the sensitivity, specificity, positive and negative predictive values and corresponding 95% confidence intervals. Excess TBF or AF expressed as a binary variable (yes/no) were used as reference. Statistical significance was considered for P<0.05.
Results
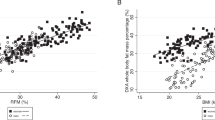
WC was significantly associated with TBF: in Ballabeina, Spearman’s r=0.682 in girls and r=0.641 in boys; in KISS, r=0.608 in girls and r=0.471 in boys (all P<0.001). Similar findings were obtained with AF: in Ballabeina, Spearman’s r=0.682 in girls and r=0.641 in boys; in KISS, r=0.817 in girls and r=0.768 in boys (all P<0.001).
Prevalence of abdominal obesity
The prevalence of abdominal obesity according to the different criteria is summarized in Table 1. In Ballabeina, the prevalence of abdominal obesity varied between 3.1 and 49.4% in boys and between 3.2 and 55.3% in girls. In KISS, the prevalence of abdominal obesity varied between 1.8 and 36.3% in boys and between 4.5 and 37.3% in girls (Table 1).
Among all children considered as being abdominally obese by at least one definition, only 32% (Ballabeina) and 44.7% (KISS) were considered as such by at least two (out of five possible) definitions. Further, among all children considered as being abdominally obese by at least one definition, only 5.9% (Ballabeina) and 8.5% (KISS) were considered as such by all five definitions.
Association of abdominal obesity with excess fat
The area under the receiver operating curve, sensitivities, specificities, positive and negative predictive values for each WC definition using excess TBF as reference are summarized in Table 2. In both studies, three definitions of abdominal obesity showed low sensitivities and high specificities; one definition (Katzmarzyk et al.6) showed high sensitivity but low-to-moderate specificity and one definition (McCarthy et al.5) achieved low-to-moderate sensitivity and high specificity. Similar findings were obtained when AF was used (Supplementary Table 1).
Discussion
Standard definitions of disease and symptoms are needed to adequately compare prevalence rates and clinical data between studies or countries.1, 14, 15 Several definitions of paediatric abdominal obesity have been proposed,2, 3, 4, 5, 6 but few studies have compared prevalence rates obtained by the existing definitions.
The prevalence of abdominal obesity varied almost 20-fold, depending on the definition used. Some definitions led to significant differences in prevalence rates of abdominal obesity between genders, while others did not. These differences are most probably because of the differing criteria to define WC thresholds. For instance, three definitions used gender- and age-specific percentiles,2, 4, 5 whereas one used s.d.3 and one an ‘optimal’ value based on other risk factors.6 The WC thresholds used to define abdominal obesity might also be population specific: optimal WC values reported by Katzmarzyk et al.6 are close to the 75th percentile of the percentile charts by McCarthy et al.5 and are lower than the 50th percentile of that reported by Fernandez et al.2 Interestingly, German values collected in the 1990 s and 2000 s4 were 4 cm higher than the British values collected in the 1970 s and 1980 s,5 suggesting a considerable secular increase in mean WC values in the paediatric population. Our results thus indicate that the WC thresholds obtained in one population might not be directly applicable to other populations, thus precluding valid comparisons. A better option would be to define global cut-offs, as it has been done with body mass index.1
A high specificity has been recognized as the most clinically important feature in order to avoid incorrect diagnosis of obesity.16 Using excess TBF as a reference, all but one6 definition presented specificity levels over 90%. Still, this occurred mostly at the expense of a lower sensitivity, indicating that only a small fraction of children with excess TBF or AF are adequately screened. Most importantly, only a minority of children were considered as presenting with abdominal obesity by all definitions. This would not only hamper diagnosis at the clinical setting (one child being considered as normal or abdominally obese depending on the definition use) but also hinder any global preventive strategy, as children in need of supportive measures would change according to the definition applied.
This study has some limitations. For instance, both studies were conducted in a specific setting and might not be fully representative of the Swiss population. Still, in the absence of a representative survey on Swiss children, we do believe that our results are of importance regarding the impact of choosing one definition of abdominal obesity relative to the others. It should also be noted that the data between Ballabeina and KISS are fairly comparable. Second, the association between WC and cardiometabolic risk factors varies according to the WC measurement site.17 Both studies used WC measured midway between the iliac crest and the lowest rib, a measurement site considered the most associated with cardiometabolic risk factors.17 Finally, supra-iliac skin-fold thickness assesses abdominal subcutaneous fat and not visceral adipose tissue that is metabolically more active than subcutaneous adipose tissue.18 Still, both abdominal visceral adipose tissue and subcutaneous adipose tissue are associated with adverse cardiometabolic risk factors, although the relationship with visceral adipose tissue is stronger.19
In summary, our results indicate that the prevalence of paediatric abdominal obesity varies considerably according to the definition applied, thus precluding direct comparisons among studies. Our results also indicate that some definitions fail to adequately screen children with excess TBF or abdominal BF.
References
Cole TJ, Bellizzi MC, Flegal KM, Dietz WH . Establishing a standard definition for child overweight and obesity worldwide: international survey. BMJ 2000; 320: 1240–1243.
Fernandez JR, Redden DT, Pietrobelli A, Allison DB . Waist circumference percentiles in nationally representative samples of African-American, European-American, and Mexican-American children and adolescents. J Pediatr 2004; 145: 439–444.
Fredriks AM, van Buuren S, Fekkes M, Verloove-Vanhorick SP, Wit JM . Are age references for waist circumference, hip circumference and waist-hip ratio in Dutch children useful in clinical practice? Eur J Pediatr 2005; 164: 216–222.
Schwandt P, Kelishadi R, Haas GM . First reference curves of waist circumference for German children in comparison to international values: the PEP Family Heart Study. World J Pediatr 2008; 4: 259–266.
McCarthy HD, Jarrett KV, Crawley HF . The development of waist circumference percentiles in British children aged 5.0-16.9 y. Eur J Clin Nutr 2001; 55: 902–907.
Katzmarzyk PT, Srinivasan SR, Chen W, Malina RM, Bouchard C, Berenson GS . Body mass index, waist circumference, and clustering of cardiovascular disease risk factors in a biracial sample of children and adolescents. Pediatrics 2004; 114: e198–e205.
Niederer I, Kriemler S, Zahner L, Burgi F, Ebenegger V, Hartmann T et al. Influence of a lifestyle intervention in preschool children on physiological and psychological parameters (Ballabeina): study design of a cluster randomized controlled trial. BMC Public Health 2009; 9: 94.
Puder JJ, Marques-Vidal P, Schindler C, Zahner L, Niederer I, Burgi F et al. Effect of multidimensional lifestyle intervention on fitness and adiposity in predominantly migrant preschool children (Ballabeina): cluster randomised controlled trial. BMJ 2011; 343: d6195.
Zahner L, Puder JJ, Roth R, Schmid M, Guldimann R, Puhse U et al. A school-based physical activity program to improve health and fitness in children aged 6-13 years ("Kinder-Sportstudie KISS"): study design of a randomized controlled trial [ISRCTN15360785]. BMC Public Health 2006; 6: 147.
Kriemler S, Zahner L, Schindler C, Meyer U, Hartmann T, Hebestreit H et al. Effect of school based physical activity programme (KISS) on fitness and adiposity in primary schoolchildren: cluster randomised controlled trial. BMJ 2010; 340: c785.
Prader A, Largo RH, Molinari L, Issler C . Physical growth of Swiss children from birth to 20 years of age. First Zurich longitudinal study of growth and development. Helv Paediatr Acta Suppl 1989; 52: 1–125.
Kriemler S, Puder J, Zahner L, Roth R, Braun-Fahrlander C, Bedogni G . Cross-validation of bioelectrical impedance analysis for the assessment of body composition in a representative sample of 6- to 13-year-old children. Eur J Clin Nutr 2009; 63: 619–626.
McCarthy HD, Cole TJ, Fry T, Jebb SA, Prentice AM . Body fat reference curves for children. Int J Obes 2006; 30: 598–602.
Mascarenhas MN, Cheung H, Mathers CD, Stevens GA . Measuring infertility in populations: constructing a standard definition for use with demographic and reproductive health surveys. Popul Health Metr 2012; 10: 17.
Thygesen K, Alpert JS, Jaffe AS, Simoons ML, Chaitman BR, White HD et al. Third universal definition of myocardial infarction. Eur Heart J 2012; 33: 2551–2567.
Krebs NF, Himes JH, Jacobson D, Nicklas TA, Guilday P, Styne D . Assessment of child and adolescent overweight and obesity. Pediatrics 2007; 120 (Suppl 4): S193–S228.
Bosy-Westphal A, Booke CA, Blocker T, Kossel E, Goele K, Later W et al. Measurement site for waist circumference affects its accuracy as an index of visceral and abdominal subcutaneous fat in a Caucasian population. J Nutr 2010; 140: 954–961.
Taksali SE, Caprio S, Dziura J, Dufour S, Cali AM, Goodman TR et al. High visceral and low abdominal subcutaneous fat stores in the obese adolescent: a determinant of an adverse metabolic phenotype. Diabetes 2008; 57: 367–371.
Liu J, Fox CS, Hickson DA, May WD, Hairston KG, Carr JJ et al. Impact of abdominal visceral and subcutaneous adipose tissue on cardiometabolic risk factors: the Jackson Heart Study. J Clin Endocrinol Metab 2010; 95: 5419–5426.
Acknowledgements
The Ballabeina study was mainly supported by the Swiss National Science Foundation (Grant number 3200B0-116837) and Health Promotion Switzerland (Project number 2104). Additional funding was obtained from a research award for Interdisciplinary Research from the University of Lausanne, a Takeda research award, the Wyeth Foundation for the Health of children and adolescents, the Freie Akademische Gesellschaft and an unrestricted educational grant from Nestlé. The KISS study was funded by the Swiss Federal Office of Sports (FOSPO), Grant number SWI05-013. We thank Professors R Gaillard, S Fanconi and F Ohl who helped to make this study possible. A special thanks to all children, their parents, the school teachers and the respective school health services.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Additional information
Author contributions
JP and AMP made part of the statistical analyses and wrote most of the manuscript; PMV directed the analyses and wrote part of the article; FB, VE, IN and SK collected the data and revised the manuscript; AN revised the article for intellectual content. PMV had full access to the data and is the guarantor of the study.
Supplementary Information accompanies this paper on the Nutrition & Diabetes website
Supplementary information
Rights and permissions
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 3.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-sa/3.0/
About this article
Cite this article
Pinto, A., Puder, J., Bürgi, F. et al. Discordances in the application of different criteria for quantification of paediatric abdominal obesity: an analysis of two Swiss studies. Nutr & Diabetes 3, e67 (2013). https://doi.org/10.1038/nutd.2013.7
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/nutd.2013.7
